Medical nutrition therapy for Hemodialysis
35
Medical Nutrition Therapy for ESRD - Hemodialysis Dietitian - Jake Brandon M. Andal
-
Upload
jakebrandonandal01 -
Category
Health & Medicine
-
view
567 -
download
2
Transcript of Medical nutrition therapy for Hemodialysis
Medical Nutrition Therapyfor ESRD - HemodialysisDietitian - Jake Brandon M. Andal
Case 3: ESRD Hemodialysis
• GFR = 12 mL/min
• Kidney not immediately available, hemodialysis was recommended
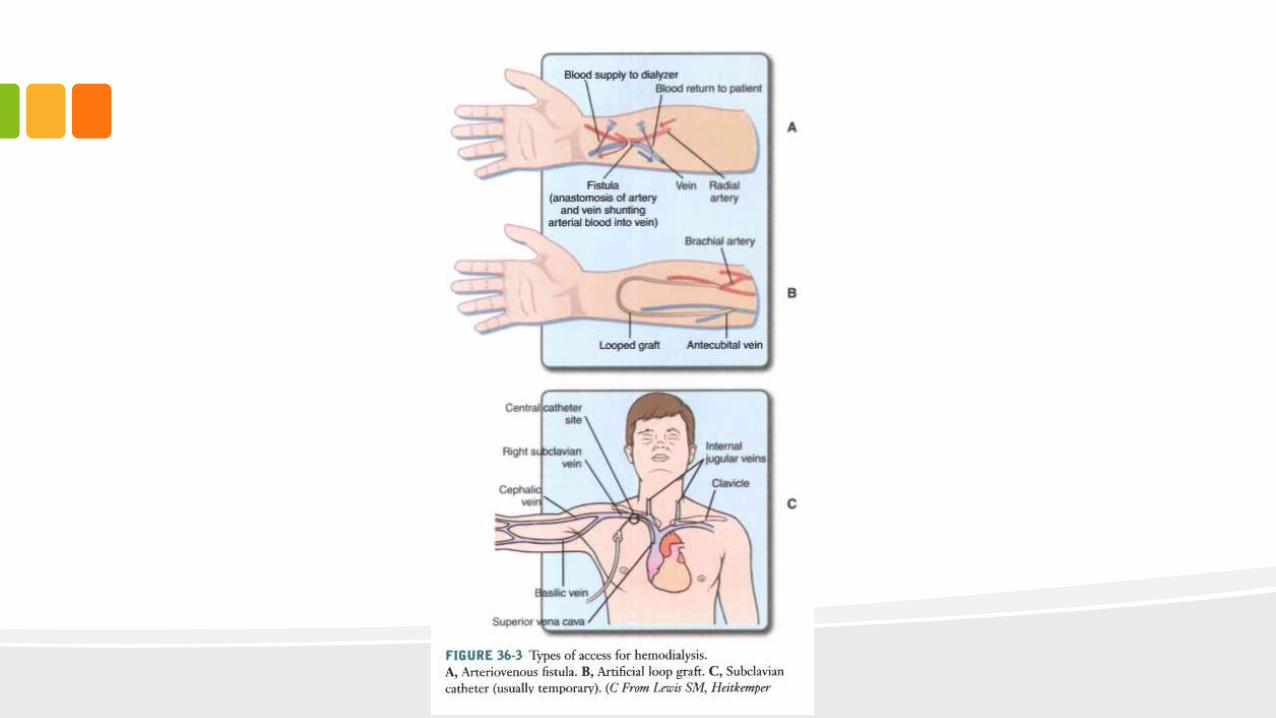
• Arteriovenous fistula was created on his left forearm
• BP na d serum potassium level has risen and BUN is 110 mg/dL
• HD is twice a week
• Instructed to continue phosphate binders and calcium supplements
• Post-dialysis weight gain is 54 kg
Pathophysiology
• End Stage Renal Disease can result from a wide variety of different kidney diseases
– Diabetes Mellitus
– Hypertension
– Glomerulonephritis or Acute Kidney Failure
– Chronic Kidney Failure
• Diagnosis: Stage 5 CKD, BUN 100 mg/dL, Cr 10-12 mg/dL
Medical Treatment
• Options include
– Dialysis <3
– Transplantation
– Medical management progressing to death
Dialysis
• Px may choose if he/she prefers:
– Outpatient dialysis facility
– Hemodialysis at home
– Peritoneal Dialysis
• Continuous Ambulatory Peritoneal Dialysis (CAPD)
• Continuous Cyclic Peritoneal Dialysis (CCPD)
Factors to consider in type of Dialysis Treatment
• Availability of family/friends/caretaker to assist therapy
• Type of water supply ate home
• Previous abdominal surgeries
• Membrane characteristics of Peritoneal Membrane
• Body size, cardiac status, presence of vascular access
• Desire to travel
What is Hemodialysis?
• Hemodialysis requires permanent access to blood stream through a FISTULA
– If the patient’s blood vessels are fragile, a GRAFT is necessary
• Large needles are inserted into the fistula or graft each dialysis and removed when dialysis is complete
• HD’s fluid is similar to that of a Human’s Plasma
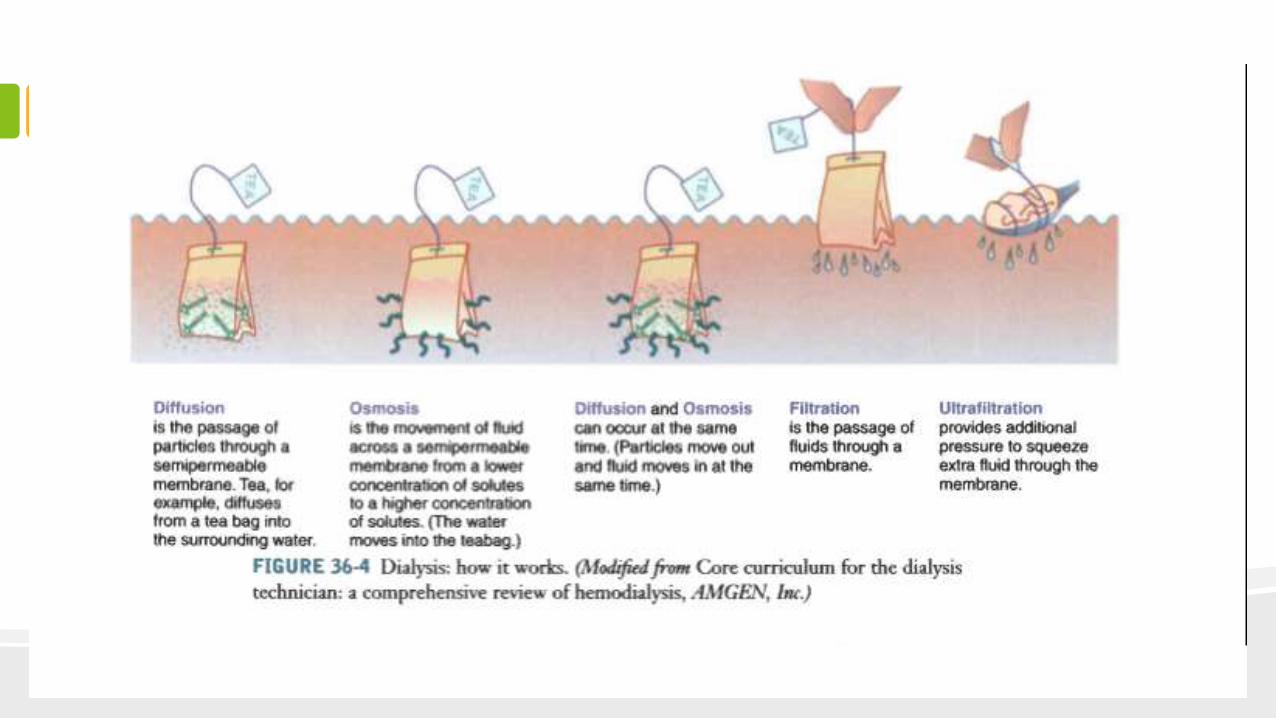
• Waste Products and Electrolytes are removed by diffusion, ultrafiltration, and osmosis from the dialysate
• Usually 3 to 5 hours ; newer treatments are shorter
What is Peritoneal Dialysis
• Uses the body’s PERITONEUM
• Dialysate containing High-dextrose solution is installed in the peritoneum
– Diffusion ; blood dialysate (wastes)
– Osmosis (water)
• Advantage compared to HD: avoids large fluctuations in blood chemistry, longer residual renal function and ability of the patient to live a normal lifestyle
• Complications: Peritonitis, Hypotension and WEIGHT GAIN
• Icodextrin – superior fluid removal without dextrose absorption
Evaluation of Dialysis Frequency
• Kinetic Modeling
– Measures the removal of urea from the patient’s blood over a given period
– Kt/V
• K – Urea Clearance
• t – Length of time of dialysis
• V – Total Body Water Volume
• Urea Reduction Ratio
– Looks ate the reduction of urea after dialysis
GOALS?????
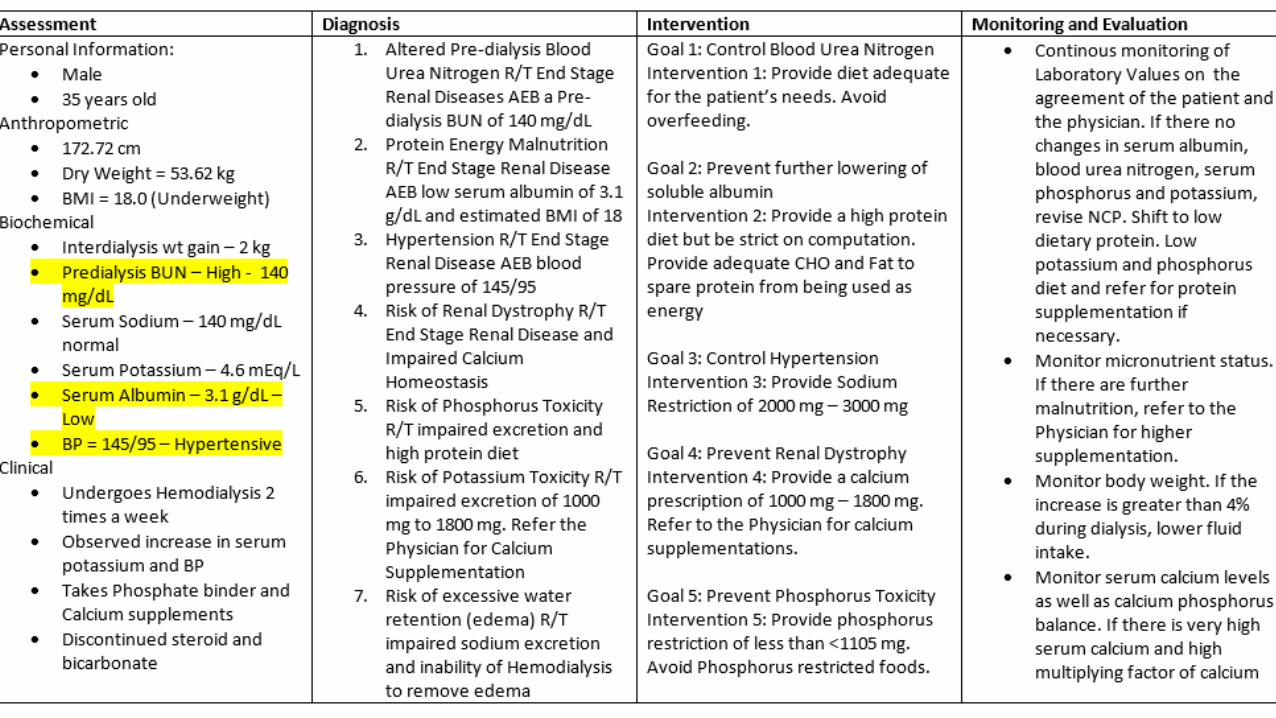
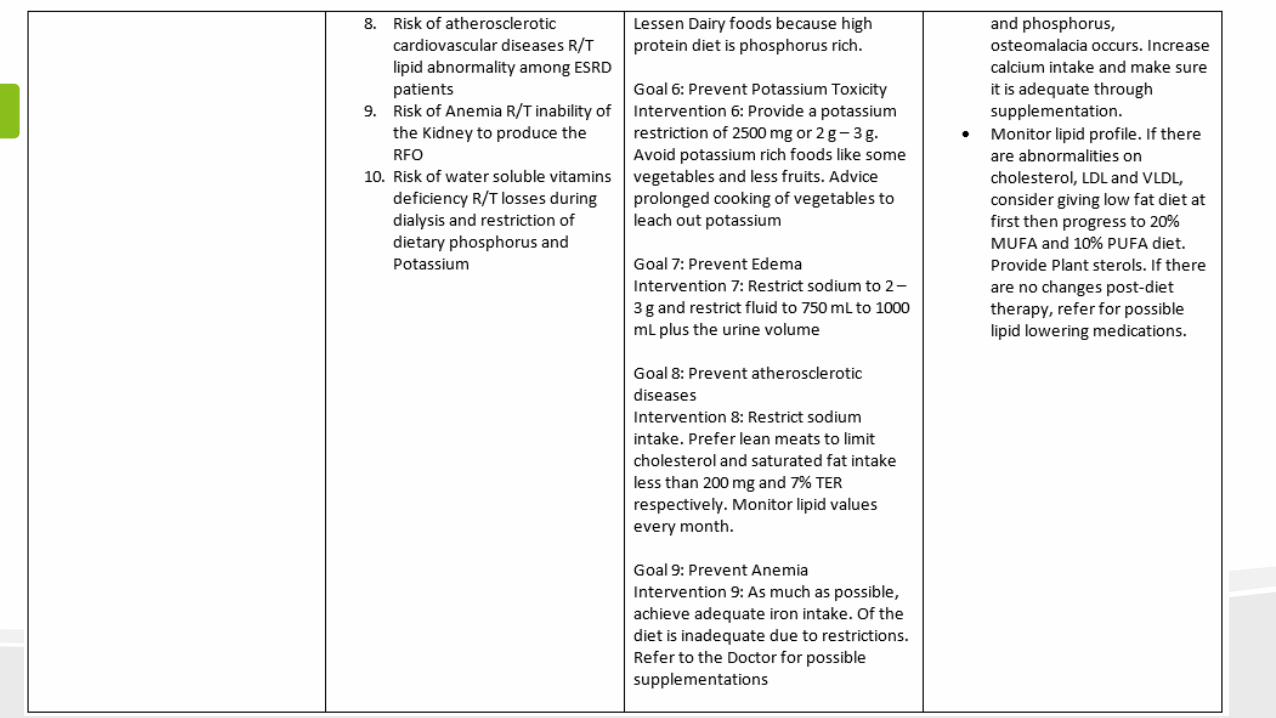
Medical Nutrition Therapy Goals
• Prevent deficiency and maintain good nutrition status through adequate protein, energy, vitamin and mineral intake
• Control edema and electrolyte imbalance by controlling sodium, potassium and fluid intake
• Prevent or retard development of renal osteodystrophy by controlling calcium, phosphorus, Vitamin D and PTH
Medical Nutrition Therapy Goals
• Enable the patient to eat a palatable, attractive diet that fits his or her lifestyle as much as possible
• Coordinate with the Healthcare Team
• Provide initial nutrition education, periodic counseling and long term monitoring of patients
PROTEIN NEEDS
• Dialysis drains body protein
• 1.2 g of Pro for patients who receive HD three times a week
• Albumin is a limited factor of protein nutriture, but is routinely used in evaluating ESRD’s NS
• Patients with Uremia have greater chances of lowered protein intake
• Patients may tolerate other sources of meats better
• Phosphate restriction may be lifted to allow dairy products
Energy
• SHOULD BE ADEQUATE TO SPARE PROTEIN
• 25 kcal – 40 kcal/g of body weight
• Higher needs for patients in PD
Fluid and Sodium Balance
• Thirst may indicate excessive sodium intake, increased fluid gain and resultant hypertension
• Allowed weight gain (fluid gain) for HD patients – 2 to 4 kilograms
• Restriction on fluid: 750 ml + urine output
• Some patients may have salt wasting tendencies which mayerequire extra sodium
• Frequent dialyses, daily PD, daily nocturnal dialysis – higher allowance for sodium and fluid
Potassium
• Restriction would be based on the frequency of Hemodialysis
• Be careful: Low sodium foods contain potassium chloride as a salt substitute
Phosphorus
• As GFR decreases, phosphorus excretion also decreases
• High-protein diet may also be equated to high phosphorus intake
• Phosphate binders
– May cause GI distress, diarrhea or gas
– Severe constipation intestinal impaction
Calcium and Parathyroid Hormone
• ESRD patients Impaired Calcium and PTH balance
• As GFR decreases, serum calcium declines because
– Decreased ability to convert Vit. D
– Increased need due to high phosphorus intake
– Hypertrophy of the Parathyroid gland• Over secretion of PTH
• Secondary hyperparathyroidism
• Calciphylaxis
– Deposition in wound tissues with resultant vascular calcification, thrombosis, non-healing wounds and gangrene
Lipids
• Risk of atherosclerotic cardiovascular diseases
• Elevated TG without increase in cholesterol
• Low cholesterol levels may lead to mortality of ESRD
Iron and EPO
• ESRD inability of the kidney to produce EPO
• EPO – stimulates bone marrow to produce red blood cells
• There is also a destruction of red blood cells
• Lost blood in dialysis
RISK FOR ANEMIA
Vitamins
• Water soluble vitamins -> lost during dialysis
• Emphasis on Folate
• Vitamin B12 is protein bound, thus, losses are minimal
• High Phosphorus foods -> High water soluble vitamins
• Niacin -> helpful in lowering phosphate levels in ESRD patients
Case Study: Dietary Computations
• Desirable Body Weight
– (172.27 cm – 100) x .90
– 65 kg
• Dry Body Weight
– NTBW = 54 kg x .50
– =27
– ATBW = (142 mEq/L / 140 mEqL x NTBW)
– =27.38
Dietary Computations
• EBW = 27.38 – 27 kg
• EBW = 0.38 L
• Estimated Dry Weight – 53.62 kg
• Estimated BMI = 18.0 (Underweight)
Total Energy Requirement
• = DBW x 35 kcal/DBW
• =65 kg x 35 kg
• = 2275 kcal ῀ 2250 kcal
Protein Requirement
• = DBW x 1.2 g/KDBW
• = 78 g Pro ῀ 80 g Pro
• NPC = 2250 – (80 g Pro x 4 kcal/g)
• NPC = 1930 kcal
Based on the Diet Manual
Non-Protein Calories Distribution
Carbohydrates
• 1930 kcal x .70
• = 1351 kcal / (4 kcal/g)
• = 337.75 g CHO
• = 340 g CHO
Fat
• 1930 kcal x .30
• = 579 kcal / (9 kcal/g)
• = 64.5 g Fat
• = 65 g Fat
Phosphorus, Potassium and Sodium Restriction
• Potassium
– DBW X 40 mg/KgIBW
– =2600 mg or 2 g - 3 g Potassium
• Phosphorus
– DBW x < 17 mg / Kg DBW
– = < 1105 mg
• Sodium
– 2 – 3 g
Fluid and Restriction
• Fluid
– 750 mL – 1000 ml / Day
• Calcium
– 1000 mg – 1800 mg (supplements as needed)
Final Diet Prescription
• 2250 kcal ; 340 g CHO ; 80 g Pro ; 65 g Fat
– 2 – 3 g Potassium
– < 1105 Phosphorus
– 750 mL – 1000 mL Fluid
– 2 – 3 g Sodium
– 1000 mg – 1800 mg Calcium
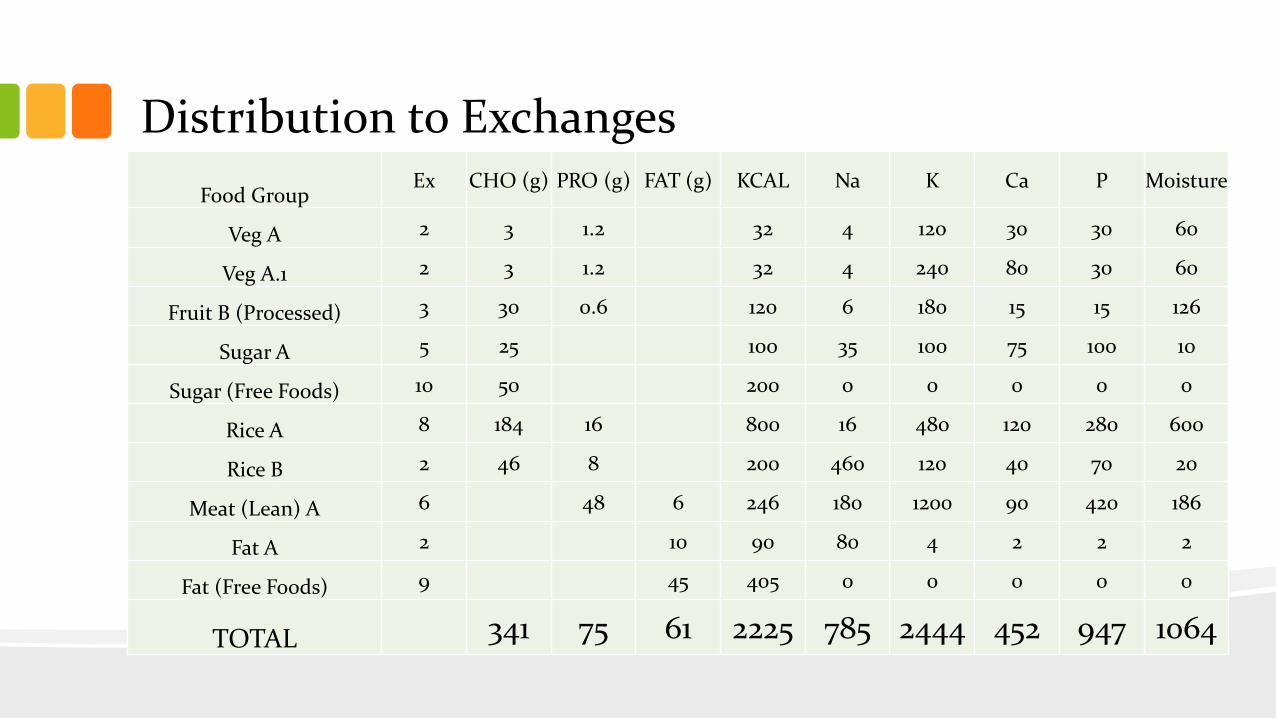
Distribution to Exchanges
Food GroupEx CHO (g) PRO (g) FAT (g) KCAL Na K Ca P Moisture
Veg A 2 3 1.2 32 4 120 30 30 60
Veg A.1 2 3 1.2 32 4 240 80 30 60
Fruit B (Processed) 3 30 0.6 120 6 180 15 15 126
Sugar A 5 25 100 35 100 75 100 10
Sugar (Free Foods) 10 50 200 0 0 0 0 0
Rice A 8 184 16 800 16 480 120 280 600
Rice B 2 46 8 200 460 120 40 70 20
Meat (Lean) A 6 48 6 246 180 1200 90 420 186
Fat A 2 10 90 80 4 2 2 2
Fat (Free Foods) 9 45 405 0 0 0 0 0
TOTAL 341 75 61 2225 785 2444 452 947 1064
Calcium and Sodium Supplement Computation
• Calcium Restriction – 1400 mg
• Less: Inherent Calcium – 467 mg
• Remaining = 933 mg Ca
– Equivalent to (2) 500 mg tablets
• Sodium Restriction – 2000 mg (Lower limit)
• Inherent Sodium – 815 mg
• Remaining = 1185 mg = 2 ¼ tablespoon Salt Solution