Mechanism and Ablation of Arrhythmia Following Total...
28
DOI: 10.1161/CIRCEP.114.001758 1 Mechanism and Ablation of Arrhythmia Following Total Cavopulmonary Connection Running title: Correa et al.; Arrhythmia post TCPC Rafael Correa, MD; Elizabeth D. Sherwin, MD*; Joshua Kovach, MD*; Douglas Y. Mah, MD; Mark E. Alexander, MD; Frank Cecchin, MD; Edward P. Walsh, MD; John K. Triedman, MD; Dominic J. Abrams, MD, MRCP Boston Children’s Hospital & Harvard Medical School, Boston, MA *contributed equally Correspondence: Dominic J. Abrams, MD, MRCP Department of Cardiology Division Cardiac Electrophysiology Children’s Hospital 300 Longwood Avenue Boston, MA 02115 Tel: (617) 355 6432 Fax: (617) 566 5671 E-mail: [email protected] Journal Subject Codes: [22] Ablation/ICD/surgery, [41] Pediatric and congenital heart disease, including cardiovascular surgery, [106] Electrophysiology, [132] Arrhythmias - basic studies P P . . . Wa Wa Wa Wals ls ls lsh h h h , , , , MD MD MD MD ; ; ; ; MRCP CP CP CP ndence : Boston Ch hil ldre e en n’s Ho Ho Hospital a a a & & & Ha arv v vard d M Med ed ed dic ic ic i al al Sch ch chool l, B Bo os o o t to t n, M M M MA A *c *c *c * on n n ntr tr tr trib ib ib ibut ut ut uted ed ed e e equ qu qu qual al al a ly ly ly y nd nden ence ce : : : by guest on June 11, 2018 http://circep.ahajournals.org/ Downloaded from by guest on June 11, 2018 http://circep.ahajournals.org/ Downloaded from by guest on June 11, 2018 http://circep.ahajournals.org/ Downloaded from
Transcript of Mechanism and Ablation of Arrhythmia Following Total...

DOI: 10.1161/CIRCEP.114.001758
1
Mechanism and Ablation of Arrhythmia Following Total
Cavopulmonary Connection
Running title: Correa et al.; Arrhythmia post TCPC
Rafael Correa, MD; Elizabeth D. Sherwin, MD*; Joshua Kovach, MD*; Douglas Y. Mah, MD;
Mark E. Alexander, MD; Frank Cecchin, MD; Edward P. Walsh, MD;
John K. Triedman, MD; Dominic J. Abrams, MD, MRCP
Boston Children’s Hospital & Harvard Medical School, Boston, MA *contributed equally
Correspondence:
Dominic J. Abrams, MD, MRCP
Department of Cardiology
Division Cardiac Electrophysiology
Children’s Hospital
300 Longwood Avenue
Boston, MA 02115
Tel: (617) 355 6432
Fax: (617) 566 5671
E-mail: [email protected]
Journal Subject Codes: [22] Ablation/ICD/surgery, [41] Pediatric and congenital heart disease, including cardiovascular surgery, [106] Electrophysiology, [132] Arrhythmias - basic studies
PP... WaWaWaWalslslslshhhh,,,, MDMDMDMD; ; ; ;
MRCPCPCPCP
ndence:
Boston Chhilldreeenn’s HoHoHospitalaaa &&& Haarvvvardd MMedededdicicici alal Schchchooll, BBoosoo ttot n, MMMMAA *c*c*c* onnnntrtrtrtribibibibututututededed eeeququququalalala lylylyy
ndndenencece::: by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
2
Abstract:
Background - The ability to identify and ablate different arrhythmia mechanisms following the
total cavopulmonary connection (TCPC) has not been studied in detail.
Methods and Results - After obtaining IRB approval according to institutional guidelines,
consecutive patients following a TCPC undergoing electrophysiology study over a 6 year period
were included (2006-2012). Arrhythmia mechanism was determined, and the procedural
outcome was defined as complete, partial success, or failure. A 12-point arrhythmia severity
score was calculated for each patient at baseline and on follow-up. Fifty-seven procedures were
performed on 52 patients (18.4 ± 11.8 years; 53.0 ± 27.2kg). Access to the pulmonary venous
atrium was necessary in 33 procedures, via fenestration (16) or transbaffle puncture (17) and in
two cases an additional retrograde approach was used. In total, 80 arrhythmias were identified in
47 cases: macroreentrant (n=25) or focal atrial tachycardia (n=8), atrioventricular nodal reentry
tachycardia (n=13), reentry via an accessory pathway (n=4) or via twin atrioventricular nodes
(n=4), ventricular tachycardia (n=5), and undefined atrial tachycardia (n=21). Procedural
outcome in 32 patients who underwent ablation was complete success (n=25), partial success
(n=3), failure (n=3), or empiric ablation (n=1). Following successful ablation there was a
significant decrease in arrhythmia score over 18.2 (4 – 32) months follow-up, with a sustained
trend even in the face of arrhythmia recurrence (50%).
Conclusions - Arrhythmia mechanism post TCPC is highly varied, encompassing simple and
more complex substrates, documentation of which facilitates a strategic approach to invasive
arrhythmia management. Despite the anatomical limitations successful and clinically
meaningful ablation is possible.
Key words: congenital heart disease, Fontan procedure, catheter ablation, electrophysiology mapping, arrhythmia, total cavopulmonary connection
p y
afafafafflflflfleeee pupupupuncncncnctutututurererere ((((17171717) ) ) ) anannn
hythmimimimiasasasas wwwwerererere e e e idididdenenenentit f
m e
a (n=13), reentry via an accessory pathway (n=4) or via twin atrioventricular nod
t
n e
u
decrease in arrhythmia score over 18.2 (4 – 32) months follow-up, with a sustain
macrcrcrcrororororeeeeentntntn rarranttt ((((n=25) or focal atrial tachhhhycycy ardia (n=8),, atriiiovovovo entricular nodal ree
a (nnnn=13), reennntrtrt yy vivivivia a a a anananan aaaacccc esesesesssoss ryrry patathhhwayay (n=n=n=n=4)4)4)4 ooor rr vviv aaa twtwwinini atrtrtrrioioiooveeentntnttriiiricucuculalalalar rrr nnonn d
tricicici ululular tachyhhh ccarrdiaaa (((n=5)5)5)5), , , and d d d uunundded fifif nnned attrialaal tacccchyhyyccacarrrdia (n=n===21212121). PrPrPrP occeedurrralll
n 32 pappap tientststst whooo uuunderwewwwent ablation n n n waaaas ss coccc mppplelelete successssss ((n=2525525),),), ppppararartial succea
ure ((((n=3)3)3), , or eeempmpmpm irii iiic ablblblatiioii n (n(n(n( 1=11).).). Follllllowiiing gg successfsfsfsfulll aaablbbb attioii n thhhere wawawawasss s a
dedecrcreaeasese iiin n ararrhhrhhyttythhmhmhmiaiaii sscocorere ooovever r 18181818.22.22 ((((4 44 4 – 322322) ) )) mommmo tntntthshsh ffffollolllololl w-w upup,, wiwiiithththth aa ssusustatainin by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.114.001758
3
Introduction
The Fontan operation has been the primary technique for surgical palliation of patients with
single ventricle physiology since its eponymous description in 1971. Early modifications
incorporated the morphological right atrium within the systemic venous-pulmonary circulation 1-
3, although in its adopted role as the sub-pulmonary chamber the right atrium hindered rather
than contributed to efficient pulmonary blood flow, and provided an ideal electroanatomic
substrate for atrial arrhythmia that contributed to long-term morbidity and mortality. To
overcome these inherent limitations, in 1988 de Leval pioneered a novel surgical variant of the
original Fontan procedure, channeling inferior vena caval blood flow directly to the pulmonary
artery via an “intracardiac baffle” created within the posterolateral aspect of the right atrium4,
generating a “pulmonary venous atrium” (PVA) from the remaining morphological right and left
atria. Subsequently the extra-cardiac connection has been increasingly used5. While these
modifications have improved the hemodynamic profile and reduced arrhythmia burden in the
short term, arrhythmia remain an important longer-term complication6, 7.
By its very nature, the total cavopulmonary connection (TCPC) limits access to a
significant proportion of atrial myocardium using a standard percutaneous approach.
Anterograde access to the pulmonary venous atrium via a fenestration in the intracardiac baffle
or a transbaffle puncture are possible in some cases but allow only a single catheter approach that
may significantly hinder accurate determination of arrhythmia mechanism and ablation. The
purpose of this study was to determine the varied arrhythmia mechanisms following the TCPC
and the feasibility, safety and success of ablation.
Methods
Data from the case records of all patients following TCPC palliation undergoing invasive
vel surggical variantnttt oooof
direcctltltltly y ttoto tttthhhehe ppppululllmommmon
a m
n
s
ons have improved the hemodynamic profile and reduced arrhythmia burden in t
arrh thmia remain an important longera term complication6, 7
an “inininintrtrtracacccararardidd acacacac baffle” created within thehehehe pposterolateraaal aspepepep ct of the right atrium
aaaa “““pulmonaryy vvennouous atattatrrirr umm”””” (PPPVVA) fromm thehehehe rrrremememmainnininnng mmoorphphphp ologgggicccall rrighhht an
sequeentnnntlylyyly the extttra-cardiacccc ccconnececcctitititiononon hhhas bbbbeeeennnn iiini crrcrcreasisisiingnglyll usedddd5555. WWWhihihih llle thehhh se
ons hhah ve iiimppprororooveddd hthhe hheh modydydynamiiiic prpp ffofililile anddd d redudd ceceeedd d arrrrhrhrhhytytythhmh iiaii bbburrdedededen nnn in t
hrh tthhmiia iai ii tta tnt lla tte lpliic tatiio 666, 777
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.114.001758
4
electrophysiology studies (EPS) over a 6-year period (March 2006 - March 2012) was collected.
This study period was based on a stable operator and institutional procedural experience in
invasive EP assessment of the TCPC patients and familiarity with mapping and ablative
technologies, thereby minimizing these as potential confounders in our analysis. All studies
were performed on clinically defined indications at Boston Children’s Hospital.
Electrophysiology study
Electrophysiology studies were performed using standard electrophysiological mapping system
(Prucka, GE Medical Systems, Milwaukee, WI) with electroanatomic mapping (CARTO,
Biosense Webster, Diamond Bar, CA) used where indicated by clinical need. Intra cardiac echo
(ICE) was used on 18 (32%) cases being employed in the majority of the EPS performed after
2009 (video 1). CARTOSOUND (CARTO, Biosense Webster, Diamond Bar, CA) was utilized
creating anatomic shells on most cases were ICE was employed. Catheters were advanced from
the femoral veins to the TCPC baffle and when needed retrograde via the femoral artery to the
systemic ventricle. Anticoagulation with Heparin was used routinely targeting activating clotting
times (ACT) >250 seconds throughout the case. Patients receiving prior oral anticoagulation (9)
were either bridged with heparin (7) or the procedure was performed with a therapeutic INR (2).
Those not formally anticoagulated who required ablation received intravenous heparin until the
following day. Venous pressure was measured within the cavopulmonary circulation and
angiography used if necessary to identify residual leaks or the position of the fenestration.
Access to the pulmonary venous atrium and when necessary the systemic ventricle was
anterograde via a baffle leak, a fenestration fashioned at the time of TCPC surgery, retrograde or
by transbaffle puncture using either a standard or radiofrequency (Baylis, Montreal, Canada)
needle. Atrial plus/minus ventricular programmed stimulation were used for definition of
mapppip ngg ((CARTO,O,O,O,
al neededdd. IIInIntrttrt a a cacardrdddiaiaiaiacc
u f
o l
n f
l
entricle Anticoag lation ith Heparin as sed ro tinel targeting acti ating c
useeeed d dd ononon 1111888 (32%2%2%2%) cases being employed ddd ininii the majority yyy offf tttthehh EPS performed af
ooo o 1). CARTOSOUOUUNNND (((CACCC RTRTRTRTOOO, Bioosensse WeWeWeWebsbsbstttet rr, DDDiiiamoonnd BBBBar, CACACAC ) wwas uututil
natomimimim ccc shshshshells on mo tstt caseseseesss weree IIIICECECECE was empmpmpmpllolol yeyeyeyedddd. CaCaCaC thththt tteters wewewewerre advdd ancedddd f
l veiini s to thehh TCTCTCTCPCPCPCP bbbaffffffllel andddd whheh n ne ddededddd rettrogrgg adddde e iviia thththhe ffeff moral lll arrrrteteteeryryryy to
ttriiclle AA tntiic llatiti itithh HHe iri ded titi ll tt titi tctii tatiin c
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
5
baseline electrophysiological parameters and arrhythmia induction, including isoproterenol when
necessary. Entrainment mapping was used at the discretion of the operator to (i) identify
reentrant circuits within either atrium, or (ii) to define electrogram (EGM) sequence after
cessation of ventricular pacing with 1:1 ventriculoatrial (VA) conduction and atrial entrainment 8
to determine arrhythmia mechanism. Single ventricular premature beats (VPBs) were introduced
during tachycardia at decreasing coupling intervals to assess for atrial reset 9.
EPS and arrhythmia definitions
In analysis of arrhythmia mechanism and underlying electroanatomic substrate the following
definitions were used:
Macroreentrant atrial tachycardia: organized atrial tachycardia with stable cycle length
(CL), EGM morphology and consistent pattern of atrial activation. In each case a complete loop
of atrial activation was demonstrable on electroanatomic activation maps supported by contact
EGM10.
Focal atrial tachycardia: organized atrial arrhythmia with stable CL, EGM morphology
and consistent pattern of centrifugal activation from a focal source.
Atrial fibrillation (AF): irregular pattern of atrial activation with beat-to-beat variability
in CL and morphology with no visually demonstrable area of organized activity 11.
Atrioventricular nodal reentry tachycardia (AVNRT): tachycardia with a regular CL and
either a 1:1 or 2:1 atrioventricular relationship, an AV response on cessation of ventricular
pacing with atrial entrainment, and no atrial reset with VPBs. The VA interval was defined as the
onset of the earliest site of ventricular activation to the earliest atrial EGM recorded within the
pulmonary venous atrium. In the context of the variable anatomy and limited access to the PVA,
AVNRT was classified as typical if the VA interval was <70 ms and atypical if >70 ms.
substrate the follooowiwiww n
croreentrant atrial tachycardia: organized atrial tachycardia with stable cycle len
M e
t
cal atrial tach cardia: organi ed atrial arrh thmia ith stable CL EGM morpholo
crororororeeeeeeeentnntrarararantnn aaatrtrtrtrial tachycardia: organizedededed aatrial tachycaraa dia aa a wiww th stable cycle len
M mmmom rphology aand coonsiiisststentttt ppatttteern of attriial aaactctcttivivivvaatiooonnn. Inn eeaccchh h caseeee aaa ccoompppleeete
tivatititiiononoon wwas ddddemon ttstrablllleeee oonon electctctctrororoaaanatttomic aaaactivivivivatioioioi nnn n maps supupupupppopop rteddd bbbby con
lal ttriiall tta hch didi ii ded ttriiall hrh tthhmiia itithh tst bablle CCLL EEGMGM hph lol
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.114.001758
6
Atrioventricular reentry tachycardia (AVRT): tachycardia with a regular CL and a 1:1
atrioventricular relationship, an AV response to cessation of ventricular pacing with atrial
entrainment, and atrial reset with VPBs.
Twin AV nodal tachycardia was defined by the presence of two non-preexcited QRS
morphologies each with a distinct His EGM, decremental anterograde and retrograde conduction,
and regular tachycardia CL with 1:1 atrioventricular relationship anterograde over one AV node
and retrograde via the alternate node 12. An AV response was seen with cessation of ventricular
pacing with atrial entrainment.
Ablation and definition of success
Conventional (50W/70oC) and irrigated radiofrequency (48W; 30mls/min) ablation were
standardly used. If the ablation site was close to the native conduction system then cryoablation
(-80oC) was used at the discretion of the individual operator. Ablation was considered successful
for any given mechanism if termination of arrhythmia was seen during the application of energy
in the absence of atrial ectopy and subsequent failure to reinduce the previously identified
tachycardia, or non-inducibility alone if ablation was performed during sinus rhythm.
Procedural case success was considered complete if all inducible arrhythmia mechanisms
were successfully ablated and partial if some, but not all, arrhythmia substrates were eliminated.
Arrhythmia recurrence was defined by documented arrhythmia on either ECG or pacemaker
telemetry.
Clinical arrhythmia severity score
Arrhythmia burden during the three months prior to EPS was assessed using a clinically relevant
12-point scoring system sub-divided into four categories (table 1) 13. An arrhythmia score was
calculated for each patient at baseline and on each clinical encounter during follow-up where
n
used. If the ablation site was close to the native conduction system then cryoabl
as used at the discretion of the individual operator. Ablation was considered succ
ven mechanism if termination of arrhythmia was seen during the application of en
nce of atrial ectop and s bseq ent fail re to reind ce the pre io sl identified
nalll (((5050505 W/W/W/W/70770oC)C)C)C) and irrigated radiofrequeueuencncn y (48W; 3000mlm s/s/s//mmmin) ablation were
uuuuseeeed. If the ablblatioonn sitetete wass cloosse too thee nnatiiiivevevee ccccoondduductionn syyystttem tttthehehenn ccryoooaaabl
as useeeeddd attatat the dddiiiscr ttetiiiion ofofofof ttthehhehe inddddivivivividiididuual lll opoperatatatatoooor. AAAAblblblb atatata ioi n was cocococonnsidddder dded succ
ven mechhhaniisi m mmm ififff termiiinatiiiion offf ar hhrhhytytythmhhh iiia was seen dududuu iriingngng tttthheh appppppliliicatititiionononon oooof en
ff tat iri lal tct dd bbs tnt ff iaill tt iindd tthhe ii lsl idid titififi ded
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
7
data was available.
Follow-up and adverse events
Adverse events were defined as any anticipated or unanticipated event for which injury could or
did occur as a consequence of performing the EP study, and assigned a severity level as trivial,
minor, moderate, major or catasthrophic. 14 Pre and post procedure pulse oximetry data was
obtained from clinic visits and follow up encounters when available, and patient or physician
concerns regarding worsening cyanosis were collected.
Statistical analysis
The Kolmogorov-Smirnov test was used to assess normal distribution. Variables with
approximately normal distribution were expressed using mean (standard deviation) and those
with non-parametric distribution using median (interquartile range). Comparison between
clinical arrhythmia scores at baseline and follow-up was made using the Wilcoxon signed rank
test.
Results
Patient demographics
In total of 57 EP procedures were performed in 52 patients (age 18.4 ± 11.8 years; weight 53 ±
27.2kg), of whom 48 had an intracardiac and 4 an extracardiac TCPC. Two patients had
undergone prior surgical conversion from an atriopulmonary Fontan with concomitant
arrhythmia surgery, and 5 patients had a repeat EPS during the study period. Arrhythmia had
been documented before in 45 patients, and at least one anti-arrhythmic agent had been used in
38, including amiodarone (n=6). The clinical Indications for EPS were palpitations (n=33),
syncope with (n=4) or without palpitations (n=2), documented arrhythmia (n=10), cardiac arrest
. Vaaririiiabbbablellless iwiwiitththt
tely normal distribution were expressed using mean (standard deviation) and tho
h r
tely y yy nononon rmrmmmalalalal disisisttrtt ibution were expressed uuusising mean (statatandddarararard deviation) and tho
aaara aaama etric distribbutttioon uuusisisiing mmedddian ((innnterqrquartrtrtillilee e e rrrangggeee). CCompmpmparissssonnn bbeetweeeen
hythhhmimimimiaaa scores at tt bbbbaselineeee aaand follllllllowowow-up p was mmmmadededede usisisingngngn thththe WiWiWiilclclclcoooxo on siiignedddd r
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.114.001758
8
(n=2) and asymptomatic ventricular pre-excitation (n=1). Eleven patients had permanent atrial
(n=10) or dual chamber (n=1) pacemakers implanted. Overall follow-up of greater than 3
months was available in 42 patients (81%) with no follow-up in 10 (19%).
Catheterization Data
The mean cavopulmonary pressure measured in 46 patients was 16.1 ± 4.1mmHg. Access to the
pulmonary venous atrium was required on 33 occasions and was achieved via a fenestration
(n=16), using a transbaffle needle (n=14) or radiofrequency puncture (n=3). A retrograde aortic
approach was used in combination with the transbaffle approach in two cases.
Arrhythmia mechanism and ablation
Eighty distinct arrhythmia substrates (CL 312 ± 78ms) were induced in 47 patients further
defined as follows:
a) Macroreentrant atrial tachycardia
Twenty-five different circuits (CL 277 ± 55ms) were identified in 17 patients (range 1-4 per
patient) using activation mapping alone (13) or in combination with entrainment mapping (12).
Using activation mapping 92 ± 5% of the tachycardia CL could be accounted for. The
cavotricuspid isthmus or CTI (cavomitral in L-looped ventricles) was critical to 14 circuits
(56%), all of which were successfully ablated at this site, either within both the intracardiac
baffle and pulmonary venous atrium (10) or in the pulmonary venous atrium alone (4)(figure 1).
A further 11 circuits (44%) were independent of the CTI, of which 8 were located and
successfully ablated within the intracardiac baffle and 3 were confined to the pulmonary venous
atrium. Of the latter, two were successfully ablated at the mitral isthmus and posterolateral
chamber, respectively and a third circuit appeared dependent on an inaccessible section of the
anterior morphological right atrium. In the 5 patients without a CTI-dependent circuit, 2 had
o cases.
t
f
e
v e
ing acti ation mapping alone (13) or in combination ith entrainment mapping (
tincccctt tt aarara rhrhrhrhytytyty hmhmhmh iaiaia substrates (CL 312 ± 78m8m8ms)s were inducecc d ininini 47 patients further
ffffolooo lllol ws:
eenttraaanttntnt atriaiii lll tttachhhycardididiiaaaa
ve dididid fffferent cicicircrcrcrcuiiiits (((CLCLCL 2227777777 ± 55555m5 s)s)s)) were idididden ititififififi dedd iiiin n 171717 pppataata ieii nts (r(r(r( angegeege 1111---4444 pepp
ii tctii tatiio iin lal (1(13)3) iin bibi titi itithh ttr iai tt iin ((
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
9
empiric CTI ablation as part of the overall ablative strategy.
b) Focal atrial tachycardia
Eight focal tachycardias (CL 380 ± 57ms) were identified in 5 patients using activation mapping
of sustained tachycardia in 7 cases and P-wave morphology during atrial ectopy in 1 case where
tachycardia could not be sustained. Six foci were within the intracardiac tunnel, and 2 in the
pulmonary venous atrium (figure 2). All 7 sustained tachycardias were successfully ablated.
c) AVNRT
Thirteen different AVNRT patterns were seen in 8 patients, of which 7 were typical (VA interval
33-65ms) and 6 were atypical (VA interval 176-260ms). Four patients had both typical and
atypical patterns, one had two atypical patterns (figure 3a), and one had typical AVNRT in the
upper of twin AV nodes. During programmed atrial stimulation, dual AV nodal physiology as
defined by recognized criteria was seen in only one patient. Using single VPBs in tachycardia at
progressively shorter coupling intervals to ventricular refractoriness (maximal V1-V2 interval
achieved 110-180ms), atrial reset was not encountered in any patient. Transient 2:1 AV block
was seen in 2 patients during tachycardia without change in the VA interval. Ablation was
attempted in 7 of 8 patients using RF alone (n=2), cryotherapy alone (n=3) or both (n=2), with
successful modification of AV nodal conduction properties in 6 patients.
d) Accessory pathway mediated AVRT
Orthodromic AVRT was seen in 4 patients. Two patients had manifest pre-excitation on surface
ECG, one of whom was asymptomatic with rapid pathway conduction demonstrable on a prior
limited study. The pathway refractory period was 280ms in both cases. Both cases with
concealed pathways showed VA conduction that was non-decremental and/or resistant to
adenosine. AVRT was induced in each case, although the preexcitation index was calculated in
7 were tyypip cal (V(VA A A A ininii
s hadddd bbbb totothhhh ttyttypipipipicac llll anaanandd
at
win AV nodes. During programmed atrial stimulation, dual AV nodal p siology
r
e r
10 180ms) atrial reset as not enco ntered in an patient Transient 2:1 AV blo
tteeernrnrnrnssss, ononnneee hahahad dd two atypical patterns (figggguuru ee 3a), and onnne hahahaddd typical AVNRT in
wiiiin AV nodes.. DDuurriniing prprprograammmmed aatttriall sstimmmmulululaaata iionnn, ddduall AVAVVV nnodaalaa ppphyhysiooolooogy
recogogogognininizzzzed critititeriaiii was seeeeeee nn in onlnlnln y y oone papatittt enenenenttt.t UsUsUsUsinnngggg siiinglelll VVVVPBPBPBPBs in tttachyhhh car
ely yy hshhorter coooupupupu lilililinggg iiintervallsl tto ve tntriculllar refrff actoriiineesss (((mamamaaxiiiimallll V1V1V11-V-V-VV2222 ininininter
1010 118080 )) ttriiall tt tt tte dd iin tatiie tnt TT iie tnt 22 1:1 AAVV blbl
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
10
only one case (70ms) due to hemodynamic instability or CL variability in the others. A single
accessory pathway was seen in each patient (2 posteroseptal and 2 left posterior), and ablation
was successful in all 4 cases. Of note, both patients with concealed pathways had undergone
prior ablation of manifest pathways located at different anatomical sites.
e) Twin AV nodal tachycardia
Twin AV nodes facilitated 4 patterns of reentrant tachycardia in 3 patients who all had the
anatomical triad of atrial isomerism, atrioventricular septal defect and discordant VA
connections. In two cases, anterograde conduction was exclusively via the superior AVN during
tachycardia, and via either the superior or inferior AVN in a single case (Figure 3c). Ablation
was successfully performed in 1 patient and deferred in two due to the risk of atrioventricular
block in minimally symptomatic patients.
f) Other atrial arrhythmias
An additional 21 atrial arrhythmias were induced in 14 patients, which led to hemodynamic
instability (n=2), were not considered clinically relevant (n=6), degenerated to AF necessitating
cardioversion (n=1) or were non-sustained (n=12). These were not mapped in sufficient detail to
define mechanism nor was ablation performed.
g) Ventricular tachycardia
Ventricular tachycardia (VT) was recorded in 5 patients, two of them with previously
documented VT. The three remaining had a history of syncope and were inducible via
ventricular drive trains with 3 extrastimuli. One patient underwent ablation for repeated episodes
of monomorphic VT despite amiodarone therapy, which was ultimately unsuccessful. The
clinical relevance of VT in the other 4 patients remains uncertain. None of these patients had
atrial arrhythmias identified during the study.
a the supperior AVVVVN N NN d
se (FFigigiigururee 3c3c33 )).)). AbAbAbAblalalalatiti
s l
i
t
nal 21 atrial arrhythmias were induced in 14 patients, which led to hemodynamic
(n 2) ere not considered clinicall rele ant (n 6) degenerated to AF necessita
ssfululullylylyl pepepeerfrfrfrfoormemememed in 1 patient and deferredededed in two due to oo thhhee e e rirr sk of atrioventricul
innnnimmmmally sympptoomatatattiic pppatatatienttntss.
trial ll araarrhrhrhrhytyy hmhhh iiai s
nal 212121 atriiai lll arararrrhrhrhrhytytythmhh iiias were iii ddnduced iiiin 141414 pppattients, wwwwhihihih chchch llll deddd to hhehh modydydydynananaamic
((n 22)) tt idid ded lili ini llll lle tnt (( 6)6) dde ttedd tto AAFF itita
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.114.001758
11
h) Non-inducible patients
Of the 5 patients with no inducible arrhythmias, four patients were symptomatic with atrial
tachycardia pre-EPS, with tachycardia documented in 3 patients on prior non-invasive
assessment. The fifth patient, who had no prior arrhythmia history but known severe ventricular
dysfunction and prior cardiac arrest, underwent empiric CTI ablation based on the possibility of
rapidly conducted atrial tachycardia
Patient outcomes:
Ablation & arrhythmia recurrence
Overall 32 of the 52 patients underwent ablation, complete procedural success was achieved in
25 patients (76%), partial success in 3 (9%), failure in 3 (9%) and empiric ablation in 1 (3%).
Five patients had second procedures in this time. One patient did not undergo ablation on the
first EPS but subsequently had a successful ablation. Four had second procedures for arrhythmia
recurrence at 8 days, 2, 11 and 39 months all following acutely successful ablation procedures.
The same arrhythmia mechanism was seen in 1 but a different mechanism in 3. The second
procedure was successful in 2, partially successful in 1 and no ablation performed in the final
patient due to induction of only non-specific atrial arrhythmia. Including patients who underwent
two procedures, of the 28 patients who had an initial ablation with either complete or partial
success, follow-up data was available for 22 (79%), of whom 11 (50%) had documented
arrhythmia recurrence.
Clinical Arrhythmia Severity Score
Over a median follow-up of 18.2 (4 - 33) months in 45 patients, 5 (2 - 8) arrhythmia scores were
recorded per patient. Arrhythmia scores are displayed in figure 4. Scores at follow-up in those
with documented arrhythmia recurrence were higher than those without, although a trend in
succcesesss wawass acachihihihievevevevee
(76%), partial success in 3 (9%), failure in 3 (9%) and empiric ablation in 1 (3%
n t
u y
u
arrh thmia mechanism as seen in 1 b t a different mechanism in 3 The second
(7776%6%6%6%),))) pppparaartialalal success in 3 (9%), failure ee ininii 3 (9%) and dd emmmpipipiric ablation in 1 (3%
ntttst hhhhad secondd pprocccededurrresess in tthhhih sss ttimee. Onene patatatieieientntntn diid not uundddderrgo aaaabblb aatioon ononon t
ut suubsbsbsbseqqeqequentttllly hhhhaddd a succecececessful lll abababablallalatititition. FFFFouuuurrrr hahahah ddd d seeeccococ nddd proceeeedudududures fffor ar hhhrhy
at 8888 dadd ysyy , 2,22 11111 and dd 393939 monthhhs llall ll fofff llll owiiinggg ac tut llelyyy suuccccc essfsfsff lulll abbblalll tiiion pppprororor cccec du
hh thth imi hch iis ii 11 bb tt didiffff tt hch iis iin 33 ThTh dnd
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
12
reduction from pre-procedure scores was still evident at >24 months follow-up despite
recurrence. In those with no arrhythmia recurrence, the median arrhythmia score at 24 months
remained at 1, with the loss of statistical significance likely relating to small numbers.
Adverse Events
Two major adverse events occurred during the study. A 47-year old man died 6 days after an
unsuccessful procedure following the onset of a wide complex tachycardia from which he could
not be resuscitated. A 31-year old male suffered a pulmonary embolus to the left lung diagnosed
on thoracic CT scan from which he made a full recovery. In addition, one patient who had
previously suffered an out-of-hospital cardiac arrest prior to EPS died from multi-organ failure 1
month later, having undergone an empiric cavotricuspid isthmus ablation during that admission.
Minor adverse events included two cases of transient atrioventricular block following AVNRT
and AVRT ablations respectively, and one case each of groin hematoma, and femoral venous
bleeding post-procedure.
There were four patients in whom an arbitrary drop in the pulse oximetry of greater than
5% was recorded when the pre-procedure saturation was compared to that during follow up
clinic encounters. Two of them had a transbaffle puncture performed during the procedure and
two did not, and no study patients had worsening cyanosis recorded as one of their main follow
up complaints or, as a concern from their referring cardiologist.
Discussion
These findings represent the largest published experience of catheter ablation following the
TCPC reported to date, providing novel information on both arrhythmia mechanism in a
heterogeneous population with single ventricle physiology and the feasibility of detailed
mapping despite the anatomical constraints. The major findings are as follows: First, arrhythmia
one pap tient who hahahahadd d
fromm mm llulultitititi-o-orgrggganannn ffffaaiai
r, having undergone an empiric cavotricuspid isthmus ablation during that admis
e N
T o
o
ere ere fo r patients in hom an arbitrar drop in the p lse o imetr of greater
r, hhhavavavavinininngg g ununu deeergrgrgr one an empiric cavotricuucuspspid isthmus aaablatatattioioion during that admis
errrsr eee e events inccluudededed twooo caseses ooof trannsssiennt atririririovovvveneene triccuuular blockckckc follololl wiwiw nng AAAVVVN
T ablllatatatatioioionnnns respe ttctiviii llely, andndndn one cacacaasesese each hh ffoff gggrorororoininin hhhhemmmmatatatatoma, andndndnd ffffemor llall venoddd
ost-prpp ocedddure.ee
e ffo tatiie tnt iin hho brbitit dd iin tthhe ll ii ttr fof tat
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
13
mechanism is highly varied, encompassing reentrant circuits, focal atrial tachycardia and the
more common substrates, atrioventricular nodal and atrioventricular reentry utilizing either an
accessory pathway or second AV node. Second, despite limited catheter access to the
pulmonary venous atrium, successful mapping, mechanistic determination and delivery of
ablation lesions is possible. Third, using a clinically relevant arrhythmia scoring system,
successful ablation is associated with a reduction in score with a trend that persisted even in the
presence of arrhythmia recurrence.
Arrhythmia mechanism
A mechanism for reentrant arrhythmias following the intracardiac TCPC was first proposed
using animal models. Suture lines created along the posterolateral wall of the right atrium
created a line of intercaval conduction block, permitting the development of a reentrant circuit
using the tricuspid annulus as the anterior central barrier, analogous to classical atrial flutter
where the crista terminalis acts as the posterior obstacle. Reentry could be induced acutely using
programmed extra-stimuli 15, or was initiated spontaneously by atrial extra-systoles 16. Initiation
of tachycardia could be prevented by creation of a further line of fixed block between the suture
line and the tricuspid annulus to interrupt the circuit 17. The data presented here would support
the clinical relevance of peri-tricuspid circuits traversing the CTI, which was the most common
single mechanism seen in 14 of 25 cases, suggesting this is a site to target using activation and/or
entrainment mapping. In all CTI-dependent circuits, successful ablation required access to the
pulmonary venous atrium to create the line between the tricuspid annulus and inferior vena cava;
no complications related to transbaffle puncture were encountered.
Interestingly, 8 of the 11 non-CTI dependent reentrant circuits and 6 of 8 focal
tachycardias were located within the intracardiac baffle, suggesting that the hemodynamic
PC wawas s fifififirsrstttt pproropopooosssesedd
m
ne of intercaval conduction block, permitting the development of a reentrant circ
r e
crista terminalis acts as the posterior obstacle. Reentry could be induced acutely
ed e tra stim li 15 or as initiated spontaneo sl b atrial e tra s stoles 16 Init
mal mmmmododododelelells.s.s.s Suuuutututut re lines created along thehehehe pposterolateraaal waaaallllll of the right atrium
nnnen of intercavvall conoonddductcttctiioii n blblblbloccckk, pererrmitttiing thththe e e ddeveeelllopmmeent t t oofo a rrreeeeeee nttraant circ
ricuspippipidddd aaaannulull s as ttthhhhe antntnttererereriiiior ceeentntntntraaallll babbb rrieiii r, aaaanananalololoogooouuusu ttto llcllassisisisicacacacallll attttriii llall ffflulll tttttte
crista termiiinaaalililiis acts as thhhe popp stterioii r obstacle. RRRReenttryryy couldldldd bbbbe iiinddudd cedd d acacacacututututelyyy
ded tt tstiim llii 151515 ii inititi tat ded tnt ll bb tat iri lal tt tst lol 161616 II initt
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
14
burden imposed by the pulmonary circulation has the ability to remodel a small section of atrial
myocardium including the crista terminalis sufficiently to facilitate arrhythmia.
More simple substrates including AVNRT and AVRT via either an accessory pathway or
a second AV node were prevalent, accounting for 21 different arrhythmia in 15 patients. Those
with relatively slow cycle length and 1:1 AV relationship may appear similar to focal atrial
tachycardia, although accurate differentiation can be performed using simple pacing maneuvers
such as the AV response on cessation of pacing.8, 9. The emergence of more common arrhythmia
substrates and specifically AVNRT may reflect the natural history of congenital cardiac surgery
over the last three decades, where palliative surgery was offered to infants with increasingly
complex cardiac disease potentially involving the intrinsic conduction system. In this study 4 of
8 patients with AVNRT had both typical and atypical variants, much higher than would be
typically seen in patients with a normal heart 18. Such mechanisms should be actively considered
in the presence of a 1:1 AV relationship, and may be highlighted by those with recurrent,
spontaneously terminating arrhythmia.
Empiric ablation at sites of slow conduction and/or low electrogram amplitude with a
view to prevent further arrhythmia recurrence was not routinely performed during this study. It
was our practice to address all inducible arrhythmias where possible. The decision to undertake
such an ablative strategy should be balanced between the true potential for future arrhythmia
reduction and the potential for incomplete, pro-arrhythmia lesions, and should be performed in a
highly individualized manner.
Patient outcomes
Despite advances in arrhythmia mapping and ablative technology, arrhythmia recurrence remains
significant in the TCPC population, a major issue in prior iterations of the Fontan procedure.
congeg nital cardiac c c susususur
fants wwiititithhhh iniini crcreaeasisisiingngngnglyly
a y
w
e s
e
sl terminating arrh thmia
ardddiaiaiaccc c dididid seseses asaa e ppopp tentially involving the inininintrttrinsic conduccctionnnn sssystem. In this study
wwwwithhh h AVNRT haad boboboth ttttyyypy icalalall andnnd attypppicaal vaaariririr anananantss, mumumuch hiigheheheh r thananaa wwooulddd bbbe
een iiin nnn paapapatititit entsttt witititi h hhh a normmmmallalal heartrtrtt 1818181 . SSSuchhh h mememechchchc ananananiiisi msmsmsms shohh uld bebebeb aactiv llely cons
ence offf a 1 1:11 AAAAV VVV rellal tiiionshhhhipipip, andd d may yy bbbe hhhigigigi hlhlhlligigighhth edddd bbbby yy thththosooo e withhthh recururururrererer ntnnn ,
lsl tte iin tatiin hrh tthhmiia
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
15
Five patients had a second procedure during the study period with a different mechanism seen in
3. This suggests an ongoing process of remodeling and arrhythmogenesis secondary to the
underlying hemodynamic limitations of the circulation, as noted in previous reports 19. However
the wisdom of using arrhythmia recurrence as the only marker of success for electrophysiology
study and catheter ablation has been questioned previously, prompting the development of the
arrhythmia scoring system used here 13. The persistent improvement seen in those who
underwent ablation, and the sustained trend even in the face of arrhythmia recurrence, supports
the notion that symptomatic improvement is not driven only by complete arrhythmia elimination.
Two serious adverse events occurred during the study; a pulmonary embolus presumably
related to thrombus developing within the intracardiac baffle after the ablation, and a fatal
arrhythmic storm several days after a failed procedure. These serve as a reminder of the
potential instability of patients following single ventricular palliation and the importance of
vigilant peri-procedural care. Despite the potential issues related to catheter stability during
ablation and potential for anomalous locations of the atrioventricular conducting system within
these patients, only 2 cases of transient AV block occurred. Synchronous dual chamber pacing
in the single ventricle population not only necessitates epicardial lead placement with the
associated procedural morbidity, but may be associated with significant decrease in ventricular
function and change in morphology secondary to the dyssynchronous effects of single site
pacing. Cryoablation with the benefits of catheter adhesion may limit the potential for AV
block.
Study limitations
This study is a retrospective analysis of 52 patients undergoing clinically necessitated
electrophysiology studies and ablation. The specific approach to each case was based on
ete arrhyythmia elimimmmini
onaryy eembmbbb lolollusus pppreeeesusususum
h
c
nstability of patients following single ventricular palliation and the importance of
r g
nd potential for anomalo s locations of the atrio entric lar cond cting s stem i
hromomomombubububusss dedededeveeelololoping within the intracardidididiacc baffle after rr the eee aaablation, and a fatal ff
sssstoooorm severall ddayyys afteeer r r a faaaililileddd pprooceeeduuree. TTTThehehesesses seerervvve aas a rerreminddddeere ooff theee
nstabbbbililiilitiitityyy of p ttatiiienttts fofff llowwwwinining siingngngglellele ventttriiiculullularararar ppalalalallllil atatatioioioi n and ddd thhhheeee imimimimpo ttrtance of
ri-prpp ocedddur lall ccccare. DeDD spppiitite the popp tte tntialll iiissues relllateddd d totototo catatathehehehetter sttabbbililililititittyy y y dududuuringgg
dnd tot titi lal ff llo ll tatiio ff thth tat iri ttriic ll dd tctiin tst ii
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
16
operator preference rather than a pre-determined protocol. Limited number of catheters within
the pulmonary venous atrium during tachycardia prevented the use of certain pacing maneuvers
that may have provided additional benefit in mechanistic determination, for example assessment
of the post-pacing interval corrected for AH delay to differentiate AVNRT from AVRT 20. The
analysis of the arrhythmia score on the subgroup of patients with arrhythmia recurrence was
limited by the fact that a documented arrhythmia itself would by definition increase at least 1
point and by up to 3 the total score. In this setting the fact that there was a strong sustained trend
of lower arrhythmia scores would suggest improvement in the overall clinical status that was
reflected on the other measured components of the scale. Finally, due to the referral pattern to
our institution, follow-up data is not uniform or complete.
Conclusions
Arrhythmia mechanism following the total cavopulmonary connection is varied, and relates to
the underlying anatomy, surgical procedures, and ongoing hemodynamic effects on atrial
myocardium. Despite the anatomical limitations imposed, successful mapping and ablation are
possible with sustained clinical benefit. Based on the findings reported here, a sequential
approach to arrhythmia mechanistic determination may be adopted.
Funding Sources: This study was possible due to generous support from the Sean Roy Johnson
Research Fund
Conflict of Interest Disclosures: John K Triedman MD is a consultant for Biosense Webster,
Inc. and Boehringer Ingelheim with a modest level of reimbursement (<10,000 US/year).
Dominic J Abrams MD, MRCP: Stock owner in Johnson and Johnson less than 5,000 US.
clinical status thatattt wwwwa
to thhhhee rerefeffferrrralalll pppatatttteteteterrnrn
t
n
a mechanism following the total cavopulmonary connection is varied, and relates
y
m Despite the anatomical limitations imposed s ccessf l mapping and ablation
tion,n,nn ffffolololo lololoow-w-w upppp dddata is not uniform or compmpm lete.
nnnsn
a mececcchahhahanininin sm fff llolllolll iiiwing thehehehe ttttotal cccavavava opoop llullmonanaryryryry cononononneeectctctc ion iiisi vararararieieieeddd,d, anddd relll ttates
yiyy nggg anatomymymy, sssus rgggicii llal ppprocedures, and ongggoiiinggg hhhhemododynynyny ammmicicii effffffects on atatatatririirial
DD ipitte tthhe tto imi ll lili imittatiti iim dd ff ll iin dnd blbl tatiio
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
17
References:
1. Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax. 1971;26:240-248.
2. Kreutzer GO, Schlichter AJ, Kreutzer C. The Fontan/Kreutzer procedure at 40: An operation for the correction of tricuspid atresia. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu.2010;13:84-90.
3. Bjork VO, Olin CL, Bjarke BB, Thoren CA. Right atrial-right ventricular anastomosis for correction of tricuspid atresia. J Thorac Cardiovasc Surg. 1979;77:452-458.
4. de Leval MR, Kilner P, Gewillig M, Bull C. Total cavopulmonary connection: A logical alternative to atriopulmonary connection for complex fontan operations. Experimental studies and early clinical experience. J Thorac Cardiovasc Surg. 1988;96:682-695.
5. Marcelletti C, Corno A, Giannico S, Marino B. Inferior vena cava-pulmonary artery extracardiac conduit. A new form of right heart bypass. J Thorac Cardiovasc Surg.1990;100:228-232.
6. d'Udekem Y, Iyengar AJ, Cochrane AD, Grigg LE, Ramsay JM, Wheaton GR, Penny DJ, Brizard CP. The Fontan procedure: Contemporary techniques have improved long-term outcomes. Circulation. 2007;116:I157-164.
7. Stephenson EA, Lu M, Berul CI, Etheridge SP, Idriss SF, Margossian R, Reed JH, Prakash A, Sleeper LA, Vetter VL, Blaufox AD, Pediatric Heart Network I. Arrhythmias in a contemporary fontan cohort: Prevalence and clinical associations in a multicenter cross-sectional study. J Am Coll Cardiol. 2010;56:890-896.
8. Knight BP, Zivin A, Souza J, Flemming M, Pelosi F, Goyal R, Man C, Strickberger SA, Morady F. A technique for the rapid diagnosis of atrial tachycardia in the electrophysiology laboratory. J Am Coll Cardiol. 1999;33:775-781.
9. Miles WM, Yee R, Klein GJ, Zipes DP, Prystowsky EN. The preexcitation index: An aid in determining the mechanism of supraventricular tachycardia and localizing accessory pathways. Circulation. 1986;74:493-500.
10. Ouyang F, Ernst S, Vogtmann T, Goya M, Volkmer M, Schaumann A, Bansch D, Antz M, Kuck KH. Characterization of reentrant circuits in left atrial macroreentrant tachycardia: Critical isthmus block can prevent atrial tachycardia recurrence. Circulation. 2002;105:1934-1942.
11. Haissaguerre M, Hocini M, Sanders P, Sacher F, Rotter M, Takahashi Y, Rostock T, Hsu LF, Bordachar P, Reuter S, Roudaut R, Clementy J, Jais P. Catheter ablation of long-lasting persistent atrial fibrillation: Clinical outcome and mechanisms of subsequent arrhythmias. JCardiovasc Electrophysiol. 2005;16:1138-1147.
12. Epstein MR, Saul JP, Weindling SN, Triedman JK, Walsh EP. Atrioventricular reciprocating
pupupupulmlmlmlmononononarararary y y y ararararteteteteryryryry diovasascc SSSuSurgrg.
m Y, Iyengar AJ, Cochrane AD, Grigg LE, Ramsay JM, Wheaton GR, Penny DJP
son EA, Lu M, Berul CI, Etheridge SP, Idriss SF, Margossian R, Reed JH, PrakaA, Vetter VL, Blaufox AD, Pediatric Heart Network I. Arrhythmias in a contempo J
l 2010;56:890 896
mmm m YY,YY Iyenggggararar AAAAJ,, CCCococochrhhh anannane eee ADADADA , ,, GrGrGrigigigg gg LEE,, Raaamsmsmsmsayaaya JJJJM,M,M,M WWWhehhh atonononn GGGGR,RR PPPenenene nynynyy DJP. TTThT e Fontan pprroceeedddureee: Contttntemmmpporaarrry tecechnnnniqiqiqi ueueueues haaavvve impmprooovved loooonngn --teermmm CiCiCirccculationnnn. 22007;;;116:III15155157-161616444.4
son EAEAEAE ,,, LuLuLu MMMM,,,, BeBeBerururur l l l l CICICIC ,, EtEtEtE heeheriririr dgdgdgdge e e e SPSSS , IdIdIdI rirrissssssss SSSSF,F,F,F MMMMarararargogogogossssssiaiaiaian n n n R,RR,R RRRReeeeeee d d d JHJHJHJH,, PrPrPrPraka aA, VeVVV tter VVVL,LL BBBBla ffufox AAAD,DD PPPeddddiiiatriiic HHHeart NNNNetwo kkrk III. ArArArA rhhhytytytthmhmhmhmiaii s iini a ccccononononteteteemppport: Prevaaaalelelelencncncnceeee anananand ddd clcc ininininicicicicalalal aaassssssssocococo iaiaiaiatitititionononons s s s inninin aaaa mmmululuultititiicececeentntn erererer ccccrorororossssssss-s-s-ssecececectitiitionononnalalaal study. J
ll 20201010 5;566:898900 898966
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
18
tachycardia involving twin atrioventricular nodes in patients with complex congenital heart disease. J Cardiovasc Electrophysiol. 2001;12:671-679.
13. Triedman JK, Alexander ME, Love BA, Collins KK, Berul CI, Bevilacqua LM, Walsh EP. Influence of patient factors and ablative technologies on outcomes of radiofrequency ablation of intra-atrial re-entrant tachycardia in patients with congenital heart disease. J Am Coll Cardiol.2002;39:1827-1835.
14. Bergersen L, Gauvreau K, Marshall A, Kreutzer J, Beekman R, Hirsch R, Foerster S, Balzer D, Vincent J, Hellenbrand W, Holzer R, Cheatham J, Moore J, Lock J, Jenkins K. Procedure-type risk categories for pediatric and congenital cardiac catheterization. Circ Cardiovasc Interv.2011;4:188-194.
15. Rodefeld MD, Bromberg BI, Schuessler RB, Boineau JP, Cox JL, Huddleston CB. Atrial flutter after lateral tunnel construction in the modified fontan operation: A canine model. JThorac Cardiovasc Surg. 1996;111:514-526.
16. Gandhi SK, Bromberg BI, Rodefeld MD, Schuessler RB, Boineau JP, Cox JL, Huddleston CB. Spontaneous atrial flutter in a chronic canine model of the modified fontan operation. J Am Coll Cardiol. 1997;30:1095-1103.
17. Rodefeld MD, Gandhi SK, Huddleston CB, Turken BJ, Schuessler RB, Boineau JP, Cox JL, Bromberg BI. Anatomically based ablation of atrial flutter in an acute canine model of the modified fontan operation. J Thorac Cardiovasc Surg. 1996;112:898-907.
18. Deisenhofer I, Zrenner B, Yin YH, Pitschner HF, Kuniss M, Grossmann G, Stiller S, Luik A, Veltmann C, Frank J, Linner J, Estner HL, Pflaumer A, Wu J, von Bary C, Ucer E, Reents T, Tzeis S, Fichtner S, Kathan S, Karch MR, Jilek C, Ammar S, Kolb C, Liu ZC, Haller B, Schmitt C, Hessling G. Cryoablation versus radiofrequency energy for the ablation of atrioventricular nodal reentrant tachycardia (the cyrano study): Results from a large multicenter prospective randomized trial. Circulation. 2010;122:2239-2245.
19. Triedman JK, Bergau DM, Saul JP, Epstein MR, Walsh EP. Efficacy of radiofrequency ablation for control of intraatrial reentrant tachycardia in patients with congenital heart disease. JAm Coll Cardiol. 1997;30:1032-1038.
20. Gonzalez-Torrecilla E, Arenal A, Atienza F, Osca J, Garcia-Fernandez J, Puchol A, Sanchez A, Almendral J. First postpacing interval after tachycardia entrainment with correction for atrioventricular node delay: A simple maneuver for differential diagnosis of atrioventricular nodal reentrant tachycardias versus orthodromic reciprocating tachycardias. Heart Rhythm.2006;3:674-679.
n: A canine modelelll.... JJJJ
JP CoCoCoCoxxxx JLJLJLJL HuHuHuHuddddddddlelelesa Jo
eld M Gandhi SK Huddleston C Turken BJ Schuessler R Boineau J CoBo
hofer Zrenner B, Yin YH, Pitschner HF, Kuniss M, Grossmann Stiller S, LuC Frank J Linner J Estner HL Pfla mer A W J on Bar C Ucer E Reents
aneeeeououououss attattririririalaa ffflululutter in a chronic canine mmmododel of the mooodififififieeed fontan operation. Jolololl. 1191 97;30:000 10101095999 -1111010103.333
lddd MMMD, Ganananandhhii SKKK, Huuuddddddlestttononono CCCB,,, TTTurkeken BJBBJB , ScSScS huuueeese sleer RB,B,B,B Boiiiinenenen auu JP,,, CCCoBI. AAAAnananatotototo iimicalllllly y babbb sed abababablalalation ooooffff atattat iirialll fffllluttttterererer iiin nn aaaan aaacucucuc tettt canineeee mmmom deddd lll ffof ttthhhe ontaaann nn opopoperereratatatioioioion.nn.n JJ J ThThThThororororacacac CCCCarrrrdididid ovovovvasasasascc SuSuSuurgrgrg.... 191919199696969 ;1;11112121212:8:8:88989898-9-9-9907070707.
hofer I, ZZZrerereennnnnnnnerererer BBBB,,,, YiYiYin nnn YHYYHYH, , , PiPiPiPitststsschchchchneneneer r r r HFHFHFHF, ,, , KuKuKuKuninininisssssss MMMM, , ,, GrGGrGrosososossmsmsmsmanananann n n n G,GG,G, SSSStittitiller S, LuCC FFr kk JJ LLiin JJ EE tst HLHL PfPflla AA WW JJ BBa CC UUc EE RRe tts
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
19
Table 1: Clinical Arrhythmia Severity Score
Documented Arrhythmia Frequency of Cardioversion
None 0 None 0
Non sustained only 1 One cardioversion 1
Sustained arrhythmia 2 AAIT* Conversion 2
Incessant 3 Two or more cardioversions 3
Arrhythmia Severity Antiarrhythmic Medications
Asymptomatic 0 None or Digoxin only 0
Palpitations only 1 Class II or Class IV 1
Syncope/CHF/Thrombosis 2 Class I or Class III 2
Cardiac Arrest 3 Amiodarone toxicity 3
Figure Legends:
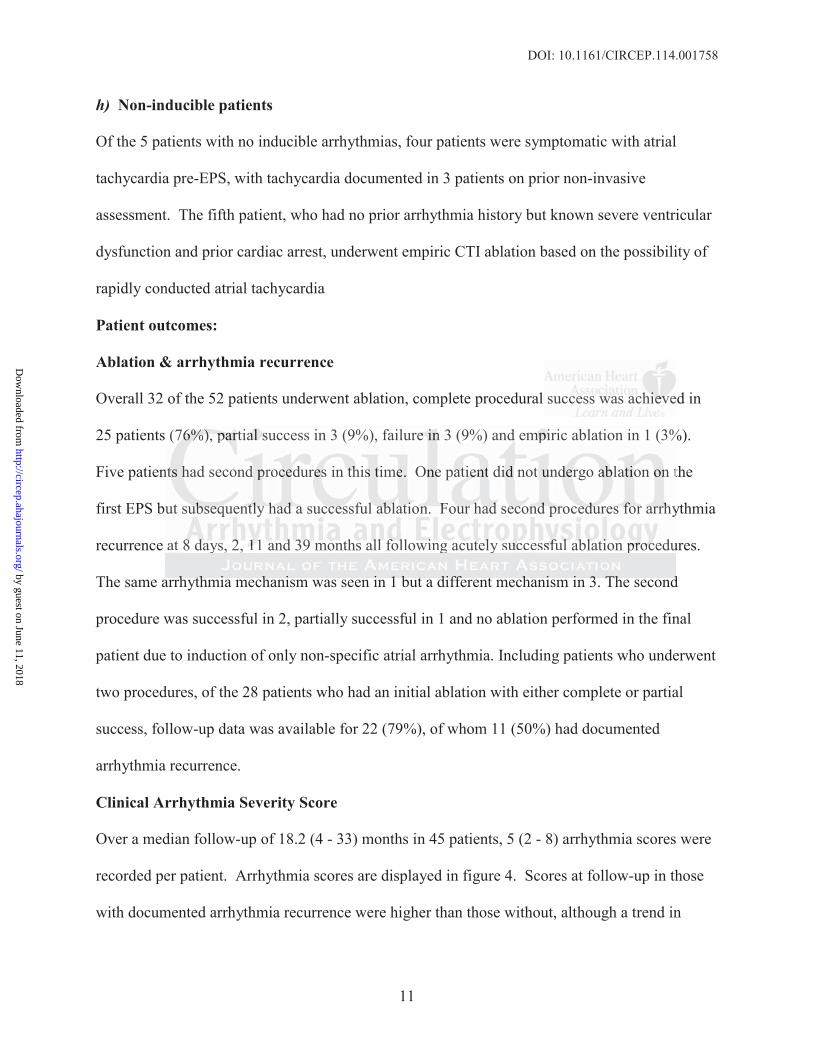
Figure 1: Activation map of the pulmonary venous atrium in a macroreentrant atrial tachycardia
traversing the cavomitral isthmus. The images depict an electroanatomic map of the pulmonary
venous atrium (anteriorly) and the lateral tunnel (posteriorly) viewed from the left anterior
oblique/caudal projection in a patient with L-looped transposition of the great arteries following
the total cavopulmonary connection. Activation is color-coded, where red denotes early and
purple late sites of local electrogram acquisition within a pre-determined time frame, and shows
counterclockwise activation of an isthmus dependent circuit around the mitral valve annulus.
0000
1
3
2
r
HHHHF/F/F/F/Thrombmbmbmbossisisisi 22 ClCC asss I orrr CCCClalll ssss IIIIIIIIIII 2
rreeesttt 333 AAAmioiodaaaarororoneee ttoxxxicccity 3
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
20
Activation within the lateral tunnel is not displayed.
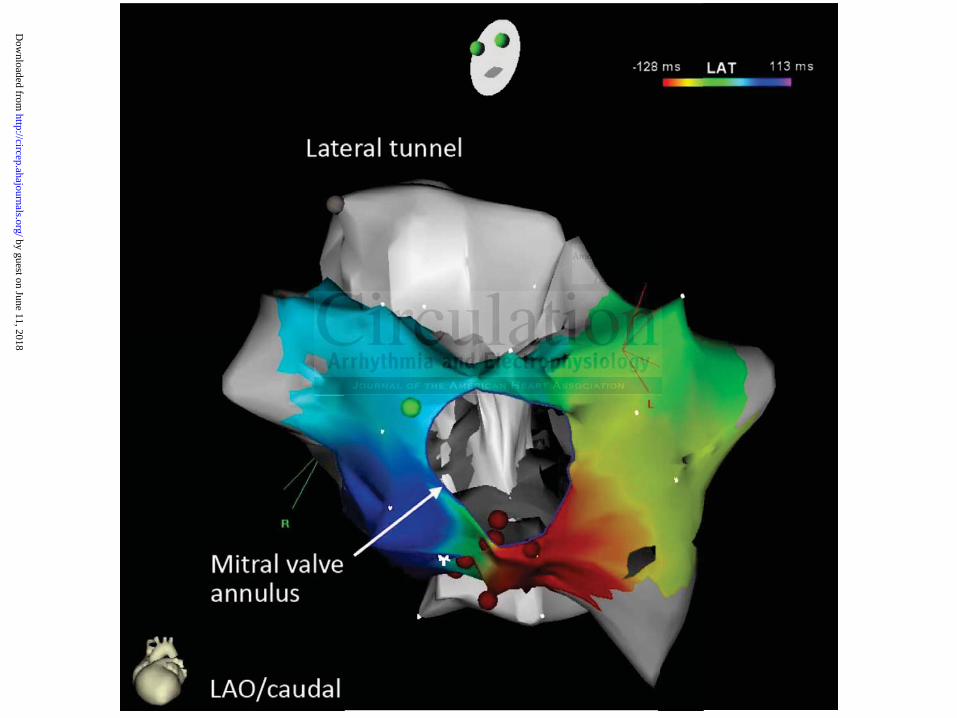
Figure 2: Activation map of a focal tachycardia. An electroanatomic map of the the lateral
tunnel demonstrates a typical centrifugal activation pattern of a focal atrial tachycardia
spreading anteriorly and inferiorly away from an area of scar (grey).
Figure 3: Contact electrograms recorded during tachycardia. Surface electrograms recorded
from leads I, aVF, V1 and V6 are displayed with contact bipolar intracardiac electrograms.
Panel (a) depicts a patient with two atypical AVNRT circuits, with catheters positioned within
the intracardiac baffle (REF), on the septum within the pulmonary venous atrium (MAP) and
retrograde via the aorta to the systemic ventricle (RV). On the left hand image the cycle length
is 400ms and VA interval 120ms, and on the right 363ms and 236ms, respectively. Successful
slow pathway ablation was performed using radiofrequency and cryoablation. Panel (b)
demonstrates a patient with atypical AVNRT (VA interval 230ms) with catheters positioned in
the systemic ventricle via a transbaffle puncture (RV) and within the intracardiac baffle (REF).
The return electrogram sequence on cessation of ventricular pacing with atrial entrainment shows
a pseudo AAV response, where the last paced ventricular complex relates to the second atrial
return electrogram (A*), which is then followed by another ventricular complex. Panel (c)
shows two different circuits in a patient with twin AV nodes where catheters have been
positioned within the intracardiac baffle (REF), at either HIS position (MAP), and retrograde via
the aorta to the systemic ventricle (RV). The left and right hand images show a circuit using the
upper and lower node, respectively, as the anterograde limb. Note the change in QRS polarity
seen in aVF indicative of a switch from a superior to inferior pattern of ventricular activation. (A
cardiac electrogrg amammmss.ss
theteersrs ppososititititiioioi nened ddd wiwiwiwitt
r n
via the aorta to the systemic ventricle RV On the left hand image the cycle len
nd VA interval 120ms, and on the right 363ms and 236ms, respectively. Succes
w
tes a patient ith at pical AVNRT (VA inter al 230ms) ith catheters positione
rdiacacacac bbbbafafafafflflflf eee (RRREEEEF), on the septum withinnnn ttthehhh pulmonaryyyy venenennoouo s atrium (MAP) an
vvvviaaaa the aorta to theee ssystemememic vvennntrriclee (RVV)). OnOnOnO tttthe lefefeft haandd iiiimmmage thheh cyycleee len
nd VVVVAAAA ininnintttervalll 1111202020ms, anndddd on thehehehe rrrigiigighththth 3336363633msmsms aaaandndndd 22223636363 msmsmsm , respecccctititiivvvev ly. SSSSucces
way yy babbllal tiiion wwwwaaasa ppperffformedddd usiiiinggg raddddiofrfff eqqquency yy and ddd crcrrryoyy abababblalalala ititiion. PPPanelelele ((((b)b)b)b
tt tatiie tnt itithh tat iic lal AAVNVNRTRT ((VAVA ii tnt ll 232300m )s) itithh thth tet isititi e
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.114.001758
21
denotes the atrial electrogram, V the ventricular, and H the HIS bundle).
Figure 4: Clinical Arrhythmia Severity Score at baseline and during follow-up. The p-value for
comparison between baseline and the post-procedure encounters is displayed under the time
interval.
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

A
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

B
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

Cecchin, Edward P. Walsh, John K. Triedman and Dominic J. AbramsRafael Correa, Elizabeth D. Sherwin, Joshua Kovach, Douglas Y. Mah, Mark E. Alexander, Frank
Mechanism and Ablation of Arrhythmia Following Total Cavopulmonary Connection
Print ISSN: 1941-3149. Online ISSN: 1941-3084 Copyright © 2015 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Arrhythmia and Electrophysiology
published online January 12, 2015;Circ Arrhythm Electrophysiol.
http://circep.ahajournals.org/content/early/2015/01/12/CIRCEP.114.001758World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org/content/suppl/2015/01/12/CIRCEP.114.001758.DC1Data Supplement (unedited) at:
http://circep.ahajournals.org//subscriptions/
is online at: Circulation: Arrhythmia and Electrophysiology Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answerinformation about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Arrhythmia and Electrophysiology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 11, 2018http://circep.ahajournals.org/
Dow
nloaded from

SUPPLEMENTAL MATERIAL
Video 1: Demonstration of most common uses of intracardiac echocardiography (ICE) during
diagnostic and ablative procedures in patients following total cavopulmonary connection.
Intracardiac echocardiography (ICE) provides detailed definition of the cardiac anatomy,
specifically the position of the atrioventricular valves, which may act as central obstacles to
conduction in reentrant circuits. Additionally ICE may help identify the precise location of
baffle fenestrations guiding catheter access to the pulmonary venous chamber, and
demonstrate good tissue contact at during radiofrequency ablation.