
Medical Management of Pulmonary Hypertension Dr. Christopher J Arendt, PharmD, RPh Assistant...
27
Medical Management of Pulmonary Hypertension Dr. Christopher J Arendt, PharmD, RPh Assistant Professor of Pharmacy Mayo Clinic College of Medicine Rochester, Minnesota
-
Upload
victor-skinner -
Category
Documents
-
view
221 -
download
0
Transcript of Medical Management of Pulmonary Hypertension Dr. Christopher J Arendt, PharmD, RPh Assistant...

Medical Management of Pulmonary Hypertension
Dr. Christopher J Arendt, PharmD, RPhAssistant Professor of PharmacyMayo Clinic College of Medicine
Rochester, Minnesota

2
Disclosure
• Nothing to disclose
• No financial interests

3
Objectives
• Describe the common mechanisms of action of 4 medication classes used to treat pulmonary hypertension.
• Recognize common drug-drug and drug-herbal interactions with pulmonary hypertension management medications and what to expect.
• Identify the most common adverse effects seen with medications used to manage pulmonary hypertension.
4
Pulmonary Arterial Hypertension
What is it?Mean pulmonary Artery Pressure(mPAP) > 25 mmHg
Normal to reduced Cardiac Output (CO)Normal capillary wedge pressure (PCWP)
Characterized by :Vascular constrictionCellular proliferationProthrombotic state
Dyspnea, fatigue, weakness, inability
to tolerate exertion

5
World Health Organization classification of functional status for Primary Pulmonary
Hypertension
Class Description
I No limitations in physical activity, ordinary physical activity does not cause dyspnea or fatigue
II Slight limitation in physical activity; ordinary physical activity produces dyspnea, fatigue, chest pain, or near-syncope; no symptoms at rest
III Marked limitation of physical activity; less than ordinary physical activity produces dyspnea, fatigue, chest pain, or near-syncope; no symptoms at rest
IV Unable to perform any physical activity without symptoms; dyspnea and/ or fatigue present at rest; discomfort increased by any physical activity

6
PAH Etiology

7
• Idiopathic Pulmonary Arterial Hypertension
• Hereditary (Genetic) Pulmonary Arterial Hypertension
• Associated Pulmonary Arterial Hypertension
8
Grouping of DiseaseDue to left heart failure (increased back pressure in the pulmonary vessels)• Left ventricular pump failure (heart attack, cardiomyopathy)• Left ventricular stiffness (hypertension, diabetes, metabolic syndrome)• Valve disease (mitral or aortic stenosis or regurgitation)Diseases affecting the whole lung (lung diseases obliterate blood vessels)• Chronic bronchitis and emphysema (combination of loss of lung plus hypoxia)• Interstitial lung diseases (destructive diseases that obliterate vessels, such as pulmonary fibrosis, sarcoidosis,and many others)Hypoxia related (decreased oxygen constricts pulmonary blood vessels)• High-altitude dwelling• Sleep apnea and other hypoventilation syndromes• Hypoxia of chronic bronchitis and emphysema (chronic obstructive pulmonary disease, or COPD)
American Thoracic Society http://thoracic.org/education/breathing-in-america/resources/chapter-17-pulmonary-hypertension.pdf

9
Grouping of DiseasePulmonary arterial hypertension (changes in the structure and function of the pulmonary arteries)• Idiopathic (formerly primary pulmonary hypertension)• Heritable (formerly familial, due to BMPR2 or Alk-1 mutations)• Drug- and toxin-induced (stimulants)• Connective tissue diseases (especially scleroderma)• HIV infection (rare occurrence <1%)• Portal hypertension (cirrhosis and other advanced liver diseases)• Congenital heart disease that allows blood to shunt around the lungs• Pulmonary veno-occlusive disease and pulmonary capillary hemangiomatosis (rare)Primarily obstructing diseases of the pulmonary vessels• Pulmonary thromboembolism• Schistosomiasis• Sickle cell anemia• Tumor emboli• Fibrosing mediastinitis (obstruction by fibrosis related to histoplasmosis)
American Thoracic Society http://thoracic.org/education/breathing-in-america/resources/chapter-17-pulmonary-hypertension.pdf
10
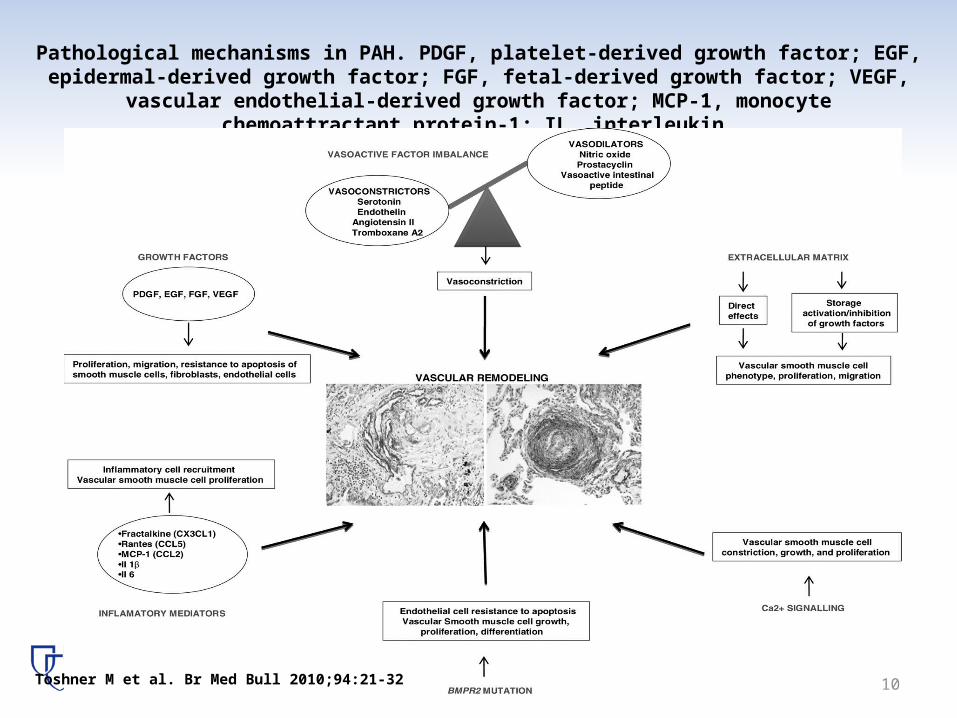
Pathological mechanisms in PAH. PDGF, platelet-derived growth factor; EGF, epidermal-derived growth factor; FGF, fetal-derived growth factor; VEGF, vascular endothelial-derived
growth factor; MCP-1, monocyte chemoattractant protein-1; IL, interleukin.
Toshner M et al. Br Med Bull 2010;94:21-32

11
Cellular Mechanisms
Am Heart J 2011;162:201-13

Classic vasodilator and vasoconstrictor systems and their translational therapies for pulmonary arterial hypertension
(PAH).
Yen-Chun Lai et al. Circulation Research. 2014;115:115-130

13
Medication Players
Adapted from Am Heart J 2011;162:201-13
(Phosphodiesterase Inhibitor)(Endothelin Receptor )Antagonist
Treprostinil Oral• 390 Patients• Class II or III
Dec 2013
2013
Riociguat Oral• 443 Patients• Class II or III
2013
Soluble Guanylate Cyclase (sGC) Stimulator
14
Supportive Therapy
• Oxygen• Diuretics• Digoxin ( K channel and Calcium )• Anticoagulants (Warfarin)
15
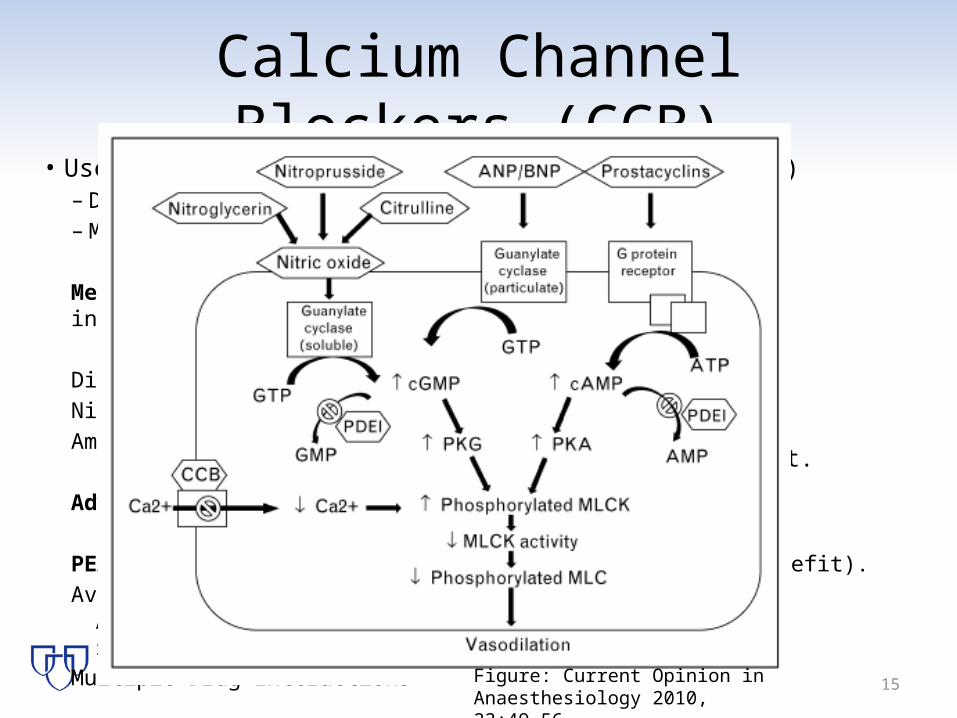
Calcium Channel Blockers (CCB)• Use if a Positive response (Vasoreactivity test)
– Decrease in mPAP ≥ 10 mmHg to a value ≤ 40 mmHg– Most beneficial in IPAH, FPAH, though limited
Mechanism: Inhibits Fast Calcium Channels, Reduces intracellular calcium, thus inhibits vasoconstriction
Diltiazem (Start 120 mg/day)Nifedipine (start 30 mg/day)Amlodipine (start 5 mg/day)
Adverse effects: Hypotension, constipation, edema
PEARL: Frequent follow up ( 50% of pts see loss of benefit).Avoid verapamil
Avoid CCB in severe PAH due to high short-term mortality. Start Stool softeners
Multiple Drug Interactions
Titrate Weekly. 3 month follow up. 1 year cath lab repeat.
Figure: Current Opinion in Anaesthesiology 2010,23:49–56

16
Prostaglandins• Epoprostenol
Mechanism: Direct vasodilation, inhibition of platelet aggregation– Epoprostenol IV (Central line) start at 2 ng/kg/min. Dose increase over 6
months. Range 25-40 ng/kg/min. Bag change every 8 hr. Refrigerated bag good for 28 hrs. Uses special diluent. Establish dosing weight.
– Room Temp Stable (RTS) product can be changed daily. No Special Diluent needed
Adverse Effects: Flushing, HA, jaw and lower extremity muscular pain, diarrhea, nausea, rash.
PEARL: watch for line associated infection and catheter associated venous thrombosis, thrombocytopenia.Back-up bag is necessary. Rebound HTN noted with abrupt DC.RTS and original formulation are not interchangeable.

17
Prostaglandins• Treprostinil
Mechanism: Direct vasodilation, inhibition of platelet aggregation– Treprostinil IV 1.25 ng/kg/min. BAG CHANGE Q48 HRS– Treprostinil SubQ 1.25 ng/kg/min: Change every 3 days.– Treprostinil Inhalation; 1 neb 4 times daily. 3 breath start. 9 max/dose.– Treprostinil Oral Extended Release Tab BID
Adverse Effects: IV: Flushing, HA, jaw and lower extremity muscular pain, diarrhea, nausea, rash. SubQ: Injection site Pain ( 85%), with 8% stopping therapy. Inh: cough and throat irritation; headache, gastrointestinal effects, muscle, jaw or bone pain, flushing and syncope Oral; Diarrhea
PEARL:IV/SubQ Back-up bag is NOT necessary due to the long half-life. No ice packs needed. Rebound HTN noted with abrupt DC.Neb uses 1 tube of drug/day, programming number of breathes on device.- 10 min pause between breaths is allowed. > 15 min pause resets the machine.

18
Prostaglandins
• IlloprostMechanism: Direct vasodilation, inhibition of platelet aggregation– Illoprost 2.5 mcg/mL initial.
6-9 times daily.
Adverse Effects: Cough, flushing, HA
PEARL:
10-15 min neb. Takes time to admin.Max dose 45 MG/DAY.3RD OR 4TH Line PAH Agent
$5,000 neb device

19
Endothelin Receptor Antagonist
• BosentanMechanism: Blocks Both Endothelin A (ET A) and B (ET B) receptors, reducing exposure to vasoconstrictive and proliferative effects of Endothelin.– Bosentan 62.5 mg oral twice daily. Titrate to 125 mg oral twice
daily.Adverse Effects: Liver toxicity (If 3x normal aminotransferases , hold therapy), HA, Dizziness, flushingPEARL:Monthly liver function tests are needed. CYP2C9 Interactions! Inhibited by fluconazole ( azoles), ginko biloba, St. Johns Wort, amidarone. Warfarin, Cyclosporine interactions.50% dose of sildenafil if given concurrently with bosentan
20
Endothelin Receptor Antagonist
• AmbrisentanMechanism: Endothelin A (ET A) to B (ET B) receptor selectivity of 77:1. Inhibiting vasoconstriction and proliferation.– Ambresentan 5 mg daily, may increase to 10 mg daily if
toleratedAdverse Effects: Liver toxicity (watch for elevated aminotransferases , hold therapy), HA, Decreased hemoglobin (Check at baseline and 1 month)PEARL:Pregnancy Test initial and monthly.P-Glycoprotein interactions (Sildenafil, loperamide), possible CYP2C19 interactions ( Clopidogrel and omeprazole)Amiodaone and cyclosporine interactions

21
Phosphodiesterase Inhibitors
• SildenafilMechanism: Inhibit phosphodiesterase-5 and acts to enhance cGMP levels, which will prolong cGMP vasodilating effects in the pulmonary vasculature. – Sildenafil 20 mg oral Three times dailyAdverse Effects: HA, abd. Discomfort, constipation, back painPEARL:APAP premed helps with HA.Interactions CYP3A4 , Itraconazole, Amiodarone, tacrolimus, cyclosporine, SIMVASTATIN(Myopathy)Avoid nitrate, and caution if SBP <90/60 or > 170/90

22
Phosphodiesterase Inhibitors
• TadalafilMechanism: Inhibit phosphodiesterase-5 and acts to enhance cGMP levels, which will prolong cGMP vasodilating effects in the pulmonary vasculature. – Tadalafil 40 mg dailyAdverse Effects: HA, abd. Discomfort, constipation, back pain, nasopharyngitisPEARL:APAP premed helps with HA.Interactions CYP3A4 , Itraconazole (Reduce tadalafil to 2.5 mg daily), Amiodarone, tacrolimus, cyclosporine, Simvastatin ( Myopathy) Avoid nitrate, and caution if SBP <90/60 or > 170/90

23
Soluble Guanylate Cyclase (sGC) Stimulator
• RiociguatMechanism: increase the sensitivity of sGC to endogenous nitric oxide (NO), a pulmonary vasodilator, and directly stimulate the receptor to mimic the action of NO
-Riociguat 1 mg oral Three times daily ( May start as low as 0.5 mg), Max 2.5 mg three times daily.
Adverse Effects: Headache, Hypotension, Dyspepsia, N/V, Anemia, Dizziness, reflux, constipation.
PEARL: Major drug interaction with CYP2C8, CYP3A4 and P-glycoprotein. PPI’s decrease riociguat serum concentrations.Pregnancy Test pre-initiation and monthly

24
Choice of therapy (PAH)
Adapted from : Lourenco A et al. Int J Card 155 (2012) 350-361
Riociguat 5th 5th

25
PAH drug and Herbal Interactions• CYP P450 Enzyme interactions ( 2C8, 2C9, 3A4, 2C19) • Over 90 possible herbal interactions • Major Interactions: Epoprostenol + L-Arginine= HoTN
– Treprostinil + Danshen or Dong Quai ir Evening Primrose, or Willow Bark or Policosanol =Bleed
– Sildenafil + St. Johns Wort= reduced effectiveness of sildenafil– Tadalafil or sildenafil + Sweet Orange= reduced P-Glycop transport= lower
sildenafil and tadalafil levels.
• Others:– Epo +Licorice= less effectiveness (HTN)– Epo + Blue Cohosh= less effective (HTN)– Epo +European Mistletoe=HoTN
26
Wrapping it up
• 3 recognized pathological contributors to pulmonary arterial hypertension… and more to come!
• Recent advances in medical management have improved survival
• Interactions are possible, with significant hypotension , bleeding and toxicity risks.

Medical Management of Pulmonary Hypertension
Dr. Christopher J Arendt, PharmD, RPhAssistant Professor of PharmacyMayo Clinic College of Medicine
Rochester, [email protected]


















