Medically Indicated Deliveries Before 39 weeks
56
Medically Indicated Deliveries Before 39 Weeks Gestational Age “MIDB39 weeks” Chukwuma I. Onyeije, M.D. Chukwuma I. Onyeije, M.D. Atlanta Perinatal Associates Atlanta Perinatal Associates 1
-
Upload
chukwuma-onyeije -
Category
Health & Medicine
-
view
1.743 -
download
1
description
A presentation on Medically Indicated Deliveries Before 39 weeks. Includes updated information from ACOG. Medically indicated late-preterm and early-term deliveries. Committee Opinion No. 560. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;121:908–10.
Transcript of Medically Indicated Deliveries Before 39 weeks

Medically Indicated Deliveries Before 39
Weeks Gestational Age
“MIDB39 weeks”
Chukwuma I. Onyeije, M.D.Chukwuma I. Onyeije, M.D.
Atlanta Perinatal AssociatesAtlanta Perinatal Associates11

22
Research and Experience Show:
Early ELECTIVE delivery without MEDICAL or OBSTETRICAL indication is linked to neonatal morbidities with NO benefit for the mother or infant.
HOWEVER….
There are numerous maternal and fetal indications for deliveries BEFORE 39 weeks gestation
ALSO…
Elective deliveries AFTER 39 weeks are not necessarily without risks for mother and infant.

Is there really a problem here?
“What’s the big deal?”
“It’s only a couple of days?”
“No one is going to tell me how to practice medicine.”
33
Actual quotes from OBGYN providers regarding 39 week policy. Circa 2002.

44
Inductions of LaborInductions of Labor
• ACOG has cautioned against inductions before 39 weeks in the absence of a medical indication since 1979. (Committee Opinion #22)
• ACOG also suggests that “a mature fetal lung maturity test result before 39 weeks of gestation, in the absence of appropriate clinical circumstances, is NOT an indication for delivery”
(Committee Practice Bulletins #97 and #107)


How did we get here?
66
1992To 2002“The Lost Decade”

Change in Distribution of Births by Gestational Age: United States, 1990-2006
Martin JA, Hamilton BE, Sutton PD, Ventura SJ, et al. Births: Final data for 2006. National vital statistics reports; vol 57 no 7. Hyattsville, MD: National Center for Health Statistics. 2009.

U.S. Cesarean Section and Labor Induction Rates Among Singleton Live Births by Week of Gestation, 1992 and 2002
Source: NCHS, Final Natality Data, Prepared by March of Dimes Perinatal Data Center, April 2006.
Gestational Age (week)
2002 Induction
2002 C-S
1992 C-S
1992 Induction
Ear
ly T
erm
Per
cen
t o
f S
ing
leto
n L
ive
Bir
ths
(%)

Rates of Induction of Labor in Singleton Births by Race and Hispanic Origin in the U.S.
Martin JA, Hamilton BE, Sutton PD, Ventura SJ, et al. Births: Final data for 2006. National vital statistics reports; vol 57 no 7.Hyattsville, MD: National Center for Health Statistics. 2009.

04/11/23Davidoff et al Sem Perinatology 2006
Per
cent
Sin
glet
on L
ive
Birt
hsChanging Distribution of US Live Births 1992 - 2002

Why are Non-medically Indicated (Elective) Deliveries
Increasing in Frequency?

Obstet Gynecol 2009;114:1254

The Gestational Age that Women Considered a Baby to be Full Term
Obstet Gynecol 2009;114:1254
3.3%3.3%
17.4%
21.7%
29.1%
4.8%
20.8%

The Gestational Age that Women Considered it Safe to Deliver
34 35 36 37 38 39 400%
5%
10%
15%
20%
25%
30%
35%
14%
7%
31%
22%
19%
3% 4%
Weeks of Gestation
Wom
en's
Resp
onse
s
Obstet Gynecol 2009;114:1254
Weeks of Gestation

Pressure on Obstetricians
Clin Obstet Gynecol 2006;49:698-704
Reasons that physicians may resist elimination of elective deliveries < 39 weeks:
•Physician Convenience• Guarantee attendance at birth
(“co-dependency”)
• Avoid scheduling conflicts
• Reduce being awakened at night
•…what’s the harm?• Bad outcomes are unrecognized and rare
• The NICU handles these issues just fine
•Limit risk of a bad pregnancy outcome

Risks of Non-medically Indicated (Elective) Delivery
Before 39 Weeks

Complications of Non-medically Indicated (Elective) Deliveries Between 37 and 39 Weeks
Clark 2009, Madar 1999, Morrison 1995, Sutton 2001, Hook 1997
• Increased NICU admissions• Increased transient tachypnea of the newborn (TTN)• Increased respiratory distress syndrome (RDS) • Increased ventilator support• Increased suspected or proven sepsis• Increased newborn feeding problems and other transition
issues

QUESTION: WHO (EXACTLY) IS TERM?
1818

1919
OLD Terminology
Modified from Drawing courtesy of William Engle, MD, Indiana University
Raju TNK. Pediatrics, 2006;118 1207.
First day of LMP
0Week # 37 0/7 416/7
Preterm Term Post term
340/720 0/7 39 0/7
Late Preterm Early Term

2020October 31, 2013
NEW Terminology

Term Pregnancy Redefined byACOG and SMFM
Published in the November 2013 Green Journal.
Four new definitions of “term pregnancy” were issued by ACOG & SMFM in a joint Committee Opinion.
Terminology designed to put the focus on preventing deliveries before 39 weeks’ gestation.
2121
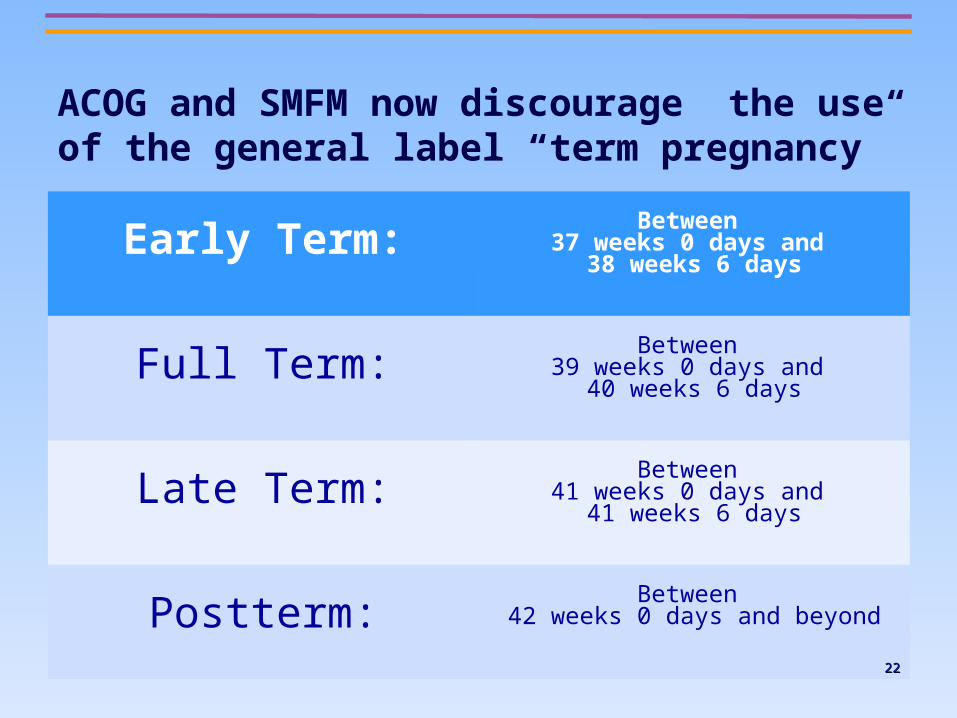
ACOG and SMFM now discourage the use of the general label “term pregnancy”
Early Term:Between
37 weeks 0 days and 38 weeks 6 days
Full Term:Between
39 weeks 0 days and 40 weeks 6 days
Late Term:Between
41 weeks 0 days and 41 weeks 6 days
Postterm:Between
42 weeks 0 days and beyond
2222

2323
Okay. How do I know if my patient is “Full Term”?

2424

Confirmation of Term Gestation
• Early ultrasound (< 20 weeks gestation) is more accurate than an ultrasound after 20 weeks gestation at determining gestational age and benchmarking < 39 weeks gestation.
• Ultrasound-established dates should take precedence over LMP-established dates when the discrepancy is greater than 7 days in the first trimester and 10 days in the second trimester… OR if the LMP-established dates are uncertain.
2525

Actual Case:
JT presented for prenatal care on 9/7/13 with an LMP of 2/19/13. She was assigned an EDD of 11/26/13 and an EGA of 28 weeks.
Her first ultrasound on 9/25/13 showed an EFW which placed her fetus at < 10 %tile.
Her second ultrasound on 10/28/13 showed an EFW which placed her fetus at < 10 %tile.
2626

At the time of her second ultrasound the physician performing the ultrasound asked if she had had any previous ultrasounds.
She pulled this out of her pocket from an emergency room visit on 5/23/13 (almost 5 months earlier) for spotting……
2727

2828
Date performed:5/23/13
CRL: 49.5 mm
EGA: 11w5d
Emergency Room Ultrasound

2929
NEW EDD: 12/7/13
NEW EFW %tile: 54%

Induction / Cesarean Scheduling Process
Induction / Cesarean Scheduling Process
Physician Leadership A. Enforce policy B. Approve exceptions
Physician Leadership A. Enforce policy B. Approve exceptions
Clinician and/or Patient Desire to Schedule a Non-medically
Indicated (Elective) Induction or Cesarean Section
Clinician and/or Patient Desire to Schedule a Non-medically
Indicated (Elective) Induction or Cesarean Section
Case NOT Scheduled if Criteria Not Met
Case NOT Scheduled if Criteria Not Met
Elective Delivery Hospital Policy
Elective Delivery Hospital Policy
Clinician, Staff & Patient EducationClinician, Staff &
Patient Education Reduce Demand
QI Data Collection & Trend Charts
QI Data Collection & Trend Charts
Public Awareness Campaign
Public Awareness Campaign
3030

3131
Okay. Okay. Let’s get Let’s get
real.real.
Not all deliveries before 39 weeks Not all deliveries before 39 weeks are for “convenience”.are for “convenience”.

Timing of Indicated Late-Preterm and Early-Term Birth.Obstetrics & Gynecology. 118(2, Part 1):323-333, August 2011.

ACOG Committee Opinion: April 2013
3333Medically indicated late-preterm and early-term deliveries. Committee Opinion No. 560. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;121:908–10.

ACOG Committee Opinion: April 2013
The neonatal risks of late preterm and early-term births are well established.
HOWEVER, there are a number of complications in which either a late-preterm or early-term delivery is warranted.
The timing of delivery must balance the maternal and newborn risks of late-preterm and early-term delivery with the risks of further continuation of pregnancy.
3434

ACOG Committee Opinion: April 2013
Decisions regarding timing of delivery must be individualized.
Amniocentesis for the determination of fetal lung maturity in well-dated pregnancies generally should not be used to guide the timing of delivery.
3535

Terminology Recall….
3636
Early Term:Between
37 weeks 0 days and 38 weeks 6 days
Full Term:Between
39 weeks 0 days and 40 weeks 6 days
Late Term:Between
41 weeks 0 days and 41 weeks 6 days
Postterm:Between
42 weeks 0 days and beyond

Terminology for Medically Indicated Deliveries
3737
Late PretermBetween 34 weeks 0 days and
36 weeks 6 days.
Early Term:Between
37 weeks 0 days and 38 weeks 6 days
Full Term:Between
39 weeks 0 days and 40 weeks 6 days
Late Term:Between
41 weeks 0 days and 41 weeks 6 days
Postterm:Between
42 weeks 0 days and beyond

Categories for Medically Indicated Deliveries:
3838

3939

Placental / Uterine Issues
Condition General Timing Suggested Specific Timing
PLACENTA PREVIA LATE PRETERM/EARLY TERM36 0/7 to 37 6/7
WEEKS OF GESTATION
PLACENTA PREVIA WITH SUSPECTED ACCRETA, INCRETA, OR
PERCRETA LATE PRETERM 34 0/7 to 35 6/7 WEEKS OF GESTATION
PRIOR CLASSICAL CESAREAN LATE PRETERM/EARLY TERM 36 0/7 to 37 6/7 WEEKS OF GESTATION
PRIOR MYOMECTOMY EARLY TERM/TERM (INDIVIDUALIZE)
37 0/7 to 38 6/7 WEEKS OF GESTATION
4040Medically indicated late-preterm and early-term deliveries. Committee Opinion No. 560. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;121:908–10.

4141

GROWTH RESTRICTION (SINGLETON)
Fetal issues
Condition General Timing Suggested Specific Timing
OTHERWISE UNCOMPLICATED, NO CONCURRENT FINDINGS EARLY TERM / TERM 38 0/7 to 39 6/7
WEEKS OF GESTATION
CONCURRENT CONDITIONS
(OLIGOHYDRAMNIOS, ABNORMALDOPPLER STUDIES, MATERNAL CO-
MORBIDITY (IE, PREECLAMPSIA, CHRONIC HYPERTENSION)
LATE PRETERM / EARLY TERM 34 0/7 to 37 6/7 WEEKS OF GESTATION
4242Medically indicated late-preterm and early-term deliveries. Committee Opinion No. 560. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;121:908–10.

GROWTH RESTRICTION (TWINS)FETAL ISSUES:
Condition General Timing Suggested Specific Timing
Di – Di TWINS WITH ISOLATED FETAL GROWTH
RESTRICTIONLATE PRETERM/EARLY TERM 36w 7d 37w 6d
GESTATION
Di – Di TWINS WITH CONCURRENT CONDITIONS LATE PRETERM 32w 7d 34w 6d
GESTATION
Mono – Di TWINS WITH ISOLATED FETAL GROWTH
RESTRICTIONLATE PRETERM 32w 7d 34w 6d
GESTATION
4343

MULTIPLE GESTATIONS
FETAL ISSUES:
Condition General Timing Suggested Specific Timing
Di – Di TWINS EARLY TERM38w 0d
38w 6dGESTATION
Mono - Di TWINS LATE PRETERM/EARLY TERM
34w 7d 37w 6d
WEEKS OF GESTATION
4444Medically indicated late-preterm and early-term deliveries. Committee Opinion No. 560. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;121:908–10.

OLIGOHYDRAMNIOS
FETAL ISSUES:
Condition General Timing Suggested Specific Timing
OLIGOHYDRAMNIOS LATE PRETERM EARLY TERM
36w 0d 37w 6d
GESTATION
4545Medically indicated late-preterm and early-term deliveries. Committee Opinion No. 560. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;121:908–10.

4646

HYPERTENSIVE DISORDERS
MATERNAL INDICATIONS
CONTROLLED & NO MEDICATIONS EARLY TERM/TERM
38w 0d 39w 6dGESTATION
CONTROLLED ON MEDICATIONS EARLY TERM/TERM
37w 0d 39w 6dGESTATION
DIFFICULT TO CONTROLLATE PRETERM/EARLY
TERM36w 0d 37w 6d
GESTATION
GESTATIONAL HYPERTENSIONEARLY TERM
37w 0d 38w 6dGESTATION
4747

HYPERTENSIVE DISORDERS(Preeclampsia)
MATERNAL INDICATIONS
SEVERE PREECLAMPSIA LATE PRETERMAT DIAGNOSIS AFTER 34w 0d GESTATION***
MILD PREECLAMPSIA EARLY TERM
AT DIAGNOSIS AFTER 37w 0d
GESTATION
4848*** Clinical judgment important
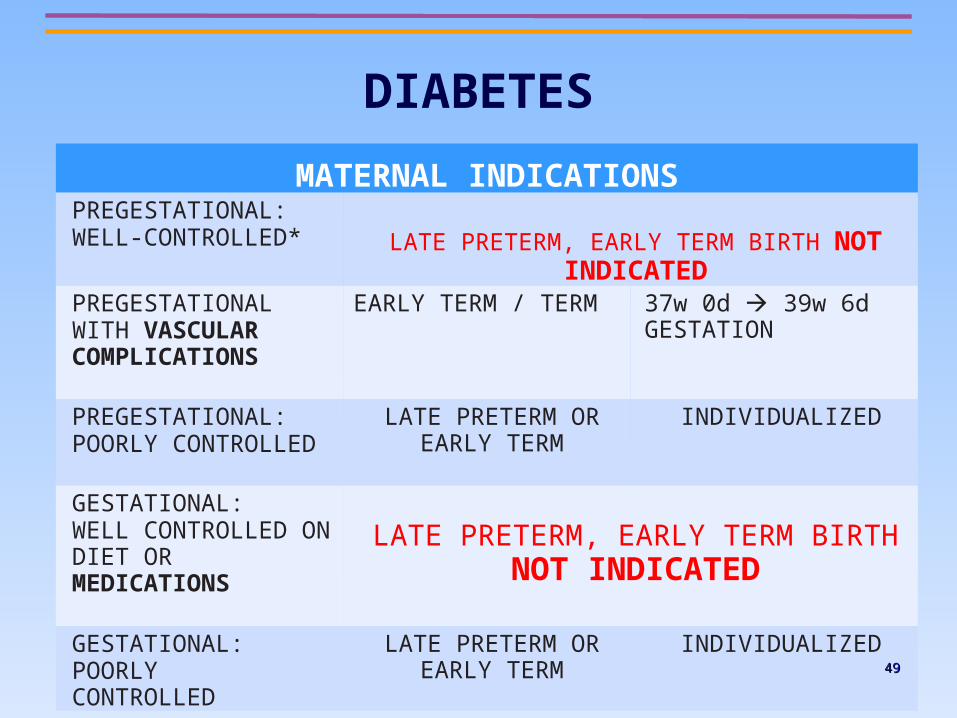
DIABETES
MATERNAL INDICATIONSPREGESTATIONAL: WELL-CONTROLLED* LATE PRETERM, EARLY TERM BIRTH NOT INDICATED
PREGESTATIONAL WITH VASCULAR COMPLICATIONS
EARLY TERM / TERM 37w 0d 39w 6d GESTATION
PREGESTATIONAL:POORLY CONTROLLED
LATE PRETERM OR EARLY TERM
INDIVIDUALIZED
GESTATIONAL:WELL CONTROLLED ON DIET OR MEDICATIONS
LATE PRETERM, EARLY TERM BIRTH NOT INDICATED
GESTATIONAL:POORLY CONTROLLED
LATE PRETERM OR EARLY TERM
INDIVIDUALIZED4949


PREMATURE RUPTURE OF MEMBRANES (PROM)
OBSTETRICAL INDICATIONS
PPROM LATE PRETERM 34w 0d GESTATION
5151

Conclusion:Reasons to Eliminate Non-Medically
Indicated (Elective) Deliveries Before 39 Weeks
Reduction of neonatal complications
No harm to mother if no medical or obstetrical indication for delivery
Strong support from ACOG
Now a national quality measure for hospital performance:- National Quality Forum (NQF)
- Leapfrog Group
- The Joint Commission (TJC)5252

04/11/2304/11/23
HOW AM I GOING TO REMEMBER ALL OF THIS?
• These are guidelines. Clinical judgement and common sense should come first.
• This presentation is available online.• http://bit.ly/midb39
• There’s an app for this.http://bit.ly/midb39app OR
• http://bit.ly/midb39play
04/11/2304/11/23

http://bit.ly/midb39play

http://bit.ly/midb39app
Mecically Indicated Deliveries Before 39 weeks.There's an app for that...