
Med_ Px with Diseases of Respi System
7
Reasons for Consultation: Symptoms Abnormal chest X-ray Both Approach: 1. History 2. P.E. With good clinical diagnosis, you may be able to manage your patient and give proper diagnosis and therapy. CLINICAL HISTORY A good clinical history should have the ff info: Most prominent symptom - chief complaint Temporal Profile - is it acute, chronic, progressive etc. Inventory of substances that can harm the lungs - inorganic substances (asbestos, silicone) - occup/envi exposure should be at least more than a year. Personal habits - Smoking - Sticks/packs per day, how long is the patient smoking Pharmacologic agents - Taking of anti-hypertensive drugs (ACE inhibitor) Family history - Carcinoma - Asthma Common Respiratory Complaints -common but not specific A. Shortness of breath / dyspnea B. Cough C. Hemoptysis D. Chest pain ( pleuritic ) - be able to eliminate diseases according to its time course - if your patient has an acute symptom, then your line of questioning and diagnosis should target acute respi diseases. Acute (<3 weeks) Sub-acute (3-8 weeks) Chronic (>8 weeks) Pattern of presentation Exacerbation and remission -asthma Progressive - COPD Triggers -Allergies (weather, allergen, dust, smoke etc) Causes of Acute Dyspnea Laryngeal edema or acute asthma - Usually caused by an allergy - Sudden onset Acute cardiogenic or non-cardiogenic pulmonary edema Bacterial pneumonia Pneumothorax pulmonary embolus - Sudden onset Example: Male patient, thin, tall, plays basketball, no risk factors. Suddenly experiences dyspnea. Suspect pneumothorax. Causes of Sub-acute Dyspnea Asthma Mycobacterial or fungal pneumonia Noninfectious inflammatory process - Autoimmune Disease - SLE Neuromuscular diseases - Myasthenia Gravis Pleural diseases - Pleural Effusion - Pneumothorax due to COPD or Chronic PTB Causes of Chronic Dyspnea Asthma Subject: Medicine Topic: Approach To Patient With Diseases Of Respiratory System Lecturer: Dr. Jacob P. Singh Date of Lecture: 14 Sept 2011 Transcriptionist: Teriyaki and Sushi Pages: 6 S Y 2 0 1 1 2 0 1 2
-
Upload
inaki-delos-santos-ramos -
Category
Documents
-
view
218 -
download
0
Transcript of Med_ Px with Diseases of Respi System

8/4/2019 Med_ Px with Diseases of Respi System
http://slidepdf.com/reader/full/med-px-with-diseases-of-respi-system 1/6
1
Reasons for Consultation:
Symptoms
Abnormal chest X-ray
Both
Approach:
1.
History2. P.E.
With good clinical diagnosis, you may be able to
manage your patient and give proper diagnosis
and therapy.
CLINICAL HISTORY
A good clinical history should have the ff info:
Most prominent symptom
- chief complaint
Temporal Profile
- is it acute, chronic, progressive etc.
Inventory of substances that can harm the
lungs
- inorganic substances (asbestos, silicone)
- occup/envi exposure should be at least
more than a year.
Personal habits
-Smoking
- Sticks/packs per day, how long is the
patient smoking
Pharmacologic agents
- Taking of anti-hypertensive drugs (ACE
inhibitor)
Family history
- Carcinoma
- Asthma
Common Respiratory Complaints
-common but not specific
A. Shortness of breath / dyspnea
B. Cough
C. Hemoptysis
D. Chest pain ( pleuritic )
A. DYSPNEA
Time course
- be able to eliminate diseases according to
its time course
- if your patient has an acute symptom, then
your line of questioning and diagnosis
should target acute respi diseases.
Acute (<3 weeks)
Sub-acute (3-8 weeks) Chronic (>8 weeks)
Pattern of presentation
Exacerbation and remission -asthma
Progressive - COPD
Triggers -Allergies (weather, allergen,
dust, smoke etc)
Causes of Acute Dyspnea
Laryngeal edema or acute asthma- Usually caused by an allergy
- Sudden onset
Acute cardiogenic or non-cardiogenic
pulmonary edema
Bacterial pneumonia
Pneumothorax pulmonary embolus
- Sudden onset
Example: Male patient, thin, tall, plays
basketball, no risk factors. Suddenly
experiences dyspnea. Suspectpneumothorax.
Causes of Sub-acute Dyspnea
Asthma
Mycobacterial or fungal pneumonia
Noninfectious inflammatory process
- Autoimmune Disease
- SLE
Neuromuscular diseases
-Myasthenia Gravis
Pleural diseases
- Pleural Effusion
- Pneumothorax due to COPD or
Chronic PTB
Causes of Chronic Dyspnea
Asthma
COPD
Pleural effusion
-long-term due to malignancy
Subject: MedicineTopic: Approach To Patient WithDiseases Of Respiratory SystemLecturer: Dr. Jacob P. Singh
Date of Lecture: 14 Sept 2011
Transcriptionist: Teriyaki and SushiPages: 6
S Y
2 0 1 1 - 2 0 1 2

8/4/2019 Med_ Px with Diseases of Respi System
http://slidepdf.com/reader/full/med-px-with-diseases-of-respi-system 2/6
2
Diffuse interstitial fibrosis
Pulmonary vascular disease
Pulmonary thromboembolic disease
Left ventricular failure
Severe anemia
Postintubation tracheal stenosis
- Patients on a long-term mechanical
ventilator
B. COUGH
Causes:
Pulmonary
- Acute / chronic infections of the lungs
- Inflammatory disorders
Tumors
- Airway obstruction
Foreign bodies
Cardiovascular
- Pulmonary congestion will affect the
pulmonary parenchyma= cough
Gastro-intestinal
- GERD (common cause of chronic cough)
EENT disorders
- Chronic sinusitis
Common causes of chronic cough:
1. Asthma
2. GERD
3. Sinusitis
PULMONARY:
risk factor
- occupational hazard/ exposure
- smoking history
- family history
- previous TB infection
- previous pneumonia
- age of the patient
dyspnea usually noted after paroxysms
cough
- simply put, cough dyspnea
- hallmark of a pulmonary problem
usually more chronic
CARDIAC:
risk factors
usually more acute in onset aggravated by supine position together with
the dyspnea
dyspneacough
Example: LV dysfunction pulmo congestion
DYSPNEA irritation of lung parenchyma
COUGH
C. HEMOPTYSIS
Upper respiratory tract
-nasopharynx
- oropharynx
Lower respiratory tract
- tracheobronchial tree
- parenchyma
Infectious Causes:
Chronic Bronchitis
Bronchiectasis
Tuberculosis
Non-tuberculous Mycobacteria
Lung Abscess
Necrotizing Pneumonia
Mycetoma
Cystic Fibrosis
From respi tract:
- bright red; frothy
- alkaline pH
From GIT:
-Dark red
- Acidic pH
- Contains food particles
Massive Hemoptysis- >100ml/ 24 hrs
Non- Massive Hemoptysis - <100ml/24 hrs
ALGORITHM FOR NON-MASSIVE HEMOPTYSIS

8/4/2019 Med_ Px with Diseases of Respi System
http://slidepdf.com/reader/full/med-px-with-diseases-of-respi-system 3/6
3
PHYSICAL EXAMINATION
General aspects
- Look for abnormalities, asymmetry,
lesions etc.
INSPECTION OF THE CHEST
rate and pattern of breathing
symmetry of lung expansion
visible abnormalities of the
thoracic cage
- AP diameter
- Pectus carinatum/ excavatum
Inspect extrapulmonary sites like nails
(clubbing), cyanosis which may be
suggestive of pulmo problems.
PALPATION OF THE CHEST
presence or absence of symmetry of tactile
fremitus (remember tres tres???)
- decreased or absent in pleural effusion or
endobronchial obstruction
- increased in consolidation
may also reveal focal tenderness
PERCUSSION OF THE CHEST
resonance or dullness of the tissueunderlying the chest
- normal is resonant
- consolidated lung or pleural effusion sounds
dull
- emphysema is hyperresonant
AUSCULTATION OF THE CHEST
listen for quality and intensity of breath
sounds
1.
Bronchial breath sound
- Expiratory phase is louder and longer
- Large or central airways
2. Vesicular breath sound
- Inspiratory phase is more prominent
- Usually heard at the periphery
Listen for the presence of extra, or
adventitious sounds
breath sound diminished or absent in
endobronchial obstruction, COPD or by air
or liquid in the pleural space
listen for Bronchophony and whispered
pectoriloquy
listen for Egophony (ee becomes ay)
Adventitious lung sounds
• Crackles
- open/close of alveoli
- pneumonia
- congestion
- lung parenchyma abnormalities
- heard best during expiratory phase
• Wheezes
- Due to constriction of airways
- Airways spasm
- Turbulence of airway due to transudate
or exudate
- Heard best during expiratory
• Rhonchi
- Patients with a lot of secretion in
airways
- Transient sound
- Relieved by expectoration
- Halak in Filipino
• Pleural friction rub
- Dses of lung pleura
•
Stridor
- Upper airway obstruction
- Heard even without the use of steth
- Patients with laryngeal/ tracheal
stenosis
*differentiation of common pulmonary
conditions can be found on the last page
DIAGNOSIS
Chest xray, pulmonary function tests, CT scans
are used just to confirm your assessment. If
you're a good doctor, then your assessment will
jive with your diagnostic tests.
Assess the age of the patient and what their risk
factors are. If cardiac or pulmonary, can be
cardiac-hypertensive, previous stroke, medicine
for Coronary Artery Diseases, Pulmonary-
smoker, inhaler, asthma treatment, TB
treatment. Get the chief complaint and to
determine whether it ’ s an acute or chronic
disease to arrive at a differential diagnosis.

8/4/2019 Med_ Px with Diseases of Respi System
http://slidepdf.com/reader/full/med-px-with-diseases-of-respi-system 4/6
4
LABORATORY TESTS
1. Chest X-Ray
2. Pulmonary Function Test
3. Bronchoscopy
4.
Computerized Tomography Scan (CTScan)
5. Magnetic Resonance Imaging (MRI)
Chest X-ray
Most common and easiest
Types of chest x-ray finding:
a. Diseases that increase lung density -
opacifications, infiltrates, fluid
b. Diseases that decrease lung
density- emphysema, peumothorax
c. Plueral disease – pneumothorax,
plueral effusion
Types of x-ray findings associated with
clinical conditions:
1. Some patients may come to you
with a respiratory complaint with
an abnormal chest x-ray
a. Solitary circumscribed density
b.
Localized opacification
(pneumonia, neoplasm,
radiation pneumonities,
bronchiolitis obliterans with
organizing pneumonia (BOOP),
bornchocentric granulomatosis,
pulmonary infarction)
c. Diffuse interstitial diseases
(idiopathic pulmonary fibrosis,
pulmonary fibrosis, sarciodosis,
drug-induced lung disease,
pneumoconiosis,
hypersensitivity pneumonitis,
infection which can be
pneumocystis or viral,
eosinophilic granuloma)
d. Diffuse alveolar disease
(cardiogenic pulmonary
edema, ARDS, diffuse alveolar
hemorrhage, infection which
can be peumocystis, viral, or
bacterial, sarcoidosis)
e. Diffuse nodular disease
(pulmonary metastasis,
hematogenous spread of
infection, pneumoconiosis,
eosinophilic granuloma)
2. But sometimes a patient will come
to you with an abnormal chest x-ray
with no respiratory complaint
a. Localized disease affecting the
airways or the pulmonary
parenchyma
b. Masses or nodules
c. Current or previous infectious
processes
3.
But sometimes a patient will come
to you with a respiratory complaint
with normal chest x-ray
a. Disease affecting the airways
which may be neuromuscular
b. Disease affecting the
respiratory pump
Pulmonary Function Test
We test for lung function via
spirometry for restrictive andobstructive lung diseases
to limit differential diagnosis
SPIROMETRY – measures lung
volumes and airflow parameters.
The patient is instructed to inhale
maximally to TLC and exhale
forcefully to RV for 6 seconds

8/4/2019 Med_ Px with Diseases of Respi System
http://slidepdf.com/reader/full/med-px-with-diseases-of-respi-system 5/6
5
BASICS OF PULMONARY FUNCTION TEST
Physiologic basis
Spirometry
Lung volume studies Diffusing capacities
Maximal respiratory pressures
SPECIAL EXTRAPULMONARY CONDITIONS
Chronic heart failure
Obesity
Decreased compliance
Increase airways resistance
Rapid,shallow breathing pattern
Decrease respiratory muscle
function
Pregnancy
Neuromuscular disorders
Diabetes mellitus
Preoperative evaluation
DYNAMIC LUNG FUNCTION
1. Forced expiratory maneuver
2. Cardio-pulmonary exercise test
*these tests are now available to predict and
measure lung function performance during
exercise
CT SCAN
-this test demonstrate the size of the tumor,
especially peripheral lesions.
OTHER DIAGNOSTIC TEST
Bronchoscopy (can be bronchogenic
carcinoma, bronchial adenoma, or
metastatic disease)
Blood chemistries
Blood gases
SUMMARY
Common signs and symptoms of
patients with respiratory disease
Common physical exam findings in
patient with respiratory disease
How to use data from history and
physical exam in arriving at a logical
clinical impression
Common diagnostic test used to work
up patients with respiratory distress
“Fear not for I am with you: be not dismayed, for I am your God: I will strengthen you, I will help you, I will uphold
you with My righteous right hand.” Isaiah 41:10
G R E E T I N G S
Thanks Armin for semi-transcribing Hello IDK!!!
Thanks Sheila for the voice recording Hello UST-Sampaloc Chapter
Hello to all Saringhimig members!!! Media 2015! Yeyat, Carl, Bruks, Charlon, Sam, Tracy, Ike
Hi Marv and Kith!!!
8/4/2019 Med_ Px with Diseases of Respi System
http://slidepdf.com/reader/full/med-px-with-diseases-of-respi-system 6/6
6
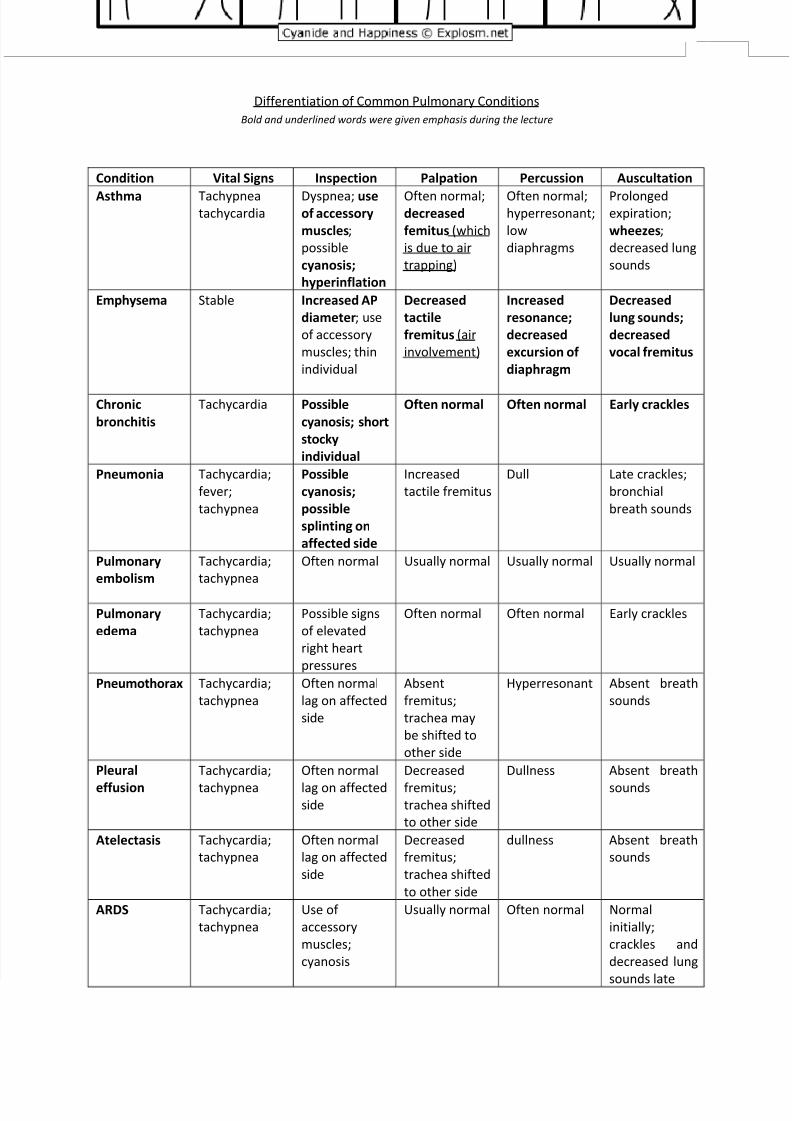
Differentiation of Common Pulmonary Conditions
Bold and underlined words were given emphasis during the lecture
Condition Vital Signs Inspection Palpation Percussion Auscultation
Asthma Tachypneatachycardia
Dyspnea; useof accessory
muscles;
possible
cyanosis;
hyperinflation
Often normal;decreased
femitus (which
is due to air
trapping)
Often normal;hyperresonant;
low
diaphragms
Prolongedexpiration;
wheezes;
decreased lung
sounds
Emphysema Stable Increased AP
diameter; use
of accessory
muscles; thin
individual
Decreased
tactile
fremitus (air
involvement)
Increased
resonance;
decreased
excursion of
diaphragm
Decreased
lung sounds;
decreased
vocal fremitus
Chronic
bronchitis
Tachycardia Possible
cyanosis; short
stocky
individual
Often normal Often normal Early crackles
Pneumonia Tachycardia;
fever;
tachypnea
Possible
cyanosis;
possible
splinting on
affected side
Increased
tactile fremitus
Dull Late crackles;
bronchial
breath sounds
Pulmonary
embolism
Tachycardia;
tachypnea
Often normal Usually normal Usually normal Usually normal
Pulmonary
edema
Tachycardia;
tachypnea
Possible signs
of elevated
right heart
pressures
Often normal Often normal Early crackles
Pneumothorax Tachycardia;
tachypnea
Often normal
lag on affected
side
Absent
fremitus;
trachea may
be shifted to
other side
Hyperresonant Absent breath
sounds
Pleural
effusion
Tachycardia;
tachypnea
Often normal
lag on affectedside
Decreased
fremitus;trachea shifted
to other side
Dullness Absent breath
sounds
Atelectasis Tachycardia;
tachypnea
Often normal
lag on affected
side
Decreased
fremitus;
trachea shifted
to other side
dullness Absent breath
sounds
ARDS Tachycardia;
tachypnea
Use of
accessory
muscles;
cyanosis
Usually normal Often normal Normal
initially;
crackles and
decreased lung
sounds late


















