Pulmonary atresia with Ventricular septal defect Pulmonary atresia with Ventricular septal defect.

SECOND HEART SOUND IN ASD/O'Toole, Reddy, Curtiss, Shaver
17. Shone JD, Sellers RD, Anderson RC, Adams P Jr, Lillihei CW, EdwardsJE: The developmental complex of "parachute mitral valve," supravalvarring of the left atrium, subaortic stenosis and coarctation of the aorta.Am J Cardiol 11: 714, 1963
18. Ellison RC, Restieaux NJ: Vectorcardiography in Congenital HeartDisease. Philadelphia, W.B. Saunders Co, 1972, p 196
19. Heath D, Edwards JE: The pathology of hypertensive pulmonaryvascular disease. A description of six grades of structural changes in thepulmonary arteries with special reference to congenital cardiac septaldefects. Circulation 18: 533, 1958
20. Davachi F, Moller JH, Edwards JE: Diseases of the mitral valve in infan-cy: An anatomic analysis of 55 cases. Circulation 43: 565, 1971
21. Humblet L, Stainer 1, Joris H, Collignon P, Kulbertus H, Delvigne J: Lastenose mitrale congenitale. Acta Cardiol 26: 5, 1971
22. Rosenquist GC: Congenital mitral valve disease associated with coarcta-tion of the aorta. Circulation 49: 985, 1974
23. Benry J, Leachman RD, Cooley DA, Klima T, Lufschanowski R:Supravalvar mitral stenosis associated with tetralogy of Fallot. Am JCardiol 37: 111, 1976
24. LaCorte M, Harada K, Williams RG: Echocardiographic features ofcongenital left ventricular inflow obstruction. Circulation 54: 562, 1976
25. Lundstrom NR: Value of echocardiography in diagnosis of congenitalmitral stenosis. Br Heart J 38: 534, 1976
26. Godman MF, Fiddler GI, Marquis RM: Echocardiography in evaluationof congenital mitral valve disease in infants and children. Br Heart J 37:783, 1975
27. Freed MD, Bernhard WF: Prosthetic valve replacement in children. ProgCardiovasc Dis 18: 131, 1975
28. Carpentier A, Guerinon J, Deloche A: Pathology of the mitral valve. In-troduction to plastic and reconstructive valve surgery. In The MitralValve, edited by Kalmanson D. Acton, Mass, Publishing Sciences Group,1976, p 65
The Mechanism of Splitting of the Second HeartSound in Atrial Septal Defect
JAMES D. O'TOOLE, M.D., P. SUDHAKAR REDDY, M.D., EDWARD I. CURTISS, M.D.,
AND JAMES A. SHAVER, M.D.
SUMMARY The mechanism underlying the width of splitting ofthe second heart sound (S,) was investigated in 27 patients with os-tium secundum atrial septal defect (ASD), all of whom had signifi-cant left to right shunting. Micromanometer catheters were used torecord simultaneous high fidelity right ventricular (RV) andpulmonary arterial (PA) pressures. Electrocardiogram and externalphonocardiograms were recorded simultaneously with pressures.QP,, QA, and Q-RV intervals were measured from the onset of theQ-wave of the ECG to the onset of P,, A, and to the downstroke ofthe RV pressure trace at the level of the pulmonary incisura, respec-tively. The width of splitting of the second heart sound (A,-P, inter-val) and hangout (HO) intervals were derived by subtracting QA,from QP, and Q-RV from QP,, respectively.The patients were divided into three groups. There were 14 patients
in group I (normotensive ASD) with sinus rhythm and normal PApressure (mean<21 mm Hg); in group II (hyperkinetic pulmonaryhypertension) there were seven patients with sinus rhythm and
WIDE FIXED SPLITTING OF THE SECOND HEARTSOUND (S,), appreciated as audible expiratory splitting, isa characteristic auscultatory feature of atrial septal defect.'Prior studies have demonstrated that this phenomenon isdue to a prolonged QP, interval,' but the mechanism un-derlying this wide splitting remains controversial.'Prolongation of right ventricular systole due to diastolicvolume overload is the most widely accepted mechanism.4'-However, several observations suggest this classic explana-tion may be only partially correct. First, there are manyreports of documented persistence of audible expiratory
From the Division of Cardiology, University of Pittsburgh, School ofMedicine, and Presbyterian-University Hospital, Pittsburgh, Pennsylvania.Supported in part by training grant 5TO0 HL5678-10 from the National
Heart and Lung Institute.Address for reprints: James D. O'Toole, M.D., Co-Director, Cardiac
Diagnostic Laboratories, Presbyterian-University Hospital, 230 LothropStreet, Pittsburgh, Pennsylvania 15213.
Received February 21, 1977; revision accepted July 14, 1977.
elevated PA pressure (mean PA>23 mm Hg) and group III consistedof six patients with atrial fibrillation. For normotensive ASD, A,-P,and hangout intervals correlated well (r=0.91) and were essentiallyequal. QA, and Q-RV intervals were also approximately equal, in-dicating that the electromechanical interval was essentially equal forright and left ventricles (LV).
In hyperkinetic pulmonary hypertension the hangout interval wasrelatively narrow as compared to group I (P<0.001) and the splittinginterval varied from narrow to wide, depending upon the relativedurations of Q-RV and QA,. The QA, indices tended to be withinnormal limits, suggesting that the duration of Q-RV was the majordeterminant of the width of splitting. In atrial fibrillation, HO wasfixed and narrow; A,-P, and Q-RV intervals were directly related topreceding cycle length.
Thus, an understanding of the mechanism of splitting of the secondheart sound in ASD must reflect the HO interval as well as therelative durations of RV and LV electromechanical systoles.
splitting of S, after proven repair of the atrial septaldefect."'10-13 Secondly, wide expiratory splitting of the sec-ond heart sound also occurs in idiopathic dilatation of thepulmonary artery, a condition where diastolic overloading isabsent.'4 Thirdly, if the abnormal splitting was due tovolume overload of the right ventricle, then one would ex-pect a significant correlation between the amount of shunt-ing and the width of splitting. Castle was unable to showsuch a correlation but he did show that, in children withatrial septal defects, the width of splitting increased as ageincreased." In light of these observations, the present studyattempted to define the mechanism underlying the widesplitting of the second heart sound seen with atrial septaldefect.
Materials and Methods
Twenty-seven patients undergoing diagnostic cardiaccatheterization were the subject of this investigation. All hadisolated ostium secundum atrial septal defects. Six were
1047
by guest on June 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL. 56, No. 6, DECEMBER 1977
male and 21 were female ranging in age from 14 to 67 years.In each case, specific permission was granted to performhigh fidelity intracardiac sound and pressure measurementsduring the course of the diagnostic study. The diagnosis wasconfirmed in all patients at catheterization which showedleft-to-right shunts of 1.9: 1 or greater as determined by oxy-gen saturations and/or the nitrous oxide inhalationmethod.i6 Twenty-four of these patients subsequently un-derwent surgical repair where the diagnosis was confirmed.Patients with ostium primum defects, right ventricular out-flow obstruction, or associated mitral regurgitation were ex-cluded.
All patients were studied in the supine position. Intracar-diac sound and pressure events were recorded withmicromanometer catheters.* These transducers allowrecording of high fidelity intracardiac pressure free of con-tour distortion and without time delay and their audiocir-cuitry has a flat response from 70 to 2,000 Hz with a roll-offof 12 decibels per octave below 70 Hz. Two catheter-tippedmicromanometers were placed in the right ventricle wheremicromanometric pressures were made equisensitive. Onemicromanometer was then placed in the pulmonary arteryjust above the valve from which sound and pressure wererecorded. Equisensitivity was checked throughout the studyby pullback of the pulmonary artery micromanometer to theright ventricular outflow tract. In three cases where it wasspecifically checked, there was no difference between the in-tervals measured with the right ventricular catheterpositioned in either the inflow or the outflow portion of theright ventricular chambers. External sound was recordedusing an Electronics for Medicine microphone and bandpass filters set at 120 and 500 Hz on a DR 12 recorder. Theexternal phonocardiogram was recorded on the chest wall at
*Millar Mikro-tip pressure transducer; Carolina Medical Electronics.
A2 rz
PHONO
/ > ~~~~~I
PULMONARY ARTERYPRESSURE
RIGHT VENTRICULARPRESSURE
ELECTROCARDIOGRAM
EPI - ELECTROPRESSORINTERVAL
the point of maximum intensity of the aortic and pulmonicclosure sounds and a simultaneous electrocardiogram wasobtained for timing purposes. Continuous respirations weremonitored with a nasal thermistor. The data were recordedsimultaneously on a multichannel Electronics for Medicinephotographic recorder at a paper speed of 100 mm/sec withtimeline markers indicating 20 msec.The following intervals were measured on each patient
and were the average of at least ten successive complexestaken during quiet respiration (fig. 1):
1) QP2 - interval from the onset of the Q-wave of the elec-trocardiogram to the onset of the pulmonic component ofthe second heart sound. Intergroup comparisons of QP2intervals were performed using QP2 indices calculatedfrom regression data for ASD by Curtiss et al.i
2) Q-RV (electromechanical interval) - interval from theonset of the QRS to the downstroke of the RV pressuretrace at the level of the pulmonary artery incisura.
3) QA2 - interval from the onset of the Q wave of the elec-trocardiogram to the onset of the first high frequencyvibration of the second heart sound. The QA2 index wasobtained using the regression equation of Weissler et al.is
4) EPI (Electropressor interval) - interval from the onsetof the QRS to the onset of right ventricular pressure rise.
5) A2-P2 (splitting interval) - QP2 minus QA2.6) Hangout interval (HO) - interval separating the right
ventricular pressure curve from the pulmonary artery in-cisura at the pressure level of the latter (QP2 minus Q-RVinterval).
Results
Group I: Normotensive Atrial Septal Defect
This group consisted of 14 patients in normal sinusrhythm with mean pulmonary artery pressures of less than
A D_
FIGURE 1. Schematic illustration of various in-tervals measured on patients with ASD.
11
II~~~~~~~~~~~~~1IIIE" 1,
Q A2I Q RVI QP2
HANG-OUT INTERVAL (HO)= Q A^ - 0 RV
1048 CIRCULATION
by guest on June 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

SECOND HEART SOUND IN ASD/O'Toole, Reddy, Curtiss, Shaver
TABLE 1. Summary of Data on 27 PatientsPAP
S D M Q-A2 Q-A2I Q-P2 Q-RV Hangout A2-P2Pt/Age/Sex Rhythm (mm Hg) Qp/Qs Rp/Rs (msec) (msec) (msec) (msec) (msec) (msec)
Group IR.M./45/F Sinus 24 8 16 2 0.07 423 563 469 425 44 46D.E./16/F Sinus 16 8 12 3.3 0.05 371 567 437 371 66 66D.Y./49/F Sinus 24 6 14 2.7 0.07 443 577 499 446 53 56J.H./28/F Sinus 20 2 10 2.2 0.05 404 564 454 409 45 50D.O./19/F Sinus 33 4 18 3.2 0.06 377 543 417 377 40 40A.M./40/F Sinus 30 10 16 2.5 411 555 461 417 44 50R.W./31/M Sinus 28 8 16 2.4 0.08 402 572 442 402 40 40S.R./23/F Sinus 32 8 16 2.5 0.08 385 547 441 390 51 56E.G./50/F Sinus 32 16 20 2.1 0.09 327 541 364 326 38 37C.E./46/F Sinus 34 14 20 2.3 0.09 371 535 411 371 40 40D.S./19/F Sinus 24 4 12 2.8 0.05 411 559 460 421 39 49J.A./33/M Sinus 24 11 16 2.4 0.08 450 580 486 450 36 36E.R./33/F Sinus 38 8 18 3.7 0.04 350 490 390 350 40 40E.K./48/F Sinus 26 2 10 2.4 0.04 363 529 402 364 38 39
Group IIN.R./14/M Sinus 80 40 55 4.5 0.16 354 560 382 354 28 28A.G./56/M Sinus 50 25 30 1.9 0.20 385 551 411 385 26 26M.M./61/F Sinus 75 10 38 2.3 0.15 428 569 468 453 15 40A.H./57/M Sinus 85 30 50 2.2 0.21 360 553 400 380 20 40S.K./54/F Sinus 52 24 36 2 0.14 400 550 464 432 32 64M.H./40/F Sinus 44 12 24 2.3 0.10 399 533 459 423 36 60A.P./64/F Sinus 100 20 50 3.3 0.18 341 481 411 389 22 70
Group IIIA.S./60/F AFib 34 8 18 2 0.09 30 30-60O.C./67/F AFib 32 12 20 2 0.10 38 36-72E.R./53/F AFib 42 14 26 3.5 0.08 20 35-55W.S./64/M AFib 40 8 21 3 0.08 25 50-76B.T./62/F AFib 56 16 26 2 0.14 24 58-74V.W./65/F AFib 38 8 18 3.7 0.07 22 34-72Abbreviations: PAP = pulmonary artery pressure; S = systolic; D = diastolic; M = mean; Qp/Qs = pulmonary to systemic flow ratio; Rp/Rs = pulmo-
nary to systemic resistance ratio; QA2I = QA2 index; Q-RV = right ventricular electromechanical systole.
21 mm Hg (table 1). They ranged in age from 16 to 50 years. A2 l A2 P2All were characterized by wide splitting of the second heart EX L PiOwosound and by the presence of a large pulmonary artery on , I',,routine chest roentgenogram. The group I patients had amean QA2 index of 552 ± 24 msec (SD). The right ven- 66msec.tricular electropressor intervals ranged from 37 to 45 msecwith a mean of 40 ± 2 msec (SD). In this group, the width ofsplitting was not significantly associated with the degree ofshunting but there was close agreement between the hangout EXPIRATION \\SP\RAT|\Ninterval and the A2-P2 interval (r= 0.9 1). These two intervals I I Onever varied by more than 10 msec although the A,-PI, inter- IJtOAR \uAval ranged from 36 to 66 msec. The QA2and Q-RV intervals | |'sec .
were essentially equal. tFigure 2 is representative of the sound and pressure cor- I
relates found in these patients. The width of splitting was 66 R0T ETRLmsec. P2 was coincident with the incisura of the pulmonaryartery pressure tracing which was separated from the right ~
ventricular pressure trace by a hangout interval of 66 msec.The QA2 and Q-RV intervals were both equal to 371 msec.
FIGURE 2. Simultaneous right ventricular and pulmonary arteryGroup II: Hyperkinetic Pulmonary Hypertension pressure curves are recorded with external sound in a 16-year-old
female with a normotensive ASD and a left-to-right shunt of3.3:1.This group consisted of seven patients wlth normal sinus Hangout refers to the interval from the right ventricular pressure
rhythm who had elevation of the mean pulmonary artery trace to the pulmonary artery pressure curve at the level of the in-pressure to a level greater than 23 mm Hg. They ranged in cisura. The A2-P2 interval of66 msec corresponds to a hangout in-age from 14 to 64 years. They were characterized by an in- terval of 66 msec. Timelines in this and subsequent illustrationscrease in the pulmonary to systemic resistance ratio as com- represent 20 msec.
1049
by guest on June 29, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL. 56, No. 6, DECEMBER 1977
EXTERNAL PHON SiSMA2 A
28 msec
tPU ARTER P2
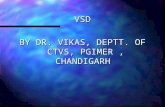
FIGURE 3. Micromanometric right ventricular and pulmonaryartery pressures in a 14-year-old male with a 4.5:1 left-to-rightshunt at the atrial level. The pulmonary artery pressure was 80/40with a mean of 55 mm Hg. External splitting of 28 msec cor-responds to a hangout interval of28 msec. (SEM = systolic ejectionmurmur).
pared to group I with significant maintenance of left-ro-rightshunting (table 1). As compared to group I, the right-sidedhangout interval was uniformly narrower (25 ± 9 vs 44 ± 8msec; P<0.001). Two patients in group II had relativelynarrow splitting of S, (<30 msec). The patient whose find-ings are depicted in figure 3 had a mean pulmonary arterypressure of 55 mm Hg, a puiinonary to systemic flow ratio of4.5: 1, and a normal QA, index of 560 msec. Narrow split-ting of S2 was observed on the external phonocardiogramand was associated with a narrow hangout interval of 28msec. Patient A.G. with a mean pulmonary artery pressureof 30 mm Hg showed a similar narrow hangout interval anda normal QA, index. In these two patients, similar to groupI subjects, the Q-RV and QA2 intervals were equal.
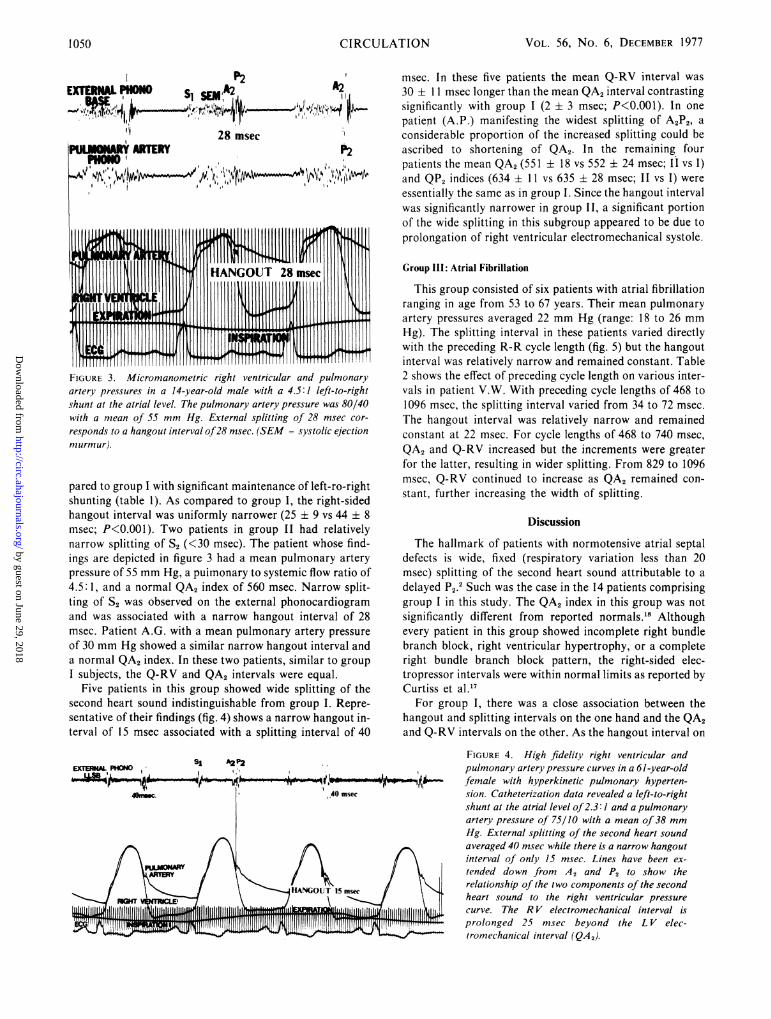
Five patients in this group showed wide splitting of thesecond heart sound indistinguishable from group I. Repre-sentative of their findings (fig. 4) shows a narrow hangout in-terval of 15 msec associated with a splitting interval of 40
S1 A2P2
msec. In these five patients the mean Q-RV interval was30 ± 11 msec longer than the mean QA, interval contrastingsignificantly with group I (2 ± 3 msec; P<0.001). In onepatient (A.P.) manifesting the widest splitting of A,P,, aconsiderable proportion of the increased splitting could beascribed to shortening of QA,. In the remaining fourpatients the mean QA, (551 ± 18 vs 552 ± 24 msec; II vs I)and QP, indices (634 ± 11 vs 635 ± 28 msec; II vs I) wereessentially the same as in group I. Since the hangout intervalwas significantly narrower in group II, a significant portionof the wide splitting in this subgroup appeared to be due toprolongation of right ventricular electromechanical systole.
Group III: Atrial Fibrillation
This group consisted of six patients with atrial fibrillationranging in age from 53 to 67 years. Their mean pulmonaryartery pressures averaged 22 mm Hg (range: 18 to 26 mmHg). The splitting interval in these patients varied directlywith the preceding R-R cycle length (fig. 5) but the hangoutinterval was relatively narrow and remained constant. Table2 shows the effect of preceding cycle length on various inter-vals in patient V.W. With preceding cycle lengths of 468 to1096 msec, the splitting interval varied from 34 to 72 msec.The hangout interval was relatively narrow and remainedconstant at 22 msec. For cycle lengths of 468 to 740 msec,QA, and Q-RV increased but the increments were greaterfor the latter, resulting in wider splitting. From 829 to 1096msec, Q-RV continued to increase as QA, remained con-stant, further increasing the width of splitting.
Discussion
The hallmark of patients with normotensive atrial septaldefects is wide, fixed (respiratory variation less than 20msec) splitting of the second heart sound attributable to adelayed P2.2 Such was the case in the 14 patients comprisinggroup I in this study. The QA, index in this group was notsignificantly different from reported normals.'8 Althoughevery patient in this group showed incomplete right bundlebranch block, right ventricular hypertrophy, or a completeright bundle branch block pattern, the right-sided elec-tropressor intervals were within normal limits as reported byCurtiss et al.17
For group I, there was a close association between thehangout and splitting intervals on the one hand and the QA,and Q-RV intervals on the other. As the hangout interval on
FIGURE 4. High fidelity right ventricular andpulmonary artery pressure curves in a 61-year-oldfemale with hyperkinetic pulmonary hyperten-sion. Catheterization data revealed a left-to-rightshunt at the atrial level of2.3: 1 and a pulmonaryartery pressure of 75/10 with a mean of 38 mmHg. External splitting of the second heart soundaveraged 40 msec while there is a narrow hangoutinterval of only 15 msec. Lines have been ex-tended down from A, and P2 to show therelationship of the two components of the secondheart sound to the right ventricular pressurecurve. The R V electromechanical interval isprolonged 25 msec beyond the L V elec-tromechanical interval (QA,).
CIRCULATION1 050
by guest on June 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

SECOND HEART SOUND IN ASD/O'Toole, Reddy, Curtiss, Shaver
FIGURE 5. Simultaneous ventricular pressure
curves obtained in a normotensive atrial septaldefect patient who was in atrial fibrillation. Themiddle complex is preceded by a relatively shortR-R cycle with external splitting ofonly 36 msec.
A longer R-R interval precedes the last complexand increases external splitting to 56 msec. Thesimultaneous ventricular pressure curves showthat the total duration of right ventricular systoleis greater in the last complex than it is in the mid-dle complex.
the left is negligible, QA2 is a good measure of the left-sidedelectromechanical interval. 9 Therefore the electro-mechanical intervals for right and left ventricles may beinferred to be almost equal. This suggests that there is a
chronic adaptation by the right ventricle which allows it toeject the increased volume load without significantly in-creasing its duration of systole. Thus, wide splitting of thesecond sound did not appear to be due to prolongation or
shortening of the electromechanical intervals of the rightand left ventricles respectively.The duration of the right-sided hangout interval has been
shown to be related to the status of the pulmonary vascularimpedance or the total opposition to forward flow.19Impedance depends not only on resistance but also on
arterial compliance and capacitance. A consequence of thelong-standing volume overload on the right side of the cir-culation is a large dilated pulmonary artery which ischaracteristic of this disorder. In the normotensive atrialseptal defect, with a marked increase in the pulmonaryblood flow, there must be a normal or low pulmonaryvascular resistance. Thus, the pulmonary vascular bed can
be characterized as a high capacitance, low resistancesystem. It is therefore no surprise that the group of nor-
motensive ASD patients all have in common wide hangoutintervals consistent with the low impedance characteristicsof the pulmonary vascular tree. Nearly equal durations ofright and left ventricular electromechanical intervalscoupled with small, absolute values of the normal left-sidedhangout interval are responsible for a good correlationbetween A2-P2 and the right-sided hangout interval. Consis-tent with the hypothesis that the mechanism of wide splittingis related to the dilated pulmonary vascular bed are thenumerous reports of persistent abnormal splitting of thesecond heart, sound following repair of the atrial septal de-fect."' 10-13 Further support for this hypothesis is found in thewide audible expiratory splitting of the second soundobserved in idiopathic dilatation of the pulmonary arterywhere there is no volume overloading of the right ventricle.'4While one can demonstrate a good correlation between
splitting of A2-P2 and the hangout interval in patients withnormotensive atrial septal defect in sinus rhythm, wide split-ting of A2-P, in other patients with this defect may be due to
prolongation of right ventricular electromechanical systole.The patients in group III with normal or slightly elevatedpulmonary artery pressures who were in atrial fibrillationwere found to have nearly constant hangout intervals in-dependent of preceding cycle length. The relatively narrow
hangout intervals for this group of patients compared to thenormotensive group may be related to an increase in im-pedance of the pulmonary vascular bed that has beenpostulated to occur with increasing age.20 Our findings con-
firm the observation of Aygen and Braunwald that longer R-R cycles are associated with wider splitting of the secondheart sound.8 Two factors appeared to be responsible for thisobservation: 1) QP2 progressively increased with increasingcycle length due to a selective increase in the duration of RVelectromechanical systole, and 2) at relatively long cyclelengths, the duration of LV electromechanical systole was
relatively fixed. It is possible that the explanation of thisfinding is related to the differences in compliance betweenthe right and left ventricles. The longer cycle lengths allowgreater time for diastolic filling and because the left ventricleis thicker and less compliant than the right, there is selec-tively more filling of the right ventricle. This greater fillingof the right ventricle then leads to selective prolongation ofthe right ventricular electromechanical interval with in-crease in the width of splitting of S2. Our observations do notexclude a significant contribution of abnormal left ven-
tricular function to wider A2-P2 splitting. They do document,however, the significant contribution of RV electro-mechanical systole prolongation to this phenomenon.The group II patients had hyperkinetic pulmonary
TABLE 2. Effect of Cycle Length on Splitting in Atrial Fibril-lation
Preceding R-Rinterval Q-A2 Q-RV Q-P2 HO A2-P2(msec) (msec) (msec) (maec) (msec) (msec)
468 320 332 354 22 34644 352 368 390 22 38740 360 380 402 22 42829 362 392 414 22 52940 364 402 424 22 601096 363 413 435 22 72
HO = hangout interval.
1051
by guest on June 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL. 56, No. 6, DECEMBER 1977
NORMOTENSIVE
SISPLITTING
A P
I I
HYPERKINET ICPULMONARY HYPERTENSION
SI AP
11SI
/ Ye
I%l
HANGOUT WIDE
fI,'
NARROW
50
mmHg
NARROW
SYSTOLE RV=LV RV= LV RV > LVFIGURE 6. Schematic representation of the physiologic basis for splitting of the second heart sound in adult patientswith atrial septal defect. On the left are representative pressures for a normotensive ASD. There is wide splitting of thesecond heart sound corresponding to a wide hangout interval and the durations ofright and left electromechanical inter-vals are nearly equal. The middle complex, representative ofhyperkinetic pulmonary hypertension with nearly equal R Vand L V electromechanical intervals, shows narrow splitting of the second heart sound with a narrowed hangout interval.The right hand pressure curves represent hyperkinetic pulmonary hypertension with the R V electromechanical interval oflonger duration than that for L V, leading to wide splitting despite the narrowed hangout interval.
hypertension. This condition has been reported to beassociated with wide splitting of S2 by several observers.21-23Our cases in group II show that a wide range of splitting canbe seen. With hyperkinetic pulmonary hypertension thehangout interval becomes narrower, probably related to in-creased impedance to pulmonary flow. The splitting intervalthen becomes a function of the relative electromechanical in-tervals of the left and right ventricles. If they are ap-proximately equal as in two of our group II patients (N.R.and A.G.), the splitting interval will be narrow. Wide split-ting can be due to several mechanisms, shortening of the leftventricular electromechanical interval, lengthening of theright ventricular electromechanical interval, or both. Whilethe second mechanism appeared to predominate in this sub-set of group II, the number of patients was too small to per-mit adequate assessment of relative prevalence.
Concepts derived from this study relating to the splittingof the second heart sound in ASD are summarized in figure6. In normotensive ASD, the electromechanical intervals ofleft and right ventricles are essentially equal and wide split-ting of the second heart sound correlates well with the right-sided hangout interval. With hyperkinetic pulmonaryhypertension the hangout interval narrows, but the rightventricular electromechanical interval may be either normalor prolonged, tending to result in narrow or wide splitting,respectively. Thus the wide spectrum of splitting of the sec-
ond heart sound encountered in ASD can most often be ex-
plained by taking into account the hangout interval as wellas the relative durations of RV and LV electromechanicalsystoles.
Acknowledgment
We gratefully acknowledge the technical assistance of Jan Brandeburg,R.N., Elizabeth Mackie, and Albert Durica, and the secretarial assistance ofLola Peluso.
References1. Adolph RJ, Fowler NO: The Second Heart Sound: A Screening Test for
Heart Disease. Mod Conc Cardiovasc Dis 39: 91, 19702. Leatham A, Gray I: Auscultatory and phonocardiographic signs of atrial
septal defect. Br Heart J 18: 193, 19563. Kumar S, Luisada AA: The second heart sound in atrial septal defect.Am J Cardiol 28: 168, 1971
4. The cause of the respiratory fixation of a split second sound. In Sym-posium on Congenital Heart Disease, edited by Campbell M. Br Heart J20: 266, 1958
5. Perloff JK, Harvey WP: Mechanisms of fixed splitting of the secondheart sound. Circulation 18: 998, 1958
6. Dimond EG, Benchimol A: Phonocardiography in atrial septal defect:Correlation between hemodynamics and phonocardiographic findingsAm Heart J 58: 343, 1959
7. Eisenberg R, Hu}tgren HN: Phonocardiographic features of atrial septaldefect. Circulation 20: 490, 1959
8. Aygen MM, Braunwald E: The splitting of the second heart sound in nor-mal subjects and in patients with congenital heart disease. Circulation 25:328, 1962
9. DePasquale NP, Burch GE, Phillips JH: The second heart sound. AmHeart J 76: 419, 1968
10. Bedford DE, Sellors TH, Somerville W, Belcher JR, Besterman EMM:Atrial septal defect and its surgical treatment. Lancet 273: 1255, 1957
11. Feruglio GA, Sreenivasan A: Intracardiac phonocardiogram in thirtycases of atrial septal defect. Circulation 20: 1087, 1959
12. Wolf PS, Vogel JHK, Pryor R, Blount SG Jr: Atrial septal defect inpatients over 45 years of age. Br Heart J 30: 115, 1968
13. Saksena FB, Aldridge HE: Atrial septal defect in the older patient - Aclinical and hemodynamic study in patients operated on after age 35. Cir-culation 42: 1009, 1970
14. Schrire V, Vogelpoel L: The role of the dilated pulmonary artery in ab-normal splitting of the second heart sound. Am Heart J 63: 501, 1962
A P
I I
CIRCULATION1052
by guest on June 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

VALVE LEAFLET MOTION IN VIVO/Ilmamura, Kaye, Davis
15. Castle RF: Variables affecting the splitting of the second heart sound inatrial septal defect. Am Heart J 73: 468, 1967
16. Morrow AG, Sanders RJ, Braunwald E: The nitrous oxide test - An im-proved method for the detection of left to right shunts. Circulation 17:284, 1958
17. Curtiss El, Reddy PS, O'Toole JD, Shaver JA: Alterations of right ven-tricular systolic time intervals by chronic pressure and volumeoverloading. Circulation 53: 997, 1976
18. Weissher AM, Harris WS, Schoenfeld CD: Systolic time intervals inheart failure in man. Circulation 37: 149, 1968
19. Shaver JA, Nadolny RA, O'Toole JD, Thompson ME, Reddy PS, Leon
DF, Curtiss El: Sound pressure correlates of the second heart sound: Anintracardiac sound study. Circulation 49: 316, 1974
20. Curtiss El, Shaver JA, Reddy PS, O'Toole JD: Newer concepts inphysiological splitting of the second heart sound. American HeartAssociation Monograph 46: 68, 1975
21. Sutton G, Harris A, Leatham A: Second heart sound in pulmonaryhypertension. Br Heart J 30: 743, 1968
22. Perloff JK: Auscultatory and phonocardiographic manifestations ofpulmonary hypertension. Prog Cardiovasc Dis 9: 303, 1967
23. Besterman E: Atrial septal defect with pulmonary hypertension. Br HeartJ 23: 587, 1961
Radiographic Assessment of Leaflet Motionof Gore-Tex Laminate Trileaflet Valves
and Hancock Xenograft in Tricuspid Position of DogsEISABURO IMAMURA, M.D., MICHAEL P. KAYE, M.D., AND GEORGE D. DAVIS, M.D.
SUMMARY Six samples of various thicknesses of Gore-Tex com-pounds were fashioned into trileaflet valves. A radiopaque marker wasplaced on the center of the free margin of each cusp, and the prostheseswere implanted in the tricuspid position of dogs. Two Hancock valveswere studied for comparison. Catheterization revealed that the hemo-dynamic function was normal in all valves tested. High-speed radiographypermitted analysis of leaflet movement throughout the cardiac cycle. Of
SUBSTANTIAL EFFORT has been directed towardduplicating the natural aortic valve configuration as a modelfor the ideal valve substitute. Minimal flow resistance andturbulence are the principal theoretic advantages of the cen-tral orifice design. In practice, however, once the pathologicprocesses responsible for leaflet stiffening occur, these hemo-dynamic benefits are lost and function deteriorates. Hence,the question is raised whether the use of materials, which areinitially "too stiff" for valve cusp construction, mightlikewise contribute to valve failure.
Increasing evidence supports the concept that thelongevity of a leaflet-type heart valve substitute depends notonly on the mechanical strength and biological and chemicalcharacteristics of the materials employed but also on thedesign,' especially the mode of valve function in vivo.Hydrodynamic function of a model aortic valve has been in-vestigated with a pulse-duplicator2 8 or an in vivo ultrasonictechnique.4' We believe that further progress toward arational choice of an appropriate leaflet material requiresdocumentation of the valve performance characteristics inthe beating heart.
In this study, we used stented trileaflet valves fabricated ofGore-Tex laminate. Gore-Tex (or expanded polytetra-fluoroethylene) is a new synthetic material that possesses
From the Section of Surgical Research and Section of Cardiac Radiology,Mayo Clinic and Mayo Foundation, Rochester, Minnesota.Supported in part by a grant from the Foundation for In-Service Training
and Welfare of the Private School Personnel.Address for reprints: Michael P. Kaye, M.D., Mayo Clinic, 200 First
Street SW, Rochester, Minnesota 55901.Received June 16, 1977; revision accepted July 22, 1977.
the six Gore-Tex valves, five opened completely. The cusps of these fivevalves were fabricated from 4, 6, 8, 10, and 12 layers of Gore-Tex fim.The remainng valve, which was fabricated from 15 layers of Gore-Texfilm, and boti porcine xenograft aortic valves did not open completely.We postulate that the laminates of 12 layers or less of Gore-Tex film aresuitable for further study to evaluate their potential applicability intrileaflet cardiac valve prostheses.
high tensile properties. Its biocompatibility has been studiedin arterial and venous grafts.6-' Additionally, Gore-Texlaminate allows use of materials with a wide range ofthickness. We used porcine xenograft aortic valves for com-parisons. The purpose of this paper is 1) to describe the ini-tial function of these valves in the tricuspid position of dogsassessed by radiopaque markers and high-speed X-raytechniques; 2) to define the thickness of Gore-Tex laminatethat is optimal for a flexible leaflet prosthesis; and 3) to dis-cuss the implications of hemodynamics for adequate long-term function.
Material and Methods
Gore-Tex laminate is manufactured by W. L. Gore andAssociates. A single film of this polymer, 0.003-mm thick,consists of nodules and fibrils of polytetrafluoroethylene(PTFE) and has uniaxial tensile strength that parallels thefibril content. The tensile strength of a single film is 60,000psi - approximately 20 times that of conventional PTFE.For use as valve leaflets, several films are laminated indiverse directions to comFpensate for the absence of the ten-sile strength in the cross-directional axis and to add strength.The Gore-Tex laminate is nonporous and transparent, un-like the Gore-Tex vascular prosthesis, which is microporousand snowy white. The number of laminated films used ineach valve leaflet studied determines the thickness, strength,and stiffness. Six samples constructed from laminates of 4,6, 8, 10, 12, and 15 layers of Gore-Tex film were studied.These samples ranged from 0.008 to 0.031 mm in thicknessas a result of compression during the lamination process.
1053
by guest on June 29, 2018http://circ.ahajournals.org/
Dow
nloaded from

J D O'Toole, P S Reddy, E I Curtiss and J A ShaverThe mechanism of splitting of the second heart sound in atrial septal defect.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1977 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.56.6.1047
1977;56:1047-1053Circulation.
http://circ.ahajournals.org/content/56/6/1047.citationthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 29, 2018http://circ.ahajournals.org/
Dow
nloaded from








![1047 bae[1]](https://static.fdocuments.in/doc/165x107/5562973cd8b42abb398b4d64/1047-bae1.jpg)