Medical Guidelines for PICU Seclusion Reviews

of 11
-
Upload
psychforall -
Category
Documents
-
view
215 -
download
0
Transcript of Medical Guidelines for PICU Seclusion Reviews
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
1/11
Review Article
Medical guidelines for PICU seclusion reviewsVishal Bhavsar1, Faisil Sethi2, Bradley Hillier3
1ST4, South London and Maudsley NHS Foundation Trust; 2Consultant Psychiatrist, South London andMaudsley NHS Foundation Trust; 3Locum ST4-6, South London and Maudsley NHS Foundation Trust
Abstract
Evidence regarding medical practice in seclusion is limited, and far outweighed by opinion. Here, wepresent one approach to medical reviews of patients in seclusion rooms, aiming to drive consistent practice.We address the work of clinicians prior to their arrival in the seclusion area, information-gathering prior to
entry into the seclusion room, relevant aspects of history-taking and mental state examination in theseclusion area, and the implications for clinical and risk-management. We discuss issues raised by thelogistics of seclusion for the planning and undertaking of the consultation. Physical examinations ofsecluded patients are commonly complicated by patient-related and environment-related factors; wesuggest a pragmatic approach to determining the scope of physical examination in seclusion. While riskassessments are a vital aspect of seclusion practice for psychiatrists, structured instruments for theassessment of risk within these environments do not exist. We lay out principles regarding risk assessmentin this population. We comment on the role of the clinician in the debrief phase of the seclusion review, anddeal with legal issues pertaining to seclusion in England. Ultimately, we are left with a number of questionsrelating to what constitutes best practice for psychiatrists fulfilling this role on the PICU.
KeywordsSeclusion; management; risk
INTRODUCTION
The management of psychiatric patients inseclusion is common (Mason, 1994; Beer et al.1997). Seclusion has been used throughoutmuch of recorded human history to contain
those suffering with mental disorder (Wells,1972). Evidence of the coverage of seclusionarrangements is greater in the West than in therest of the world, where data on the use ofseclusion is more patchy (Beer et al. 2008).Literature on seclusion broadly breaks down
into investigations of the legal and ethicalimplications of the practice, the examinationof the effects of seclusion on levels of violencein the inpatient setting, and the demographicprofiles of patient populations. In the UK,seclusion rooms are not located in every unit,
However, all wards will have the capacity totransfer patients to seclusion rooms in situtationswhere violence is uncontainable on the ward.While local, trust-based protocols are available,national guidance on clinical management ofsecluded patients is sparse. NICE guidance onthe management of violence notes that evidenceon the effectiveness of physical interventions,including seclusion, is limited (National Institutefor Health and Clinical Excellence, 2005).
Correspondence to: Dr Vishal Bhavsar, Pyschosis Clinical AcademicGroup, Maudsley Hospital, London SE5 8AZ. E-mail :[email protected]
Jc NAPICU 2013:00:111 1
Journal of PsychiatricIntensive Care
Journal of Psychiatric Intensive CareVol.00 No.0:111doi:10.1017/S1742646413000198Jc NAPICU 2013
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?- -
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
2/11
Guidance on what medical practitioners shouldbe doing during seclusion reviews is absent.Most advice on the medical management ofviolence relates to prescribing in acute beha-vioural disturbance, a concept known as rapidtranquillisation (RT). The other aspect of themanagement of severely violent behaviour is theuse of seclusion, which will be our concern inthis article.
No treatment of seclusion in any context canavoid discussion on whether seclusion can everbe justified. The pervasiveness of seclusionenvironments in psychiatric care indicates thatthis question should be approached carefully.The use of seclusion can be argued for in termsof consequentialist ethics (better consequencesarise from confining a violent patient comparedto not doing so), or evidence (the presence ofa seclusion area within a service reduces violenceor other negative outcomes). The lawfulnessof seclusion, and in particular the departure ofseclusion policy from the MHA Code of Practice,has been the subject of a number of legal casesheard by the Court of Appeal. Debates aroundthe moral and ethical justifiability of seclusion arelong, winding and parallel those that surroundpsychiatry itself. So, while seclusion raises ethicaland legal questions, in this article we will dealspecifically with the role of clinicians in the careof secluded patients.
DEFINITIONS
Definitions of seclusion have two components:the act of containment, and its purpose. Seclusionis usually defined as the restriction of a personalone in a locked room for the protection ofothers from significant harm (Beer et al. 2008).
The Code of Practice for the Mental HealthAct (Code of Practice: Mental Health Act 1983)forms the most authoritative source of guidanceon the use of seclusion. The Munjaz case(Munjaz v UK, 2012) established that departurefrom the Code was not lawful in the absence ofcogent reasons; in this case, the treating hospitalwas held to have acted unlawfully in deviatingfrom the Code in its seclusion policy. The Codedefined seclusion as the supervised confinement
of a service user in a room, which may be locked.Its sole aim is to contain severely disturbedbehaviour which is likely to cause harm toothers. While the ruling related to a case in ahigh-secure setting, it emphasised the principleof not deviating from the Code of Practicewithout cogent reason, and that in appropriatecircumstances the use of seclusion can be
justified. The Code calls for the ready availabilityof a nurse at all times, including the need for thephysical presence of a nurse with a patient whohas been sedated. The Code also refers to othertreatment models, such as therapeutic isolationand open supervised confinement, under thebanner of seclusion, indicating that these termsshould never be used to deprive patients of thesafeguards established for seclusion (Departmentof Health, 2008, para. 15.44).
Seclusion can be regarded as a group ofinterventions designed to contain acutely dis-turbed behaviour that exposes other patientsand staff to risk of serious harm. In this article,we focus on the review of patients being nursedin seclusion rooms; we will not consider otherinterventions for the management of acutelydisturbed behaviour such as time-out, zoning,nursing in the extra care area (ECA), therapeuticisolation, and open supervised confinement.Seclusion reviews tend to share a number offeatures. They usually follow violent incidents,and are accompanied by ongoing processes ofrisk assessment and incident management. Manyseclusion reviews take place out-of-hours, andclinicians called to attend reviews usually doso as part of out-of-hours work. The seclusionreview is among the first experiences manytrainee psychiatrists have of multi-disciplinarymanagement of acutely unwell patients. Theyare one of the few patient engagements in thepsychiatric hospital that are always undertaken
by a multi-disciplinary care team, rather than byone or two individuals.
The seclusion review will be focussed on theassessment of behaviour and mental state, and onan interview recalling a violent risk incident. Wedivide the process into the information gather-ing phase, the examination of mental state, theassessment of physical status, the assessment ofrisk and the debrief. We conclude by making
Bhavsar V et al
Jc NAPICU 2013:00:1112
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
3/11
some points about the psychiatrists role in teamdecision-making. Our approach is laid out inFigure 1.
A WORD ON LOGISTICS
A multi-disciplinary team (MDT) is defined as agroup of health workers, from varied profes-sional backgrounds, brought together to planand deliver coordinated health care interventionsfor patients with complex medical conditions.
The seclusion review team consists of a teamleader, usually an experienced psychiatric nurse,together with a reviewing clinician, a numberof other nurses, and occasionally health careassistants trained in control and restraint techni-ques. Given the limited evidence on seclusion,the practice of the MDT around seclusion seemsto vary greatly between, and possibly within,centres. Most policies describe a timetable forscheduling regular reviews of secluded patients,aiming to review the patients clinical state, andwhether criteria for seclusion continue to be
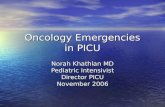
met. An example of a review schedule is shownin Figure 2; this presents a framework for thescheduling of senior reviews at regular intervals.The escalation of clinical reviews to clinical leadsor managers is not uncommon, particularly incases where seclusion continues for more than24 hours. In high secure forensic settings forexample, longer term seclusion is necessary for asmall group of patients. Staff on the review teamshould be appropriately trained and refreshed in
the practice of up-to-date physical interventionsfor the management of disturbed behaviour, andin emergency resuscitation techniques.
Seclusion reviews usually involve, in a step-wise fashion: an explanation to the patient ofwhat is about to happen; the entry into theseclusion room of the review team; the securingof the patient in holds; an explanation of whatwill happen next; the measurement of vitalsigns; the medical interview; the administrationof medication; the provision of food and drinkto the patient; a further explanation of what willhappen next; and finally the exit of the reviewteam from the room. There will then follow adiscussion amongst the members of the reviewteam about the appropriate course of action,a debrief, and a recording of events.
There are some points to be made aboutplanning and preparation. The team of profes-sionals identified to conduct the seclusion review,or the review team, would not usually beresident on the ward; arrangements should be
made to bring this team together in a timelyfashion (Department of Health, 2008, para.15.50). Levels of training in physical restrainttechniques are likely to vary within the team andwill influence discussions of who does what,when. Gathering information from the staff in acalm environment, away from the clinical area,usually proves beneficial. The individual roles ofthe members of the review team should be clearlyassigned in advance. If a face-to-face review is
Figure 1. (Colour online) The seclusion review process
Medical guidelines for PICU seclusion reviews
Jc NAPICU 2013:00:111 3
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
4/11
taking place, who will actually enter the room,and who will be responsible for securing thepatient in the relevant holds? Will a nurse conductan initial conversation with the patient, followedby the clinician, or will the clinician begin thediscussion? When is the physical examination totake place? Is the physical examination likely torequire assistance from another professional?Usually, the senior nurse will be responsible forthese decisions. The reviewing clinician will needto ensure that the patient has a clear grasp of thesematters before the review happens.
INFORMATION GATHERING
Professionals conducting seclusion reviews havea number of information-gathering skills at theirdisposal. Identifying the reason for the patientbeing in seclusion should be high amongst theconcerns: why have other approaches failed?Patients may have advance statements recordedin their clinical notes indicating a wish to benursed in a particular way, with respect tomedication and restraint. Decisions will need to
be made after taking into account factorsrelating to the patients general health. Forexample, pregnancy or haemodynamic compro-mise will have great implications for behaviouralmanagement, and the balance between physicaland pharmacological management of agitatedbehaviour. Other patient-related factors includecommunication impairments or language differ-ences, which can present barriers to effectivede-escalation techniques.
The reviewing clinician should note theinterventions that have failed and resulted intransfer to seclusion. Changes in the frequencyof periodic assessment of behaviour mental stateand risk by nursing staff (nursing observations)could reflect changes in the patients conditionover time. Typical management responses tobehavioural disturbance would be an increasedfrequency of nursing observations, or thecommencement of continuous face-to-faceobservations, or one-to-one. Increased obser-vations can involve unacceptable risks of harmto staff, with whom relationships with thepatient may have broken down. Changing aviolent persons status to continuous observa-tions by a single staff member requires anappropriate r isk assessment contingent on thenature and extent of violent behaviour, as well asthe characteristics of the ward and of theputative observer. Gathering background infor-mation on the patient and the reasons forseclusion should be done in a timely manner,and guided by evidence of risk to others, giventhat this is likely to be the main area forassessment.
The reviewing clinician should evaluate theward staffs emotional response to the patient,and to prepare themselves for what follows.Psychiatric intensive care units are emotionallycharged, highly active units where antagonismand aggression may be frequent, aspects whichcompound uncertainties regarding staffing andresource limitations. The social and affectivemilieu around the patient needs to be assessed
Initiation
30minutes
Hour2
Hour4
Hour6
Hour8
Hour10
Hour12
Hour14
Hour16
Hour18
Hour20
Hour22
Hour24
Nursing
ReviewJuniorMedicalReview
SeniorMedicalReview
ConsultantReview
Figure 2. Seclusion review pathway
Bhavsar V et al
Jc NAPICU 2013:00:1114
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
5/11
through discussions with the medical andnursing team, who are likely to display feelingsof anger, hopelessness, perhaps against abackground of declining morale. No healthprofessional reacts in the same way to a givenscenario, and the responses of the care team tothe patient will depend on the professionalsprevious experiences, gender, training and otherfactors. Team members often react in starklydifferent ways to a patient, leading to differentviews on what to do. On occasion, a teamappears divided, along disciplinary or otherlines, and this needs to be pointed out. Thereviewing clinician should take stock of theseresponses and the impact these are having onpatient care, in order to adopt an approach thatis as patient-centred as possible. The relationshipbetween the care team and the patient will beshaped by the patients personality; patients withborderline features may engender splits withinthe team, for example on the basis of gender orethnicity. Team members can begin to feelthemselves responsible for a patients situation; itis not uncommon for clinicians to interpret thesefeelings as a reflection of underlying projectivemechanisms emanating from the patient.
MENTAL STATE REVIEW
In this section we cover aspects of the mentalstate which are of particular significance duringseclusion reviews. The priority is to try to havesome sort of therapeutic engagement with thepatient. In dealing with the role of the mentalstate examination framework in reviewingsecluded patients, we are guided by four mainprovisions.
Firstly, it is unlikely that the mental stateexamination one carries out will be full in any
real respect. Experience suggests that most, ifnot all, mental state examinations are driven bya need to do the maximum that the patientwill tolerate, or the maximum which is safefor the multi-disciplinary team, without losingtherapeutic engagement. A certain amount offlexibility is necessary. Second comes thequestion of how representative the mental stateassessment will be of the underlying mentalillness (seclusions can cause high levels of distress
in and of themselves) mental state assessmentsundertaken in seclusion should be contextua-lised in this regard. Thus, much of the evidencefor a mental state review should derive fromobservations of behaviour and mental statusoutside the period of review itself. Thirdly, it isimpossible to disentangle the assessment ofmental signs and symptoms from the impactthat those have on the risk of violence. As such,we will refer frequently to the risk implicationsof certain mental phenomena.
Such discussions are a matter for conjecture tosome degree, and there are no hard rules, oreven, in many cases, good evidence. Finally,while the approach of a mental state examina-tion should be to investigate the reasons for apatients distress, this ought to be done from anempathic base, as an attempt to understand thepatients experience; in particular, care shouldbe taken to avoid focussing entirely on theincident, which will interfere with any usefulgathering of information on affect. Indeed, theclinician will have to negotiate a significantfeeling of injustice coming from the patient.
Appearance & behaviour
States of undress, or inappropriate dress, can
reflect the patients mental state and should havea bearing on care planning. Signs of physicalinjury and r ipped clothing related to previousviolence should be recorded. A good assessmentof a patients appearance and behaviour shouldincorporate an evaluation of aspects related tothe patients dignity, given the limitations totheir freedom.
Physical build should be noted, so as to guidethe assessment and management of violence;physically strong patients can warrant different
procedures by the review team. Restlessness andphysical arousal ought to be recorded; a patientwho cannot keep still is likely to pace aroundthe ward, make repeated demands and intrudeinto other patients affairs.
Behaviour should be assessed longitudinally aswell; a patient moving straight to the door toprevent the team from entering the room couldbe extremely fearful, or present risks to himself.
Medical guidelines for PICU seclusion reviews
Jc NAPICU 2013:00:111 5
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
6/11
Excretions in the seclusion room are notuncommon, and their intention and physicalcontext (constipation, infection and diet) shouldbe assessed; deliberate defecation in the seclu-sion room might be conceptualised as exertionof control in an environment where all controlhas been removed from the patient.
Mood and affect
The assessment of mood and affect in seclusioncan be straightforward; a threatening attitude,anger and hostility are common among secludedpatients. A key objective of the medical reviewshould be to identify how these phenomena arerelated to the violence that precipitated thetransfer into seclusion. Hostile, angry, externa-lising engagement over recent events on theward might be more comforting for a reviewingclinician than a withdrawn patient with whom itis difficult to have a conversation, although suchimpressions should be formed in the context ofthe patients known risk factors. The role ofanger in influencing violent behaviour shouldbe distinguished from other elements of themental state. On its own, anger is not necessarilypathological, and serves psychological functions,for example in motivating corrective beha-viours, facilitating persistence at relevant tasks,and aiding the expression of negative senti-ments. In epidemiological studies, anger ispredictive of violence before, during and afterpsychiatric admissions (Otto, 2000; Douglaset al. 1999).
As part of the mental state assessment of apatient at risk of being violent, the role of angershould be carefully clarified. Anger in psychoticdisorder for example, emerges secondary toparanoid delusions about others. Command
hallucinations to harm others have been associatedwith violence in some studies (Rogers et al.1990; Junginger, 1990); threat/control overridesymptoms, where a patient experiences a level ofthreat that overrides internal proscriptions toviolence, also raise the risk of violence duringpsychosis. In this regard, the reviewing clinicianshould assess the level of threat the patientexperiences on the ward, and how this changedduring the incident.
In assessing the relationship between mentalstate, anger and violence, the assessment ofpersonality traits is valuable. Personality featuresfrom the cluster B group of personality disorders(antisocial, borderline and narcissistic types) areparticularly relevant. Violence emanating fromanger as part of borderline personality organisa-tions requires consistent, highly structuredmanagement and careful attention to previousmanagement plans (National Institute for Healthand Clinical Excellence, 2009).
Attempts should be made to identify theeffect of seclusion on mood disturbance; is thepatient low in mood because of their confine-ment? Affective instability and the presenceof a fearful affect point towards the possibility offurther violence.
Speech
A patients speech should be assessed for featuresthat relate not only to the mental state (classicalformal thought disorder, or loud rapid speechthat maintains variations in tone and pitch), butalso to the risk of violence. Experience suggeststhat some patients choose to express anger inthe form of loud, abusive rudeness. Slurredspeech may indicate an overmedicated patient.
Communication which is impaired by formalthought disorder or by the side- effects ofmedication may render the patient vulnerable tofurther altercations with other unwell patients.
Perception
A patient who is distracted by disturbances inperception, with whom it is impossible toconverse, is more difficult to review. Behaviourconsistent with auditory hallucinations indicates
a need for a review of the diagnosis andmanagement plan. In particular the effects ofsuch psychopathology on behaviour should beassessed: does the patient look behind themfrom time to time, as if looking for the source ofhis experiences, or is he able to maintain hisfocus throughout the interview? Whilst data onthe link between command hallucinations andviolence is equivocal (McNiel et al. 2000;Rogers et al. 2002), such phenomena ought to
Bhavsar V et al
Jc NAPICU 2013:00:1116
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
7/11
be noted. Active psychosis, quite apart fromcommand hallucinations, displays an associationwith violence (Mullen, 2006).
Thought content
Delusional beliefs are a key feature of the mentalstate to be clearly ascertained. Screening fordelusional beliefs will be carried out duringhistory-taking from the patient about theincident(s) which led to the seclusion. However,an assessment of delusional belief should gobeyond identifying a falsely-held paranoid belief;assessment should be made of the extension ofthe belief into the patients life, including other,non-violent effects of the belief on the patientsbehaviour; for example, the avoidance of food
and water. Delusions involving other individuals,such as the patients family, peers on the ward, orthe ward staff have a bearing on risk assessmentand management planning. Thought contentassessment should also involve evaluation ofobsessional beliefs, over-valued ideas and beliefsrelating to the events which resulted in theinitiation of seclusion.
Orientation
The assessment of orientation in time, place andperson, as well as providing significant evidencefor the assessment of the patients mental stateand response to medications, offers the oppor-tunity for straightforward non-confrontationalexchanges with the patient, in contrast toquestions about paranoid ideas or bizarrepsychotic phenomena. Cognitive functioninghas a bearing on the aetiology of violence andrisks of further violent behaviour. For example,the misidentification of staff in the context ofdelirium should point towards a careful assess-
ment of their physical status, and urgenttreatment of the organic cause. In any case, thedifferential diagnosis of an organic confusionalstate should be noted and considered togetherwith the patients physical status. As in othersettings, the assessment of orientation should beapproached with care; direct, closed questioningof a secluded patient with do you know where
you are? may elicit an unintended and unhelpfulresponse.
Insight
The assessment of insight in seclusion can beapproached in two ways. On the one hand,elaborating the patients insight into the eventspreceding seclusion should reveal aspects relatingthe patients views of their condition, treatmentand their relationships on the ward. Alternatively,an approach which contextualises the triggerincident in wider issues, such as the patientslonger term state of mind, engagement withtreatment, and behaviour, could stand a greaterchance of maintaining engagement with thepatient. What is the patients understanding ofthe reasons for his admission, and for his transferto the seclusion? Having gathered the patientsaccount of the incident(s) that led to theseclusion, does he share the teams views on whathappened? Does the patient have alternativesuggestions for action, and how realistic are these?
The reviewing clinician should monitor theimpact of these discussions on the patients mentalstate; a patient who calmly gives his account andeven shows some appreciation of other possiblepoints of view, plainly displays healthier insightthat one who begins the interview calmly butwho becomes angry and agitated on discussion ofthe trigger incident. The patients view of eventsshould be recorded, as should his thoughts onhow treatment planning should proceed in thefuture. The ability to successfully undertake atwo-way dialogue in the seclusion room, howeverartificial it appears, is one of the few tests of socialfunctioning that is conducted with a patient inthis environment.
PHYSICAL EXAMINATION
The key question in driving the physical
examination should be: what is relevant and safeto do within the space, time and risk constraintsoffered by the seclusion review? Clearly none ofwhat follows can replace the exercise of clinical
judgement based on experience. However, it ispossible to suggest pointers for the exercise ofphysical assessments in seclusion. Firstly, at nostage should the physical safety of any member ofthe review team be compromised by the processof carrying out a physical; if a patient requires
Medical guidelines for PICU seclusion reviews
Jc NAPICU 2013:00:111 7
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
8/11
an abdominal examination urgently, then isseclusion the right place for them to be? Theinevitable limitation to the physical examinationmust lead to increased focus on ancillaryassessments of physical status.
Prior to entry into the seclusion area, notesand charts recording food and fluid intake andexcretions should be reviewed alongside thenursing notes describing the patients mental stateand behaviour. A secluded patient will usuallyhave had a series of vital signs taken at 2-hourlyintervals, which should be reviewed. A record ofmedicines administered in the previous 72 hourswill contextualise the assessment. It will benecessary to note results of any recent physicalinvestigations; for example, ECGs, blood tests,urine drug screens and the results of the mostrecent physical examination. Knowledge ofco-existing medical conditions, both arising fromthe violent incident and existing independently,will help to guide care planning.
Alertness should be assessed alongside acareful review of medicines administered bothregularly and as necessary, in order to assess boththe need for greater levels of anxiolysis tomanage violence, and the need for taperingmedicines because of unwanted sedation. Sleep
pattern should be assessed with this background,as should changes in libido. Given that secludedpatients are frequently the most medicatedpatients in the psychiatric hospital, seriousadverse effects, both long and short term needto be looked for carefully, alongside thetreatment chart. It is possible to carry out anassessment for most dystonias and respiratorydepression without touching the patient directly,if necessary. At the same time, managing apatient in seclusion should not stand in the wayof undertaking the physical health screening that
is routine for psychiatric in patients.
The first step for patients who refuse allcontact with the reviewing clinician, should beto encourage them to allow recording of theirphysical observations. The level of cooperationwith physical examination and investigations isan excellent indicator of the patients engage-ment; a patient who readily cooperates with acomplete physical and an ECG, for example, is
unlikely to warrant seclusion for much longer.As with any area of medicine, a more completephysical assessment involving history, examina-tion and investigations will reduce the index ofsuspicion around the patients condition.
Situations where a secluded patient becomesacutely and seriously medically unwell are notuncommon, but understandably occasion greatanxiety among reviewing clinicians. Decisionsregarding behavioural management, prescribingand consent become even more challenging onthese occasions. In general, three scenariospresent themselves. Where a patient is not fullycompliant with the physical review, and wherethere are no urgent concerns, the patient shouldbe reviewed regularly by the review as per localprotocols. Urgent review should be arrangedwhere new concerns about a patients physicalcondition arise. Where a patient is fully com-pliant with the physical assessment, but thereremains an indication for ongoing seclusion, thenregular reviews should proceed as normal, unlessnew urgent physical concerns emerge, whichshould bring about an urgent review. Finally, anypatient who requires immediate attention in anacute medical setting, including the emergencydepartment or ICU, should be transferred as soonas possible, after an assessment of their capacity toconsent to the management plan.
Finally, entering into some sort of conversationabout the future with the patient, usually towardsthe end of the review, is inevitable. Theseinterchanges should be tackled dispassionately;the patients views should be noted alongsidethose of the team in order to formulate themanagement plan.
RISK ASSESSMENT
As with any risk assessment in psychiatry,assessing risk in seclusion rests on certainassumptions. For example, it is assumed that itis possible to predict future behaviour on thebasis of known facts about the case and theconsistency of an individuals behaviour overtime. Risk assessment tools like the HCR-20emphasise historical risk items. However, itwould be wise to remember that a persons
Bhavsar V et al
Jc NAPICU 2013:00:1118
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
9/11
behavioural strategies change over time, and apersons response to circumstances ten years agomay not necessarily be the same as in the present,particularly in light of therapeutic interventions.Structured methods for the assessment of riskin seclusion do not exist to our knowledge.However, structured risk assessment instrumentsfor inpatient units usually score previous violencein terms of severity, include violence towardsproperty as well as to the person, and generate anoverall score at the end.
We recommend that a sensible risk assessmentin seclusion should proceed in a similar fashionto other situations in the intensive care unit; inother words, taking account historical andcurrent risks, and static together with dynamicfactors. Recent incidents of violence shouldbe recorded and understood in terms ofprecipitants, triggers, contexts, alleviating andexacerbating factors, and so on. Violent inci-dents precipitating seclusion may be analysedusing an ABC technique, by noting antecedentsto violence, the behaviour itself and theconsequences for the patient, in order to assesswhether possible antecedents remain, and there-fore evaluate the potential for further violence.It is likely that a secluded patient has beenviolent already. Given this, acute managementin seclusion will probably not result in theelimination of all risk. In particular, the patientmay display behaviours which present real risksto himself, for example head banging (in thecontext of psychosis, a disorder of personality, ora protest at his containment).
Risky behaviour can persist despite the bestefforts of the care team and the environmentalsafety interventions. Despite the increasedprocedural, physical, and relational securityoffered by the seclusion room, there remains
the potential for ligatures and sharp blades tobe concealed and brought into the room andused to inflict self-harm, damage to theseclusion room itself and cause harm to others.In situations where substance misuse has beenidentified as a trigger for an escalation ofaggressive behaviour, the seclusion review oftenaffords the first opportunity for assessment forintoxication and withdrawal. The seclusionreview can also be useful as an arena for the
assessment for the side-effects of increasing dosesof psychotropic medication. Further, removingthe patient from the open ward could allow asafer investigation into the procedures andpolicy that led to the incidents, where relevant.
It will be necessary to review how the patienthas coped and behaved in the context ofinstitutional containment and seclusion and con-finement in the past. Formulating risk in terms ofnature (risk of what), extent (how big is the risk),direction (risk to whom or what), alleviating andexacerbating factors, and contingencies for the riskbeing realised, is useful. The scheduling of regularseclusion reviews should form an active part of themanagement of risk, offering an opportunity forregular review of treatment, and of concordancewith treatment plans. The seclusion review cycleshould also provide a structure for seeking theopinions of colleagues.
Given the key role of information quality informing a good impression of risks, assessing thepatients engagement with interview is especiallyrelevant; the accessibility of the patients internalworld must be commented upon, to give an ideaof how reliable the risk assessment might be.Potential victims of violence should also beconsidered. If there was a victim involved inprevious aggressive behaviour, is that person atrisk currently and how might this risk bereduced, for example by outward transfer toanother ward? Patients with cognitive impair-ment, challenging behaviour, or limited socialskills should be regarded as especially vulnerable.
THE DEBRIEF
The above sections (information gathering,mental state assessment, physical assessment, risk
assessment) will not be addressed purely insequence; in practice these will occur in parallel.At the conclusion of the seclusion review, adiscussion, or debrief, should take place amongthe multi-disciplinary team. In our experience,it is most helpful to separate the emotional,transference-oriented debrief part of the discus-sion from the decision making part to avoidfrank mixture of the emotional responses andthe decision making process itself. The clinician
Medical guidelines for PICU seclusion reviews
Jc NAPICU 2013:00:111 9
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
10/11
should feel able to comment on counter-transference processes occurring within thereview team. Jagarlamudi et al. (2012) pointedout that such responses are common onintensive care units. The care teams experiencesof intense feelings of inadequacy, frustration,and anger around a secluded patients careshould be commented upon, where relevant.
For the clinicians themselves, discussing theiremotional responses to the patient under reviewwill also be beneficial; the clinician should be ableto comment on transference/counter-transferenceexplanations for the responses of the reviewteam to the patient, and the patients behaviour.Of course, it is also possible that members ofnursing staff may have experience of comment-ing on interpersonal dynamics and transference
issues, but this should not be assumed. Thediagnosis and effects of treatment should bereviewed in this setting.
THE TERMINATION OF SECLUSION
Discussions during the review will tend torevolve around whether seclusion should beterminated or not. Where a decision is made by
the review team that the patient no longermeets criteria for being cared for in seclusion,the decision to end may be relayed to the patientvia any member of the review team. It is oftenappropriate to instigate a step-down manage-ment plan, which could constitute a period ofintermittent observations, a segregation plan toa particular section of the ward, or a behaviouralcontract. Making a decision to end seclusionmust be done as a team, and appropriate spacemust be given to contrary views, and to those ofprofessionals who may have particular experi-ence of that patient, or of the particular factorsinvolved. No decision should be made withouttaking into account background factors thatmay not be patient-related; for example: has thenursing staff composition changed to a morefavourable one; are there more staff available
now, so that step-down to 2:1 observations ispossible and safe; has the patient populationchanged, so that further altercations are muchless likely? Finally, it is often wise to trial thetermination of seclusion, where appropriateprocesses have been followed, where re-initiationof seclusion is easily available. The serial failure ofseclusion and other measures to reduce violenceshould lead to consideration of onward referral tolow secure or forensic services.
Date and Time of Medical review with MDT:
Name of patient (DOB):
PICU admission date:
Date and time of initiation of seclusion:
Indications for initiation of seclusion:
Nursing Report pre-review:
Mental State Examination:Physical status:
Risk assessment:
MDT discussion:
Diagnosis and current concerns:
Need for ongoing seclusion:
Impression of clinical and risk management:
PLAN
1. Decision and termination
2. Step-down planning3. Medication changes4. Physical monitoring/care
5. Risk monitoring6. Liaison (family, nursing team, police/legal, social worker, second
opinions, collateral sources)7. Note time frame for the next review
Figure 3. An example format for the documentation of seclusion reviews
Bhavsar V et al
Jc NAPICU 2013:00:11110
-
7/28/2019 Medical Guidelines for PICU Seclusion Reviews
11/11
DOCUMENTING THE SECLUSIONREVIEW
Clear, consistent and thorough documentationof the encounter is pivotal in a setting whererisk issues predominate, where the multi-disciplinary team changes frequently with shiftpatterns, and where complex decisions need tobe made. In Figure 3 we lay out one example ofhow a seclusion review might be documented.Such a framework could also be used in theform of an electronic document.
CONCLUSIONS
In reality, on-call clinicians will arrive in theseclusion area with a number of competing
considerations to do with patient care, resources,staff safety, and the management of their ownanxiety, fear and workload. The circumstances,no matter how much structured knowledgethey enter the situation with, will be dynamicand require considerable flexibility. Factors willbe in play that the on-call clinician will knownothing about, not being part of the regularclinical team. How to behave clinically in thisscenario, particularly when more junior, may bea subject of some worry for core trainees. It ishoped that the framework presented here
provides a starting point for approaching thesescenarios in a structured, safe, and patient-centred way. We are reminded that the evidenceon which we base our practice in this area islacking on a number of levels; from the utility ofseclusion in general, to the appropriateness ofseclusion in given patient scenarios, to compre-hensive risk assessments, to the paucity of dataon the right way to do things in seclusion, andremains a central area for future research inpsychiatric intensive care units. Instruments forthe formal assessment of risk to others inseclusion have not been tested, and currentseclusion policies appear to rely on commonsense rather than empirical evidence. For thetrainee, discussion of seclusion reviews inclinical supervision and Balint groups shouldguide the development of clinical experience inthis area of mental health inpatient work.
References
Beer, M.D., Paton, C. and Pereira, S. (1997) Hot beds of
general psychiatry: a national survey of psychiatric intensive
care units. Psychiatric Bulletin. 21(3): 142144.
Beer, M.D., Pereira, S.M. and Paton, C. (2008) Psychiatric
Intensive Care, 2nd edition. Cambridge University Press, 369 pp.
Department of Health. (2008) Code of Practice: Mental Health
Act 1983. TSO, London. http://www.lbhf.gov.uk/Images/
Code%20of%20practice%201983%20rev%202008%20dh_
087073%5B1%5D_tcm21-145032.pdf
Douglas, K.S., Ogloff, J.R., Nicholls, T.L. and Grant, I.
(1999) Assessing risk for violence among psychiatric patients:
the HCR-20 violence risk assessment scheme and the
Psychopathy Checklist: screening version. Journal of
Consulting and Clinical Psychology. 67(6): 917930.
Jagarlamudi, K., Portillo, G. and Dubin, W.R. (2012)
Countertransference effects in acutely disturbed inpatients.
Journal of Psychiatric Intensive Care. 8(2): 105112.
Junginger, J. (1990) Predicting compliance with commandhallucinations. American Journal of Psychiatry. 147(2): 245247.
Mason, T. (1994) Seclusion: an international comparison.
Medicine, Science and the Law. 34(1): 5460.
McNiel, D.E., Eisner, J.P. and Binder, R.L. (2000) The
relationship between command hallucinations and violence.
Psychiatric Services. 51(10): 12881292.
Mullen, P.E. (2006) Schizophrenia and violence: from
correlations to preventive strategies. Advances in Psychiatric
Treatment. 12(4): 239248.
Munjaz v UK (2012) 2913/06 MHLO 79 (ECHR).
National Institute for Health and Clinical Excellence.
(2005) Violence: The short term management of disturbed andviolent behaviour in inpatient psychiatric settings and emergency
departments. Clinical Guideline 25. NICE, 83pp.
National Institute for Health and Clinical Excellence
(2009) Borderline Personality Disorder: Treatment and management.
Clinical Guideline 78. London: NICE.
Otto, R.K. (2000) Assessing and managing violence risk in
outpatient settings. Journal of Clinical Psychology. 56(10):
12391262.
Rogers, P., Watt, A., Gray, N.S., MacCulloch, M. and
Gournay, K. (2002) Content of command hallucinations
predicts self-harm but not violence in a medium secure unit.
The Journal of Forensic Psychiatry. 13(2): 251262.Rogers, R., Gillis, J.R., Turner, R.E. and Frise-Smith, T.
(1990) The clinical presentation of command hallucinations
in a forensic population. American Journal of Psychiatry.
147(10): 13041307.
Wells, D.A. (1972) The use of seclusion on a university
hospital psychiatric floor. Archives of General Psychiatry. 26(5):
410413.
Medical guidelines for PICU seclusion reviews
Jc NAPICU 2013:00:111 11