![[PPT]Cheek and Onion Cell Lab - BellevilleBiology.combellevillebiology.com/worksheets/Cells/CellLabs/Cheek and... · Web viewCheek and Onion Cell Lab Biology ONION CELLS Cheek Cells](https://static.fdocuments.in/doc/165x107/5ae5344c7f8b9a495c8f9dba/pptcheek-and-onion-cell-lab-andweb-viewcheek-and-onion-cell-lab-biology-onion.jpg)
MEDICAID – CONTEXT FOR CHANGE Mike Cheek Vice President, Medicaid and Long Term Care Policy.
23
MEDICAID – CONTEXT FOR CHANGE Mike Cheek Vice President, Medicaid and Long Term Care Policy
-
Upload
vanessa-rhymer -
Category
Documents
-
view
216 -
download
0
Transcript of MEDICAID – CONTEXT FOR CHANGE Mike Cheek Vice President, Medicaid and Long Term Care Policy.

MEDICAID – CONTEXT FOR CHANGE
Mike Cheek
Vice President, Medicaid and Long Term Care Policy

Executive Summary
Fiscal Pressures are Driving the Dialogue States are Restructuring Financing, Delivery
Systems and Government to Slow Cost Growth Centers for Medicare and Medicaid Services
has a Wide Array of Activities Underway and Planned that will Impact Long Term Care Providers
On the Horizon are Congressional Concepts Aimed at Slowing Cost Growth
Considerations for Long Term Care Professionals focus on Rapidly Changing Medicaid Landscape and Opportunities Related to Coordinating Services for People Eligible for Medicare and Medicaid (duals)

Fiscal Pressures are Driving the Dialogue
Fiscal Pressure

Medicaid is the Largest Single Share of Federal Funds to States
Source: National Association of State Budget Officers, 2009 State Expenditure Report, December 2010

Costs are Driving the Medicaid Reform Dialogue
$0
$100
$200
$300
$400
$500
$600
$700
$800
$900
$1,000
State Medicaid
Federal Medicaid
Source: Centers for Medicare and Medicaid Services Office of the Actuary – National Health Expenditure Projections 2010 – 2020
Federal Stimulus Funds Begin
Federal Stimulus Funds End
Affordable Care Act Expands Eligibility

States are Restructuring Financing, Delivery Systems and Government to Slow Cost Growth
State Restructuring

States Budgeted for Little Medicaid Growth
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
4.1%3.4%
4.7%
6.8%
8.7%
10.4%
12.7%
8.5%7.7%
6.4%
1.3%
3.8%
5.8%
7.6%6.6%
7.3%
2.2%
Economic Downturn (2000-2003)
Welfare Reform, Managed Care
Part D
Economic Downturn and End of Enhanced FMAP (2008 – 2012)
Total Medicaid Spending Growth, FY 1996 – FY 2012
Source: KCMU Analysis of CMS Form 64 Data; KCMU survey of Medicaid officials conducted by Health Management Associates, 2011

Common State Savings Strategies
Provider reimbursement Eligibility and enrollment process Copays and premiums Benefits LTC and HCBS Prescription drug utilization and cost control
initiatives Managed Care Program Integrity Health Information Technology Duals Integration Efforts

Affordable Care Act Efforts are Mixed
010203040
Definitely Plan Not to PursueUnder ConsiderationDon't KnowDefinitely Plan to Implement
Source: Cheek, M., et. al., On the Verge: The Transformation of Long-Term Services and Supports. AARP Public Policy Institute (February 2012)
Num
ber
of
Sta
tes

Managed LTC is a Systems Used in Lieu of Fee For Service
Capitated MMLTC Medicaid agency and contractors enter into agreement
under which contractor accepts risk of providing defined Medicaid LTC services
Alternative types of MMLTC capitation packages: Medicaid-covered LTC services only All Medicaid-covered acute and LTC services All Medicare and Medicaid-covered services
(additional plan contract with CMS required for Medicare portion
ManagedCareContractor
ManagedCareContractorCapitated
Payment
StateMedicaidAgency
StateMedicaidAgency
ProvidersProviders
NegotiatedPayments(FFS, Per Diem, etc.)
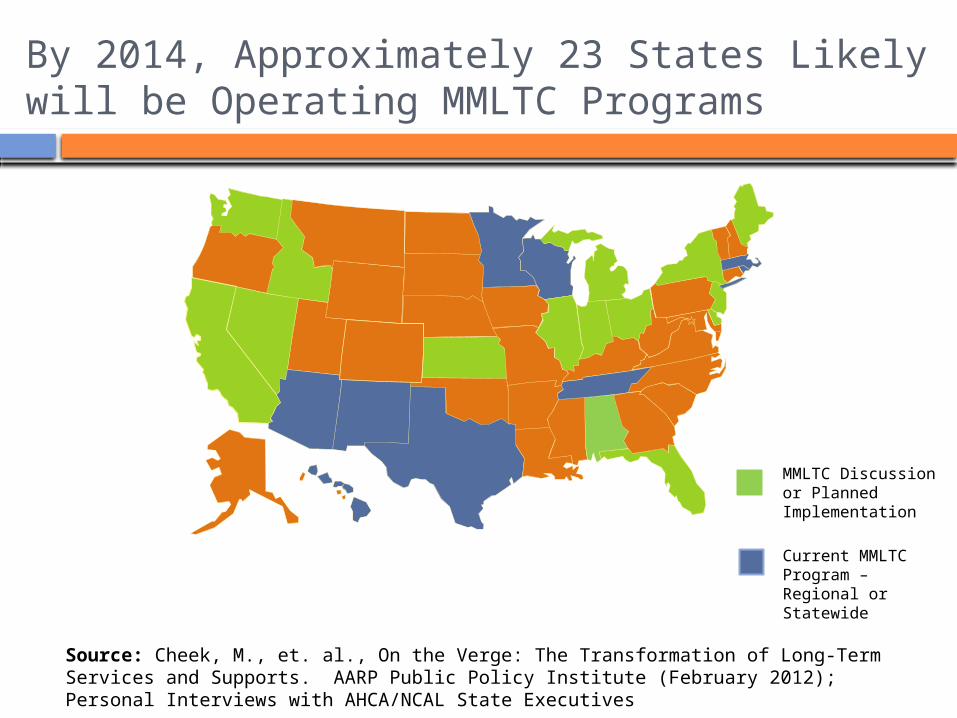
By 2014, Approximately 23 States Likely will be Operating MMLTC Programs
Source: Cheek, M., et. al., On the Verge: The Transformation of Long-Term Services and Supports. AARP Public Policy Institute (February 2012); Personal Interviews with AHCA/NCAL State Executives
MMLTC Discussion or Planned Implementation
Current MMLTC Program – Regional or Statewide

State Government is Downsizing
Less Than 5%
Between 6% and
10%
Between 11% and
15%
Between 16% and
25%
More than 25%
0
5
10
15
20
25
30
35
20092011
Perc
en
t of
Sta
tes
Percentage of State Staff Eligible for Retirement by Percent of Total FTESource: Cheek, M., et. al., State of the States Survey 2011 – State Aging and Disability
Agencies in Times of Change. National Association of States United for Aging and Disabilities

CMS has a Wide Array of Activities Underway and Planned that will Impact Long Term Care Providers
Centers for Medicare and Medicaid Services (CMS)

CMS Disabled and Elderly Health Programs Group Expanded its Purview

Duals are a Significant area of Focus because of Costs and Acuity
0%
40%
80%
120%
79% 64% 85%61%
21% 36% 15%39%
DualsNon-Duals
Source: Kaiser Family Foundation, The Role of Medicare for People Dually Eligible for Medicare and Medicaid (January 2011)

New CMS Divisions
Center for Medicare and Medicaid Innovation Health Care Innovation Challenge funding Innovation advisors program
Medicare-Medicaid Coordination Office State Demonstrations to Integrate Care for Dual Eligible
Individuals Medicare Data for Dual Eligibles for States Initiative to Align the Medicare and Medicaid Programs Financial Models to Support State Efforts to Integrate Care
for Medicare-Medicaid Enrollees Reducing Preventable Hospitalizations Among Nursing
Facility Residents Integrated Care Resource Center Available to All States
AHCA Staff and Members Actively Been Working with These Offices

In Terms of ACA Options, States are Most Heavily Focused on Duals
Letter of Intent – Both Models
Demo Design
Capitation
MFFS** Managed Fee-for-Service (MFFS)
Both a Demo Design and Letter of Intent

Other Core CMS Activity Themes
Medicaid Program Integrity Reshaping Medicaid Managed Care Health Information Technology New Medicaid Data Systems Preparing for 2014 Home and Community-Based Services
Expansion using Affordable Care Act and other options

On the Horizon are Congressional Concepts Aimed at Slowing Cost Growth
Congress

Block Grants Have Re-Emerged Currently, states draw down federal
Medicaid dollars on a quarterly basis based on expenditures
Under a Block Grant, states would receive some form of a fixed dollar amount and would be required to manage to that dollar amount

Incremental Change may Occur First
New state Medicaid program authorities to coordinate financing and services for people eligible for both Medicare and Medicaid
Increased Medicaid program integrity efforts Further trimming of state capacity to draw
down additional federal dollars Provider Taxes Intergovernmental Transfers
Enhancement of state flexibility

Implications

At the End of the Day, Owner/Operators Should Consider …
Partnering with other segments of the health care sector on efforts to better coordinate services to people who are eligible for Medicare and Medicaid
Highlighting the value of CCNC as a viable option to Managed Long Term Care
Exploring opportunities to tap any new health information technology funding the state may leverage
Monitoring Medicaid cost containment activity Program integrity Specialized Medicaid authority to make changes not
normally allowable Monitoring continued emphasis on Home and
Community-Based Services

















![Cheek to cheek [jazz] - Free- · PDF fileHe was also a student in jazz interpretation from 1992 until ... About the piece Title: Cheek to cheek [jazz] Composer: ... piano, upright](https://static.fdocuments.in/doc/165x107/5a727ae17f8b9a98538d9d52/cheek-to-cheek-jazz-free-scorescomwwwfree-scorescompdfenanonymous-cheek-to-cheek-58125pdfpdf.jpg)