Medicaid/Medicare Integration: Opportunities for States & Dual Eligibles

Medicaid and Managed Care:
Missouri and a National Perspective
for
MO HealthNet Oversight Committee
April 30, 2015
Vernon K. Smith, PhD
Health Management Associates © 2015
0

Medicaid and Managed Care: Missouri and a National Perspective
• Where Medicaid is now and how it got here – the trends driving the program across states:
– Growth in health costs, insurance premiums, health insurance coverage, the uninsured
• Medicaid enrollment and spending growth, before and after the ACA.
• State strategies for controlling spending.
– Why the big Medicaid story of 2015 is delivery and payment system reforms
– Why states increasingly rely on MCOs.
1

2
“Medicaid coverage is …
“… extremely valuable to the low-income families and individuals who qualify for the services provided by the program.”
“… valuable to society at large, as it enables the least-fortunate members of the population to obtain the health care they need in an orderly way.”
– CMS, Actuarial Report on the Financial Outlook for Medicaid, 2014.

The Value and Impact of Medicaid Is Shown in Many Studies
– Improves access to medically needed care
– Improves health status
– Improves financial security
– Improves school performance and the productivity of current and future workforce
– Benefits medical providers, especially safety net hospitals and community health centers
– Lowers cost of health insurance for business
– Adds economic activity and jobs
– Saves state general funds in mental health, others
– Operates efficiently, very low administrative costs

Employer-Sponsored 172 million
48%
Medicaid 70 million 20%
Medicare 54 Million 15% Private
20 Million 6%
Uninsured 28 million 8%
CHIP 6 million 2%
Source: HMA estimates 2015.
Insurance Status of Americans, 2015 Medicaid: The Nation’s Largest Single Health Program

[VALUE] [VALUE]
$1,080
[VALUE]
$345
Medicaidand CHIP
Medicare PrivateInsurance
DOD, VA,IHS, Others
Out ofPocket
20%
11%
Note: Medicaid includes $15 billion for CHIP. Source: HMA estimates for 2015.
Medicaid is a Significant Payer for Medical Care: U.S. Health Expenditures, by Payer, 2015
2015 U.S. Health Spending: $3.2 Billion
17%
34%
19%
In $Billions

U.S. Medicaid Spending Trend: 2000 to 2015
$203
$317
$355
$521 $560
2000 2005 2010 20152013
$450
6
Note: Includes Medicaid and CHIP enrollment. Source: HMA, based on CMS, Office of the Actuary, 2015.
$Billions: All State and Federal Funds

General Fund Spending for Medicaid and K-12 Education, as Percent of All GF Spending:
All States and Missouri, FY 2014 35.0%
19.1%
34.9%
21.9%
K-12 Education GF Medicaid GF
All States
MO
All States
MO
Source: HMA, based on: National Association of State Budget Officers, State Expenditure Survey, 2014. 7

Total Spending on Medicaid and K–12 Education as % of Total State Spending
Average State Percentages, 2008 – 2014
22.0%
20.0% 19.9% 19.5% 20.5%
23.7%
24.4%
25.8%
19%
20%
21%
22%
23%
24%
25%
26%
2008 2009 2010 2011 2012 2013 2014
Medicaid
K-12 Education
8
Source: HMA, based on data in: NASBO, State Expenditure Report, 2014 and Earlier Years.

Medicaid Spending Now Averages 26% of Total State Budgets
8%
13%
20%
26%
1985 1990 2000 2014
1985 - 2013
9
Source: HMA, based on NASBO, State Expenditure Report, 2014 and earlier years.
Total Medicaid Spending,
as % of Total State Spending,
Average across all states,
And Missouri for 2014.
U.S. MO
31%

What Are the Key Factors Driving Growth In Medicaid Spending?
• Rising health care and insurance costs
• Downward trend in employers offering health insurance
• Upward trend in the number of persons uninsured

Health Insurance Premiums (Reflecting Medical Costs) Have Increased Much Faster than Inflation and Earnings
Cumulative Percent Increases 1999-2014
191%
54%
43%
0%
50%
100%
150%
200%
250%
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Health Insurance Premiums
Workers' Contribution toPremiums
Workers' Earnings
Overall Inflation
212%
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2014. Bureau of Labor Statistics, Consumer Price Index, U.S. City Average of Annual Inflation (April to April), 1999-2014; Bureau of Labor Statistics, Seasonally Adjusted Data from the Current Employment Statistics Survey, 1999-2014 (April to April).
1999 to 2014: Avg. Annual Growth Premiums = 7.9% CPI = 2.4%
10 11

$15,073*
$13,770*
$13,375*
$12,680*
$12,106*
$11,480*
$10,880*
$9,950*
$9,068*
$8,003*
$16,834*
$16,351*
$7,061
[VALUE]
$5,791
$5,429*
$5,049*
$4,824
$4,704*
$4,479*
$4,242*
$4,024*
$3,695*
$3,383*
$3,083*
$2,689*
$2,471*
$2,689
$2,471
$2,196
$0 $2,000 $4,000 $6,000 $8,000 $10,000 $12,000 $14,000 $16,000 $18,000
2014
2013
2012
2011
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999Single Coverage
Family Coverage
$5,615*
Premiums Up 70% Over Last Decade: Average Annual Premiums for Single and Family Health Insurance Coverage
1999-2014
• indicates estimate is statistically different from estimate for the previous year shown.
• Source: Kaiser/HRET, Employer Health Benefit Survey, 2014.
$15,745
12

$6,199
$9,580
$11,995
$15,073
2000-01 2004-05 2008-09 2012-13
Family Premiums
Source: HMA, based on: State Health Access Data Assistance Center, “State-Level Trends in Employer-Sponsored Insurance,” 2015.
Missouri Health Insurance Premiums Growth Parallels National Trend
2000 - 2013

As Premiums Increase, Fewer Firms Offer Coverage: Share of U.S. Firms Offering
Health Insurance: 2001 and 2013 68%
58% 57%
45%
All U.S. Firms Small Firms (3 - 9 Employees)
2001 2013 2001 2013
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2013.
14

Missouri Workers with Employer Sponsored Insurance Also Dropping
75%
63%
2000 2011
15
Source: HMA, based on: State Health Access Data Assistance Center, “State-Level Trends in Employer-Sponsored Insurance,” April 2013. Includes workers and dependents.

37
50 48 47 46
2000 2010 2011 2012 2013
Uninsured Increased by 13 Million 2000 – 2010, but dropped since 2010, primarily due to ACA
Millions of U.S. Uninsured
Source: HMA, prepared from: U.S. Census Bureau and CMS NHE projections, 2013.
13 16

Uninsurance Rate for Adults Dropped to Historic Lows Across All States in 2 years, from 2013 to 2015
Source: Sharon K. Long, et al., “Taking Stock: Gains in Health Insurance Coverage under the ACA as of March 2015,” Urban Institute, April 16, 2015
“The uninsured rate among U.S. adults declined to a record low since Gallup began tracking it in 2008.” --Gallup, April 13, 2015.

15 Million adults Gained Coverage Sept. 2013 to March 2015, as Un-Insurance Rate Dropped by 43%
17.6% 15.8%
20.7%
10.1%
7.5%
14.4%
0%
5%
10%
15%
20%
25%
All StatesDecrease of 43%
States ExpandingMedicaid
Decrease of 53%
States Not ExpandingMedicaid
Decrease of 31%
Percentage of Adults With No Health Insurance, Sept. 2013 and March 2015
Sept. 2013 Mar-15
18
Source: Sharon K. Long, et al., “Taking Stock: Gains in Health Insurance Coverage under the ACA as of March 2015,” Urban Institute, Health Policy Center, April 16, 2015

U.S. Medicaid Enrollment Trend: 2000 to 2015
37
50
56
64
72 76
30
35
40
45
50
55
60
65
70
75
80
2000 2005 2010 20152013
+28%
19
Note: Includes Medicaid and CHIP enrollment. Source: HMA, based on CMS, Office of the Actuary, 2014 and prior years.
Millions of Enrollees
+35% +19%
ACA

Missouri Medicaid Enrollment Trend 2001 – 2014
500
1000
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
877,000
718,000
745,000
824,000
20
Source: Health Management Associates, based on data compiled by HMA for the Kaiser Commission on Medicaid and the Uninsured. 2000 – 2005 from “Medicaid Enrollment: June 2012 Data Snapshot,” August 2013.; 2006 – 2013 from “Medicaid Enrollment: June 2013 Data Snapshot,” January 2014. http://kff.org/medicaid/issue-brief/medicaid-enrollment-june-2013-data-snapshot/ June 2014 estimated by HMA.
Note: Includes only Full-Benefit Medicaid. Does not include CHIP or Partial Benefit, e.g., Family Planning

6%
8%
3%
1%
-17%
-1%
5% 4%
5%
1%
-1% -2% -5%
5%
9%
6%
4% 3%
0% -1%
3%
8% 7%
4% 3% 3%
9%
6%
-20%
-10%
0%
10%
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
NOTE: Enrollment percentage changes from June to June of each year.
SOURCE: Medicaid Enrollment June 2013 Data Snapshot, KCMU, 2014. FY 2014 - 2015 data based on KCMU survey of Medicaid officials in 50 states and DC conducted by Health Management Associates, 2014.
Missouri Annual Medicaid Enrollment Growth Has Been Much Lower Than U.S. Average
Annual Percent Changes FY 2002 – FY 2014
Missouri
U.S.

“Non-Expansion” States Have Still Seen Growth in Medicaid and CHIP Enrollment
4.7%
10.5%
-6%
4%
14%
Ne
bra
ska
Ala
ska
Uta
h
Wy
om
ing
So
uth
Da
ko
ta
Mis
sou
ri
Ok
lah
om
a
Lo
uis
ian
a
Vir
gin
ia
Te
xa
s
Wis
con
sin
Ka
nsa
s
Ala
ba
ma
Flo
rid
a
So
uth
Ca
roli
na
Mo
nta
na
Mis
siss
ipp
i
Ge
org
ia
Ida
ho
No
rth
Ca
rolin
a
Te
nn
ess
ee
Percent Change in Medicaid/Chip Enrollment From Pre-ACA (July - Sept. 2013) to January 2015
22
Note: Maine data omitted by CMS because data not comparable to other states.
OURCE: CMS, “Medicaid & CHIP: January 2015 Monthly Applications, Eligibility Determinations, and Enrollment Report,” March 20, 2015
Missouri = 2.1% Average of These States = 7.8%
15.2%
2.1%

“Expansion” States: Medicaid and CHIP Enrollment Growth Avg. of 26%
8%
19% 25%
34%
47%
0%
20%
40%
60%
80%
100%
Iow
a
Dis
tric
t o
f C
olu
mb
ia
Ha
wa
ii
Ne
w Y
ork
Ve
rmo
nt
Mic
hig
an
Illin
ois
Min
ne
sota
Ari
zon
a
Ma
ssa
chu
sett
s
Oh
io
Ne
w J
erse
y
Ca
lifo
rnia
Ne
w H
am
psh
ire
Ma
ryla
nd
Rh
od
e Is
lan
d
Wa
shin
gto
n
We
st V
irg
inia
Ark
an
sas
Ne
w M
ex
ico
Co
lora
do
Ne
vad
a
Ore
go
n
Ke
ntu
cky
Percent Change in Medicaid/Chip Enrollment From Pre-ACA (July – Sept. 2013) to January 2015
82%
23
Note: Connecticut excluded because of missing data. Indiana (6.9%) and Pennsylvania (4.5%) excluded due to 2015 implementation.
SOURCE: CMS, “Medicaid & CHIP: January 2015 Monthly Applications, Eligibility Determinations, and Enrollment Report,” March 20, 2015.
Average = 26.1%

169 171 173
21 28 32 51
56 63
64 81
84 45
23 23
2013 2016 2020
Uninsured
Medicaid
Medicare
Other
Employer
Source; HMA, based on CMS, Office of the Actuary, 2014.
U.S. Health Coverage Changes: 2013 – 2020 Number Uninsured To Drop by Half
Millions of Americans

169 171 173
21 28 32 51
56 63
64 81
84 45
23 23
2013 2016 2020
Uninsured
Medicaid
Medicare
Other
Employer
Source; HMA, based on CMS, Office of the Actuary, 2014.
U.S. Health Coverage Changes: 2013 – 2020 Employer – Based Insurance Up Slightly
Millions of Americans

169 171 173
21 28 32 51
56 63
64 81
84 45
23 23
2013 2016 2020
Uninsured
Medicaid
Medicare
Other
Employer
Source; HMA, based on CMS, Office of the Actuary, 2014.
U.S. Health Coverage Changes: 2013 – 2020 Medicaid to Increase by 20 million by 2020
Millions of Americans

How Are States Responding to Need to Control Medicaid Spending?
• A Focus on Improving Quality, Controlling Costs and Increasing Value
– Focus on high-need, high cost populations, including persons with chronic conditions, disabilities, in LTC and on both Medicaid and Medicare (dual eligibles)
– Quality improvement: strengthening contract requirements for health plans, pay-for-performance, special initiatives e.g., on non-emergency ER use.
– Cost savings through managed care, delivery system and payment reforms, payment restrictions.
27
SOURCE: Vernon Smith, et al., “Medicaid in an Era of Health & Delivery System Reform: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2014 and 2015,” Kaiser Family Foundation, October 2014.

Missouri Medicaid Has Used Several Strategies to Improve Care, Control Cost
Cost and enrollment growth are well below national trends
– Controls on benefits and eligibility
– Focus on program integrity
– National model for Health Homes
– Increasing use of managed care, with new contract requirements for MCOs and patient incentives
28

Nationally, Delivery System and Payment Reforms are a Priority for Medicaid in 2015
– Focus on improving care, cost and outcomes for high-need, high cost populations
• Managed care, care management, coordinated and integrated care, often using State Innovation Model (SIM) grants or Delivery System Reform Incentive Payment (DSRIP) waivers.
• Payers are strengthening contractual requirements for health plans, with Pay-for-Performance, withhold incentives based on performance, auto – assignment algorithms, other initiatives, e.g., non-emergency ER use.
SOURCE: Vernon Smith, et al., “Medicaid in an Era of Health & Delivery System Reform: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2014 and 2015,” Kaiser Family Foundation, October 2014.
29

24
12
5 5
31
17 14
6
10
30
20
26
10
19
40
PCMH ACA Sec. 2703Health Home
ACO Initiative Dual EligibleInitiative
Any DeliverySystem Initiatives
In Place in FY 2013 New/Expanded in FY 2014 New/Expanded in FY 2015
NOTE: Expansions of existing initiatives include rollouts of existing initiatives to new areas or groups and significant increases in enrollment or providers. Dual Eligible Initiatives include those through and outside CMS financial alignment demonstration. SOURCE: Vernon Smith, et al., “Medicaid in an Era of Health & Delivery System Reform: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2014 and 2015,” Kaiser Family Foundation, October 2014.
Delivery System Reforms to Coordinate Care and Control Costs Are in Most States in 2014 - 2015
30

31
The Need for Effective Systems of Care for an Aging Population Is Seen in Increasing Share of
Population Age 65+
7% 8%
9% 10%
12% 13% 13% 13%
17%
20% 21%
1940 1950 1960 1970 1980 1990 2000 2010 2020 2030 2040
Source: U.S., Administration on Aging.
Compared to health costs for a 40-year-old: Ages 65-74, are 3X higher Ages 75 + are 5.65X higher

5
20
6
22
6
18
9
23
GeographicExpansions
Eligibility GroupExpansions
NewMandatoryEnrollment
Any ManagedCare
Expansions
Actions to Expand Managed Care
FY 2014 FY 2015
SOURCE: Vernon Smith, et al., “Medicaid in an Era of Health & Delivery System Reform: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2014 and 2015,” Kaiser Family Foundation, October 2014.
33 34
ManagedCare
Expansions
QualityInitiatives
Policy Changes in Either Year
In FY 2015, States Continue to Expand and Improve Managed Care.
32

33
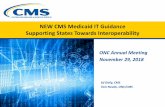
In 2011, Half of U.S. Enrollees Were in MCOs, but Most Dollars Were Not
Share of Medicaid Enrollees and Dollars in Managed Care: (LTC and Dual Eligibles Account for Large Share of FFS Dollars)
50%
24%
45%
14%
Enrollees $$ Enrollees $$
U.S.. Missouri
FFS
Note: Managed care includes risk- and non-risk based, including MCOs, PCCMs, and limited benefit plans. Data are for 2011. Source: HMA, prepared from data in: MACPAC, Medicaid and CHIP Program Statistics, June 2014.

34
Share of Missouri Medicaid Dollars in Managed Care, by Eligibility Group, 2011
14%
47% 43%
0.2% [VALUE]
All MO $$ Children Adults Disabled Aged
.
FFS
Note: Managed care includes risk- based MCOs. Data are for 2011. Source: HMA, prepared from data in: MACPAC, Medicaid and CHIP Program Statistics, June 2014.

Conclusion: Significant Changes Are Occurring in Medicaid
• Innovations with payment and delivery system initiatives, greater use of managed care and care management, to achieve greater value for state tax dollars.
• Managed care is the platform for accountability for better care, access, quality and health outcomes, and for saving costs.
– Priorities involve care for all Medicaid groups, including persons with disabilities and chronic conditions, long term care, and dual eligibles.

Medicaid Can Make a Significant Difference
“We are unashamed to use the power of Medicaid to raise the standard of care for all the citizens of our state.”
-- State Medicaid director, describing
initiatives in his state.