Mechanisms of Trauma Coagulopathy - ANZCA · Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi...
34
Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi General Hospital Singapore
Transcript of Mechanisms of Trauma Coagulopathy - ANZCA · Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi...

Mechanisms of Trauma Coagulopathy
Dr B M Schyma
Changi General Hospital
Singapore


A continued cause of PREVENTABLE death.
24% of trauma patients are coagulopathic on arrival1
• 56% of severe trauma patients have coagulation abnormalities at 25min (samples taken on scene)
Time to Definitive Haemorrhage Control is a key determinant of outcome 3.
HAEMORRHAGE
1) Brohi, J Trauma (2003) 2) Floccard et al, Injury (2012) 3) Macleod, J Trauma (2003)

Coagulopathy is the Harbinger of Mortality
1) Frith et al, J Throm Haemost (2010)
• Pooled data from 5693 patients in 5 countries
• Samples taken on admission
Number of Units in 24hrs

The Triad of Death – The Complete Story?
HYPOTHERMIA
ACIDAEMIA COAGULOPATHY
CLOTTING FACTOR DYSFUNCTION
CLOTTING FACTOR LOSS DILUTION
CONSUMPTION

BUT…..of 701,491 patients:
• Only 11,026 (1.57%) had an admission temperature < 35°C1
Hypothermia
1) Martin et al, Shock (2005)

ROTEM
• CT: Time to initiation of fibrin formation • Alpha Angle: Rapidity of Fibrin Build up and Cross Linking • CFT: Clot Kinetics (2mm to 20mm) • MCF: Clot strength
ROTEM

p < 0.00001, r = 0.85 p < 0.00001, r = 0.89

Clot Strength
pH
MC
F (m
m)
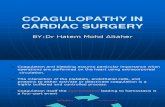
Dilution
1. Maegele, World Journal of Emergency Medicine (2010)

71 Patients, ISS > 15
Stratified to degree of hypoperfusion by base deficit
Similar volume of crystalloid
Venous sample taken on admission
• Factor assay
Clotting factor DEFICIENCY?
1) Jansen et al , J Trauma (2011)

Base Deficit Vs. Factor Activity
1) Jansen et al , J Trauma (2011)

76% factor activity remained in the normal range
42% of patients had no deficiency
Factor 5 behaves differently
• Significant association between BD and factor activity for 2,7,9,10 &,11
• No association between BD and Factor 5 Activity
• Lowest level of activity of all factors
• 54% had a level below normal range
However…

A significant number of our trauma patients arrive with significant coagulopathy.
Mechanisms traditionally thought to cause coagulopathy appear to only occur in extremes.
An interesting juxtaposition…

Is There Something Else?

This Next Slide May Contain The Sexiest Graph You Will See Today

1) Frith et al, J Throm Haemost (2010)

Similar Pattern with Mortality
1) Frith et al, J Throm Haemost (2010)

Protein C • Activated by Thrombin-Thrombomodulin Complex
• Inhibits Factors 5 & 8
• Promotes Fibrinolysis
Cohen et al • 206 patients
• Serial Blood Samples at 6,12, and 24 hrs
• Stratified by Base Deficit and ISS
Potential Mechanism?
1. Cohen et al, Ann Surg (2012)

Increased Activation of Protein C
*p < 0.05
Activated Protein C Levels Protein C Levels

Associated with Decreased Factor 5 & 8
*p < 0.05
Factor Va Level Factor VIIIa Level

Fibrinolysis
FIBRINOGEN
CROSS LINKED FIBRIN
Thrombin
FIBRIN DEGRADATION
PRODUCTS
PLASMIN
PLASMINOGEN
tPA

APC Associated with De-Repression of Fibrinolysis
*p < 0.05

The Thrombin Switch
SHOCK
THROMBOMODULIN
THROMBIN-THROMBOMODULIN
THROMBIN
PROTEIN C
ACTIVATED PROTEIN C
Fibrinolysis

Fibrinogen concentration falls quickly
Low fibrinogen predictor of mortality at 24hrs and 28 days1
Degree of fibrinolysis related to mortality2
Fibrinogen & Fibrinolysis
1. Rourke et al, J Thromb Haemost (2012) 2. Tauber et al, Br J Anaesth (2011)

Platelets
• Limited knowledge of the role of platelets in Trauma Induced Coagulopathy
Endothelial Dysfunction
What have we not talked about…
‘Imbalance of the Dynamic Equilibrium Between Procoagulant Factors, Anti-coagulant Factors, Platelets, Endothelium and
Fibrinolysis’1
Multi-Factorial • Acute Coagulopathy of Trauma
• Hyperfibrinolysis
• Factor Deficiency • (Dilutional) • (Acidaemia) • (Hypothermia)
Trauma Induced Coagulopaty (TIC)
1. Frith and Brohi, Curr Opin Crit Care (2012)

Remember • Identify the bleeding coagulopathic patient early.
• Classical tests of coagulation may not detect TIC
Instigate Damage Control Resuscitation • Haemostatic Resuscitation
• Haemostatic Packaging
• Minimal, Targeted, Crystalloid Administration
• Early High Ratio Component Therapy
• Address Fibrinolysis
• Point of care coagulation testing
Managing TIC

Khan et al 2014
106 patients
• Median ISS 35 (25-41)
INTERN (International Trauma Research Network)
Lactate and ROTEM analysed at 4, 8 and 12 units PRBC
FFP:PRBC 2:3
Platelets & Cryoprecipitate at 6 PRBC
FULL CIRCLE…

*versus time zero
4 Unit Transfusions 8 Unit Transfusions 12 Unit Transfusions

ROTEM 5min Clot Amplitude (CA5) ROTEM Mean Clot Firmness (MCF)
ROTEM Clotting Time (CT)

Resuscitation is not an end-point, it is a means to
facilitating definitive management.

Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma. 2003;54:1127-1130.
Floccard B, Rugeri L, Faure A et al. Early coagulopathy in trauma patients: an on-scene and hospital admission
study. Injury. 2012;43:26-32.
MacLeod JB, Lynn M, McKenney MG, Cohn SM, Murtha M. Early coagulopathy predicts mortality in trauma. J
Trauma. 2003;55:39-44.
Frith D, Goslings JC, Gaarder C et al. Definition and drivers of acute traumatic coagulopathy: clinical and
experimental investigations. J Thromb Haemost. 2010;8:1919-1925.
Martin RS, Kilgo PD, Miller PR, Hoth JJ, Meredith JW, Chang MC. Injury-associated hypothermia: an analysis of
the 2004 National Trauma Data Bank. Shock. 2005;24:114-118.
Engstrom M, Schott U, Romner B, Reinstrup P. Acidosis impairs the coagulation: A thromboelastographic
study. J Trauma. 2006;61:624-628.
Maegele M. Acute traumatic coagulopathy: Incidence, risk stratification and therapeutic options. World J
Emerg Med. 2010;1:12-21.
References (1)

Jansen JO, Scarpelini S, Pinto R, Tien HC, Callum J, Rizoli SB. Hypoperfusion in severely injured trauma patients
is associated with reduced coagulation factor activity. J Trauma. 2011;71:S435-S440.
Cohen MJ, Call M, Nelson M et al. Critical role of activated protein C in early coagulopathy and later organ
failure, infection and death in trauma patients. Ann Surg. 2012;255:379-385.
Rourke C, Curry N, Khan S et al. Fibrinogen levels during trauma hemorrhage, response to replacement
therapy, and association with patient outcomes. J Thromb Haemost. 2012;10:1342-1351.
Tauber H, Innerhofer P, Breitkopf R et al. Prevalence and impact of abnormal ROTEM(R) assays in severe blunt
trauma: results of the ‘Diagnosis and Treatment of Trauma-Induced Coagulopathy (DIA-TRE-TIC) study’. Br J
Anaesth. 2011;107:378-387.
Frith D, Brohi K. The pathophysiology of trauma-induced coagulopathy. Curr Opin Crit Care. 2012;18:631-636.
Khan S, Brohi K, Chana M et al. Hemostatic resuscitation is neither hemostatic nor resuscitative in trauma
hemorrhage. J Trauma Acute Care Surg. 2014;76:561-7; discussion 567.
References (2)