Medical emergencies in dental practice
21
EMERGENCY PREPAREDNESS AND MEDICAL EMERGENCIES IN DENTAL PRACTICE - AN INTENSIVIST‘S PERSPECTIVE Dr Vaidyanathan.R Consultant anaesthesiologist and intensivist CAUVERY HOSPITAL MYSORE
-
Upload
vaidyanathan-r -
Category
Health & Medicine
-
view
191 -
download
2
Transcript of Medical emergencies in dental practice

EMERGENCY PREPAREDNESS AND MEDICAL EMERGENCIES IN
DENTAL PRACTICE- AN INTENSIVIST‘S PERSPECTIVE
Dr Vaidyanathan.R Consultant anaesthesiologist and intensivist
CAUVERY HOSPITALMYSORE
PREPAREDNESS• Medical emergencies are rare in dental practice
though not uncommon.• Studies show that anywhere from 19% to 44% of
dentists had a patient with a medical emergency in any one year.
• Most of these complications,approximately 90% were mild but 8% were considered to be serious.
• It was found that 35% of the patients were known to have some underlying disease.

contd• OVER 50% of the emergencies were syncope with
hyperventilation the next most frequent at 7-8 %.
• Allergic reactions,angina pectoris/myocardial infarction/ACS
• Cardiac arrest, postural hypotension, seizures, bronchospasm and diabetic emergencies.
• ALL these constitute less than 1%.
PREVENTION IS BETTER • Anticipate potential emergency and act
appropriately
• Prevention and preparedness is the key.
• Accomplished by a thorough medical history appropriate alterations to dental treatment as required
• Patients should be asked to bring their medications to each dental appointment in case of an emergency *( Eg nitrates, salbutamol inhaler,etc)

contd• All dentists should have basic BLS skills.
• All personnel in dental OPD should preferably be trained in BLS and know basic handling and management of ABCs in emergencies.
• Emergency kit and drugs should be there in all offices, clinics and procedure rooms
• Enroll and organise RRT IN bigger hospitals.

Emergency kit and drugs• Oxygen - 100%, Ambu bag (BMV), LMA• Salbutamol – preferably inhalers.• Epinephrine /ADRENALINE• Sorbitrate tablets• Acetylsalicylic acid (ASA) 160 or 325 mg)• Hydrocortisone• Diphenhydramine (inj.avil)• Sugar cubes 1 or 2 cubes• Atropine,Ephedrine,BZDs(midaz/loraz)morphine.

RAPID RESPONSE TEAM(RRT)• RRT is a designated group of healthcare personnel who can be
assembled quickly to deliver critical care expertise in response to grave clinical deterioration of a patient located outside a ICU
THE TEAM :• Physician – senior resident / intensivist/ hospitalist• Physician’s assistant• Clinical nurse specialist/CCN• Respiratory therapist
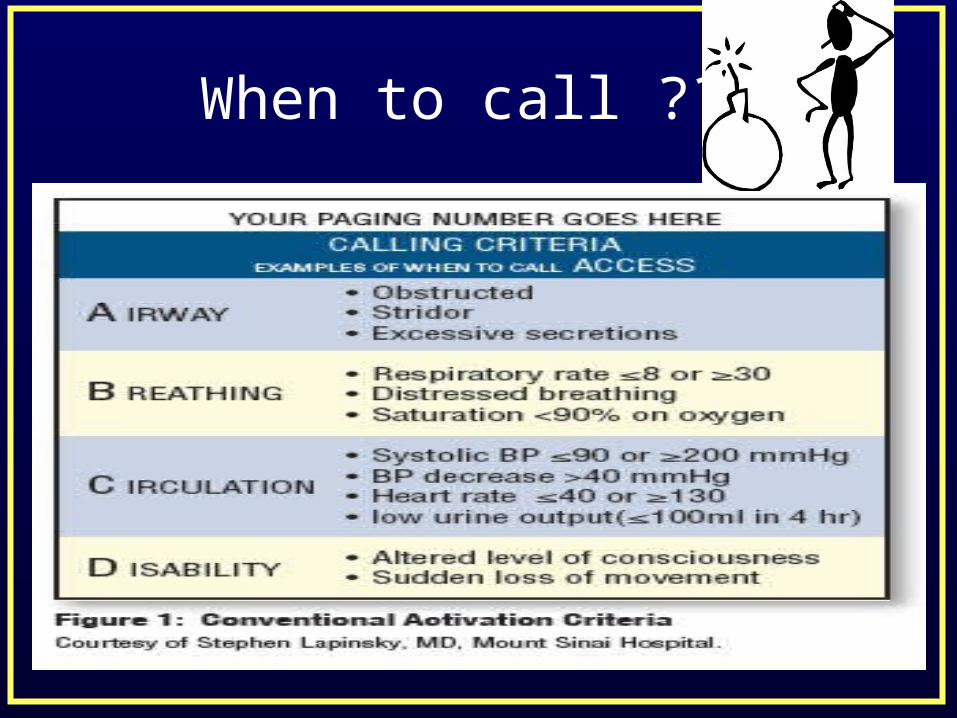
When to call ??

contd
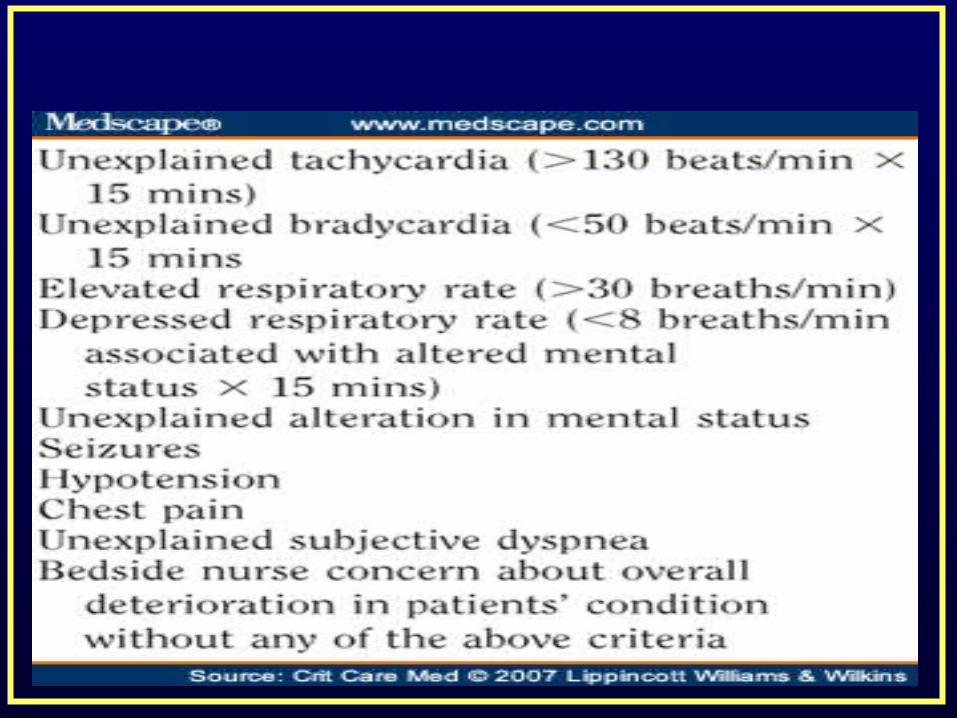
contd

The acute conditions…..• SYNCOPAL ATTACK :
• Commonest. More than 50% of all emergencies.• Predisposing factors– fear,anxiety,sight of blood.• Often has a prodromal phase-light headedness,dizzy..• Classical feature is bradycardia and hypotension.• Self limiting.Rarely aggressive therapy indicated• Stop the procedure. Supine position. Legs elevated.
Administer oxygen. Assess ABCs.
HYPERVENTILATION SYNDROME :
• Characterised by rapid and deep breathing often more than 25 breaths per min
• Anxiety and fear common predisposing factors.• All vital signs-HR,BP,RR often elevated.• Tingling ,numbness , perioral anesthesia• Symptoms of hypocalcemia-twitching,carpopedal
spasm,tremors .• Treatment : upright position,loosen clothing,
rebreathing into cupped hands or paper bag.

Anaphylaxis /severe allergy• Patient experiences sinking feeling,intense itching,
flushing over face and chest.• Rhintis,conjunctivitis,nasea,vomiting,cramps,palpitations
,tachycardia,substernal tightness,wheezing and dyspnea.• Pale looking. Severe hypotension /cardiac arrest.• Supine position. Assess ABCs• TRY TO ESTABLISH IV LINE AND START IV
FLUIDS.• INJ Avil 25 mg iv stat. inj hydrocortisone 100 mg iv /im.
Inj adrenaline 1in 10000 im/sc.• Inj adrenaline 1 in 1000 iv in severe cases.
Local anaesthetic overdose
• Patient experiences - Agitation,confusion,excitement,talkativeness,slurred speech, twitching and tremors.
• Head ache,visual disturbances and flushed feeling. • Numbness of tongue,tingling and numbness of
perioral region.• Drowsiness and rarely seizures.• Reassurance,im midazolam 1 or 2 mg increase upto
5mg if seizures occur.• CPR if cardiac arrest.

ADRENALINE OVERDOSE
• Anxiety,fear, restlessness,throbbing headache ,tremors
• Rapid and bounding pulse,perspirations.• Elevated BP• Treated by reassurance• Semi sitting or upright position• Midazolam 1 or 2 mg im.
Acute severe asthma.
• Earlier called status astmaticus.• Precipitation of severe acute bronchospasm in
known patients.• Breathlessness,audible wheeze, rhonchi,cyanosis in
severe cases.• Administer oxygen. Salbutamol inhalation 2 puffs
repeated every 5-10 min.• Inj hydrocortisone 100mg iv• Inj adrenaline 1in 10000 sc/im in refractory cases.
Angina/chest pain/MI/ACS
• Sudden onset chest tightness ,heaviness ,chest pain or breathlessness.
• Predisposed in elderly ,DM, HT,smoking or previous history of MI/CVA/IHD
• Upright position, 100% oxygen,Aspirin 325 mg. sorbitrate 10 mg sublingually.
• Shift to cardiac centre.• Administer morphine and clopidogrel if available.• CPR if cardiac arrest.

Seizures.• Predisposing factors are known
epileptics,pediatric patients, old CVA• Local anaesthetic toxicity• Assess ABCs.• Supine position.• Administer midazolam im 3-5mg or lorazepam 2-
4mg• Assess airway again and administer 100%
oxygen.• Plan for shift

Diabetic emergencies.• Hypoglycemia ; Light headedness, tremors ,sweating drowsiness ,
rarely unresponsiveness. Prdisposed in elderly,starving ,OHA s Managed by sugar cubes orally repeated till
symptoms revert. Hyperglycemia Predisposed in acute infections,poor diet compliance
and binge eatingNo specific signs except in DKA/NKHCPlan to shift.

TIAS, CVAs• Present similar to syncopal attack• More prolonged phase of unresposiveness or altered
sensorium.• Accompanied by slurred speech,weakness of one or
more limbs, deviation of angle of mouth.• Rarely presents with seizures,abnormal laboured
breathing.• Assess ABCs..• Place in supine.Give 100% oxygen. • Need to differentiate b/w bleed or embolism.
THANK YOU