
Medication Adherence: Understanding and Measuring Patients’ Treatment-Related Behaviour - ICON...
41
The ICON Signature Series ICON’s thought and leadership program
-
Upload
iconplc -
Category
Health & Medicine
-
view
118 -
download
0
Transcript of Medication Adherence: Understanding and Measuring Patients’ Treatment-Related Behaviour - ICON...
The ICON Signature Series
ICON’s thought and leadership program

ICON Signature Series is ICON’s thought
leadership program that offers expert
insight into value-driven strategies for
clinical development.
Built on over 20 years of helping biopharma
companies accelerate the development and
reimbursement of their drugs, ICON
Signature Series brings together ICON
and industry experts to share knowledge
and expertise across all aspects of clinical
development and post-approval strategies.
To access the latest materials and schedule
of upcoming events, go to
ICONplc.com/icon-views

Medication Adherence: Understanding and Measuring Patients’ Treatment-Related Behaviour
18 June 2014
Expert Panellists:
Sarah Clifford, PhDDirector of Patient Reported OutcomesICON plc
Jennifer Devlen, PhDLead Outcomes ResearcherPatient Reported Outcomes ICON plc

“Drugs don’t work in patients who don’t take them”
- Former US surgeon general C.Everett Koop
Why Are We Interested?
1) To provide an overview of terminology associated with patients’ medication-taking behavior: adherence, compliance, concordance, persistence
2) To summarize the extent and consequences of non-adherence
3) To discuss the reasons why patients are non-adherent to their prescribed medication
4) To provide an overview of methods to measure medication adherence, with a particular focus on patient-reported methods
5) To explore evidence on interventions to improve medication adherence
Objectives

Terminology
• Adherence/ComplianceExtent to which a patient acts in accordance with the prescribed interval and dose (Cramer et al, 2008) • Dosage• Frequency• Timing
• PersistenceExtent to which patient continues the treatment for the prescribed length of time

Terminology
• ConcordanceAgreement between the patient and health care professional, reached after negotiation….in determining whether, when and how their medicine is taken and (in which) the primacy of the patient’s decision (is recognized)” (Marinker et al, 1997)
Emphasizes shared decision making
Concordance relates to a process, and represents a model of care (Cushing and Metcalfe, 2007)
• Adherence (Compliance) and Persistence should be the terms for measurement (De las Cuevas, 2011)
• In chronic conditions, adherence averages 50% (WHO 2013)
• Up to 20% of patients do not fill prescription (initial non-adherence) (McHorney 2009)
• Approximately 50% discontinue medication within 6 months (lack of persistence) (McHorney 2009)
• Even in clinical trials, adherence rates are only 43% - 78% (Osterberg & Baschke, 2005)
What is the Magnitude of the Problem?
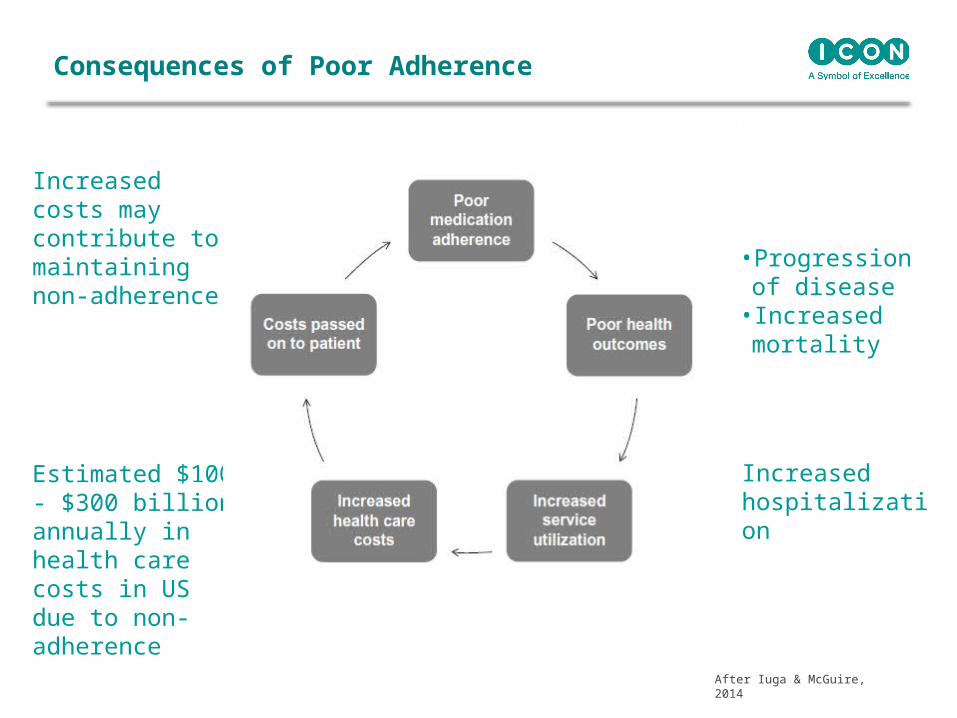
Increased costs may contribute to maintaining non-adherence
After Iuga & McGuire, 2014
Estimated $100 - $300 billion annually in health care costs in US due to non-adherence
• Progression of disease
• Increased mortality
• Increased hospitalization
Consequences of Poor Adherence
Commercialisation & Outcomes
Diabetes
Examples: Adherence and Methods
Inflammatory Bowel Disease
Adherence to oral hypoglycemic agents (OHAs) 36% - 93% of doses taken as prescribed (Cramer 2004)
Persistence with OHAs16% - 80% remaining on treatment at end of study period (Cramer 2004)
Adherence to insulin4.5 % incorrect dosing of insulin (Mulvaney et al, 2010)
2% incorrect dosing at potentially dangerous level (Toussi et al, 2008)
Diabetes: Adherence
• Large study of patients with diabetes treated with oral hypoglycemics, antihypertensives and statin medications (Ho et al, 2006)
• Adherence calculated as proportion of days covered for filled prescriptions
• Compared to adherent patients, non-adherent patients (proportion of days covered <80%) had poorer clinical outcomes:
-Higher glycosylated hemoglobin
-Higher LDL cholesterol levels
-Higher systolic and diastolic blood pressure
-Higher all-cause hospitalization
-Higher all-cause mortality
Diabetes: Consequences of Non-Adherence
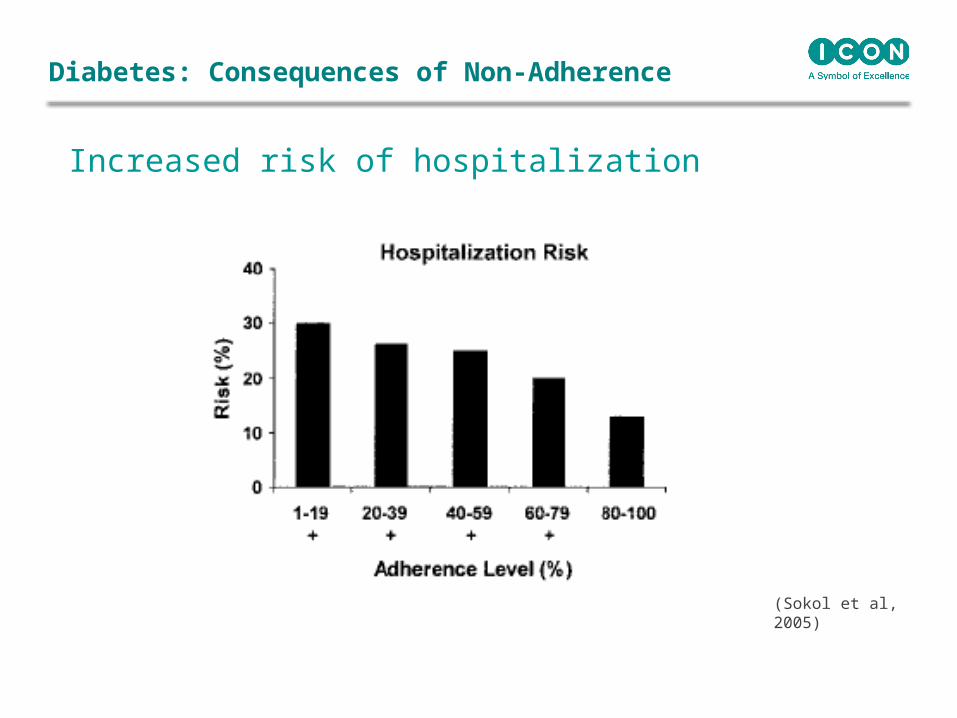
Increased risk of hospitalization
Diabetes: Consequences of Non-Adherence
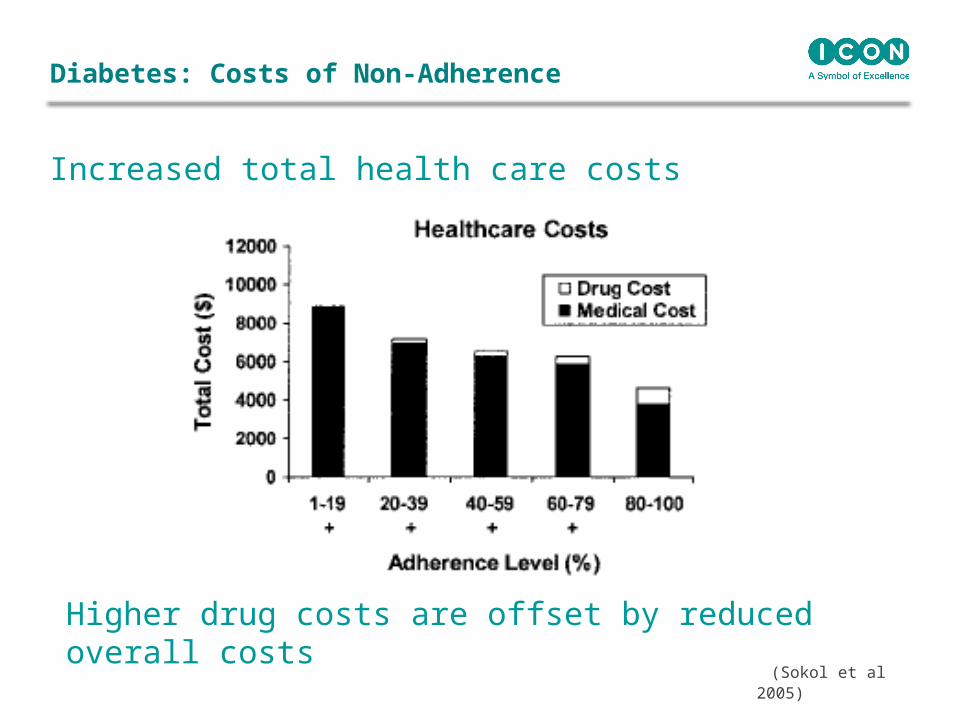
(Sokol et al, 2005)
(Sokol et al 2005)
Increased total health care costs
Higher drug costs are offset by reduced overall costs
Diabetes: Costs of Non-Adherence
• Ulcerative Colitis and Crohn’s Diseaseo Mesalamines to induce and maintain remission
• Non-adherence is high: 20%-50% (Kane et al, 2008)
• Associated with poorer outcomes - increased risk of flare and of colorectal cancer
• Qualitative research to explore patient adherence (Devlen et al, 2014)
• Patient descriptions of adherence and reasons for non-adherence
• Focus groups or one-on-one interviews with 27 patients
11% (n=3) complete adherence
89% (n=24) reported non-adherence and/or non-persistence
Inflammatory Bowel Disease: Adherence

Missing doses- Missed a few times a week- Regularly missed some doses per day, many days per week
“I was trying to space them out throughout the day - breakfast, lunch, dinner, and bedtime. Invariably I would miss a couple of those. ..Almost every day”.
- Regularly missed whole days“I would take it some days and some days I'd forget, or I'd be just like ah, whatever”.
Patients may not perceive late dosing as non-adherenceInterviewer: what happens if you forget pills or doses?
Patient: It hasn’t happened
On further probing…
Interviewer: Have you ever taken it late?
Patient: Yes...it’s still in the same day, the same day cycle, but it’s later than normal.
If timing of medication is important, need to enquire about adherence to the schedule.
Inflammatory Bowel Disease: Non-Adherence

Taking more than prescribed
“There are days where maybe I took 6 and maybe I took 0…I might take it twice”
Lack of Persistence
“I kind of gave up on it. .. I doubted that it was even doing anything for me. So, I just stopped taking it”
Inflammatory Bowel Disease
Devlen et al, 2014
• Missed doses • Delayed doses• Reduced dosing• Increased doses• Medication breaks/‘holidays’ and discontinuation • Other deviations from regimen requirements e.g. food or fasting
requirements, remaining upright
• Qualitative research can provide valuable information:• To understand patients’ medication-taking behavior
- Can inform optimal method of measuring adherence
Eg. if patients decant pills into portable bags, electronic monitoring of pill bottle would be less useful method
• To understand reasons for non-adherence- Can inform interventions to improve adherence
Non-Adherence and Non-Persistence across all conditions
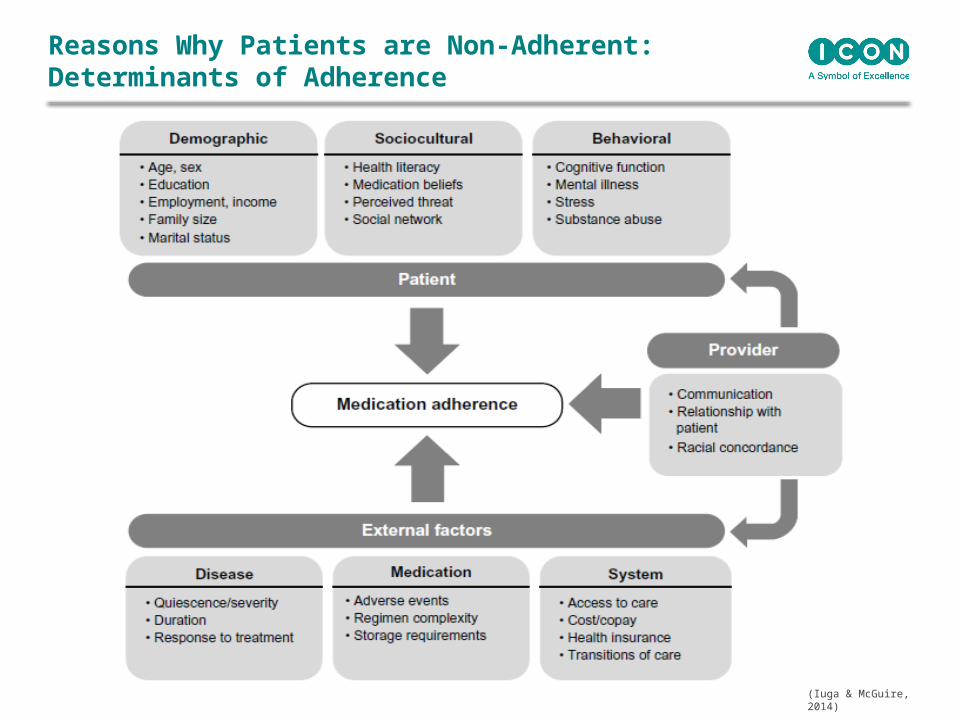
(Iuga & McGuire, 2014)
Reasons Why Patients are Non-Adherent: Determinants of Adherence

Measurements
Similarities/Differences of Adherence to other PROs
Similarities
• Relies heavily on patient self-report
• Measurement issues such as reliability and validity are crucial
• Prone to issues such as recall bias, hence choice of appropriate recall period is critical
Differences
• Medication adherence is a different type of concept – i.e. behavior, rather than symptom or QoL impact
• Social desirability is more of an issue as we are asking patients to report on something they are supposed to be actively doing, rather than something they experience or perceive

Measuring Medication Adherence
Adherence Measurement
Strength Weakness
Patient self-report (questionnaires, interviews, diaries)
Easy to administer (in-person, phone, mail, ePRO), can capture overall adherence or details on intentional vs. unintentional non-adherence, can be inexpensive compared to other methods
May overestimate true level of adherence, potential for recall bias, numeracy and literacy issues could influence reporting
Pharmacy refill claims (to calculate MPR)
Avoids the “Hawthorne effect”, data are relatively accessible and inexpensive compared to some other methods of measuring adherence
Prescription refill is not equivalent to medication ingestion, patients may use more than one pharmacy, documentation errors, no insight in to reasons for non-adherence
Electronic monitoring (e.g. MEMS)
Precise, tracks patterns of medication-taking (electronic chip records time and date medication bottle was opened)
Expense prevents widespread use, bottle opening is not equivalent to medication ingestion
Pill count Opportunity to discuss reasons for non-adherence with the patient when they bring in their pills for counting
Inconvenient as patient has to bring in pills , data easily altered by the patient (e.g. pill dumping), human error can occur when counting the pills
Medication level in blood or urine
Seen as a direct method of measuring adherence, can verify recent use of the medication
Variation in pharmacokinetics between individuals may affect accuracy of results, patients may take meds only before having the blood/urine test

Selecting a Method of Measurement
• No universally accepted “gold standard” method of measurement and wide range of methods available
• When selecting an appropriate method, consider:• Research question• Study design• Target patient population• Timeline• Resources
Systematic Review of PRO Adherence Measures

Methods: Aim and Databases
• Aim: to conduct a systematic review of studies addressing the development, validation and reliability of self-reported adherence measures
• Electronic databases:• Medline• EMBASE• Pharmline• CINAHL• PsychINFO• HaPI
Garfield, Clifford et al (2011)

Key Findings
Characteristic Summary
Number of items Ranged from 1 to 21
Recall period 2 days, 3 days, 4 days, 7 days, 1 week, 1 month, 2 months, 3 months, 6 months, in general (or none reported)
Mode of administration Pen and paper, electronic, face to face or telephone interview
Response options Dichotomous, Likert scale, Visual Analogue Scale
• 1,026 abstracts were screened, and 264 full-text articles• 76 papers met the inclusion criteria• 58 adherence PRO measures identified
Garfield, Clifford et al (2011)
Limitations with Previous PRO Adherence Measures
• Relatively limited psychometric evaluation
• Little detail provided about the scale development
• Few were described as being based on a conceptual/theoretical model
• Intentional and unintentional non-adherence were only distinguished from each other in one measure
• No measures which reported having a version that could be completed by carers of patients
Garfield, Clifford et al (2011)
Adherence PROs: Generic Examples
• Morisky Medication Adherence Scale (MMAS)
• Medication Adherence Report Scale (MARS)
• Medication Assessment Questionnaire (MAQ)
• Brief Medication Questionnaire (BMQ)
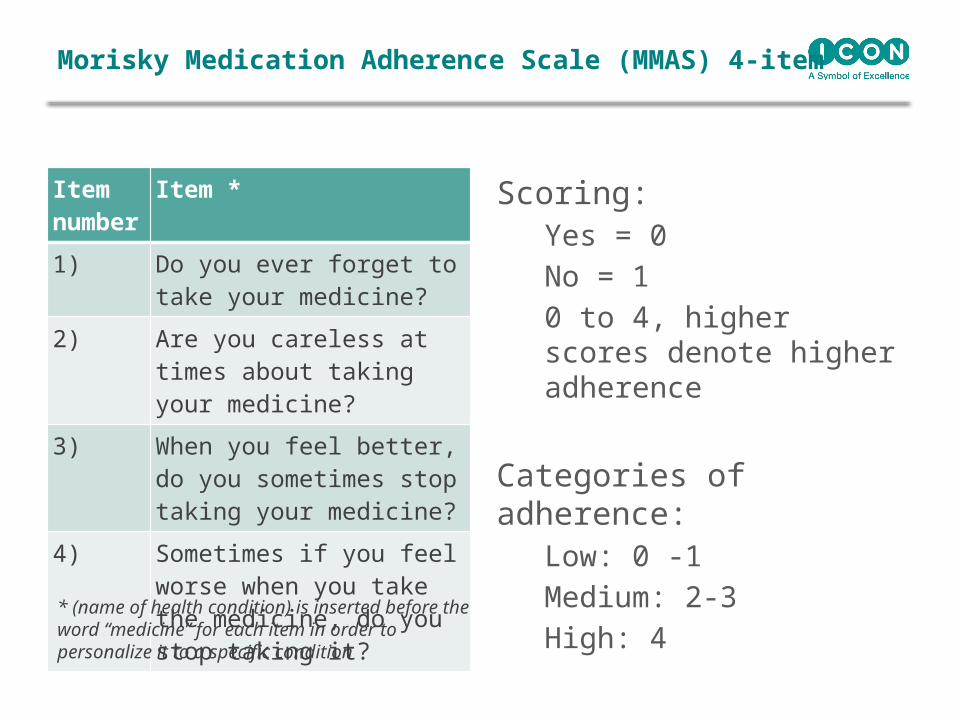
Item number
Item *
1) Do you ever forget to take your medicine?
2) Are you careless at times about taking your medicine?
3) When you feel better, do you sometimes stop taking your medicine?
4) Sometimes if you feel worse when you take the medicine, do you stop taking it?
Scoring:Yes = 0
No = 1
0 to 4, higher scores denote higher adherence
Categories of adherence:Low: 0 -1
Medium: 2-3
High: 4
Morisky Medication Adherence Scale (MMAS) 4-item
* (name of health condition) is inserted before the word “medicine” for each item in order to personalize it to a specific condition

Adherence PROs: Disease-Specific Examples
• Diabetes: • Diabetes Self-Care Inventory (DSCI)• Diabetes Self-Care Activities (DSCA)• Diabetes Self-Management Profile (DSMP)
• HIV:• Adult AIDS Clinical Trials Group (AACTG) Instrument
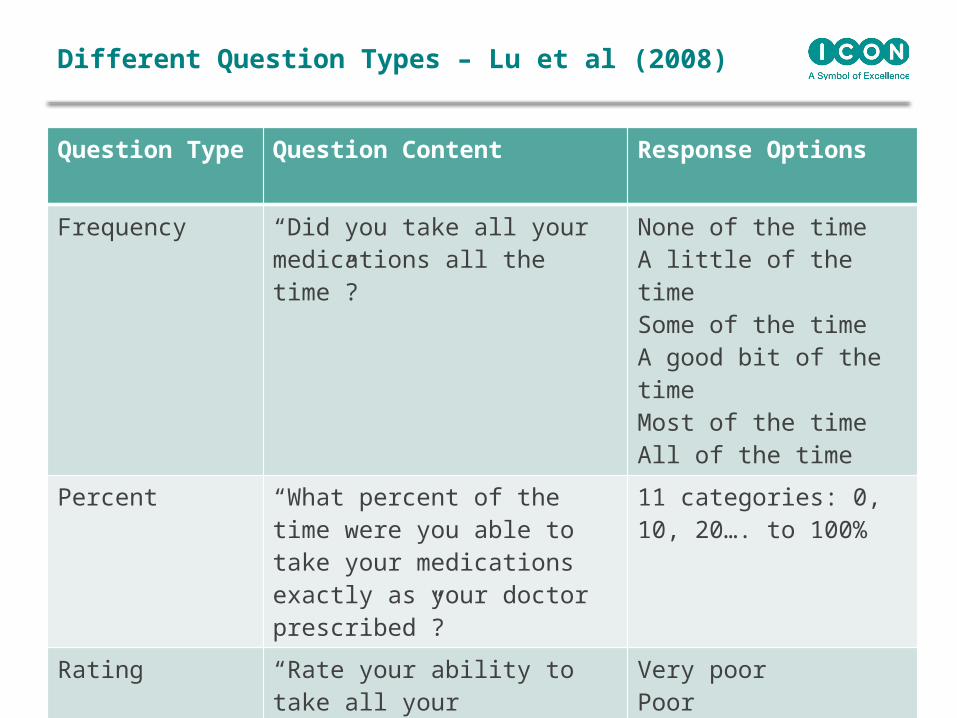
Different Question Types – Lu et al (2008)
Question Type Question Content Response Options
Frequency “Did you take all your medications all the time”?
None of the timeA little of the timeSome of the timeA good bit of the timeMost of the timeAll of the time
Percent “What percent of the time were you able to take your medications exactly as your doctor prescribed”?
11 categories: 0, 10, 20…. to 100%
Rating “Rate your ability to take all your medications as prescribed”
Very poorPoorFairGoodVery goodExcellent
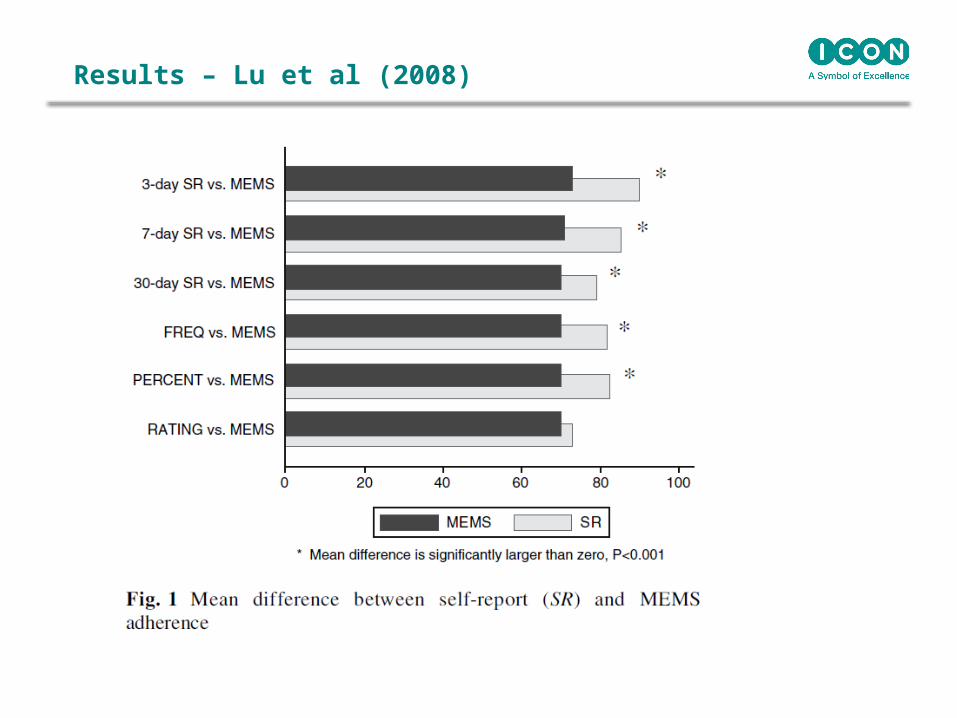
Results – Lu et al (2008)

Selecting a PRO Measure of Adherence
• No universally accepted “gold standard” PRO measure of adherence
• When selecting an appropriate measure, consider:• Target patient population:
- Disease-specific version may be available and more relevant than one of the typically used generic adherence PROs
• Research question:
- Measure extent AND/OR reasons for non-adherence?• Study design and mode of administration

How Much Adherence is Enough?
• Widely used cutoff: 80%
• Appropriate cutoff will depend on:• The specific disease, medication, formulation etc.
• Disease-specific examples:• HIV: 95% (Paterson et al, 2000)• Chronic myeloid leukemia: 90% (Marin et al, 2010)
• Further research is needed in other conditions to understand appropriate cutoffs to classify patients as adherent vs. non-adherent
Clifford & Coyne (in press – July/Aug 2014) JMCP – What is the Value of Medication Adherence?

Improving Adherence

Patient
Family Payers
Pharmaceutical Industry
Policy makers
Health care providers
Who is Interested in Improving Adherence?
Can We Improve Adherence?
• Cochrane Review (Haynes et al, 2008):
• Yes we can, but…there is no “one-size fits all” solution.
• Patient-focused solutions are most successful
• Educational interventions alone are typically not successful
• Need to target knowledge, memory AND motivation
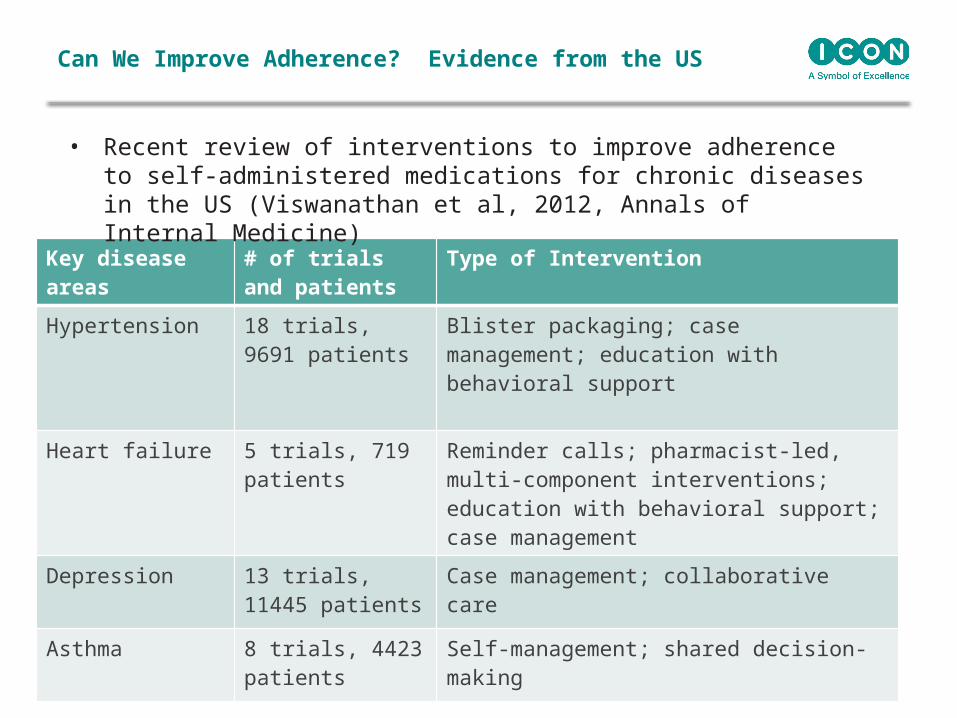
Can We Improve Adherence? Evidence from the US
Key disease areas
# of trials and patients
Type of Intervention
Hypertension 18 trials, 9691 patients
Blister packaging; case management; education with behavioral support
Heart failure 5 trials, 719 patients
Reminder calls; pharmacist-led, multi-component interventions; education with behavioral support; case management
Depression 13 trials, 11445 patients
Case management; collaborative care
Asthma 8 trials, 4423 patients
Self-management; shared decision-making
• Recent review of interventions to improve adherence to self-administered medications for chronic diseases in the US (Viswanathan et al, 2012, Annals of Internal Medicine)
Need for Further Research
• Measurement:• Appropriate PROs that are valid and reliable• Appropriate cut-points for adherent/non-adherent
• Understanding:• Reasons for non-adherence relevant to specific patient
populations
• Interventions:• Better understanding of how and why interventions work
(or don’t work)• Inclusion of clinical and cost outcomes• Approaches for patients with multiple comorbid conditions
Conclusion
• Non-adherence to medication is a significant problem:• Missed opportunity for therapeutic gain• Poor health outcomes/quality of life impact• Increased costs
• Range of methods available to measure adherence:• Consider research question, study design, patient
population, resources
• Increasing evidence on interventions to improve adherence:• From policy to patient-level initiatives – potential to
improve adherence and health outcomes and reduce unnecessary health care costs
Like to know more?
Twitter handle: @ICONplc
Join us on social:


















