Correlation of Her-2 neu over-expression with clinico pathological features of carcinoma breast

Genitourin Med 1992;68:75-79
Clinico-pathological conference
Disseminated cytomegalovirus infection
A Grant, C Sargent, I V D Weller, F Scaravilli, L Michaels, R F Miller
Department ofMedicineA GrantR F MillerAcademic Departmentof GenitourinaryMedicineI V D WellerDepartment ofHistopathology,UCMSM, MiddlesexHospital, London,W1N 8AAC SargentL MichaelsDepartment ofNeuropathology;Institute of Neurology,The National Hospitalfor Neurology andNeurosurgery, QueenSquare, London,WC1N 3BGF ScaravilliAddress for correspondence:Dr R F Miller, Departmentof Medicine, UCMSM, FirstFloor Cross Piece,Middlesex Hospital,London, WIN 8AA, UKAccepted for publication14 February 1992
Case presentation (DrA Grant)A 42 year old male Caucasian homosexual wasfound to be HIV antibody positive in May1986. In June 1986 he was recruited to theMRC/ANRS Concorde Study. This is adouble-blind placebo controlled study of zido-vudine in asymptomatic HIV infected individ-uals, to assess its effect on the progression ofHIV disease and survival.' He remained welluntil January 1990, when because of evidenceof progression of his HIV disease (he haddeveloped ARC symptoms with weight lossand night sweats and his CD4 count had fallento 60/mm3 on two occasions), trial capsuleswere stopped and "open" zidovudine was usedat a dose of 250 mg four times daily. Primaryprophylaxis for Pneumocystis carinii pneumoniawas started with monthly inhaled pentamidine.In April 1991 he was notified to CDSC ashaving AIDS on the basis of chronic perianalilceration due to Herpes simplex infection, butotherwise remained well on zidovudine andexperienced no haematological or biochemicaladverse reactions to this drug. He was alsotaking acyclovir 200 mg as prophylaxis for Hsimplex.
In June 1991 he was admitted to hospitalwith a six week history of watery diarrhoea,passing up to six stools per day. He alsocomplained of increasing right upper quadrantabdominal pain, constant in nature, madeworse by ingestion of food and numbness ofthe feet. Examination revealed a thin man whohad a low grade fever (37.4°C). The liver edgewas just palpable. Fundoscopy showed evi-dence of cotton wool spots but no haemor-rhages or other evidence of cytomegalovirusretinitis (fig 1). Investigations at this timerevealed a haemoglobin of 9.7 g/dl and a whiteblood count of 2 1 x 1 09/dl (neutrophils =1 *68 x 1 09/dl). Urea and electrolytes werenormal. Liver function tests showed an alkalinephosphatase of 678 (normal < 282) iu/l, ASTwas at the upper limit of normal at 55 iu/1,serum albumin and bilirubin levels were nor-mal. Ultrasonography of the upper abdomenshowed that the common bile duct was dilatedat 7 mm; no stones were evident within thebiliary tree and the pancreas was normal. Atechnetium IODIDA scan was performed. Thisis a nuclear medicine imaging technique. Innormal patients following intravenous injec-tion of the radiotracer it is taken up by the liverwithin five to ten minutes and is then rapidlyexcreted into the biliary tree, appearing in theduodenum within 20 minutes. In this patient
the scan showed rapid uptake of radiotracerinto the liver parenchyma but there was delayof excretion into the duodenum and retentionwithin the intra- and extrahepatic ducts.2These appearances were highly suggestive ofsclerosing cholangitis. Stool culture revealedSalmonella enteritidis. Nerve conduction studiesshowed evidence of a mild peripheral sensoryaxonal type neuropathy. The patient was trea-ted with oral ciprofloxacin 500 mg bd given forten days for the salmonella infection.Endoscopic retrograde cholangiopancrea-
tography (ERCP) was performed. At ERCPthe ampulla appeared inflamed and this wasbiopsied. A sphincterotomy was performed asthe bile duct orifice appeared stenosed. Acholangiogram showed a dilated common bileduct and also dilated intra- and extrahepaticducts.There was little pain relief following sphinc-
terotomy but the alkaline phosphatase enzymelevels which had risen peaking at 1208 iu/1 justprior to ERCP and the AST which had risen to98 iu/l both rapidly fell to normal levels.Histological examination of biopsy tissuerevealed intranuclear and intracytoplasmicinclusions of cytomegalovirus infection (fig 2).Culture of biopsies from the ampulla latergrew cytomegalovirus. Treatment with ganci-clovir at a dose of 5 mg/kg twice daily wasgiven for 21 days. He later developed aStaphylococcus aureus chest infection which wastreated with erythromycin. A follow up stool
Figure 1 Fundal appearances showing numerous cottonwool spots.
75
on 16 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.68.2.75 on 1 A
pril 1992. Dow
nloaded from

Grant, Sargent, Weller, Scaravilli, Michaels, Miller
*s~ ~~~ ~ ~~ ~~~~~~ ~ ~~~~~~~~~~ .s b....
* fSe
......
wE5.-' .W.;pppk
e :t *̂ < *S e z ". -:'::::*.. .* . * *., .- % * t ....oll
*, &
'-,.,*
--
,
#*.:.1
(a) (b)Figure 2 Ampullary biopsy obtained at ERCP (a) low power view (x 10) (b) medium power view showingintracycloplasmic inclusions (arrows) x 40, haematoxylin and eosin.
culture off ciprafloxacin treatment was neg-ative for Salmonella enteritidis. The patient was
discharged home in mid-August 1991 withoutdiarrhoea, apyrexial and well.He was readmitted from home four weeks
later. The problems were of two weeks increas-ing confusion and mental slowness, lethargyand weakness and unsteadiness of gait. Hisdiarrhoea had also recurred. On examinationhe appeared very ill. He was pyrexial and hadreduced skin turgor. He was slow to answer
questions and was disorientated in time, placeand person. Bilateral grasp reflexes were eli-cited and the reflexes were globally brisk,otherwise there were no localising signs on
neurological examination. Fundoscopy was
entirely normal. The cotton wool spots pre-viously noted had spontaneously resolved.Auscultation of the chest was normal andabdominal examination revealed a 4 cm firmtender liver edge. The pulse was 1 14 perminute and blood pressure was 75/40 mmHg.Investigations at this stage showed a haemoglo-bin of 10O3 g/dl, a white blood count of6-6 x 109/dl (85% neutrophils). The plasmasodium was normal, serum potassium was 3-4(normal 3.5-5.0) mmol/l and blood urea 16.7(normal < 8.0) mmolIl. Serum creatinine was
143 (normal < 125) ,umol/l. The greater eleva-don of the urea compared to the creatininesuggested pre-renal failure ie dehydration.Liver function tests showed an AST of 174 iu/1 (normal < 55 iu/l) and an alkaline phospha-tase of 447 iu/l, serum albumin was 29 g/l.Hep B sAg, anti-HBc and anti-HCV were allnegative. Plasma glucose was 4-2 mmol/l andthe serum calcium corrected for the lowalbumin was normal. Multiple blood cultureswere negative. An MRI scan of the headshowed multiple small high signal abnor-
malities in the frontal lobe, which were non-specific. Generalised atrophic changes werenoted in the cerebrum and cerebellum. Theseappearances were consistent with a diagnosisof HIV encephalopathy. Lumbar punctureshowed clear colourless fluid. Gram, Auramineand India ink stains and subsequent culturewere negative. The cryptococcal antigen wasnegative. No white cells were seen on micros-copy and cytology revealed no abnormal cells.The CSF protein was 0.88 g/l and the CSF/blood glucose ratio was 2-1/4.7 mmol/l. Tox-oplasma and syphilis serology were negative inboth CSF and blood.
It was felt that the patient was dehydratedsecondary to septicaemia. He was treated withintravenous cefuroxime and gentamicin. Acentral line was placed; the central venouspressure was + 1 (normal 5-8 cm) H20. Withfluid resuscitation the blood pressure rose to95/55 mmHg and the temperature fell tonormal over the next ten hours. Subsequentlythere was a further rapid deterioration in thepatient's clinical condition. He became hypo-tensive with a tachycardia and his feverrecurred. Re-examination of the chest at thispoint revealed end inspiratory crackles at bothbases. Arterial blood gases taken with thepatient breathing room air revealed pH = 7.45,PO2= 8.0 kPa and PCO2= 3.8 kPa. Theplasma bicarbonate was 20 mmol/l and thestandard bicarbonate was 24 mmol/l (normal).A chest radiograph taken at this point (fig 3)showed bilateral interstitial shadowing in themid and lower zones, sparing the apices andcostophrenic angles. A clinical diagnosis ofPneumocystis carinii pneumonia was made andtreatment with intravenous high dose co-trimoxazole was begun; adjunctive therapywith methylprednisolone 1 g intravenously on
76
k
|
:..
on 16 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.68.2.75 on 1 A
pril 1992. Dow
nloaded from

Disseminated cytomegalovirus infection
*~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.. X.....I ....
I:nFigure 3 Chest radiograph showing bilateral interstitialshadowing in the mid and lower zones.
three successive days was commenced. Supple-mental oxygen was given but despite this thePO2 fell to 7-7 kPa with the patient breathing60% oxygen via a face mask. Despite institu-tion of continuous positive airways pressureventilation the patient continued to deteriorateand he was transferred to the intensive careunit for mechanical ventilati'on. A metabolicacidosis then developed. This occurred on thebackground of a normal blood glucose, neg-ative urinary ketones and normal urea andelectrolytes and corrected serum calcium. Theserum amylase was 400 (normal < 280) iu/l.The patient became increasingly acidotic andhypoxaemic and subsequently died.
Discussion (Professor I V D Weller)The patient was admitted with a progressivesix week history of watery diarrhoea and rightupper quadrant abdominal pain and I notewhilst he was taking zidovudine haemato-logical and biochemical monitoring hadremained normal. The clinical presentationtogether with the cholestatic liver functionabnormalities are highly suggestive of scleros-ing cholangitis and you confirmed this diag-nosis both with the technetium IODIDA scan
and at ERCP. At this stage two thoughts gothrough my mind. In HIV positive patientssclerosing cholangitis is often associated eitherwith the presence of cytomegalovirus or cryp-tosporidium.3 Indeed, my initial thought wasthat you would find cryptosporidium in thestool. Instead, Salmonella enteritidis4 was iden-tified and cytomegalovirus infection in theampulla was demonstrated histologically andon culture. Following the sphincterotomy andcoinciding with ciprofloxacin treatment theliver function tests returned to normal. It is notclear whether this improvement was due to thesphincterotomy or to treatment with anti-biotics; this biochemical improvement occur-red before ganciclovir treatment was given.Other organisms that have been found in
association with sclerosing cholangitis in HIVpositive patients include Gram negative bacte-ria.35 I just wonder whether he also hadSalmonella enteritidis in his biliary tree?
Following recovery from this episode he wasat home for a period of several weeks and thenre-presented in a critically ill condition, hypo-tensive, pyrexial, confused, dehydrated andsubsequently developed hypoxia and diffuseshadowing on the chest radiograph. This pre-sentation was clearly compatible with a septi-caemia but blood cultures were negative. Thedevelopment of an abnormal chest radiographand hypoxaemia then suggested he had apulmonary problem. The chest radiograph andhypoxaemia are entirely compatible with Pneu-mocystis carinii pneumonia. Another possibilitywas that he had a cytomegalovirus pneumoni-tis? You had already isolated cytomegalovirusfrom one site and although you had treatedhim for three weeks with full dose ganciclovirthis was not followed by maintenance therapy.However, it is rare to find cytomegaloviruscausing a diffuse pneumonitis in HIV positivepatients as a single pathogen. It usually occursas a co-pathogen and we know that by treatingthe co-pathogen we can usually secure recov-ery without the need to specifically treatcytomegalovirus.6 So my guess is that if therewas cytomegalovirus in this man's lungs thenthere was also another infection as well, eitherPneumocystis carinii pneumonia or a bacterialinfection.MRI of the head showed cortical and cer-
ebellar atrophy and non-specific areas of highsignal. These appearances are well described inHIV infection' and are compatible with adiagnosis of HIV encephalopathy. Despitegeneral support with of broad spectrum anti-biotics and antipneumocystis treatment withadjunctive steroids the patient's conditiondeteriorated and he died. As the story unfoldedI began to lean increasingly towards a diagnosisof disseminated cytomegalovirus infection.This man had advanced HIV disease and hisCD4 count had been recorded at 60/mm3 20months before his terminal admission.
Clinical diagnoses1 In the lung Pneurmocystis carinii pneumonia?
or bacterial pneumonia with evidence ofcytomegalovirus infection.
2 In 'the abdomen sclerosing cholangitis withevidence of cytomegalovirus in the biliarytree, gut and liver, adrenals and I justwonder about the pancreas.
3 HIV encephalopathy and possible cytome-galovirus infection.
Pathology (Dr C Sargent and Professor LMichaels)The body was that of a thin, Caucasian man.There was no evidence of Kaposi's sarcoma onthe skin or palate. Microscopic examination ofthe respiratory system showed that the larynx,trachea and bronchi were congested and theairways contained pink fluid. The right lungweighed 1,900 g (normal = 500-600 g), theleft lung weighed 1,750 g (normal = 450-
77
on 16 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.68.2.75 on 1 A
pril 1992. Dow
nloaded from
Grant, Sargent, Weller, Scaravilli, Michaels, Miller
500 g). All lobes showed rubbery consolida-tion and at the apices there were yellow areas ofsoftening 0.5 cm in diameter over an area ofapproximately 3 cm. In the alimentary systemno mucosal lesions were detected in theoesophagus, stomach or duodenum. The liverweighed 2,520 g (normal = 1,400-1,650 g)and was pale with an enhanced lobular pattern.The bile ducts contained inspissated greenmaterial. The gall bladder appeared dilatedand also contained green material. The com-mon bile duct was dilated, circumference2.2 cm, the wall had a granular appearance.The pancreas was swollen and congested.There was possible fat necrosis on the surfaceof the pancreas and on the surrounding omen-tal tissue. The pancreatic ampulla was swollenand the proximal pancreatic duct was nar-rowed. The spleen was congested and weighed480 g (normal 125-195 g). The adrenals wereswollen and adherent to the surrounding adi-pose tissue.
Histological examination showed the lungparenchyma to be very abnormal, with changesbeing most marked in the apices. The overallpattern was that of diffuse alveolar damagewith intra-alveolar haemorrhage. Pneumocystiscarinii pneumonia with atypical histologicalappearance was present.7 There was wide-spread intra-alveolar foamy exudate withinwhich organisms of Pneumocystis carinii wereseen. There was also sub-pleural emphysema-tous change with bulla formation, interstitialinflammation and fibrosis with patchy calcifi-cation (fig 4). Pneumocystis carinii organismswere seen within the areas of calcification andthere was a focal granulomatous response inassociation with this. In addition, throughoutboth lungs there was widespread evidence ofcytomegalovirus infection with infected cellscontaining both intranuclear and intracyto-plasmic inclusions. The viral infection wassufficiently severe to have contributed to theinterstitial inflammation and alveolar damage.
Dissection of the pancreatic and biliary treesrevealed a normal anatomical variation, seen in5% of the population, with the common bileduct and pancreatic ducts opening separatelyonto the duodenal papilla rather than at acommon orifice as is more usually the case. Asnoted at autopsy the ampulla was oedematous.The orifice of the common bile duct was
4
*%,..~~~~~~~~~A... ...
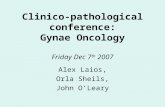
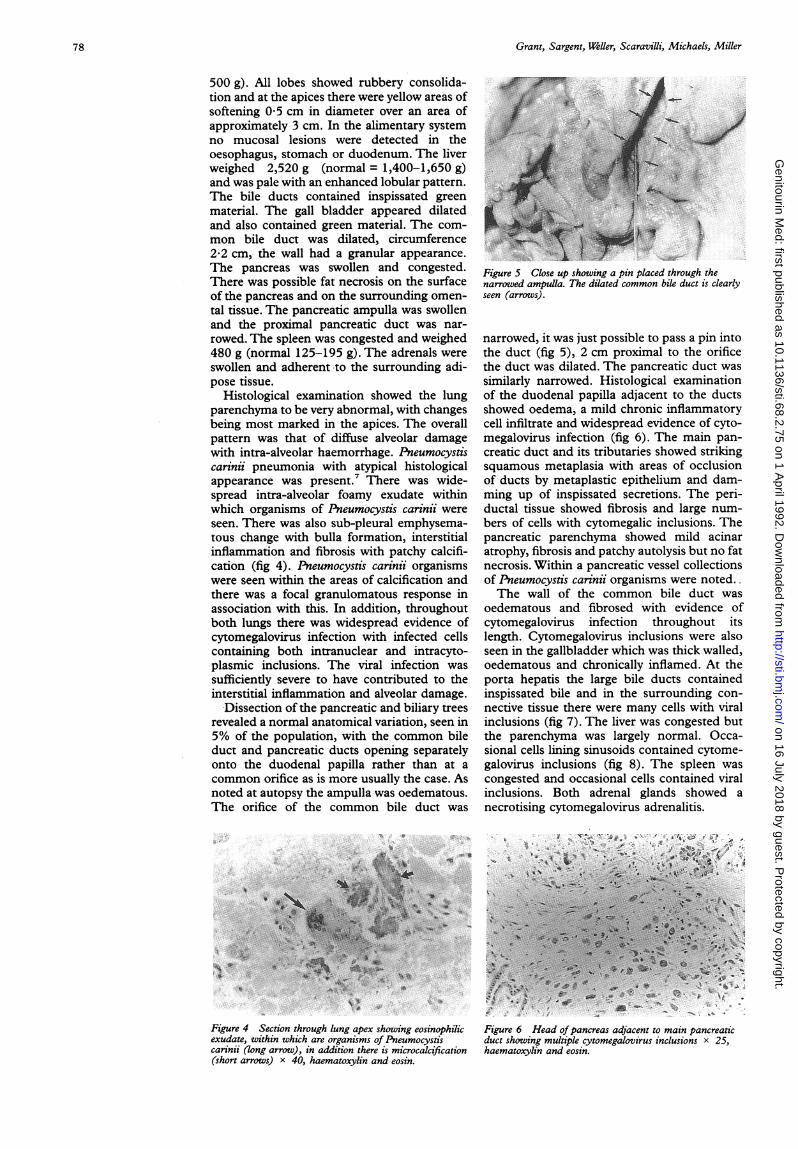
Figure 4 Section through lung apex showing eosinophilicexudate, within which are organisms of Pneumocystiscarinii (long arrow), in addition there is microcalcification(short arrows) x 40, haematoxylin and eosin.
Figure S Close up showing a pin placed through thenarrowed ampulla. The dilated common bile duct is clearlyseen (arrows).
narrowed, it was just possible to pass a pin intothe duct (fig 5), 2 cm proximal to the orificethe duct was dilated. The pancreatic duct wassimilarly narrowed. Histological examinationof the duodenal papilla adjacent to the ductsshowed oedema, a mild chronic inflammatorycell infiltrate and widespread evidence of cyto-megalovirus infection (fig 6). The main pan-creatic duct and its tributaries showed strikingsquamous metaplasia with areas of occlusionof ducts by metaplastic epithelium and dam-ming up of inspissated secretions. The peri-ductal tissue showed fibrosis and large num-bers of cells with cytomegalic inclusions. Thepancreatic parenchyma showed mild acinaratrophy, fibrosis and patchy autolysis but no fatnecrosis. Within a pancreatic vessel collectionsof Pneumocystis carinii organisms were noted..The wall of the common bile duct was
oedematous and fibrosed with evidence ofcytomegalovirus infection throughout itslength. Cytomegalovirus inclusions were alsoseen in the gallbladder which was thick walled,oedematous and chronically inflamed. At theporta hepatis the large bile ducts containedinspissated bile and in the surrounding con-nective tissue there were many cells with viralinclusions (fig 7). The liver was congested butthe parenchyma was largely normal. Occa-sional cells lining sinusoids contained cytome-galovirus inclusions (fig 8). The spleen wascongested and occasional cells contained viralinclusions. Both adrenal glands showed anecrotising cytomegalovirus adrenalitis.
i,.>'x,_''i'''-w~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.....P ~~~~~~ A~A
....
\ ~* 0
p...
Figure 6 Head ofpancreas adjacent to main pancreaticduct showing multiple cytomegalovirus inclusions x 25,haematoxylin and eosin.
78
.X
on 16 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.68.2.75 on 1 A
pril 1992. Dow
nloaded from
Disseminated cytomegalovirus infection
Figure 7 Bile ducts at porta hepatis showing inspissatedbile (arrows) x 10 haematoxylin and eosin.
. ~~~~~~~~~~~~~~ ~~~~~~~~~~~~~~~~~~~~~~~. s.... -.. ,.
,#~~~_,'
Figure 8 Liver sinusoid showing cytomegalovirusinclusion (arrow) x 25 haematoxylin and eosin.
Neuropathology (Dr F Scaravillh)The brain, which weighed 1560 g, was sym-metrical and of normal size. The leptome-ninges were thin and transparent. Coronalsections showed normal appearances. No mac-roscopic abnormalities were seen in the cer-ebellum, brain stem and spinal cord.
Histological examination was carried outusing routine methods. Immunohistochemicaltechniques were applied using the followingantibodies: anti-GFAP, HAM56 for microglia,p24 for HIV and anti-cytomegalovirus. Thecortex showed a discrete diffuse increase in thenumber of GFAP positive glial cells andcontained numerous microglial nodules. Thesewere usually of small size and consisted of rodcells and smaller numbers of macrophages andincluded an occasional large astrocyte contain-ing an intranuclear inclusion which wereimmunostained by the CMV antibody. Nomultinucleated giant cells were seen andimmunostaining with p24 was negative. Thespinal cord showed myelin pallor circum-scribed to the gracile tract.
In conclusion, the appearances were those ofcytomegalovirus encephalitis, no HIV ence-phalitis was evident. In addition there was
pallor of the gracile tract.
Pathological diagnosis1 Disseminated cytomegalovirus infection
lungpancreasbiliary treeadrenalsspleenbrain
2 Disseminated Pneumocystis carinii infectionwith atypical pulmonary features
- bullae formation- diffuse alveolar damage- interstitial fibrosis- calcification- granuloma formation- intra-alveolar haemorrhage
Discussion (Dr R F Miller)Presumably because this patient had receivedinhaled pentamidine and not systemic prophy-latic therapy for Pneumocystis carinii the lungabnormalities were most evident in the apices.We know that predominantly apical disease canoccur in this patient group.8 The lack ofsystemic prophylaxis may also account for thefinding of Pneumocystis carinii in the pancreas,ie disseminated Pneumocystis carinii infection.9The terminal event in this man looks to likelyto have been an Addisonian crisis.
Professor IVD WellerI think we are going to see even more patientslike this in the future as the nature of HIVdisease is modified. Effective treatment andprophylaxis for many of the opportunisticinfections will improve. We are already seeingan improved survival of patients with estab-lished CDC group IV disease. Increasingly thecauses of morbidity and mortality will be theopportunistic malignancies, neurological dis-ease and also infections where we have little inthe way of really effective therapy, such asdisseminated Mycobacterium avium intracellu-lare, cytomegalovirus infection and progressivemultifocal leucoencephalopathy. With respectto the disseminated cytomegalovirus infection,in 1989 progressive cytomegalovirus diseaseassociated with ganciclovir resistant viruseswas reported.'0 The mechanism of this resist-ance is still not clear. This patient had onlyreceived 21 days of ganciclovir therapy but itwould be interesting to know whether hisagonal cytomegalovirus isolates were sensitiveto the drug.
1 SwartAM,Weller IVD, Darbyshire JH. Early HIV infection:to treat or not to treat. BMJ 1990;301:825-6.
2 Buscombe J, Miller RF, Ell PJ. Hepatobiliary scintigraphy inthe diagnosis of AIDS related sclerosing cholangitis. NucMed Comm 1992;13:154-60.
3 Dowsett J, Miller RF, Davidson R et al. Sclerosing chol-angitis in acquired immunodeficiency syndrome. Scan JGastroent 1988;23:1267-74.
4 Celum CL, Chaisson RE, Rutherford GW, Barnhart JL,Echenberg DF. Incidence of salmonellosis in patientswith AIDS. J Infect Dis 1987;156:998-1001.
5 Cello JP. Acquired immunodeficiency cholangiopathy: spec-trum of disease. Am J Med 1989;86:539-46.
6 Millar AB, Patou G, Miller RF et al. Cytomegalovirus in thelungs of patients with AIDS: respiratory pathogen orpassenger? Am Rev Resp Dis 1990;141:1474-7.
7 Travis WD, Pittaluga S, Lipschik GY et al. Atypicalpathologic manifestations of Pneumocystis carinii pneumo-nia in the acquired immunodeficiency syndrome. Am JSurg Pathol 1990;14:615-25.
8 Jules-Elysee K M, StoverD E, ZamanM B et al. Aerosolizedpentamidine: effect on diagnosis and presentation ofPneumocystis carinii pneumonia. Ann Intern Med1990;112:750-7.
9 Coker R, Clark D, Claydon FL et al. DisseminatedPneumocystis carinii infection in patients with AIDS. Jf ClinPathol 199 1;44:820-3.
10 Erice A, Chou S, Biron KK, Stanet S C, Balfour HH,Jordan MC. Progressive disease due to ganciclovir-resistant cytomegalovirus in immunocompromisedpatients. N EnglJ_ Med 1989;320:289-93.
79
on 16 July 2018 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.68.2.75 on 1 A
pril 1992. Dow
nloaded from














![Clinico-pathological case 1 [Trinity College Dublin] Prof T Rogers Prof O Sheils Dr C D’Adhemar.](https://static.fdocuments.in/doc/165x107/56649f355503460f94c53b07/clinico-pathological-case-1-trinity-college-dublin-prof-t-rogers-prof-o-sheils.jpg)