Medical Management and Risk Factor Modification SVS clinical research priorities meeting 2011 Peter...
48
Medical Management and Risk Factor Modification SVS clinical research priorities meeting 2011 Peter Henke, MD University of Michigan
-
Upload
rigoberto-debnam -
Category
Documents
-
view
216 -
download
1
Transcript of Medical Management and Risk Factor Modification SVS clinical research priorities meeting 2011 Peter...

Medical Management and Risk Factor Modification
SVS clinical research priorities meeting 2011
Peter Henke, MDUniversity of Michigan

Overview• Epidemiology of atherosclerotic/-
atherothrombotic manifestations in vascular surgical patients
• Current medical management of arterial vascular disease patients– Evidence for major therapies
• Preoperative risk assessment pathways• Current and potential study areas/questions

Background Issues
• Goals of medical management and risk factor modification for the vascular surgeon– Clinic setting and peri-operative setting
• Local practice patterns often dictate the vascular medicine interest– Do it all yourself to consult specialists for everything
• Costs saved for preventative care by vascular surgeons
• Costs incurred due to multiple consultants and elaborate workups with no discernable patient benefit

Epidemiology
Lloyd-Jones D, etal Circulation 2010;121:e1
• All our patients have atherosclerosis

Epidemiology
Steg PG, etal. JAMA 2007;297:1197
REACH RegistryN = 64,977 with CAD, CVOD, PAD or >3 risk factors
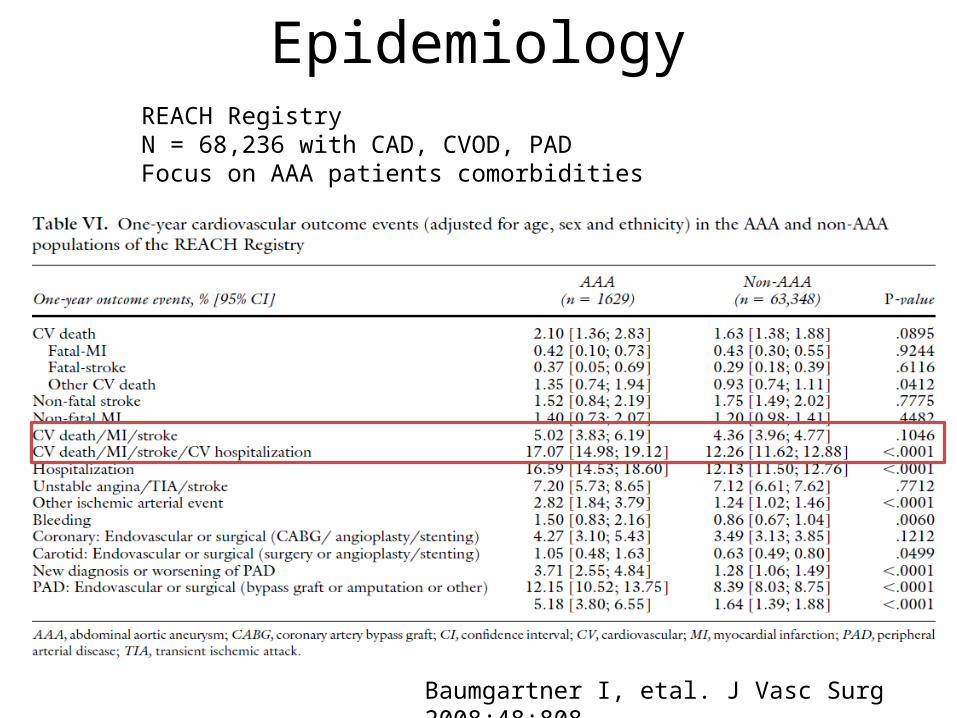
Epidemiology
Baumgartner I, etal. J Vasc Surg 2008;48:808
REACH RegistryN = 68,236 with CAD, CVOD, PADFocus on AAA patients comorbidities

Epidemiology
Baumgartner I, etal. J Vasc Surg 2008;48:808

Epidemiology
Bhatt, D, etal. JAMA 2010;304:1350
REACH RegistryN = 45,227 patients with CAD, CVOD, PAD or > 3 risks4 yr outcomeSig increased risk with DM (OR = 1.44); prior event (1.71); polyvasc Dz (1.99)

Atherothrombotic Costs
AHA statistics 2010
Heidenreich PA, etal. Circ 2011;123:933
It’s expensive!

Strong Evidence exists for Treating our Patients
• Anti-platelet therapy (ASA, IA)• Lipid mngt (LDL<100 mg/dL, IB) • HTN control (BP < 140/90 or 130/80, IB)
– RAAS (IA) and B-blockers (IA)• Smoking cessation (IB)• Fitness and weight mngt (IB)Smith SC, etal. Circulation 2006;113:2363

Medications: ASA
Meta-analysis of ASA for primary preventionN = 95,000
12% reduction in serious vascular events
ATT collaboration. Lancet 2009;373:1849
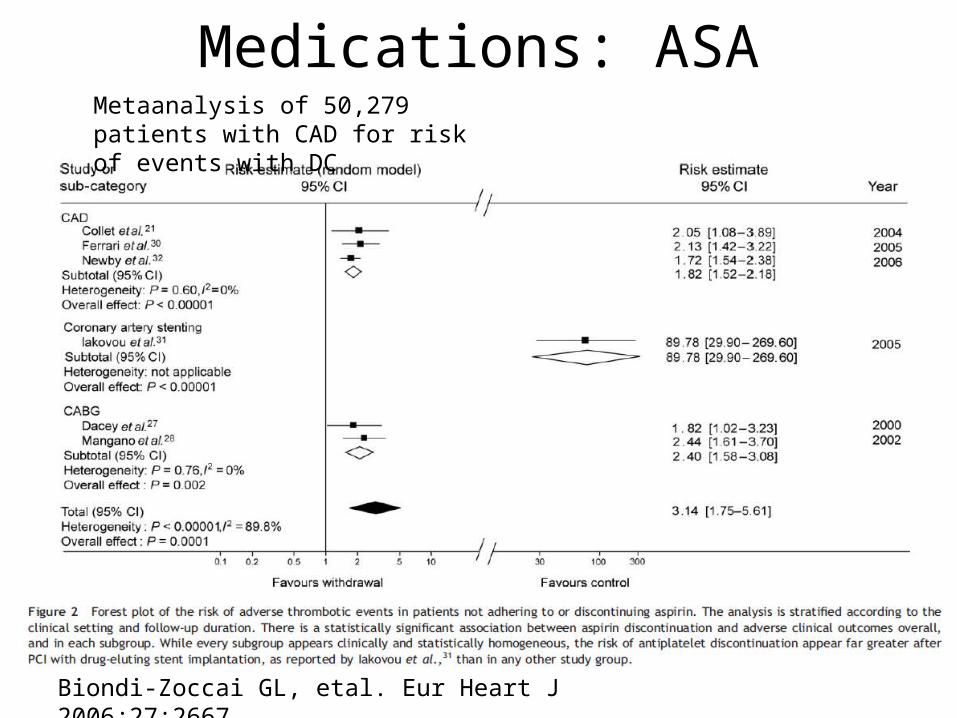
Medications: ASA
Biondi-Zoccai GL, etal. Eur Heart J 2006;27:2667
Metaanalysis of 50,279 patients with CAD for risk of events with DC

Medications: B-blockers
Adjusted Odds Ratio of In-hospital Mortality Associated with Beta Blocker Therapy in Major Noncardiac Surgery Stratified by Revised Cardiac Index (RCRI) Score
Lindenaeur PK, et al. N Engl J Med 2005;353:349-61
N= ~ 663,000Propensity matched cohort from 329 US hospitalsMajor non cardiac surgery

Medications: B-blockers
Bauer SM, etal. J Vasc Surg 2010;51:242

Medications: B-blockers
P<0.001
0 7 14 21 28Days after Surgery
Per
cen
tag
e o
f P
atie
nts
0
10
20
30
40
Standard care
Bisoprolol
N = 112High risk vasc surgeryBisoprolol 7-89 days pre-op (mean 37)
D(%) MI(%) p
CONT 17 17 0.02BIS 3.4 0<0.001
Poldermans D et al. NEJM 1999;341:1789

Medications: Statins
Bauer SM, etal. J Vasc Surg 2010;51:242

Medications: Statins
Schauten O, etal. NEJM 2009;361:10
N = 497 RCT, mean duration of use 37d
MI, Trop T was primary composite outcome
Decreased CRP, IL-6
All on b-blocker

Medications: Statins
Schauten O, etal. NEJM 2009;361:10

Medications: Statins
Kapoor AS, etal. BMJ doi:10.1136
Metaanalysis of ~800,000 pts for perioperative risk reduction effects

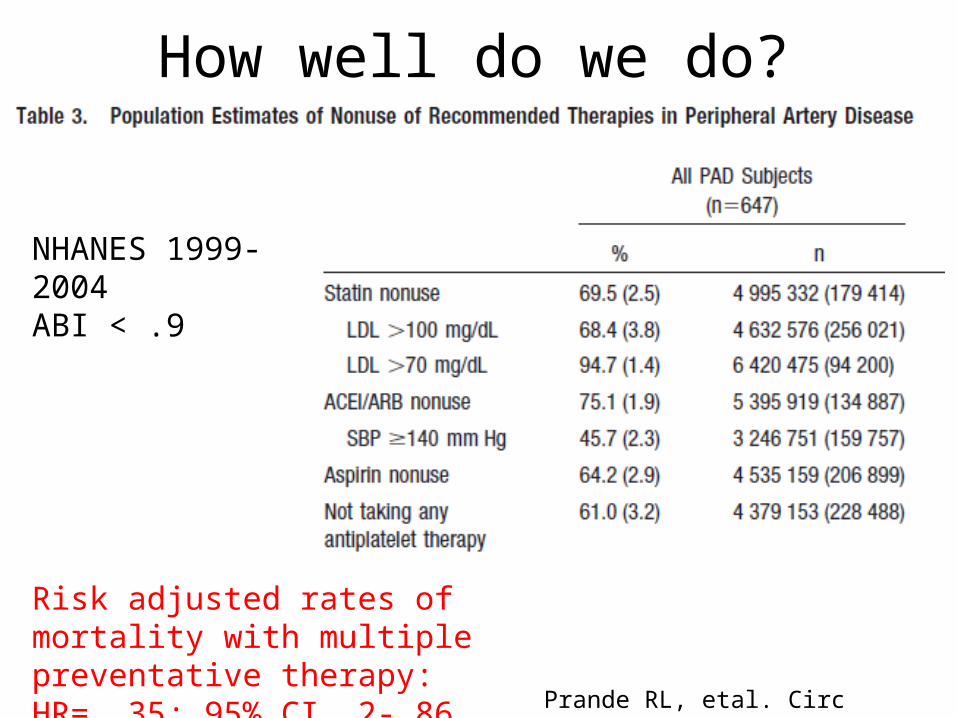
How well do we do?
Database study of 2839 patients with PADReviewed by ICD-9 codes, pharmacy, and labs
Rehring TF, etal. J Vasc Surg 2005;41:816

How well do we do?
Marchall C, etal. Vasc Endovasc Surg 2009;43:238
N = 325 vascular surgical patients
How well do we do?
Prande RL, etal. Circ 2011;124:17.
Risk adjusted rates of mortality with multiple preventative therapy: HR= .35; 95% CI .2-.86
NHANES 1999-2004ABI < .9

Post Op MI
Landesberg G, etal. Circulation 2009;119:2936

Post Op MI
Landesberg G, etal. Circulation 2009;119:2936
Well established guidelines
But are they actually followed?

Preoperative Evaluation
• Accepted and non-controversial indications for full cardiac w/u prior to surgery
Fleisher LA, etal. Circulation 2007;116:1971

Preop risk tools• RCRI
Lee TH, etal. Circulation 1999;100:1043

Preoperative Evaluation• Derived from VSGNE (N = 10,081)• Validated• More sensitive in vascular surgical patients
than RCRI
Bertges DJ, etal. JVS 2010;52:674

Preop Risk: Biomarkers
Choi JH, etal. Heart 2010;96:56
N = 2054 elective vascular surgery ptsPMCE = MI, pul. edema, deathRCRI improved
~ 20% on BB or statin

Preop Risk: Biomarkers
Owens CD, etal. JVS 2007;45:2
N = 91 LEB patientshsCRP, fibrinogen, SAAFU ~ 1 yr

Preop Risk: Biomarkers
Karthikeyan G, etal. JACC 2009;54:1599
Metaanalysis of 3,281 pts with perioperative CV complications

Preop Evaluation
Bauer SM, etal. J Vasc Surg 2010;51:242

Preop Stress testingMeta-analysis of 68 studies with N = 10,049LR = 8.35; 5.6-12.5 of po MI if positive
Beattie WS, etal. Anesth Analg 2006;102:8

Does preoperative stress testing help?
Falcone RA, etal. J Cardio Vasc Anesth 2003;17:694
N = 99RCT of preop stress test vs. none after AHA guideline stratification
No difference at one year; 1 % CV morbidity/mortality
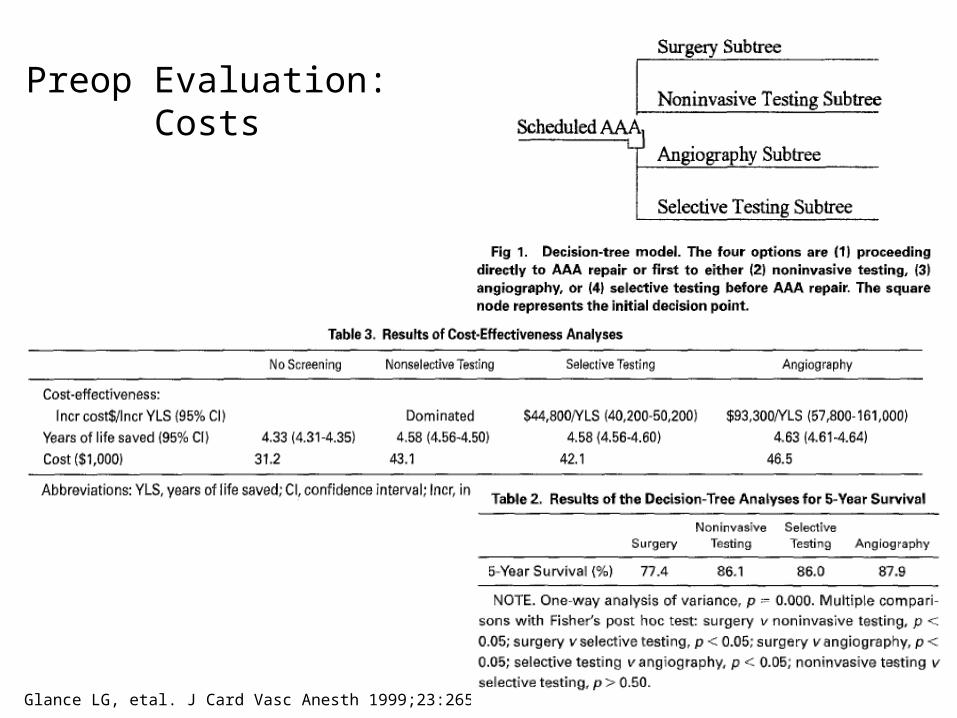
Preop Evaluation: Costs
Glance LG, etal. J Card Vasc Anesth 1999;23:265
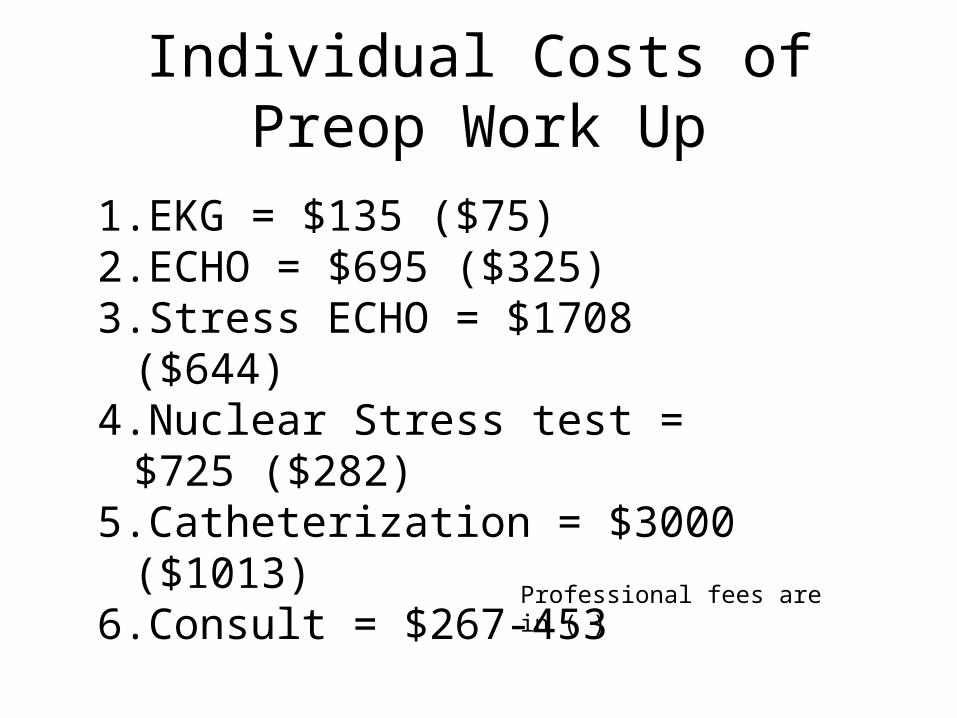
Individual Costs of Preop Work Up
1.EKG = $135 ($75)2.ECHO = $695 ($325)3.Stress ECHO = $1708 ($644)4.Nuclear Stress test = $725
($282)5.Catheterization = $3000 ($1013)6.Consult = $267-453
Professional fees are in ( )
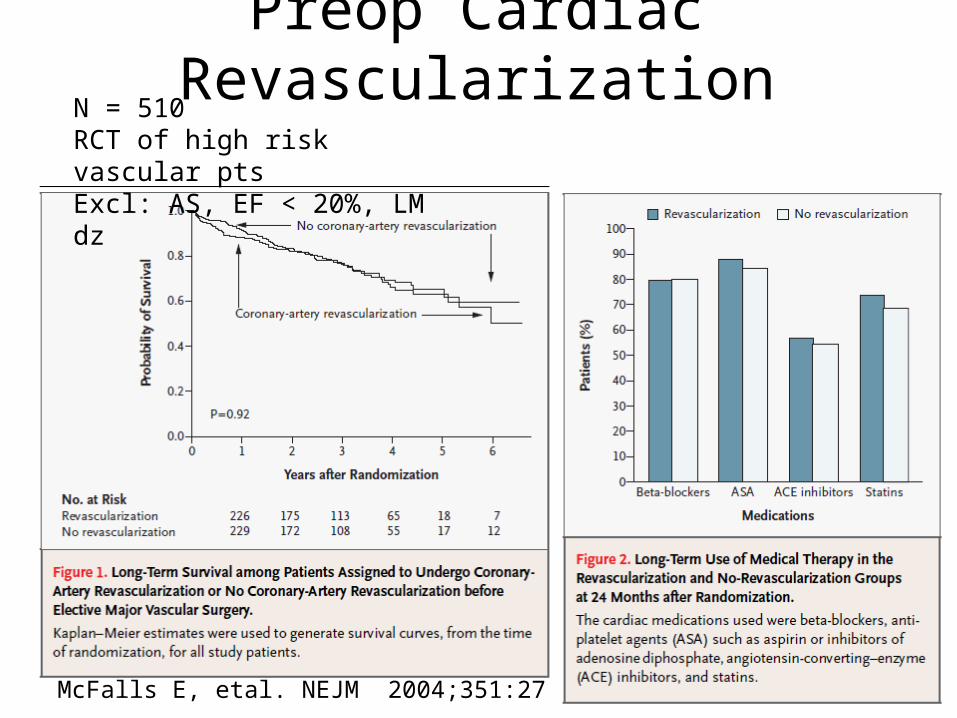
Preop Cardiac Revascularization
McFalls E, etal. NEJM 2004;351:27
N = 510RCT of high risk vascular ptsExcl: AS, EF < 20%, LM dz
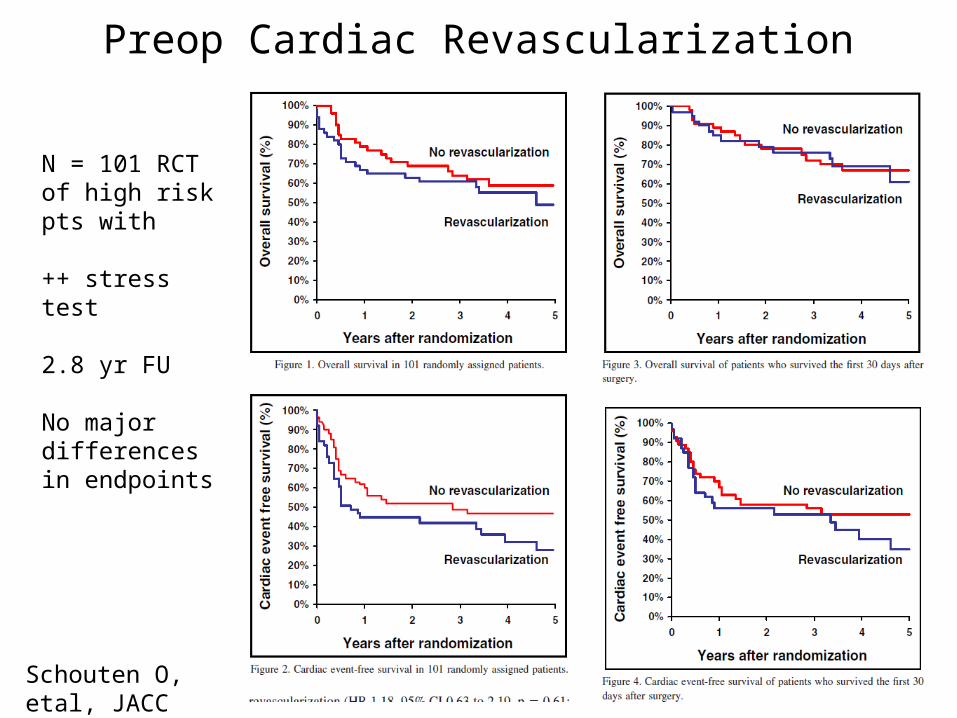
Preop Cardiac Revascularization
Schouten O, etal, JACC 2009;103:897
N = 101 RCT of high risk pts with
++ stress test
2.8 yr FU
No major differences in endpoints

Preop Cardiac Revascularization
Biccard BM , etal. Anesthesia 2009;64:1105

What probably doesn’t need study• Individual comparison of antiplatelet, statin, b-
blocker, and ACEI therapy in vascular disease patient outcomes– Evidence very strong from large CV trials, Registries,
Guidelines• Preoperative cardiac revascularization in vascular
surgical patients– Done twice; very intensive trials
• Antiplatelet therapy types for primary/secondary prevention

Current Relevant Trialswww.clinicaltrials.gov
• Predictors of po outcome in PV surgical patients• NCT01417910
• Cardiopulmonary exercise testing and preoperative risk stratification
• NCT00737828
• Prospective study to assess screening value of NT-proBNP for the identification of pts that benefit from additional cardiac testing prior to vascular surgery
• NCT00519961
• POISE-2 (ASA and clonidine)• NCT00144937

Current Relevant Trials
• Multifactoral Intervention on CV risk factors in subjects with PAD
• NCT00144937
• Multifactoral risk reduction for optimal management of PAD
• NCT00537225
• Vascular events in noncardiac surgery patients cohort evaluation
• NCT00512109

Potential Topics to Study• Preoperative cardiac risk stratification comparative study
– Risk equation and added biomarkers to increase pretest probability
– Preoperative stress testing usefulness• Postoperative MI care – heterogeneous
– Large multicenter survey / Study best practices• Intensive vs. usual cardiovascular medical care in high
risk arterial disease patients– GWtG/GAP paradigm for following AMI pathway – Active pathway intervention vs. simple recommendation
reminders– Steno II paradigm of multimodal intensive therapy for DM

GWtG
Lewis WR, etal. Arch Int Med 2006;168:1813

GAP
Eagle KA, etal. JACC 2005;46:1242

GAP
Eagle KA, etal. JACC 2005;46:1242

Steno-2 Model
• N = 160• RCT of intensive
multimodality therapy vs. usual care
• F/U ~ 8 yrs• Composite
endpoint of death, CV morbidity, amputation
Gaede P, etal. NEJM 2003;348:383

Steno-2 Model
Gaede P, etal. NEJM 2003;348:383

![Svs Agencies[1]](https://static.fdocuments.in/doc/165x107/577cc7a71a28aba711a191e1/svs-agencies1.jpg)