Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation,...

of 17
-
Upload
nasa-bastina-tomislavgrad -
Category
Documents
-
view
213 -
download
0
Transcript of Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation,...
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
1/17
Medical Services of Croat People in Bosnia and Herzegovina during1992-1995 War: Losses, Adaptation, Organization, and Transformation
Ivan Bagari
Ministry of Health of the Federation of Bosnia and Herzegovina, Sarajevo; and Mostar University School ofMedicine, Mostar, Bosnia and Herzegovina
Duringthe1992-1995 war in Bosniaand Herzegovina (BH), Croatian peoplein BH had19,600(26%)killed and135,000 (176%) displaced persons, and 222,500 (289%) refugees They lost around two thirds of both physi-cians andotherhealthpersonnel, and were left with 85%of prewarpatient bedsFortunately, theorganized de-fence against Serbs was initiated in time and Croats defended the territories where they formed majority Thefirst defense unit established was the Medical Corps Headquarters (MCH), caring for soldiers and civiliansalike MCH was soon incorporated in the Croatian Defense Council (CDC, armed forces of Croatian people inBH)MCHhadtwochainsofcommandThefirstonewentthroughthedistrictcommandersofmedicalservicesand their subordinatedphysicians to paramedics in military units, and the other one directly to the command-ers of 14 war hospitals Afterits formation in 1993, theMinistry of Health took thejurisdictionover the civilian
medical services and after the Washington Peace Agreement (April 1994) over the war hospitals, too, whereasthe medical services within military units remained under control of the Ministry of Defense Dayton PeaceAgreement divided BH into the Federation of BH and Republic Srpska, each with their own army The Federa-tionofBHArmyiscomposedoftheCDCandBosniac-controlledArmyofBH,withoverallnumericalratio1:23forBosniacs, and organized in accordance with NATO standards Military medical services areprovidedby theLogistics Sector of both Ministry of Defense and Military Corps Headquarters (Joint Command)
Key wo rds: armed forces personnel; Bosnia and Herzegovina; Croatia; hospitals, military; military medicine; militarypersonnel; military science; military veterinary service; soldiers; war
Contrary to the expectations (1,2), in the1992-1995 war in Bosnia and Herzegovina (BH), theCroats managed to organize and defend themselvesagainst powerful Yugoslav Federal Army (YFA) Theirdefense forces were formed under the name of theCroatian Defense Council (CDC) In the beginning,the Medical Services were established in parallelwith the CDC Later they were incorporated in theCDC, but retained a great degree of independenceAfter the war both were incorporated into the BHArmy as an undivided peacetime military organiza-tion
The aim of this article is to analyze the organi-zation of Medical Services within the CDC, espe-cially with respect to its specificities imposed by
unique political and martial setting, its adaptationto wartime circumstances, and final integration intothe BH Federation system The establishment of theCDC Medical Services and the way they were orga-nized illustrate the quality, adaptability, and loyaltyof the civilian medical services, from which all thewartime medical services were formed
Organization of Military Medical Services
In many countries, military and civilian med-ical services are separated For example, USA hasa large system of health facilities (more than 300)for war veterans (3-5), that operates under the De-partment of Veterans Affairs and answers mainlyveterans service-related needs The health carefor the military is provided by the three separatemedical service corps each within the corre-
sponding military service the Army, the AirForce, and the Navy, with the medical servicecorps of the Navy caring for the Marine Corps Themilitary provides the continuum of medical care
124www.vms.hr/cmj
41(2):124-140,2000
EDITORIAL
Dr Ivan Bagari is the assistant to the Minister of Health of theFederation of Bosnia and Herzegovina (BH), in charge of health care
organization As a physician and a member of the BH Parliament, heorganized medical service forthe Croat population in BH, and becamethe first Head of the Medical Corps Headquarters of the Croatian De-fense Council in BH (1992-1996) During the war he achieved therank of Major General
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
2/17
from the primary level health care units to the ter-tiary level health care hospitals These facilitiessupport the military whether peacetime or war-time (6)
In some other countries, military and civilianhealth care services are integrated, and the numberof countries seriously considering such a type ofhealth care system organization is increasing (7,8)Israel is an example of the country with well-organized health service in which the civilian andmilitary health services are integrated (9,10) The Is-raeli medical professionals are prepared through ad-ditional education to work in war conditions (11)
Former Yugoslavia followed the model of theSoviet Union (12,13) and had a large military healthcare (14) The Republic of Croatia, which sufferedgreat material damage in the 1991-1995 war (15-17),including the intentional destruction of the healthcare facilities (18-21), starteddeveloping its militarymedical services with the beginning of the war(18,19) First, the mobile surgical teams were orga-nized (22) and the civilian health care facilities ur-gently adapted to the war circumstances (23-26)Then, the establishment of war hospitals followed(27) and, in the end, Croatia had a well-organizedand efficient health care system (28) Today, Cro-atian military medical services are integrated in the
civilian health care system (19) Similar, but in anumber of aspects also different, process took placein BH (29-35)
Within systems (states, armies) where militaryhealth care is separated from the civilian one, theformer follows hierarchical organization: from thefirst echelon where medical care is provided by amedical orderly in a platoon, to the echelon levelswhere the wounded are given subspecializedhealth care (36,37) Basically, we accepted thisscheme, but united civilian and military medicalservices (30-33) Echelon system was replaced by(an imposed!) positioning the war hospitals in thewar zones, often very close to the front line
Setting
Bosnia and Herzegovina
Before the war, BH was one of the six repub-lics of the former socialist Yugoslavia It had a con-siderable degree of autonomy, which included theright to separation, and the population of 43 mil-lion people (38) The BH population consisted ofthree nations: Muslims (recognized as a nation informer Yugoslavia; took the name Bosniacs afterthe war) (434%), Serbs (312%), and Croats(174%), all three officially equal and constitutive
125
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
1
10
6
7
8
4
3
2
95
LIVNO
BGRAHOVO
TOMISLAVGRAD
GLAMO
KUPRES
POSUJE
BRIJEG
ITLUKLJUBUKI
GRUDE
DRVAR
BIHA
APLJINANEUM
STOLAC
MOSTAR
SARAJEVO
BANJA LUKA
TUZLA
1
10
6
78
4
3
2
95
LIVNO
BGRAHOVO
TOMISLAVGRAD
POSUSJE
BIHABRKO
.EPE
VARE
JAJCE
USORA
VITEZ
KISELJAK
NTRAVNIK
BUGOJNO
KUPRESGLAMO
DRVAR
TUZLA
SARAJEVO
2
PROZOR
BANJA LUKA
STOLAC
LJUBUKI ITLUK
BRIJEG
GRUDE MOSTAR
APLJINA
NEUM
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
3/17
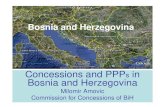
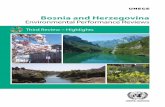
(Fig 1) Minorities and Yugoslavs accounted for79% of the population
The war in BH started in April 1992, followingthe 1991 war, which YFA started against former Yu-goslav Republics of Slovenia and Croatia In boththese conflicts, YFA in Slovenia, and YFA and Serb
paramilitary forces in Croatia, were defeated Theywithdrew to BH (wherefrom they continued to at-tack Croatia), while Slovenia and Croatia becamerecognized as independent states BH proclaimed
its independence early in 1992 This proclamationelicited the aggression of Bosnian Serb paramilitaryforces and YFA, which tried to gain control over theBH by arms In 1992, BH Croatian people and Mus-lims (Bosniacs) lost much of their territories andmanpower, but managed to hold out Having
learned from the war experience of the Republic ofCroatia during 1991, Croatian people in BH wasbetter prepared for the armed conflict and actuallyled the defense Thus, throughout the 1992, the de-
126
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Table 1.The chronology of the most important events related to the Croat population in Bosnia and Herzegovina (BH)during the 1992-1995 war (adapted from ref 41)
Date Event Comment
November 18, 1990 Multi-party elections Bosniac (Muslim), Serb, and Croat national partiesformed the government according to the votes wonat the elections
September 19, 1991 Yugoslav Army forces attacked the villageof Ravno
As a part of the aggression against Republic ofCroatia (the offensive against Dubrovnik)
November 17,1991 Announcement of the decision to establishthe Croatian Community of Herzeg-Bosnia
Facing the threat of Serbian aggression against theRepublic of Croatia and BH, representatives of Croatnation in BH, elected on November 18, 1990,founded Croatian Community of Herzeg-Bosnia as apolitical, cultural, economical, and geographicalentity within the sovereign and democratic BH
January, 25,1992 The Parliament of BH brought decision onthe referendum for sovereign and inde-
pendent BH
Bosniacs and Croats won two-thirds and were ableto proclaim a sovereign and independent BH (inrespect to the former Yugoslavia) Serbrepresentatives then left the Parliament and Serbsstarted the war
April 18, 1992 The decision to establish the Croatian De-fense Council
Founded by Croatian Community of Herzeg-Bosnia,as the supreme body of defense of Croats in BH andthe highest executive and governing body of theCroatian Community of Herzeg-Bosnia
October, 27,1992 Vance-Owen Plan on the draft of the con-stitution and map of cantonization of BH
An attempt to achieve peace by cantonization of BHSigned by Croats only
May 8/9, 1992 Fights between Croatian Defense Counciland BH Army
The clashes started as soon as January 1992, due todisagreements about the application of Vance-Owenplan and the arrival of thousands of displacedBosniacs to the area liberated by CDC
June 23, 1993 Owen-Stoltenberg Plan and map on theorganization of BH
Another attempt to achieve peace by cantonizationof BH Immediately signed by Croats, rejected by
Serbs, and reluctantly accepted by BosniacsAugust 28, 1993 Proclamation of the Croatian Republic of
Herzeg-BosniaFormed with all governing attributes, as theresponse to already proclaimed Republic Srpskaand Bosniac Assembly in Sarajevo at which BHMuslims changed their name into Bosniacs (BHCroats felt that this reflected an intention toorganize BH as a centralized state with Bosniacdominance)
March 1, 1994 The Washington Peace Agreement on thepeaceful solution of the crisis in BH
It marked the lasting armistice between Bosniacsand Croats and laid grounds for foundation of(Bosniac-Croat) Federation of BH
November 21, 1995 The Dayton Peace Agreement Representatives of Bosniacs, Serbs, and Croats, withthe assistance of international community, endedthe war, and agreed on the organization of BH as astate consisting of two entities: Federation of BH(Bosniacs and Croats) and Republic Srpska (Serbs)The Federation was further divided into 10 cantons
May, 1997 All-Croatian Assembly in Neumproclaimed Croatian Community ofHerzeg-Bosnia as a cultural association ofCroats in BH
Within the Dayton Peace Agreement, Croats wereobliged to dissolve the Croatian Republic ofHerzeg-Bosnia, but wanted to retain some form ofcultural and economical unity
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
4/17
fense was predominantly organized and led by theCDC, while Bosniacs were either included in theCDC forces or were fighting organized as TerritorialDefense Forces Rather complicated geographic dis-tribution and different interests of the three nationsin BH gradually weakened the alliance between BH
Croats and Bosniacs (Table 1) They fought togetheragainst Bosnian Serb paramilitary forces and YFAuntil early 1993, but then, forced by Serbs to onethird of the BH territory, they began fighting againsteach other These fights lasted until early 1994 Asthis conflict begun, the CDC and Territorial DefenseForces separated The war in BH ended in 1995,with Dayton (USA) Peace Agreement Two entitieswere created, the Serb-controlled Republic Srpska(49% of the territory) and the Federation of BH (51%of the territory) controlled by both Bosniac and Cro-atian people The Federation was divided into 10cantons, 5 with Bosniac and 3 with Croat peoplemajority, and 2 mixed
During the war, except losing the major part ofPosavina, Croats successfully defended other areasin BH where they formed majority, whereasBosniacs lost the entire eastern half of BH Duringthe armed conflict between Croats and Bosniacs,Croats lost some parts of the territory in centralBosnia, where they ended up in enclaves encircledby either Serb or Bosniac forces for a long period(Fig 1) (40)
Key EventsKey events related to 1992-1995 war in BH are
listed in Table 1 (41) The official date of the com-mencement of the war in BH is still a matter of contro-versy In reality, the Serbian aggression againstnon-Serb nations in BH started on September 19,
1991, with the occupation and destruction of theCroat-populated Ravno village in southeast BH (32)However, since this attack was connected with theSerbian offensive against the Dubrovnik area in theRepublic of Croatia (42), it is considered that the warin BH really started early in 1992, when BH Serbs,backed by YFA, attacked other two nations after the
January referendum on BH independence (see Table1) Croats and Bosniacs voted in favor of independ-ence and Serbs voted against it The BH Parliamentbrought the Declarationof Independencethat was fol-lowed by referendum Since they lost in the Parlia-ment, Serb representatives left and Serb paramilitaryforces, backed by YFA, attacked Croatian people andBosniacs The aggression spread over the country andthe war continued for 4 years until the Dayton PeaceAgreement signed in USA on November 21, 1995(41,43) The armed conflict between Bosniac forcesand Croats (CDC) started as sporadic small groupclashes, early in 1993 The clashes became more andmore frequent and grew to a large-scale conflict inMay 1993, which lasted until March 1, 1994, whenthe Washington Peace Agreement was signed (41) It
127
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Table 2.General data (No, %) on human suffering in Bosnia and Herzegovina during the 1992-1995 war
Nations No (%)a Killed and missingb Displacedb Refugeesb Total affectedb
Bosniacs 1898,963 (434) 138,800 (72) 602,000 (311) 640,000 (330) 1380,800 (727)
Serbs 1365,093 (312) 89,300 (65) 350,000 (254) 330,000 (235) 769,300 (564)Croats 759,906 (174) 19,600 (26) 135,000 (176) 222,500 (289) 377,100 (496)Other 353,071 (80) 10,300 (29) 83,000 (231) 57,500 (160) 150,800 (427)Total 4377,033 (1000) 248,000 (58) 1170,000 (267) 1250,000 (286) 2678,000 (612)
aBefore the war (1991)bAccording to ref 44 Percentages in brackets are with respect to the size of the entity
Table 3.Self-management units of health carea in Bosnia and Herzegovina before the war (1991) and their fate in war
LocationNo of health professionalsb No of patient bedsc
Jurisdictionafter wardTotal Physicians Total Per 1,000population
Banja Luka 3,935 849 2,696 45 SerbsBiha 1,429 286 899 34 BosniacsBosanski Brod 117 27 SerbsDoboj 2,338 513 2,783 70 SerbsKonjic 192 49 13 03 BosniacsLivno 436 86 338 41 CroatsMostar 2,313 472 1,352 42 CroatsPrijedor 1,307 302 616 24 SerbsSarajevo 9,030 2,298 5,672 67 BosniacsTrebinje 468 103 242 42 SerbsTuzla 5,524 1,305 3,349 34 BosniacsZenica 3,058 737 1,952 37 BosniacsTotal 30,147 7,027 19,912 45
aIn the communist Yugoslavia, health system was self-managed; theinstitutions were organized in units which didnot correspond to ei-
ther municipalities, districts, or institutionsb According to ref 45 The data are as of 31 December 1991, except for Mostar and Livno (1990)cAccording to ref 46 The data are for 1989dAs a result of the war, but the division has persisted after the Dayton Peace Agreement in 1995
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
5/17
must be emphasized that BH survived due to the re-sistance and survival of the Croatian people in the en-claves scattered through Central BH and Posavina(Fig 1),which functioned as a connective tissuekeep-ing the country from being taken apart
Losses
Losses during the 4-year war were huge oneach side (Table 2) Since the exact data are not yet
available due to the destruction of services, proto-cols, and archives, Table 2 offers rough estimatesprovided by Bosniacs, which have been the onlyestimates given so far (44) Nevertheless, even on
the grounds of these estimates only, the trend andextent of the catastrophe are obvious
Health Care System War-Related Damagesin Bosnia and Herzegovina
Resources
In 1991, at the time of dissipation of the formerYugoslavia (wars in Slovenia and Croatia had al-ready started), the health care services in BH were
still organized in a socialist manner specific for for-mer Yugoslavia, ie, there were self-managementunits of health care and insurance These units werefinancially independent, constituting thus centers
128
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Table 4. Territorial distribution of hospitals and other health care institutions in parts of Bosnia and Herzegovina with Croatmajority before the war, number of inhabitants for which they cared until the war, and hospitals to which they referred thepatients
Town Largest healthinstitutiona No of healthcare workersb Population under carec Referring hospital
Total CroatsJajce MC 367 45,007 15,811 JajceBosanski Brod HCa 117 34,138 13,993 DobojDerventa HC 296 56,489 21,951 DobojOd.ak HC 78 30,056 16,338 DobojOraje HC 76 28,367 21,308 DobojDoboj Regional HC 1,255 102,549 13,264 DobojKonjic HC 193 43,878 11,513 MostarTomislavgrad HC 87 30,009 25,976 LivnoLivno MC 274 40,600 29,324 Livnoapljina HC 103 27,882 14,969 Mostaritluk HC 49 15,083 14,823 MostarGrude HC 87 16,358 16,210 Mostar
Jablanica HC 54 12,691 2,291 Mostariroki Brijeg HC 68 27,160 26,884 MostarLjubuki HC 73 28,340 26,127 MostarMostar Regional MC 1,528 126,628 43,037 MostarNeum HC 20 4,325 3,792 MostarPosuje HC 70 17,134 16,963 MostarProzor (Rama) HC 56 19,760 12,259 MostarStolac HC 104 18,681 6,188 MostarFojnica HC 170 16,296 6,623 SarajevoKiseljak HC 99 24,164 12,550 SarajevoKreevo HC 24 6,731 4,714 SarajevoVare HC 111 22,203 9,016 SarajevoSarajevo University MC 4,200 527,049 34,873 SarajevoBosanski amac HC 134 32,960 14,731 BrkoBrko MC 513 87,627 22,252 BrkoTuzla University MC 2,148 131,618 20,398 TuzlaBugojno HC 163 46,889 16,031 TravnikBusovaa HC 41 18,878 9,093 TravnikKakanj HC 160 55,950 16,556 ZenicaKupres HC 28 9,618 3,813 TravnikNovi Travnik HC 100 30,713 12,162 TravnikTravnik MC 600 70,747 26,118 TravnikVitez HC 71 27,859 12,675 TravnikUskoplje (G Vakuf) HC 59 57,164 10,706 TravnikZenica Regional MC 1,490 145,517 22,510 Zenica.epe HC 59 22,966 9,100 ZenicaBanja Luka University MC 2,318 195,692 29,026 Banja Luka
aHealth Center (HC) health careinstitutionwithoutpatient specialist services MedicalCenter (MC) health careinstitutionwithspecialistpatient bedsbTotal number of the health workers in the town, dentists not included According to refs 45 and 47 Data are for 1991cAccording to ref 38 Data are for 1991
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
6/17
of power that determined the organization and way
of financing of the area they covered (Table 3)There were 45 patient beds per 1,000 inhabitantson average, but their distribution was relatively un-even (from 03 in Konjic to 70 in Doboj), with re-mote rural areas faring the worst (45) The distribu-tion of physicians was just as uneven (Table 3)
During 1992, Croatian people in BH andBosniacs used the same health facilities, but withthe development of Croat-Bosniac conflict (early1993) only a small fraction of human and materialresources remained under Croat control a gen-eral hospital in Livno and less than a half of Mostarhealth care staff, which made about 85% of the to-tal patient beds in BH (Table 3) Such a situation
continued after the war, with lasting political divi-sion of the country and separate canton jurisdic-tion
Table 4 shows basic data on health care re-sources in the areas with considerable proportionof Croatian people in the local population Whenneeded, people living in these areas were referredto the nearest medical center With the war devel-opments, only those with access to Mostar andLivno hospitals had the opportunity to receive sec-ondary medical care
Since the very beginning of the war (April1992), Sarajevo, the capital of BH and the seat of
central administration, had been cut off from therest of the country, and the periphery was left with-out any material and financial supplies or guidanceMoreover, the martial developments brought anumber of areas and groups of people (eg, Croatianpeople in Central Bosnia, see Fig 1) under militarysiege, isolating them and preventing any help andassistance from their allies For example, Mostarstayed under Serb siege for six months in 1992 and,until it was liberated by Croat and Bosniac forcesunited under CDC, its medical services were acces-sible to its inhabitants only Also, at that time of thewar, the assistance from international humanitarianorganizations was relatively small
PhysiciansThe prewar distribution of specialists in the
surgical fields of medicine, extremely important inwar situation, in different BH regions is shown in
Table 5 During the war, almost all of these areas
came under heavy military attacks and/or siegeThis caused migrations of the people and a corre-sponding the migration of health personnel (Table6) Approximately two thirds of physicians andother health professionals left their domicile insti-tutions during the war (Table 6) The consequenceof this was that, for example, Croat populationcould receive medical specialist services only inMostar and, to a smaller extent, in Livno Mostarwas left with less than a half of its prewar person-nel, eg, only one out of 14 pre-war anesthesiolo-gists stayed in the hospital (Table 6) Some areaslisted in Table 6 were lost in the war to either Serbs(Bosanski Brod, Jajce, Derventa, and Brko) or
Bosniacs (Jablanica, Bugojno, Kakanj, Zenica, andKonjic) In the case of Bosanski amac area, its big-ger part was lost to Serb forces, but in a small zonethat was successfully defended, DomaljevacHealth Center was established The same was doneafter losing Brko Brko Ravne Health Centerwas formed in the defended part of the Brko areaIt should be emphasized that, in the beginning ofthe war, Croat and Bosniac forces, as the CDCforces, jointly defended the areas with Croat andBosniac majority This explains why it was the CDCthat organized war hospitals in the locations listedin Table 5 at that phase of the war During the1993-1994 conflict with Bosniacs, Fojnica and
Vare came under Bosniac control After losingVare, the CDC instituted a health center in the vil-lage of Datansko, and did the same after losingFojnica, moving its medical services to a nearby vil-lage When Travnik was lost to Bosniac forces, partof its medical services moved to Nova Bila Anotherexample is the town of Kupres with its surround-ings, which was lost to Serb forces early in 1992,and regained in 1995 All these war events influ-enced the number of physicians who remained inthose areas after the war, especially as the controlover the territories imposed in the war still persists
Health personnel were also injured or killed attheir workplace (Table 7)
There were three sources of assistance to Croatmedical personnel in BH (Table 8): volunteers fromthe Republic of Croatia, volunteers from other coun-tries, and personnel of Croat nationality displaced
129
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Table 5. Regional distribution of physicians specialists in Bosniaand Herzegovina before the wara
Location
No of physicians specialists
Surgery Anesthe-siology Transfu-siology Gyneco-logy Othersurgical
Pathology,
forensicmedicine
Neurology,
psychiatry,physiatry Publichealth Total
Banja Luka 66 17 6 66 38 2 72 19 286Biha 17 4 1 12 6 2 10 5 57Doboj 23 4 5 19 21 1 31 12 118Foa 7 2 1 12 6 7 5 40Mostar 40 14 5 38 25 2 39 18 181Sarajevo 148 51 9 100 127 12 188 88 723Tuzla 70 18 7 74 50 1 46 88 354Zenica 49 10 5 41 28 1 36 18 188Total 420 120 39 362 301 21 429 253 1,945
aOnly specialties important for war-related medicine are presented According to ref 45
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
7/17
from other parts of BH to Croat-controlled territo-ries The numbers given in Table 8 apply to person-
nel who were within the CDC Medical Corps fromthe start of the war until the Washington PeaceAgreement (April 1994) Since then, within the pro-gram of humanitarian assistance, approximately
1,000 physicians from Croatia came to assist theircolleagues in BH for a shorter or longer period Theymostly came as organized medical teams
Loss of manpower in health care was not acharacteristic of the areas with the Croat majorityonly Major demographic changes within healthpersonnel occurred in all parts of BH (Table 9)
Hospitals
Before the war, the BH medical institutions pro-viding secondary and tertiary medical care wereuniversity hospitals, regional medical centers, andlocal medical centers (Table 10) Primary care was
provided by health centers in each municipalityThe difference between medical centers and healthcenters was that the former had specialists and pa-tient beds, whereas health centers offered outpa-tient services only The institutions listed in Table10, which represent most of the countrys capaci-ties, had a total of 15,159 beds and 2,435 physiciansAs the only health institutions that remained underCroat control, in Livno and Mostar, were in thesouth of the country (Table 10), the Croats thatended up encircled in enclaves in central northernBH (Fig 1) when the Croat-Bosniac armed conflictstarted in 1993, were left without secondary and ter-tiary levels of health care
Damage or destruction of the medical institu-tions caused further losses to the health care sys-tem In the areas with Croat majority, only 4 out of35 institutions did not suffer any damage (Table
130
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Table 6. Number of physicians and other medical personnelin areas with Croat majority, before and after the war inBosniaand Hercegovinaa
Location
No of personnel
Before war After warPhysicians Other Physicians Other
Jajce 79 288 4 15Bosanski Brod 27 90 bDerventa 74 222 bOd.ak 24 54 3 85Tomislavgrad 17 70 16 154Livno 56 218 46 151apljina 25 76 15 46itluk 9 40 8 42Grude 19 68 11 61
Jablanica 14 40 cLjubuki 16 57 16 51Mostar 312 1,216 243 685Neum 4 16 6 14Posuje 14 56 7 56Prozor 11 45 7 23Stolac 19 85 8 24iroki Brijeg 17 51 15 58Fojnica 37 133 1 11dKiseljak 27 72 25 83Kreevo 6 18 4 25Vare 26 85 4 13dBrko (Ravne) 141 372 10 40Bosanski amac
(Domaljevac)39 95 1 5b
Oraje 21 56 29 73Bugojno 44 119 cBusovaa 11 30 7 34Kakanj 44 116 cKupres 7 21 2 7Novi Travnik 25 75 12 37Travnik 137 463 18 74eVitez 18 53 10 41.epe 14 45 8 68Zenica 358 1,132 cUskoplje 18 41 10 30Konjic 49 135 cUsora 3 15Total 1,759 5,773 549 2,021
aThedata areforthemunicipalities of theformer Croatian Republicof Herzeg-Bosnia in Bosnia and Herzegovina,with Croatmajority Theprewar data are according toref45, as of31December 1991, except for
Mostar and Livno (1990) The postwar data are according to ref 48Physicians include all physicians in the area Other include dentists,pharmacists, and auxiliary medical personnelbLost to Serbian control In the case of Bosanski amac, theHealth Center Domaljevac was established in the small areathat remained under our control (7,000 inhabitants)cLost to Bosniaccontrol either by military force (eg, Bugojno)orpolitical division (eg, Zenica)dCDC hospital was lost to Bosniac forces, and we were left withonly one medical office located in a small village that remainedunder the CDC controleAfter Travnik was lost to Bosniac forces, the hospital in NovaBila was reactivated
Table 7. Casualties among the personnel of the CroatianDefense Council Military Medical Service duringthe1992-1995 war in Bosnia and Herzegovinaa
Health professionalsbNo of casualties
Wounded Killed TotalPhysicians(300-360) 13 3 16Nurses and technicians(1,000-1,200)
97 16 123
Ambulancedrivers(280-300)
85 19 104
aData on casualties of soldiers educated to serve as paramedics arenot known because they were registered among soldier casualtiesbNumbers in brackets are estimates because a formal census ofthe health professionals was not done, and their number variedduring the war
Table 8. Assistance to medical personnelin theCroatian
Defense Council Military Medical Service duringthe1992-1995 war in Bosnia and Herzegovina (BH)a
Origin of the personnel Physicians Nurses andtechniciansVolunteers from the
Republic of Croatia25 67
Volunteers from otherforeign countries
6 23
Personnel from other partsof BH
45 77
aOnlythe personnel working permanently for the Corps; temporaryvolunteers (some of them coming and leaving several times) werenot included
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
8/17
11) The extent of destruction varied, but 5 institu-
tions were destroyed to the ground As describedearlier, some of the institutions (Travnik, .epe,Oraje, Brko, and Usora) were what remained ofthe institutions organized and held by the CDC at
the beginning of the war; during the war, these ar-eas were lost and medical services were then orga-nized in the neighboring locations which werestill under Croat control After the war, these insti-tutions became either health centers (Nova Bila,Datansko, Ravne Brko) or general hospitals (Ora-je, which replaced the CDC Tolisa war hospital)The case of Usora is especially interesting: beforethe war, this location did not have its own medicalservice During the war, it became the onlyCroat-controlled part of Teanj and Tesli area,where the medical service was organized for theneeds of the local population under siege Theseinstitutions continued to work after the war
The war caused considerable number of peopleto migrate (Table 11) The number of Croats de-creased 353% from 784,176 in 1991 (before thewar) to 507,007 in 1996 However, this did not easethe burden the health care system had to carry be-cause the needs increased: large numbers of injured
and psychically traumatized soldiers and civiliansdemanded organization of medical services in areaswithout adequate health care institutions (Table 12)These needs were met by the war hospitals institu-
131
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Table 9.Number of physicians in 10 cantons of Bosniaand Herzegovina before (1991) and after the war (1995)a
No of health care personnel
Year Physiciansb DentistsPharma-cists Techni-cians Total
Canton 1: Unsko-Sanski1991 377 (162) 86 33 1,248 1,7441995 168 (80) 23 14 797 1,002Diff -209 (-82) -63 -19 -451 -742Canton 2: Posavski1991 35 (9) 11 4 104 1541995 21 (10) 5 5 43 74Diff -14 (1) -6 1 -61 -80Canton 3: Tuzla-Podrinje1991 799 (394) 115 90 2,304 3,3081995 688 (330) 60 50 2,083 2,881
Diff -111 (-64) -55 -40 -221 -427Canton 4: Zenica-Doboj1991 632 (310) 130 73 1,703 2,5381995 317 (192) 66 49 1,642 2,074Diff -315 (-118) -64 -24 -61 -64Canton 5: Gora.de1991 47 (24) 13 7 126 1931995 22 (3) 3 0 66 91Diff -25 (-21) -10 -7 -60 -102Canton 6: Central Bosnia1991 418 (212) 65 49 1,224 1,7561995 224 (119) 33 16 959 1,232Diff -194 (-93) -32 -33 -265 -524Canton 7: Neretva-Herzegovina1991 443 (278) 100 78 1,477 2,0981995 300 (159) 53 13 980 1,346Diff -143 (-119) -47 -65 -497 -752Canton 8: West Herzegovina1991 66 (18) 33 1 198 2981995 49 (24) 19 3 203 274Diff -17 (4) -14 2 5 -24Canton 9: Sarajevo1991 1,799 (1,299) 342 170 4,408 6,7191995 955 (639) 175 103 2,146 3,379Diff -844 (-660) -167 -67 -2,262 -3,340Canton 10: Herzeg-Bosnia1991 137 (54) 39 22 434 632
1995 65 (35) 12 2 236 315Diff -72 (-19) -27 -20 -198 -317Total: Federation of Bosnia and Herzegovina1991 4,753 (2,760) 934 527 13,226 19,4401995 2,809 (1,591) 449 255 9,155 12,668Diff -1,944 (-1,169) -485 -272 -4,071 -6,772aPrewar data are from ref 45, and post-war data from refs 47 and48bTotal number of physicians; number in brackets shows thenumber of specialists
Table 10. University and regional health care institutions inBosnia and Herzegovina before the war, and their fate in thewara
Location No of
physicians No of beds Jurisdiction
after warb
University Medical Centerc
Sarajevo 913 4,256 BosniacsTuzla 317 1,519 BosniacsBanja Luka 249 1,586 Serbs
Regional Medical Centerd
Biha 93 825 BosniacsDoboj 131 998 SerbsMostar 145 914 CroatsFoa 44 412 SerbsZenica 158 1,047 Bosniacs
Local Medical Centere
BosanskaGradika
22 245 Serbs
Jajce 22 170 SerbsPrijedor 60 452 SerbsDrvar 13 200 SerbsDerventa 19 408 SerbsLivno 33 338 CroatsTrebinje 30 217 SerbsBijeljina 32 296 SerbsBrko 54 488 SerbsZvornik 37 273 SerbsTravnik 63 515 Bosniacs
Total 2,435 15,159aData according to ref 45, as of 30 December 1991, except forMostar andLivno(1990) Physicians andbeds from primary healthcare (HC, special hospitals, rehabilitation centers) are not counted
inbAs a result of the war, but the division has persisted after theDayton Peace Agreement in 1995cLarge institutions with medical school teaching facilities and per-sonneldInstitutions with special hospital bedseInstitutions with outpatient specialist services
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
9/17
tions established by the Medical Corps Headquar-ters of the CDC, which received the wounded fromthe most active battlefields Various buildings of dif-
ferent sizes and prewar functions were transformedinto the war hospitals 14 in total (Table 13) Theyprovided secondary and tertiary health care for themilitary as well as for the civilian population (seebelow) In the beginning of the war, and before theconflict with Bosniacs, all these hospitals were orga-nized by the CDC and served local inhabitants andsoldiers regardless of their nationality During theconflict with Bosniacs, Jablanica, Bugojno, Fojnica,and Kostajnica (near Konjic) came completely un-der the Bosniac control, except for the Fojnica warhospital, which was transferred to Kiseljak
Organization of the Croatian DefenseCouncil Medical Services
The development, adaptations, and transforma-tions of the CDC Medical Services corresponded to
those that went on in the CDC military part: from asimple organization of the people by themselves,followed by amateur forms of organization, and fi-
nally to a relatively well organized armyThe Beginning
Croat population in BH was the first to face theSerbian aggression in 1992 The data in Tables 2-11illustrate the (rather sudden) loss of resources,which was worsened by a lack of any experience oreducation in war medicine When the war brokeout, a group of physicians, who were all members ofthe BH Parliament, too, started a systematic plan-ning of the concept of medical care for the oncom-ing catastrophe They used the war experience ofthe Croatian health care and were helped by thephysicians from Croatia, mostly those who were of
BH origin I was one of the physicians from the BHParliament who initiated the establishment of theMilitary Medical Headquarters, by the end of March1992, just before the open Serbian aggression Ser-
132
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Table 11. Health care institutions withinthe political territorial areas of Bosnia and Herzegovina under Croat jurisdiction;situation after the war (1996)
Location Categorya
Area (m2) and
percent (%) ofdestructionbNo of
physicianscPopulation
1991d
Population 1996b
(% differenceto 1991)Grude HC 2,010 (38) 11 16,358 19,635 (+203)Ljubuki HC 1,950 (24) 16 28,340 32,636 (+156)Posuje HC 1,000 (0) 7 17,134 19,183 (+119)iroki Brijeg HC 1,860 (0) 15 27,180 3,100 (+148)apljina HC 3,250 (14) 15 72,882 28,000 (-615)itluk HC 2,100 (0) 8 15,083 20,239 (+341)Mostar HC+UH 3,302 (99) 243 126,626 49,914 (-605)Neum HC 1,008 (69) 6 4,325 6,882 (+591)Rama HC 1,400 (71) 7 19,760 12,350 (-375)Stolac HC 2,000 (65) 8 18,681 10,000 (-464)Kreevo HC 432 (27) 4 6,731 6,426 (-45)Fojnica HC 250 (64) 1 16,298 2,500 (-84)Kiseljake HC 860 (19) 25 24,164 20,396 (-155)
Busovaa HC 550 (34) 7 18,897 11,081 (-413)Vitez HC 1,450 (32) 10 27,859 17,155 (-384)Novi Travnik HC 1,650 (26) 12 30,713 10,000 (-674)Travnike HC Nova Bilaf 700 (59) 18 6,000Uskoplje HC 350 (100) 10 25,181 7,645 (-696)
Jajce HC 1,900 (30) 4 45,007 12,810 (-715)Vare HC Datansko 250 (100) 4 22,203 2,500 (-887).epee HC 1,100 (60) 8 22,066 20,000 (-93)B Grahovo HC 1,850 (12) 1 8,311 500 (-93)Glamo HC 2,400 (98) 1 12,593 3,000 (-761)Drvar HC 2,500 (29) 17,126 3,000 (-824)Kupres HC 1,450 (72) 2 9,618 3,813 (-603)Livno HC+GH 1,900 (13) 46 40,600 34,000 (-162)Tomislavgrad HC 2,300 (0) 16 30,009 32,284 (+75)Od.ak HC 2,500 (80) 3 30,056 4,000 (-866)
Orajee GH 1,660 (95) 29 28,376 24,082 (-151)Ravne Brko HC 950 (37) 7 22,000 17,236 (-216)Usoraf HC 600 (40) 3 11,400
Total 51,020 547 784,176 507,007 (-353)
aHC Health Center (outpatient facilities only), GH General Hospital, UH University HospitalbAccording to the official estimates of the Intercounty Institute for Public Health, Mostar 1997cAccording to refs 47 and 48dAccording to ref 38eLocations of war hospitals, that were transformed into civilian institutions after the warfDid not exist before the war, but were created during the war due to isolation of the area
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
10/17
bian occupation and destruction of the Croat-popu-lated Ravno village in the southeast of BH occurredas early as September 1991, and it was obvious thatthe aggression would spread over the whole countryin no time
We toured the areas populated by Croats, listedall the health centers, and prompted their adapta-tion to the situations of emergency in which therewould be a large number of the wounded Strategicpoints for the war surgery units future war hospi-tals were determined Health care institutionswere connected by a computer network and packetradio connection (49), which soon proved ex-tremely important since many of the war hospitalsbecame isolated and this technology was the onlymeans of communication for a long time War expe-rience of the Republic of Croatia (where the war
started in May 1991) was kept in mind: the conceptof Medical Corps Headquarters was adopted (19), butmobile surgical teams (22) were not organized in BHbecause we had neither surgical clinics nor suffi-cient number of surgery specialists Thus, we optedto use primary health care institutions with what-ever personnel they had The Croatian model ofcomputer network, which helped Croats immenselyduring the evacuation of the Vukovar hospital inNovember 1991 (49), was used in its entirety Laterit proved crucial for commanding and coordinatingmedical activities Since there were no military for-mations, we asked the heads of health institutions tobe in charge of preparing municipal medical ser-vices for a war situation This reflected the futurestructure and organization of the MCH, ie, Munici-pal Medical Service Headquarters were establishedin each municipality where it was possible Mosthealth institutions had already started building upthe reserves of drugs and medical material for futureneeds related to emergency situations
These preparations were done in time We rec-ognized the danger for Croat population to be leftwithout any larger medical institution and with in-sufficient medical personnel in case of war Ourstrong belief that the war was imminent stemmedfrom the political developments in the BH Parlia-
ment, and the knowledge about the tragic experi-ence of our colleagues from the Republic of Croatiain 1991 war (27,50-52) was precious to us Welearned a lot from contacts with the health person-nel who worked in the neighboring parts of Croatiaand with whom we had always cooperated sincelarge areas of northern and southern BH relied onthe secondary and tertiary health care services inCroatia in former Yugoslavia
The overall result of our activities was the es-tablishment of the Medical Corps Headquarters(MCH) of the BH Croat population on March 12,1992, which makes it the oldest defense unit in the
entire BH Not much later, the Croatian DefenseCouncil (CDC) was formed as a civilian and militaryorganization in charge of defense of the Croat-populated areas from Serbian aggression (53)
133
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Table 12.Medical institutions and other buildings in areaswith Croatian majority, transformed into warhospitalsat thebeginning of the war in Bosnia and Herzegovina
Location Previousfunction of thebuilding BeginningofworkTomislavgrad health centera 1992Livno medical centerb 1992
Sturba anti-atom bombshelter
1992
Mostar newhospital underconstruction and surgerywardc
1992
Grude tobacco repository 1992Neum Sunce Hotel 1992
Jablanica health centerd 1992Rama floppy disc factory 1992Gornji Vakuf Franciscan rectory 1993
Jajce city hospital 1992
Bugojno Kalin Hoteld
1992Kiseljak health center 1993Fojnica rehabilitation centerd 1992Nova Bila church 1992Busovaa health center 1993.epe primary school 1992Bosanska Bijela primary school 1993Oraje Tolisa Franciscan rectory 1992Kostajnica private housed 1993
aHealth care institution with outpatient specialist servicesbHealth care institution with specialist patient bedscNewhospitalwasunder construction; old hospitalwaspartly de-stroyedatthebeginningofwar, andonlythe surgeryward wasuseddEstablished by the CDC Medical Corps Headquarters, but lost insubsequent war operations
Table 13. War hospitals of the Croatian Defense Council onterritories with Croat majority in Bosniaand Herzegovina,with numbers of workersa, hospital bedsb, and inhabitantscfor which they cared
Location No ofphysici-
ans
No of otherhealth care
workers
No ofbeds
Populationunder care
Tomislavgrad 10 56 40 30,000Livno 12 64 60 40,000Rama 14 35 40 20,000Grude 7 30 15 30,000Mostar 32 120 200 80,000
Tolisa 11 30 35 30,000.epe 8 18 40 25,000Fojnica 9 35 60 35,000Kiseljak 25 67 56 25,000Bos Bijela 5 18 30 20,000Nova Bila 10 54 50 50,000Bugojno 15 42 30 46,000
Jajce 10 32 40 45,000Uskoplje 10 30 10 27,000
aThe numbers include only personnel working in war hospitals,which were eitherthe only healthcare institution in theregion ora part of the existing civilian health institution Other health per-sonnel worked in HealthCenters, civilian parts of local healthin-stitutions, or battlefield in medical unitsbThenumber of beds in war hospitals; those were emergencybeds,from which the wounded either returned to theunit or were sent toanother health institution for final treatmentcThe population changed greatly according to the war situation many left thearea and refugeessettled in Thenumbers in thetableare estimates of an average population during the war
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
11/17
134
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Growth of the Croatian Defense Council
The establishment of the CDC was immedi-ately followed by the organization of military
units These units were organized on a territorialprinciple soldier volunteers were assigned tounits defending their homes The MCH joined theCDC and with the CDC Headquarters became thekey leading factor in the defense of the BH Croatand all other populations in the areas it covered
It should be emphasized that neither the CDCHeadquarters nor MCH had emerged as a continu-ation of an organization of the former YFA and hadnot taken over their doctrine either The number ofofficers of the Croat nationality in the prewar YFAwas insignificant and there was nobody of suchprofile to contact or learn from Besides, with the1991 wars in Slovenia and Croatia, the YFA be-
came completely Serb-controlled Since the MCHand CDC Headquarters were organized independ-ently from each other, the MCH did not become aformal part of the CDC Military Headquarters; thetwo bodies cooperated closely, but, within theCDC, they were on the same hierarchical level(Fig 2), which is probably a unique case in mili-tary medicine
The MCH had 4 departments (Fig 2): 1) Pre-ventive medical care, veterinary services and med-ical supplies; 2) War hospitals; 3) Echelon medicalservices; and 4) Informatics This scheme was es-tablished before the actual organization of the mil-itary units and formal establishment of CDC (April
1992) and Military Headquarters (May 1992) Ech-elon Medical Services took care of the woundeduntil they would reach a hospital with tertiarymedical care Municipal military commands in-cluded municipal heads of medical services as as-sistants to the military commanders in the DistrictMilitary Headquarters In the field, the ArmedForces Headquarters had the military commandersof the municipalities under command, and thesemilitary commanders had the heads of the head-quarters of the municipal military medical ser-vices as assistants (Fig 3) Military medical ser-vices encompassed physicians in military units(brigades and battalions), medical technicians,
and finally paramedics in companies, platoons,and squads The chain of command of the medicalservices went from the MCH, to the municipalheads of medical services, to brigade physicians,to battalion physicians, to medical technicians,and to paramedics Another vertical chain of com-mand went directly from MCH to the commandersof war hospitals (Fig 3)
Figure 4 depicts changes in the structure ofMCH As of October 14, 1992, the MCH becameintegrated into the CDC Department of Defenseand became its Health Care Sector To increasecommand efficacy, the commands of field medicalunits and war hospitals were integrated at the
level of the Department of Operative Medical Ser-vice of the Health Care Sector This Service wassimilar to an echelon medical care system, withthe difference that it did not have a proper eche-
Croatian Defense Council
Medical Headquarters Military Headquarters
Departmentof War
Hospitals
Departmentof
Informatics
Departmentof Preventive
Medicine,Veterinary
Medicine, andSupplies
District MilitaryHeadquarters
Department ofOperativeMedicalService
echelons)(
Figure 2 Hierarchical structure of the Military MedicalCorps of the Croatian Defense Council (CDC) in the Cro-atian Community of Herzeg-Bosnia (CC H-B) from the be-ginning of the war in Bosnia and Herzegovina until Octo-ber 1992
Medical DistrictCommander
Commander ofWar Hospital
Military DistrictCommander
Brigade Head Physician
Medical technicians
CDC Military Headquarters CDC Medical Headquarters
Paramedics in thecompany, platoon,squad
Battalion physicians
Figure 3 Commanding line in the Military Medical Corpsof the Croatian Defense Council (CDC) in the CroatianCommunity of Herzeg-Bosnia (CC H-B) from the begin-ning of the war in Bosnia and Herzegovina until October1992
Department of Defense
Health Care Sector
Department for OperativeMedical Service(Echelons
Medical Service)
Control and InspectionService Medical Logistics
War HospitalOperative
zone MedicalUnit
BrigadeMedical Unit
BattalionMedical
Team
Infectious disease,Epidemiology
and Toxicology
Informatics andInvestigation
Medical Supplies
Missing Soldiers
Administration
War Psychology
Dental Medicine
WarSurgery/Logistics
Figure 4 Structure of the Croatian Defense Council mili-tary medicalservicefromOctober1992 until August 1993
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
12/17
lon organization Commander of the OperativeMedical Service was a surgeon, who receivedcommands from the Health Care Sector Head-quarters, and was directly superior to the com-
manders of operative medical units Commandersof the brigade medical corps were responsible forthe physicians in battalions, and the downwardchain of command remained as before Althoughthe commander of the Operative Medical Servicewas technically a superior officer to the com-manders of the War hospitals, these hospitals hada special position, which will be described later
Due to the growth of the system, a Control andInspection Service was formed and headed by aspecialist in occupational medicine
Operative Medical Sector Service and Controland Inspection Service were the operative part ofthe Health Care Sector, whereas Medical LogisticsService provided logistics to their work, as well ashealth care other than direct treatment of thewounded in the field, such as epidemiological ser-vice, dental medicine, psychology, and psychiatry(Fig 4)
Formation of the Ministries
On the basis of war experiences in 1992, theCDC and Health Care Sector underwent anothermajor reform in August 1993 (Fig 5) With the for-mation of the Ministry of Health, standard civilianmedical services and their organization in the ar-eas that were not affected by war became the re-sponsibility of the Ministry of Health MCH was
assigned the jurisdiction over the military medicalservices only Civilian and military medicine hadnever been completely separated but their organi-zation and functioning were adapted to the local
situations Basically, all medical institutions andpersonnel in the given area in the war zones, in-cluding the war hospitals and medical personnelserving in military units, were obliged to assist
both military and civilian populations and were incharge of the entire medical care of the area Withthis reform, civilian medical institutions in the ar-eas unaffected by war came under the jurisdictionof the newly formed Ministry of Health At thattime, MCH had 3 departments: 1) Department ofPreventive Medical Care and Supplies, with theEpidemiological Division, Division for VeterinaryMedicine, and Division for Medical Supplies; 2)Department of Specialist Medicine, with Divisionsfor War Hospitals (War Surgery), Psychology andPsychiatry, Dentistry, and Physical Health Assess-ment; 3) Department of Education and MedicalDocumentation, with Divisions for Education and
Analysis, and for Communications, Acquisitionand Archiving of Information
After the CDC forces liberated Mostar from theSerbian occupation in August 1992, most of theHealth Care Sector moved to this city Only a smallpart of it remained in Tomislavgrad, the town atthe crossroads of communication routes definedby military developments (see Fig 1) This loca-tion rendered optimal communications with thefield units and institutions and served the unitsand war hospitals in the central and northwest BH
The Head of the Health Care Sector was firststationed at the Ministry of Defense, located in
Mostar, but soon moved to the premises of theHealth Care Sector at the Mostar War Hospital(from March 1993 until the Vienna Peace Agree-ment in March 1994)
135
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Ministry of Health Ministry of Defense
Health Care Sector
Department ofPreventiveMedicine
Departmentof Specialist
Medicine
Department ofEducation andDocumentation
Medical Assistantto District
Commander
Epidemiology DentalMedicine
Medical Assistantto BrigadeCommander
Supplies War Hospitals Medical Assistant toBattalion Commander
War Psychologyand Psychiatry
Physical HealthAssessment
District MilitaryCommander
Assistant to the Minister
of Defense
Data Analysis
Communication
and Archiving
VeterinaryMedicine
HeadquartersCDC Military
Figure 5.Structure of the Croatian Defense Council military medical service from August 1993 until the end of the war inBosnia and Herzegovina
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
13/17
Hierarchically, Health Care Sector was undercommand of the Ministry of Defense and the Headof the Military Medical Services served as an Assis-tant to the Minister of Defense He also collaboratedwith the Ministry of Health (Fig 5) The samescheme was applied to all commanding instances:all medical commanders in military units were as-sistants to the military commanders of the respec-tive unit However, war hospitals, regardless of theirlocations, were completely autonomous from theboth the military and civilian commanding chainThey also had a high degree of freedom within theHealth Care Sector For example, the Head of theHealth Care Sector appointed their commanders,but their connection with the Sectors Departmentfor War Hospitals was primarily a logistical and nota commanding one The Chief Surgeon from theHealth Care Sector (previously the Commander of
the Operative Medical Service), who headed the De-partment forWar Hospitals, controlled the quality ofmedical work, but in decision-making respect, warhospitals were quite autonomous This featurestemmed from the way in which they were estab-lished and high professionalism of their personnel,but also from the fact that many of them ended up inencircled enclaves, having only computer packet ra-dios as the means of communication with theHealth Care Sector Thus, the Sectors strategy to-ward war hospitals was freedom in initiative andcommanding and taking full responsibility for thework It should be emphasized that a military com-mander never entered any war hospital and issued a
command
After Washington Peace Agreement
After the Washington Peace Agreement be-tween Bosniacs and Croats in April 1994, as a con-sequence of cessation of hostilities and a sign ofgood will, the Head of the Health Care Sector sug-gested to the Minister of Defense to transfer the ju-risdiction over all war hospitals to the Ministry ofHealth, except those in Oraje and Bosanska Bijela(Posavina, north-east BH), where the war with Serbscontinued From that time on, the personnel of theHealth Care Sector were considerably reduced andHealth Care Sector became one of the administra-tion departments of the Ministry of Defense, headedby the Head for Health Administration
Several war hospitals were reactivated in 1995,when BH Army (Bosniac armed forces), CDC, andArmy of the Republic of Croatia jointly undertookseveral offensives to liberate west BH from Serb oc-cupation For example, during the battles for the lib-eration of Kupres and other southwest parts of BH(west of Livno to Grahovo, see Fig 1), war hospitalsin Rama, Tomislavgrad, and Livno were reactivatedwithin several hours Immediately after the libera-tion of Kupres, 4 days after the commencement ofoffensive, Kupres War Hospital was formed by com-
bining the personnel and equipment from other 3war hospitals, to serve the armed forces in their fur-ther military advancements Soon, the same hap-pened in Jajce after it was liberated (see Fig 1)
Military Medical Service
Medical Services in Militar y FormationsIn the beginning of 1992, when the defense
was organized on the municipal level, the munici-pal military formations relied on local health cen-ters for medical personnel and supplies Whenneeded, local military formations included physi-cians and other medical personnel as ordered bythe municipal head of medical services (director ofthe health center in most cases) These local for-mations had from several hundred to 1,500 men;two medical teams took care of 500 soldiers Eachteam consisted of a physician, two medical techni-cians, and two ambulance drivers Selected sol-diers were trained in first aid and resuscitation,and then assigned as paramedics to every platoon
With the formation of the brigades, brigade
medical service commanders were appointed, andthe function of the municipal head of medical ser-vices was abolished Commanders of the brigademedical service took care of the personnel in bat-talions and companies Each battalion had a physi-cian, 2 medical technicians, and 2 ambulancedrivers There was a medical technician on eachcompany and a paramedic for every 10 soldiers
Subsequent reorganization of military forma-tions included the formation of operative zones,with their medical service commanders in chargeof medical service of all brigades constituting theoperative zone They relied upon all medical insti-tutions in the area and the closest war hospital
In the military conflict with the Serb forces,there was a regular front-line because the YFA pre-ferred classical warfare, with artillery, armored ve-hicles, and infantry The rear was shelled, and airforces were used in attacks at the beginning of thewar This allowed us to position physicians veryclose to the front-line, where they could help thewounded much quicker and send them by shortevacuation routes to a brigade medical station,where basic resuscitation measures were under-taken (hemostasis, inspection of airways, place-ment of iv line) (32) These medical stations werepositioned from few hundred meters to at most 2km away from the front-line, and all the wounded
would reach them within an hour after injury Af-ter that, a patient would be transported to a warhospital All routes of evacuation were relativelysafe, aside from artillery attacks In contrast,mostly city fights, often head-to-head, character-ized the conflict with Bosniacs, and echelon prin-ciple was inapplicable Instead, the woundedwould be taken directly to the nearby war hospitalThey were very close to most of the places of fight-ing , anyway
War HospitalsAll CDC war hospitals were located in build-
ings Almost all were within the zone of the active
fighting, and some were on the very front-line in thecities, especially during the armed conflict withBosniacs The closeness of the front-line was thereason that the CDC, in distinction from many other
136
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
14/17
armies, including that in Croatia, neither needednor could use mobile surgical teams or field hospi-tals This was probably the most specific character-istic of the CDC medical services in BH
In the CDC military medical service, surgeonhad a key position in a war hospital Due to thecloseness of the front-line and location of war hos-pitals, positioning surgeons in the rear was neithernecessary nor advisable, unlike the positioning ofbattalion surgeons within the framework of theNATO doctrine (36)
Only the most serious cases, such as head andbrain injuries, were transported further after firstaid and stabilization, most often to Croatia (32)
Although generally short in personnel andequipment, the war hospitals were able to offercomplete medical care, after which the soldiers
would return to their units Most of the woundedreceived definite treatment in the war hospitalsPatients needing longer recovery and rehabilita-tion were sent to civilian hospitals in the rear
The 1-5 echelon principle of care for thewounded, as well as distribution of the equip-ment, was mostly condensed to two or three stepsof care (31)
War hospitals did not have a strict organiza-tional structure, but were the result of needs, ca-pacities, and initiative of their commanders Itshould be emphasized that the war hospitals, al-beit located within operational zones, were undercommand of the Health Care Sector of the Depart-
ment of Defense (Fig 4) Moreover, since all CDCphysicians were officers, they had a considerableindependence and freedom in making decisions,which not only resulted in high-quality leadershipbut was also indispensable for survival in encir-cled enclaves
After Dayton Peace Agreement
Dayton Peace Agreement (21 November 1995)divided BH into two entities Croat-Bosniac Fed-eration of BH and the Republic Srpska, with tworespective armies The Federation of BH had thearmy composed of two components the CDC and
the Bosniac-controlled Army of BH, whose organi-zation stemmed from the key principles of authen-ticity and sovereignty of both nations of the Feder-ation of BH Currently, every commanding posthas a deputy position alternately occupied byBosniacs and Croats Overall numerical ratio is23:1 for Bosniacs The army is organized in accor-dance with NATO standards, which means that itsorganization and training is provided through theEquip and Train program by the Military Profes-sional Resource Inc (MPRI, Alexandria, VA, USA),a forum of US military experts
At the level of the Ministry of Defense, medi-cal service, together with veterinary medicine, ispart of the Logistics Sector (Fig 6)
At the level of Military Corps Headquarters(Joint Command) military medical and veterinary
services also belong to the Logistics Sector (Fig 7)Discussion
The MCH was established as a managerial andorganizational body with the task to conceptualizethe system of health care in war circumstancesThe concept of integrated civilian and militarymedical services was adopted Health care wasbased on the resources within the primary healthcare (health centers), small local hospital in Livno,and Mostar regional center, whose personnel wasreduced by at least a half The development of mil-itary formations was adequately followed by thedevelopment of medical formations within them
War hospitals were established depending on thedevelopment of military actions, and most of themwere positioned close to the battlefront War hos-pitals cared for both soldiers and civilians Since acomplete treatment and rehabilitation of thewounded were provided, these war hospitals
137
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
Minister of Defense
Logistics Sector
Medical and VeterinaryServices
Figure 6 Proposal of the structure of the Ministry of De-fense of the Federation of Bosnia and Herzegovina (afterDayton PeaceAgreement in 1995) Lines with arrows indi-cate other Sectors or Departments
Commander of the Joint HeadquartersDeputy Commander of the Joint
Headquarters
Commander of the
Joint HeadquartersDeputy Commander
Assistant and DeputyAssistant Commander
for Logistics
Medical and Veterinary Services
Figure 7 Structure of the Joint Headquarters of theArmy of Bosnia and Herzegovina and Croatian DefenseCouncil (Army of the Federation of Bosnia and Herze-govina) after Dayton Peace Agreement in 1995 Lineswith arrows indicate other Sectors or Departments
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
15/17
could be considered the 5th echelon (36), althoughthey were too close to the front-line (31)
Patients who needed further medical care
were sent to the tertiary level institutions in theRepublic of Croatia There were many of them,and they were sent to Croatia from both Bosniacand Croat medical institutions in BH (19,23,31,32,34,35,54), regardless of patients combat status,nationality, or religion (55,56) The cost of care forBH patients in the Republic of Croatia reachedDM35 million (official data from the CroatianHealth Insurance Institute), which is surely one ofthe greatest humanitarian supports ever givenfrom one state to another
In addition to with primary health care for thewounded and the sick, preventive and epidemiolo-gic measures were also carried out efficiently, be-
cause there were no epidemic outbreaks despite thesharp decrease in the living standard and a large-scale refugee crisis
Medical supplies, equipment, and sanitarymaterials were not manufactured in BH, but theirsupply to war and civilian medical institutionswas adequate The help came from many humani-tarian organizations and individuals from all overthe world, especially those who had experience orconnection with Meugorje (a famous pilgrimagedestination in West Herzegovina)
Our doctrine of independent war hospitals,headed by a strong-minded and highly educatedcommander, grossly alleviated problems of person-
nel shortage A smart commander could greatly af-fect functioning of the hospital by retraining of thepersonnel (eg, dentist into surgeon), or organizingadditional training (eg, of a medical technician toperform anesthesia) Medical specialists were re-cruited partly from displaced physicians fromother parts of BH, and partly (at the beginning)from the volunteers from abroad, mostly Croatia
Although we were acquainted with militarymedical doctrine of the former Yugoslav FederalArmy, NATO, and other countries, we could notuse any of their models We were actually com-pelled to build a unique system of our own Oursystem was a mixture of NATO (36), Israeli (9-11),
and Croatian (19,52) doctrine, but on the whole, itwas our own doctrine, specific for the given situa-tion (31) Its main feature was independence ofpolitics and of the army Relative independence,high level of education, and experience of the phy-sicians resulted in satisfactory organization of mil-itary/civilian medical services and made thesevery physicians, as those in Croatia a year earlier(57), leading figures in peace initiatives, ex-changes of prisoners of war, and humanitarian ac-tions Organizing care for the refugees and dis-placed persons and the surveillance of prisonswere physicians merits
Since there were not many highly educated
military commanders, the MCH opted for independ-ent position in the planning and organizing, as wellas in operational activities All head physicians inarmed units were officers and completely autono-
mous in their medical command Although theywere the assistants to the commanding officers, theywere not subordinated to them Commander of theMCH was at the same hierarchical level as the com-mander-in-chief of the armed forces
After the Dayton Peace Agreement and cessa-tion of war in BH, integration of war hospitals intothe civilian health system allowed the establish-ment of the civilian sector of medical services,whereas the CDC military services remained in theCDC armed units, ie, in professional brigades andteaching centers integrated into the BH FederationArmy The MCH was dissolved, with only medicaldocumentation remaining
Medical service and its professionals in theBH Federation Army now exist within the bothMinistry of Defence and Joint Army Headquarters
My personal opinion is that Medical Service is notgiven the importance it should have in a militarysystem Low positioning of medical officerswithin the officer personnel, as well as the hierar-chical position of the medical service itself, is notadequate It is true that the current BH Armymodel has been made according to the NATO sys-tem, but neither tradition, health care experience,nor traditionally respected status of a physicianwere taken into account Communication with thecivilian health care system is weak, which is a set-back for any country or situation Hopefully, theexisting tendency of reducing armed units in BHwill lead to eventual demilitarization of BH, mak-ing the discussion on the position of medicine andphysicians in BH armed forces unnecessary
References
1 Mandi D Bosna i Hercegovina III Etnika povijestBosne i Hercegovine Rome: Croatian History Insti-tute; 1967
2 Ivanovi V, Vlahui A, editors Ethnic cleansing ofCroats in Bosnia and Herzegovina 1991-1993 Grude:Croatian Community of Herzeg-Bosnia; 1993
3 Adley R, Evans DHC, Mahoney PF, Riley B, RodgersCR, Shanks T, et al The Gulf war: anesthetic experi-ence at 32 Field Hospital Department of Anaesthesiaand Resuscitation Anaesthesia 1992;47:996-9
4 Jennings SA, Cohen DL, Corrow LK, Harper ML,McCain G, Wiedeman J Deployment of an air trans-portable hospital in support of allied forces duringoperation provide comfort: April 29 to July 17, 1991Mil Med 1993;158:135-41
5 Kizer KW The healthof Persian Gulf veterans JAMA1995;273:1817
6 Beary JF III, Bisgard JC, Armstrong PC The civil-ian-military contingency hospital system (CMCHS) pro and con N Engl J Med 1982;306:738-40
7 Wedel KH Military-civilian collaboration for disas-ter medicine in the Federal Republic of Germany(FRG) Prehosp Disast Med (J WAEDM) 1985;1:33-4
8 Rocha Da Silva FF Military concepts and emergencymedical services in Portugal Prehosp Disast Med (J
WAEDM) 1985;1:259 Adler Y Military-civilian collaboration for disaster
medicine in Israel Prehosp Disast Med (J WAEDM)1985;1:32
138
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
16/17
10 Naggan L Medical planning for disaster in IsraelEvaluation of the military surgical experience in theOctober 1973 War, and implications for the organi-zation of the civilian disaster services Injury 1986;
4:279-8511 Reches M Integration of health services in Israel civilian and military health services coordinationduring the Israel wars and peacetime [PhD thesis]Bethesda (MD): Uniformed Services University ofHealth Services; 1985
12 Pogodin IUI, Gurov AN The significance of the ex-perience in organizing medical support for thetroops during the war years for the development ofthe modern military medical infrastructure Vojno-medicinski Zhurnal 1995;79:10-2
13 Chizh M The organizational bases for the buildingof a modern medical support system for the ArmedForces Vojnomedicinski Zhurnal 1996;317:4-20
14 Savezni sekretarijat za narodnu odbranu, Sanitetska
uprava Pravilo sanitetske slu.be oru.anih snaga uratu Belgrade: Vojnoizdavaki zavod; 197715 Kostovi I, Juda M Mass killing and genocide in
Croatia 1991/92: a book of evidence Zagreb: Hrvatskasveuilina naklada; 1992
16 Lang S The war in Croatia through the prism of hu-man rights Peace Psychology Reviews1994;1:15-23
17 Lang S, Marui M Peace and human rights: Painfullessons of the Balkan war International Minds 1993;4:6-13
18 Lackovi Z, Markeljevi J, Marui M Croatian med-icine in 1991 war against Croatia: a preliminary re-port Croat Med J 1992;33 War Suppl 2:110-9
19 Hebrang A Reorganization of the Croatian health
care system Croat Med J 1994;35:130-620 Marui M, Kostovi I Attacks on Croatias hospi-tals Lancet 1991;338:1018
21 Markeljevi J, Lackovi Z The case of Croatian hos-pitals: is this the end of humanitarian rules? MedWar 1994;10:50-62
22 Husar J, Eltz J Mobile surgical teams in Croatianspecial forces units (1990-1993) Croat Med J 1993;34:276-9
23 Puntari D, Brki K Formation and organization ofmilitary medical service at the East Slavonia front inthe 1991/1992 war in Croatia Mil Med 1995;160:412-6
24 Rukavina A, Glavi Z, Fajdi J, Vukoja M, Gveri D,Mustapi S War-related transformation and work of
Surgery Service of the Po.ega Medical Center,East-Croatian hospital unaffected by direct war ac-tivities Mil Med 1995;160:604-8
25 Batinica J, Batinica S War wounds in the ibenikarea during the 1991-1992 war against Croatia MilMed 1995;160:124-8
26 Peri M, Hamel D, Rac S, Pirc-Tiljak D, Bekavac-Belin M, Turjak J, et al Civilian medicine and warTransformation of the health center to a war hospitalin Croatia (July 1991-October 1992) Injury 1996;27:395-9
27 Stani V, Gopevi A, Heitzler-Nikoli V, Bekavac-Belin M, eni B, Peri M War hospital in VelikaGorica: the first seventy days Croat Med J 1992;33War Suppl 2:175-83
28 Butkovi-Soldo S, Brki K, Puntari D, Petroviki ZMedical corps support to a brigade action during anoffensive action including river crossing Mil Med1995;160:408-11
29 Martinovi M Destruction of Mostar Medical centerduring 1992 Serbian aggression Croat Med J 1994;35:56-8
30 Tomi Z, Mami I Second year medical students on
the battlefield in Bosnia-Herzegovina studentBMJ1995;3:167-831 ari V, Atias-Nikolov V, Kova T, Frankovi E, Mri
V, Luka J NATO war medicine doctrine revisited inBosnia and Herzegovina J Royal Army Med Corps1994;140:132-4
32 Atias-Nikolov V, ari V, Kova T, Frankovi E, MriV, Luka J, et al Organization and work of the warhospital in Sturba near the town of Livno, Bosniaand Herzegovina Mil Med 1995;160:62-9
33 Rado D, Kne.evi A, Ezgeta I, Vlahui A, Celina PHealth care in the .epe region during the war(1992-1995) in Bosnia and Herzegovina Croat Med J1995;36:212-4
34 Radoni V, Pavi A, Aras N Organization and func-tioning of the front-line surgical station at Rama inBosnia and Herzegovina Mil Med 1993;12:763-9
35 Petrievi A, Radoni V, Ili N, Petrievi M, Zeli Z,Ferenca J, et al Surgical experience at the Rama warhospital in Bosnia and Herzegovina Israel J Med Sci1995;31:630-4
36 Bowen TE, Bellamy RF, editors Emergency war sur-gery NATO handbook, 2nd US revision Washing-ton DC: US Department of Defense; 1988
37 Ryan NM, Cooper GJ, Haywood IR, Milner SM Fieldsurgery on a future conventional battlefield: strategyand wound management Ann R Coll Surg Engl1991;73:13-20
38 Dr.avni zavod za statistiku Republike Hrvatske
Stanovnitvo Bosne i Hercegovine Narodnosni sastavpo naseljima Zagreb: DZS; 199539 arac I, Bagari I, Orekovi S, Reamy J, imunovi
VJ, Lang S Physician requirements for the Croatpopulation in Bosnia and Herzegovina Croat Med J1997;38:83-7
40 Marui A, Marui M, Lang S White Road for NovaBila and Silver Bosnia: a chronology of the humani-tarian convoy Croat Med J 1994;35:3-7
41 Ivankovi A, Rebac Z Financing of dental healthcare in the Federation of Bosnia and HerzegovinaCroat Med J 1999;40:166-74
42 Bogdanovi S, Margaritoni M, Kojic N, Rakigija A,egedin J, oa I, et al Dubrovnik General Hospital:
civilian surgery in the besieged town Croat Med J1994;35:94-943 Anonymous Opi okvirni sporazum za mir u Bosni
i Hercegovini Sarajevo: Dnevni avaz 1995 Novem-ber 28; 2-3
44 Smajki A, editor Zdravstveno-socijalne posljedicerata u BiH Sarajevo: Svjetlost and Federalni zavodza zdravstvenu zatitu BiH; 1997
45 Zavod za zdravstvenu zatitu Bosne i HercegovineMre.a, kapaciteti i djelatnost zdravstvene slu.be uBosni i Hercegovini u 1991 godini Sarajevo: ZZZBH;1992
46 SIZ zdravstvene zatite Bosne i Hercegovine Izvje-taj o radu SIZ zdravstvene zatite BiH u sprovo-enju zdravstvene zatite u SR BIH u 1989 god Sara-
jevo: SIZZZBH; 199047 Zavod za javno zdravstvo Federacije BiH Mre.a,
kapaciteti i djelatnost zdravstvene slu.be u FederacijiBiH 1991-1995 Sarajevo: ZZJZ Federacije BiH; 1998
139
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
-
8/10/2019 Medical Services of Croat People in Bosnia and Herzegovina during 1992-1995 War: Losses, Adaptation, Organizati
17/17
Bagari: Croat Medical Services during War in BH Croat Med J 2000;41:124-140
48 Meu.upanijski zavod za javno zdravstvo Pregledmre.e, kapaciteta i djelatnosti zdravstvene slu.be u1996 godini Mostar: MZJZ; 1997
49 Mijatovi D, Henigsberg N, Juda M, Kostovi I Use
of digital wireless communications system for rapidand efficient communication between Croatianmedical centers in war Croat Med J 1996;37:71-4
50 Kapulica Z Croatian Medical Corps first echelon: afront line doctor Croat Med J 1992;33 War Suppl 2:172-4
51 Petra D, Georgijevi A, Kusi Z, Valent I Organiza-tion and functioning of the Sisters of Mercy Univer-sity Hospital in the war against Croatia Croat Med J1992;33 War Suppl 2:193-6
52 Janoi K, Lovri Z War surgery in Osijek during1991/92 war in Croatia Croat Med J 1995;36:104-7
53 Boban M Odluka o formiranju Hrvatskog vijeaobrane Narodni list HZ Herceg-Bosna 1992;(I):4
54 Balen I, Prgomet D, Gjani D, Puntari D Work of the
Slavonski Brod General Hospital during the war in
Croatia and Bosnia and Herzegovina in 1991-1992Mil Med 1995;160:588-92
55 Gottstein U International Physicians for the Preven-tion of Nuclear War (IPPNW) delegate visit to the hos-
pitals in Split, West Mostar and East Mostar, Novem-ber29-December6, 1993 Croat MedJ 1994;35: 53-856 Becker S The Angel of Mostar London: Hutchinson;
199457 Blaskovich J Anatomy of deceit An American phy-
sicians first-hand encounter with the results of thewar in Croatia New York (NY): Dunhill PublishingCo; 1997
Received: February 22, 2000Accepted: April 18, 2000
Correspondence to:Ivan BagariMinistry of Health Care of the Federation of
Bosnia and HerzegovinaTitova 9
71000 Sarajevo, Bosnia and Herzegovinaivanbagaric@zgtelhr
The 3rd International Conference on Priorities in Health Care
Amsterdam, The Nederlands23-24 November, 2000
Constrained resources and increasing demands make the setting of priorities in health care apressing issueThe conference will focus on the daily practice in which choices are made What is the role ofthe various parties involved, and which factors exert influence? What can be learned from theway in which the issue of choice is handled at all levels of the health care system? What are theconsequences of implementing priorities in health care? The conference will show that,
although results from health services research and health technology assessment are needed,translating from theory into practice needs to be done with great careThe conference will offer a stimulating exploration of two main themes: The role of variousactors in priority setting and Why choose for investing in health The former concentrates onhow choices are made in the interactions between the different actors, eg, policy makers,managers, physicians and other health professionals, patient and consumer organizations, andresearchers, and what is needed to achieve change The second theme is more reflective in itsorientation: investments in health care are compared with other social issues like housing andeducationAll parties involved in or affected by decision-making concerning priorities in health care areinvited to submit papers on this issue and to participate in the conference
For more information, visit the web site: www.healthpriorities.netor contact:
Boerhaave Congress Office, c/o Mr JJL Muller, PO Box 2084, 2301 CB Leiden, the Netherlandsfax: +31 71 527 5262; phone: +31 71 527 5294;[email protected]
mailto:[email protected]:[email protected]:[email protected]