Mechanical Ventilation of the Neonate: Should We … · target variable, pressure or volume, is...
8
Mechanical Ventilation of the Neonate: Should We Target Volume or Pressure? Steven M Donn MD and Win Boon MD Introduction Gas Delivery Limitations of Volume Ventilation Volume-Targeted Modalities Hybrid Modalities Providing Volume-Targeted Ventilation Volume-Guarantee Ventilation Pressure-Regulated Volume Control Ventilation Volume-Assured Pressure Support Volume-Support Ventilation Pressure Augmentation The Evidence Volume-Controlled Ventilation Volume-Guarantee Ventilation Pressure-Regulated Volume Control Meta-analysis Why Does It Work? Summary For more than 40 years conventional mechanical ventilation has been used for the treatment of neonatal respiratory failure. Until relatively recently, this was accomplished with time-cycled pres- sure-limited ventilation, using intermittent mandatory ventilation. Earlier attempts at volume- targeted ventilation were largely ineffective because of technological limitations. The advent of microprocessor-based devices gives the clinician an option to choose either target variable to treat neonatal patients. This paper reviews the principles of each and the accumulated evidence. Key words: newborn, respiratory failure, mechanical ventilation, pressure-targeted, volume-targeted. [Respir Care 2009;54(9):1236 –1243. © 2009 Daedalus Enterprises] Introduction The traditional method of mechanical ventilation to treat neonatal respiratory failure has been time-cycled pressure- limited ventilation. Originally this was accomplished by modification of adult ventilators. Time-cycled pressure- limited ventilation was easy to use and was felt to safe- guard against barotrauma because the peak inspiratory pres- sure (PIP) could be limited and the ventilator would not exceed this pressure. Unfortunately, the delivered tidal vol- ume (V T ) would fluctuate according to pulmonary com- pliance; a smaller volume of gas would be delivered at low Steven M Donn MD and Win Boon MD are affiliated with the Division of Neonatal-Perinatal Medicine, Department of Pediatrics, CS Mott Chil- dren’s Hospital, University of Michigan Health System, Ann Arbor, Mich- igan. Dr Donn has disclosed relationships with Discovery Laboratories, Dey, Cardinal Health, and Hamilton Medical. Dr Boon has disclosed no con- flicts of interest. Dr Donn presented a version of this manuscript at the New Horizons Symposium, “Neonatal Respiratory Care,” at the International Respira- tory Congress of the American Association for Respiratory Care, at the 54th International Respiratory Congress of the American Association for Respiratory Care, held December 13-16, 2008, in Anaheim, California. 1236 RESPIRATORY CARE • SEPTEMBER 2009 VOL 54 NO 9
Transcript of Mechanical Ventilation of the Neonate: Should We … · target variable, pressure or volume, is...

Mechanical Ventilation of the Neonate:Should We Target Volume or Pressure?
Steven M Donn MD and Win Boon MD
IntroductionGas DeliveryLimitations of Volume VentilationVolume-Targeted ModalitiesHybrid Modalities Providing Volume-Targeted Ventilation
Volume-Guarantee VentilationPressure-Regulated Volume Control VentilationVolume-Assured Pressure SupportVolume-Support VentilationPressure Augmentation
The EvidenceVolume-Controlled VentilationVolume-Guarantee VentilationPressure-Regulated Volume Control
Meta-analysisWhy Does It Work?Summary
For more than 40 years conventional mechanical ventilation has been used for the treatment ofneonatal respiratory failure. Until relatively recently, this was accomplished with time-cycled pres-sure-limited ventilation, using intermittent mandatory ventilation. Earlier attempts at volume-targeted ventilation were largely ineffective because of technological limitations. The advent ofmicroprocessor-based devices gives the clinician an option to choose either target variable to treatneonatal patients. This paper reviews the principles of each and the accumulated evidence. Keywords: newborn, respiratory failure, mechanical ventilation, pressure-targeted, volume-targeted. [RespirCare 2009;54(9):1236–1243. © 2009 Daedalus Enterprises]
Introduction
The traditional method of mechanical ventilation to treatneonatal respiratory failure has been time-cycled pressure-limited ventilation. Originally this was accomplished bymodification of adult ventilators. Time-cycled pressure-limited ventilation was easy to use and was felt to safe-guard against barotrauma because the peak inspiratory pres-sure (PIP) could be limited and the ventilator would notexceed this pressure. Unfortunately, the delivered tidal vol-ume (VT) would fluctuate according to pulmonary com-pliance; a smaller volume of gas would be delivered at low
Steven M Donn MD and Win Boon MD are affiliated with the Divisionof Neonatal-Perinatal Medicine, Department of Pediatrics, CS Mott Chil-dren’s Hospital, University of Michigan Health System, Ann Arbor, Mich-igan.
Dr Donn has disclosed relationships with Discovery Laboratories, Dey,Cardinal Health, and Hamilton Medical. Dr Boon has disclosed no con-flicts of interest.
Dr Donn presented a version of this manuscript at the New HorizonsSymposium, “Neonatal Respiratory Care,” at the International Respira-tory Congress of the American Association for Respiratory Care, at the54th International Respiratory Congress of the American Association forRespiratory Care, held December 13-16, 2008, in Anaheim, California.
1236 RESPIRATORY CARE • SEPTEMBER 2009 VOL 54 NO 9

compliance, whereas a higher volume would be deliveredas compliance improved, unless the clinician vigilantlyadjusted the PIP.
In the mid-1970s an infant ventilator was specificallydesigned to deliver volume-controlled breaths to newborninfants. The clinician would target a volume of gas to bedelivered to the baby, and the pressure was permitted tofluctuate to deliver the desired VT. Although the principleseemed sound, there were severe technological limitations,including the inability to measure VT, compliant ventilatorcircuits that increased compressible volume loss, slow re-sponse times, incompatibility with continuous flow, and,most importantly, insufficient knowledge about neonatallung mechanics. In the early 1980s the manufacturerstopped producing the ventilator, and for the next decadealmost all neonatal ventilation was pressure-limited.
The incorporation of microprocessor-based technologyinto neonatal ventilators and the development of small,lightweight, and low-dead-space transducers and accuratereal-time monitoring enabled the reintroduction of vol-ume-targeted ventilation into neonatal intensive care.1 Thispaper will examine the current controversy as to whichtarget variable, pressure or volume, is better for the treat-ment of neonatal respiratory failure.
Gas Delivery
The major difference between pressure and volumebreaths is the way in which inspiratory gas flow is deliv-ered to the patient. In both time-cycled pressure-limitedventilation and pressure-control ventilation there is a rapid
acceleration of gas flow at the onset of inspiration, result-ing in rapid pressurization of the circuit and the achieve-ment of peak pressure and volume delivery early in inspi-ration. Flow then decelerates. This creates a peaked flowwaveform and rapidly rising and falling pressure wave-form (Fig. 1). Thus, breaths may be considered as being“front-end loaded.” Theoretically this might be advanta-geous when the primary pathophysiology is diffuse andcharacterized by the need for a high opening pressure. Incontrast, flow delivery during volume-controlled ventila-tion (VCV) accelerates at the start of inspiration but is heldconstant throughout inspiration, creating a square wave-form (Fig. 2). This results in a ramping effect, where peakpressure and peak volume delivery occur late in inspira-tion. These breaths are “back-end loaded,” resulting inslower inflation of the lung. VCV might be advantageouswhen lung disease is more heterogeneous and in situationswhere compliance changes quickly, such as following theadministration of surfactant.2
Limitations of Volume Ventilation
The major drawback to the use of volume ventilation innewborns is related to the use of uncuffed endotrachealtubes. This results in a variable degree of leak around theendotracheal tube, which affects the volume of gas thebaby actually receives. Ventilators are set to deliver atargeted VT, but this is based on how much gas leaves themachine. A certain amount of this gas will be compressedwithin the ventilator, and this is referred to as compress-ible volume loss. This is affected by the compliance ofboth the lungs and the circuit, in addition to other factors,such as humidification. Because of compressible volumeloss, it is imperative to measure the delivered VT as closeto the airway as possible.3
Correspondence: Steven M Donn MD, Division of Neonatal-PerinatalMedicine, Department of Pediatrics, F5790, Mott Children’s’ Hospital,University of Michigan Health System, 1500 E Medical Center Drive,Ann Arbor MI 48109-0254. E-mail: [email protected].
Fig. 1. Graphic representation of flow waveform (middle panel) inpressure-control ventilation. Note the rapid acceleration and de-celeration of inspiratory flow, producing a peaked waveform.
Fig. 2. Graphic representation of flow waveform (middle panel) involume-targeted ventilation. Note the constant inspiratory flow,producing a square waveform.
MECHANICAL VENTILATION OF THE NEONATE: SHOULD WE TARGET VOLUME OR PRESSURE?
RESPIRATORY CARE • SEPTEMBER 2009 VOL 54 NO 9 1237

Volume-Targeted Modalities
Volume-targeted ventilation has been achieved in sev-eral ways. True volume-targeting involves all of the fea-tures described earlier, including constant flow delivery(square waveform) and auto-adjustment of pressure as com-pliance changes (Fig. 3). There are several hybrid forms ofvolume-targeting, where pressure adjustments are made toassure the delivery of a minimal VT. One might also arguethat volume-targeting of time-cycled pressure-limited ven-tilation is possible if the clinician is vigilant and constantlyattends to the ventilator so that delivered VT stays withina tight range. However, delivered breaths will still havethe characteristics of pressure-targeted breaths, and it seemsdoubtful that even the most astute clinician could makeadjustments as fast as a microprocessor.
Hybrid Modalities ProvidingVolume-Targeted Ventilation
Both VCV and time-cycled pressure-limited ventilationhave certain advantages and disadvantages. Hybrid mo-dalities try to combine the most desirable features of each.These include volume guarantee, pressure-regulated vol-ume control, and volume-assured pressure support. Theyare essentially pressure-targeted forms of ventilation, bututilize microprocessor servo-controlled ventilation with analgorithm that adjusts the rise and fall of pressure for VT
delivery within a desired range. Volume guarantee andpressure-regulated volume control use the VT of previousbreaths as a reference, with follow-up adjustments in PIPon averages of 4–6 breaths. Volume-assured pressure sup-port makes intra-breath adjustments of inspiratory timeand/or pressure, until the desired volume has been deliv-ered. All of these try to optimize VT delivery, althougheach does so differently.
Volume-Guarantee Ventilation
Volume-guarantee ventilation, available on the Babylog8000-plus ventilator (Drager Medical, Telford, Pennsylva-nia), is a popular form of volume targeting. It is bestdescribed as a dual-loop synchronized modality that ven-tilates with time-cycled pressure-limited ventilation butallows pressure to be adjusted to deliver a VT in a clini-cian-chosen range. The clinician selects a target VT andlimits the pressure (referred to as the working pressure).The device measures the exhaled VT of the previous breathas a reference and adjusts the working pressure to reachthe target volume over the next few breaths. The feedbackloop has some limitations. For example, because adjust-ments to PIP are based on the exhaled VT and are made insmall increments to avoid overcompensation, the deliveredVT may not compensate for substantial breath-to-breathfluctuations in the presence of large leaks. When the leak
exceeds 40%, volume guarantee is less reliable because ofthe inability to accurately measure the real VT. Catch-upadjustments in pressure occur every few breaths, so if theventilatory rate is set too low, its effectiveness may bequestionable.
Potential advantages of volume guarantee include de-creased volutrauma because the clinician sets a VT that isnot exceeded, and as lung compliance improves, pressureis automatically decreased.4 Volume guarantee can be usedonly with patient-triggered modes: assist-control, synchro-nized intermittent mandatory ventilation (SIMV), or pres-sure-support ventilation (PSV). The addition of volumeguarantee to one of these modes enables the clinician to seta mean VT to be delivered, as well as the standard venti-lator settings of PIP, positive end-expiratory pressure, in-spiratory time, and respiratory rate. No more than 130% ofthe target VT is supposed to be delivered. The usual initialtarget is 4–5 mL/kg. The pressure limit is set approxi-mately 15% to 20% above the peak pressure needed toconsistently deliver the desired VT. Because the adjust-ment of PIP is in reference to exhaled VT and changes aremade in small increments to prevent overcompensation,the PIP cannot be adjusted instantaneously to compensatefor large breath-to-breath fluctuations. Consequently, al-though the delivered VT is more consistent with volumeguarantee than without it, there is fluctuation around thetarget value. Most infants can be extubated when theymaintain VT at or above the target value at a PIP � 10–12 cm H2O with reliable respiratory effort.
Pressure-Regulated Volume Control Ventilation
Pressure-regulated volume control is another modalitythat attempts to combine the benefits of time-cycled pres-sure-limited ventilation and VCV. It is available on theServo 300A and the Servo-i ventilators (Maquet, Bridge-water, New Jersey). It is flow-cycled and offers the “vari-able” flow rate of pressure-control ventilation and volume
Fig. 3. Schematic comparison of pressure-volume loops in pres-sure-targeted (left) and volume-targeted (right) ventilation. Duringpressure-targeting a decrease in pulmonary compliance (movingfrom light loop to dark loop) results in a loss of tidal volume,despite consistency of inspiratory pressure. During volume-target-ing, a decrease in compliance (moving from the dark loop to thelight loop) results in an automatic increase in pressure to assureconstant volume delivery.
MECHANICAL VENTILATION OF THE NEONATE: SHOULD WE TARGET VOLUME OR PRESSURE?
1238 RESPIRATORY CARE • SEPTEMBER 2009 VOL 54 NO 9

targeting. Like volume guarantee, pressure-regulated vol-ume control is a form of closed-loop ventilation; pressureis adjusted according to the delivered VT. The new Servo-iventilator measures pressure at the proximal airway, as-suring better accuracy.5
The clinician selects a target VT and the maximum al-lowable pressure. The microprocessor attempts to use thelowest pressure (with a decelerating-flow waveform) todeliver the set VT. The first breath is delivered 10 cm H2Oabove the baseline setting (positive end-expiratory pres-sure) and is utilized as a test breath to calculate the pres-sure needed to deliver the desired VT in accordance withthe patient’s compliance. The next 3 breaths are deliveredat a pressure that is 75% of the calculated necessary pres-sure. If the targeted VT fails to be delivered, the inspiratorypressure is increased by 3 cm H2O for each breath until thetargeted volume is reached. If the targeted VT is exceeded,the converse occurs, and pressure is decreased by 3 cm H2O.Inspiratory pressure is regulated between the positive end-expiratory pressure and 5 cm H2O below the clinician-limited PIP. Variations in delivered volume also occurbecause pressure adjustments are based on a 4-breath mov-ing average.
Volume-Assured Pressure Support
Volume-assured pressure support is available on theVIP Bird Gold infant/pediatric ventilator (CareFusion, SanDiego, California). This modality combines the advan-tages of pressure-targeted and volume-targeted ventilationwithin a single breath. It can be used with both assist-control and SIMV, or by itself in babies with reliablerespiratory drive. It may be described as “variable-flowvolume ventilation.” This is a true hybrid modality, withdecelerating, variable inspiratory flow, and guaranteed vol-ume delivery. The breath is patient-triggered and begins asa PSV breath. The device measures delivered volume wheninspiratory flow has decelerated to the set minimum. If thedelivered volume exceeds the desired level, the breath isterminated by flow-cycling. However, if the preset volumehas not been delivered, the breath transitions to a volume-targeted breath; the set flow will persist and the inspiratorytime will be prolonged until the desired volume has beenreached. In this situation the sinusoidal flow waveformtransitions to a square waveform. If the delivered volumeis considerably below the desired level, the pressure mayalso increase slightly.6
Volume-Support Ventilation
Volume-support ventilation is another hybrid modality,available on the Servo-i device (Maquet, Bridgewater, NewJersey), which is similar to PSV and pressure-regulatedvolume control.5 The volume-supported breath is patient-triggered, pressure-limited, and flow-cycled. It is used in
spontaneously breathing patients with adequate respiratorydrive. Breath rate, VT, and minute volume are chosen bythe clinician; inspiratory time is determined by the patient.The algorithm adjusts the pressure limit by no more than3 cm H2O at a time. Adjustments are made in consecutivebreaths until the targeted VT is reached. The flow, pres-sure, and volume waveforms for a volume-supported breathare similar to those of pressure-supported breaths; how-ever, the efficacy of volume support can be determinedonly by evaluating sequential graphic presentations. TheVT waveform will increase in a stepwise fashion until thetarget volume is reached.
Pressure Augmentation
Pressure augmentation, available on the Bear 1000 ven-tilator (CareFusion, San Diego, California), is another hy-brid modality that matches the patient’s flow demand whileguaranteeing a minimum VT.2 Pressure augmentation isunique in the following ways: the pre-set VT is only aminimum, and the patient can go above this; minimum VT
is guaranteed by adjustment in flow rather than pressure,which is fixed; and adjustment to flow is made within asingle breath, like volume-assured pressure support. Pres-sure augmentation matches the patient’s flow demand andlung dynamics and can be delivered in either assist-controlor SIMV modes.
The Evidence
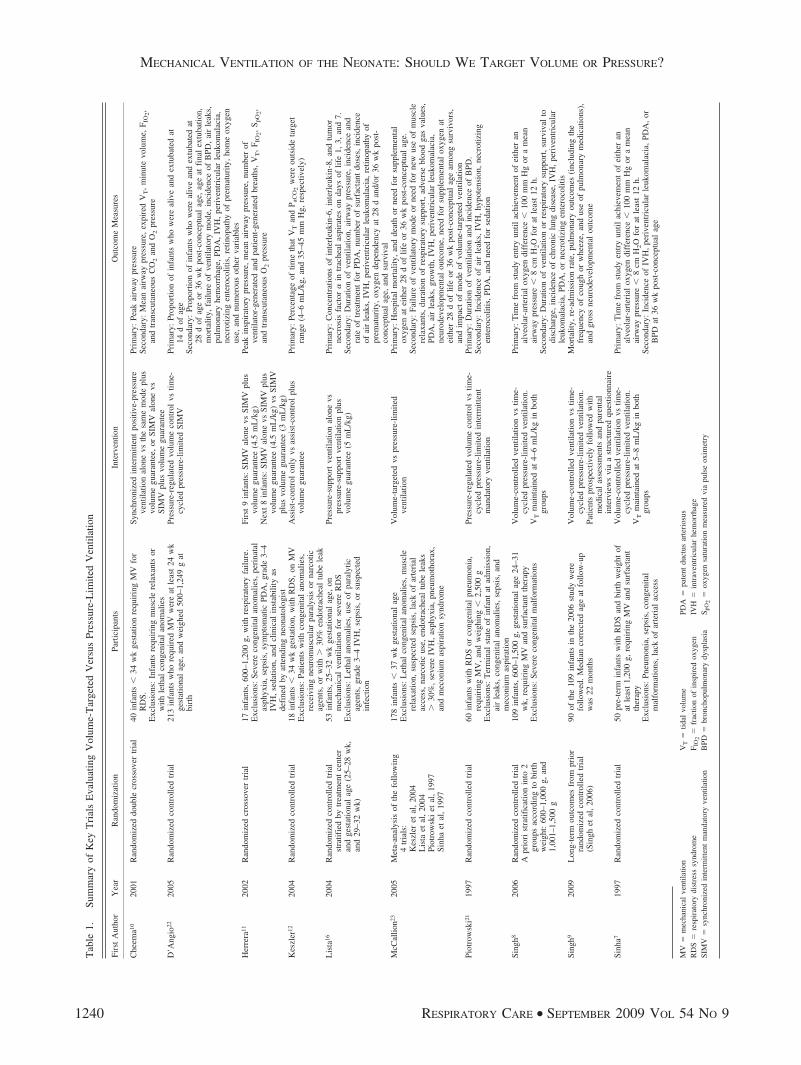
Table 1 summarizes studies on volume-targeted and pres-sure-limited ventilation.
Volume-Controlled Ventilation
One of the first trials evaluating VCV was conducted bySinha and colleagues.7 Fifty pre-term infants with respi-ratory distress syndrome (RDS) and birth weights of atleast 1,200 g requiring mechanical ventilation and surfac-tant therapy were randomized to receive either VCV ortime-cycled pressure-limited ventilation. VT was tightlymaintained between 5–8 mL/kg for both treatment groups.Primary outcome measures included the time from studyentry until achievement of either an alveolar-arterial oxy-gen difference less than 100 mm Hg, or a mean airwaypressure less than 8 cm H2O for at least 12 hours. Infantsreceiving VCV reached success criteria faster than thetime-cycled pressure-limited ventilation group, with a meantime of 65.5 hours versus 125.6 hours (P � .001). Thetotal duration of ventilation for the VCV group was loweras well (122.4 h vs 161.9 h, P � .001). Secondary out-comes included the incidence of intraventricular hemor-rhage, periventricular leukomalacia, patent ductus arterio-sus, and bronchopulmonary dysplasia (BPD, defined asoxygen requirement beyond 36 weeks post-menstrual age,
MECHANICAL VENTILATION OF THE NEONATE: SHOULD WE TARGET VOLUME OR PRESSURE?
RESPIRATORY CARE • SEPTEMBER 2009 VOL 54 NO 9 1239
Tab
le1.
Sum
mar
yof
Key
Tri
als
Eva
luat
ing
Vol
ume-
Tar
gete
dV
ersu
sPr
essu
re-L
imite
dV
entil
atio
n
Firs
tA
utho
rY
ear
Ran
dom
izat
ion
Part
icip
ants
Inte
rven
tion
Out
com
eM
easu
res
Che
ema1
020
01R
ando
miz
eddo
uble
cros
sove
rtr
ial
40in
fant
s�
34w
kge
stat
ion
requ
irin
gM
Vfo
rR
DS.
Exc
lusi
ons:
Infa
nts
requ
irin
gm
uscl
ere
laxa
nts
orw
ithle
thal
cong
enita
lan
omal
ies
Sync
hron
ized
inte
rmitt
ent
posi
tive-
pres
sure
vent
ilatio
nal
one
vsth
esa
me
mod
epl
usvo
lum
egu
aran
tee,
orSI
MV
alon
evs
SIM
Vpl
usvo
lum
egu
aran
tee
Prim
ary:
Peak
airw
aypr
essu
reSe
cond
ary:
Mea
nai
rway
pres
sure
,ex
pire
dV
T,
min
ute
volu
me,
F IO
2,an
dtr
ansc
utan
eous
CO
2an
dO
2pr
essu
re
D’A
ngio
2220
05R
ando
miz
edco
ntro
lled
tria
l21
3in
fant
sw
hore
quir
edM
Vw
ere
atle
ast
24w
kge
stat
iona
lag
e,an
dw
eigh
ed50
0–1,
249
gat
birt
h
Pres
sure
-reg
ulat
edvo
lum
eco
ntro
lvs
time-
cycl
edpr
essu
re-l
imite
dSI
MV
Prim
ary:
Prop
ortio
nof
infa
nts
who
wer
eal
ive
and
extu
bate
dat
14d
ofag
eSe
cond
ary:
Prop
ortio
nof
infa
nts
who
wer
eal
ive
and
extu
bate
dat
28d
ofag
eor
36w
kpo
st-c
once
ptua
lag
e,ag
eat
fina
lex
tuba
tion,
mor
talit
y,fa
ilure
ofve
ntila
tory
mod
e,in
cide
nce
ofB
PD,
air
leak
s,pu
lmon
ary
hem
orrh
age,
PDA
,IV
H,
peri
vent
ricu
lar
leuk
omal
acia
,ne
crot
izin
gen
tero
colit
is,
retin
opat
hyof
prem
atur
ity,
hom
eox
ygen
use,
and
num
erou
sot
her
vari
able
sH
erre
ra11
2002
Ran
dom
ized
cros
sove
rtr
ial
17in
fant
s,60
0–1,
200
g,w
ithre
spir
ator
yfa
ilure
.E
xclu
sion
s:Se
vere
cong
enita
lan
omal
ies,
peri
nata
las
phyx
ia,
seps
is,
sym
ptom
atic
PDA
,gr
ade
3–4
IVH
,se
datio
n,an
dcl
inic
alin
stab
ility
asde
fine
dby
atte
ndin
gne
onat
olog
ist
Firs
t9
infa
nts:
SIM
Val
one
vsSI
MV
plus
volu
me
guar
ante
e(4
.5m
L/k
g)N
ext
8in
fant
s:SI
MV
alon
evs
SIM
Vpl
usvo
lum
egu
aran
tee
(4.5
mL
/kg)
vsSI
MV
plus
volu
me
guar
ante
e(3
mL
/kg)
Peak
insp
irat
ory
pres
sure
,m
ean
airw
aypr
essu
re,
num
ber
ofve
ntila
tor-
gene
rate
dan
dpa
tient
-gen
erat
edbr
eath
s,V
T,
F IO
2,S p
O2,
and
tran
scut
aneo
usO
2pr
essu
re
Kes
zler
1220
04R
ando
miz
edco
ntro
lled
tria
l18
infa
nts
�34
wk
gest
atio
n,w
ithR
DS,
onM
VE
xclu
sion
s:Pa
tient
sw
ithco
ngen
ital
anom
alie
s,re
ceiv
ing
neur
omus
cula
rpa
raly
sis
orna
rcot
icag
ents
,or
with
�30
%en
dotr
ache
altu
bele
ak
Ass
ist-
cont
rol
only
vsas
sist
-con
trol
plus
volu
me
guar
ante
ePr
imar
y:Pe
rcen
tage
oftim
eth
atV
Tan
dP a
CO
2w
ere
outs
ide
targ
etra
nge
(4–6
mL
/kg,
and
35–4
5m
mH
g,re
spec
tivel
y)
Lis
ta16
2004
Ran
dom
ized
cont
rolle
dtr
ial
stra
tifie
dby
trea
tmen
tce
nter
and
gest
atio
nal
age
(25–
28w
k,an
d29
–32
wk)
53in
fant
s,25
–32
wk
gest
atio
nal
age,
onm
echa
nica
lve
ntila
tion
for
seve
reR
DS
Exc
lusi
ons:
Let
hal
anom
alie
s,us
eof
para
lytic
agen
ts,
grad
e3–
4IV
H,
seps
is,
orsu
spec
ted
infe
ctio
n
Pres
sure
-sup
port
vent
ilatio
nal
one
vspr
essu
re-s
uppo
rtve
ntila
tion
plus
volu
me
guar
ante
e(5
mL
/kg)
Prim
ary:
Con
cent
ratio
nsof
inte
rleu
kin-
6,in
terl
euki
n-8,
and
tum
orne
cros
isfa
ctor
�in
trac
heal
aspi
rate
son
days
oflif
e1,
3,an
d7.
Seco
ndar
y:D
urat
ion
ofve
ntila
tion,
airw
aypr
essu
re,
inci
denc
ean
dra
teof
trea
tmen
tfo
rPD
A,
num
ber
ofsu
rfac
tant
dose
s,in
cide
nce
ofai
rle
aks,
IVH
,pe
rive
ntri
cula
rle
ukom
alac
ia,
retin
opat
hyof
prem
atur
ity,
oxyg
ende
pend
ency
at28
dan
d/or
36w
kpo
st-
conc
eptu
alag
e,an
dsu
rviv
alM
cCal
lion2
320
05M
eta-
anal
ysis
ofth
efo
llow
ing
4tr
ials
:K
eszl
eret
al,
2004
Lis
taet
al,
2004
Piot
row
ski
etal
,19
97Si
nha
etal
,19
97
178
infa
nts
�37
wk
gest
atio
nal
age
Exc
lusi
ons:
Let
hal
cong
enita
lan
omal
ies,
mus
cle
rela
xatio
n,su
spec
ted
seps
is,
lack
ofar
teri
alac
cess
,na
rcot
icus
e,en
dotr
ache
altu
bele
aks
�30
%,
seve
reIV
H,
asph
yxia
,pn
eum
otho
rax,
and
mec
oniu
mas
pira
tion
synd
rom
e
Vol
ume-
targ
eted
vspr
essu
re-l
imite
dve
ntila
tion
Prim
ary:
Hos
pita
lm
orta
lity,
and
deat
hor
need
for
supp
lem
enta
lox
ygen
atei
ther
28d
oflif
eor
36w
kpo
st-c
once
ptua
lag
e.Se
cond
ary:
Failu
reof
vent
ilato
rym
ode
orne
edfo
rne
wus
eof
mus
cle
rela
xant
s,du
ratio
nof
resp
irat
ory
supp
ort,
adve
rse
bloo
dga
sva
lues
,PD
A,
air
leak
s,gr
owth
,IV
H,
peri
vent
ricu
lar
leuk
omal
acia
,ne
urod
evel
opm
enta
lou
tcom
e,ne
edfo
rsu
pple
men
tal
oxyg
enat
eith
er28
dof
life
or36
wk
post
-con
cept
ual
age
amon
gsu
rviv
ors,
and
impa
ctof
mod
eof
volu
me-
targ
eted
vent
ilatio
nPi
otro
wsk
i21
1997
Ran
dom
ized
cont
rolle
dtr
ial
60in
fant
sw
ithR
DS
orco
ngen
ital
pneu
mon
ia,
requ
irin
gM
V,
and
wei
ghin
g�
2,50
0g
Exc
lusi
ons:
Ter
min
alst
ate
ofin
fant
atad
mis
sion
,ai
rle
aks,
cong
enita
lan
omal
ies,
seps
is,
and
mec
oniu
mas
pira
tion
Pres
sure
-reg
ulat
edvo
lum
eco
ntro
lvs
time-
cycl
edpr
essu
re-l
imite
din
term
itten
tm
anda
tory
vent
ilatio
n
Prim
ary:
Dur
atio
nof
vent
ilatio
nan
din
cide
nce
ofB
PD.
Seco
ndar
y:In
cide
nce
ofai
rle
aks,
IVH
,hy
pote
nsio
n,ne
crot
izin
gen
tero
colit
is,
PDA
,an
dne
edfo
rse
datio
n
Sing
h820
06R
ando
miz
edco
ntro
lled
tria
lA
prio
rist
ratif
icat
ion
into
2gr
oups
acco
rdin
gto
birt
hw
eigh
t:60
0–1,
000
g,an
d1,
001–
1,50
0g
109
infa
nts,
600–
1,50
0g,
gest
atio
nal
age
24–3
1w
k,re
quir
ing
MV
and
surf
acta
ntth
erap
yE
xclu
sion
s:Se
vere
cong
enita
lm
alfo
rmat
ions
Vol
ume-
cont
rolle
dve
ntila
tion
vstim
e-cy
cled
pres
sure
-lim
ited
vent
ilatio
n.V
Tm
aint
aine
dat
4–6
mL
/kg
inbo
thgr
oups
Prim
ary:
Tim
efr
omst
udy
entr
yun
tilac
hiev
emen
tof
eith
eran
alve
olar
-art
eria
lox
ygen
diff
eren
ce�
100
mm
Hg
ora
mea
nai
rway
pres
sure
�8
cmH
2Ofo
rat
leas
t12
h.Se
cond
ary:
Dur
atio
nof
vent
ilatio
nor
resp
irat
ory
supp
ort,
surv
ival
todi
scha
rge,
inci
denc
eof
chro
nic
lung
dise
ase,
IVH
,pe
rive
ntri
cula
rle
ukom
alac
ia,
PDA
,or
necr
otiz
ing
ente
roco
litis
Sing
h920
09L
ong-
term
outc
omes
from
prio
rra
ndom
ized
cont
rolle
dtr
ial
(Sin
ghet
al,
2006
)
90of
the
109
infa
nts
inth
e20
06st
udy
wer
efo
llow
ed.
Med
ian
corr
ecte
dag
eat
follo
w-u
pw
as22
mon
ths
Vol
ume-
cont
rolle
dve
ntila
tion
vstim
e-cy
cled
pres
sure
-lim
ited
vent
ilatio
n.Pa
tient
spr
ospe
ctiv
ely
follo
wed
with
med
ical
asse
ssm
ents
and
pare
ntal
inte
rvie
ws
via
ast
ruct
ured
ques
tionn
aire
Mor
talit
y,re
-adm
issi
onra
te,
pulm
onar
you
tcom
es(i
nclu
ding
the
freq
uenc
yof
coug
hor
whe
eze,
and
use
ofpu
lmon
ary
med
icat
ions
),an
dgr
oss
neur
odev
elop
men
tal
outc
ome
Sinh
a719
97R
ando
miz
edco
ntro
lled
tria
l50
pre-
term
infa
nts
with
RD
San
dbi
rth
wei
ght
ofat
leas
t1,
200
g,re
quir
ing
MV
and
surf
acta
ntth
erap
yE
xclu
sion
s:Pn
eum
onia
,se
psis
,co
ngen
ital
mal
form
atio
ns,
lack
ofar
teri
alac
cess
Vol
ume-
cont
rolle
dve
ntila
tion
vstim
e-cy
cled
pres
sure
-lim
ited
vent
ilatio
n.V
Tm
aint
aine
dat
5–8
mL
/kg
inbo
thgr
oups
Prim
ary:
Tim
efr
omst
udy
entr
yun
tilac
hiev
emen
tof
eith
eran
alve
olar
-art
eria
lox
ygen
diff
eren
ce�
100
mm
Hg
ora
mea
nai
rway
pres
sure
�8
cmH
2Ofo
rat
leas
t12
h.Se
cond
ary:
Inci
denc
eof
IVH
,pe
rive
ntri
cula
rle
ukom
alac
ia,
PDA
,or
BPD
at36
wk
post
-con
cept
ual
age
MV
�m
echa
nica
lve
ntila
tion
RD
S�
resp
irat
ory
dist
ress
synd
rom
eSI
MV
�sy
nchr
oniz
edin
term
itten
tm
anda
tory
vent
ilatio
n
VT
�tid
alvo
lum
eF I
O2
�fr
actio
nof
insp
ired
oxyg
enB
PD�
bron
chop
ulm
onar
ydy
spla
sia
PDA
�pa
tent
duct
usar
teri
osus
IVH
�in
trav
entr
icul
arhe
mor
rhag
eS p
O2
�ox
ygen
satu
ratio
nm
easu
red
via
puls
eox
imet
ry
MECHANICAL VENTILATION OF THE NEONATE: SHOULD WE TARGET VOLUME OR PRESSURE?
1240 RESPIRATORY CARE • SEPTEMBER 2009 VOL 54 NO 9

with correlating radiographic findings). The frequency ofmajor scan abnormality (large intraventricular hemorrhage,ventriculomegaly, and intraparenchymal echodensities)was lower in the VCV group than in the time-cycled pres-sure-limited ventilation group (P � .5). While there wasless BPD in the VCV group (4% vs 25%), this did notreach statistical significance. There were no significantdifferences in the incidence of air leaks or patent ductusarteriosus requiring therapy. The authors concluded thatVCV appeared to be both safe and effective in this groupof patients. At the time of this study, technological limi-tations of the ventilator precluded enrolling smaller infants.
A subsequent study by the same group further bolsteredthe efficacy of VCV.8 Refinements in ventilator designeventually led to the ability to deliver even smaller VT,therefore providing VCV as an option to smaller babiesthan before. The second trial enrolled 109 infants, weigh-ing 600–1,500 g, with gestational ages of 24–31 weeks.These babies also had RDS requiring mechanical ventila-tion and surfactant therapy, and were randomized to re-ceive either VCV or time-cycled pressure-limited ventila-tion. A priori stratification into 2 groups according to birthweight was performed (600–1,000 g, and 1,001–1,500 g).Target VT was 4–6 mL/kg for both groups. Primary out-comes evaluating the alveolar-arterial oxygen differenceor mean airway pressure were identical to their prior study.There were no statistically significant differences in pri-mary outcomes between the 2 groups in aggregate, al-though there was a trend toward faster weaning from theventilator in the VCV group. However, in the cohort ofinfants weighing 600–1,000 g, those assigned to VCVreached their primary end point faster than those assignedto time-cycled pressure-limited ventilation, with a meantime of 21 hours versus 58 hours (P � .03). No statisti-cally significant differences were found among the sec-ondary outcomes, which included duration of ventilationand respiratory support, survival to neonatal intensive careunit discharge, and frequency of other complications, suchas intraventricular hemorrhage, periventricular leukomala-cia, patent ductus arteriosus, and necrotizing enterocolitisBell stage II or greater. The authors concluded that VCVis safe and efficacious in very-low-birth-weight infantsand may have advantages over time-cycled pressure-lim-ited ventilation, especially in smaller infants.
Singh and colleagues later reported the long-term out-comes of this study population.9 Ninety of the 109 infantsenrolled in the initial study were prospectively followedusing medical assessments and parental interviews via astructured questionnaire, to obtain masked evaluation ofhealth status and gross neurodevelopment. The mediancorrected age at follow-up was 22 months. Fewer childrenin the VCV group required inhaled medications at the timeof follow-up (odds ratio of 0.3, with a 95% confidenceinterval [CI] of 0.09–0.98, P � .04). Mortality, readmis-
sion rate, and frequency or severity of respiratory dysfunc-tion were not affected by the type of ventilation received.The authors noted that the trend toward less chronic lungdisease at 36 weeks post-conceptual age has a clinicalcorrelate at 22 months, with fewer children requiring in-haled medications for chronic lung disease.
Volume-Guarantee Ventilation
Cheema and Ahluwalia were among the first to evaluatethe efficacy of volume-guarantee ventilation in the neona-tal population.10 In their crossover trial, 40 infants� 34 weeks gestation requiring mechanical ventilation forRDS received synchronized intermittent positive-pressureventilation alone, versus synchronized intermittent posi-tive-pressure ventilation plus volume guarantee, or SIMValone versus SIMV plus volume guarantee. Patients whoreceived synchronized intermittent positive-pressure ven-tilation were in the acute phase of RDS, while those whoreceived SIMV were in the recovery (weaning) phase.There were slight decreases in PIP and mean airway pres-sure in both volume-guarantee groups, which reached sta-tistical significance. There were no significant differencesin overall gas exchange or adverse outcomes between thosewith and without volume guarantee. While this was a smallshort-term study, it did suggest that volume-targeted mo-dalities are feasible for the neonatal population.
In another crossover trial, Herrera and colleagues notedthat SIMV plus volume guarantee, compared to SIMValone, had a statistically significant reduction in peak andmean airway pressure.11
Keszler and Abubakar performed the first randomizedcontrolled trial of volume guarantee.12 Eighteen infants� 34 weeks gestation, who had RDS, were randomized toreceive assist-control alone, or assist-control plus volumeguarantee. Patients who received assist-control plus vol-ume guarantee had fewer breaths outside the targeted VT
range, compared to assist-control alone (37% vs 61%,P � .001). The volume-guarantee group also had signifi-cantly fewer episodes of inadvertent hypocapnia, furthersupporting the potential for volume guarantee.
A more recent trial by Cheema and colleagues evaluatedinitial arterial blood gases in infants with RDS shortlyafter they were placed on synchronized intermittent posi-tive-pressure ventilation versus synchronized intermittentpositive-pressure ventilation plus volume guarantee.13
Stratified analysis revealed that infants � 25 weeks gesta-tion had significantly less hypocarbia when volume guaran-tee was used (27% vs 61%, P � .05).
Further studies have addressed the efficacy of the var-ious volume-guarantee modes. Fully supported breaths ap-pear to be more effective, as demonstrated by Abubakarand Keszler’s crossover trial of assist-control plus volumeguarantee versus SIMV plus volume guarantee.14 Another
MECHANICAL VENTILATION OF THE NEONATE: SHOULD WE TARGET VOLUME OR PRESSURE?
RESPIRATORY CARE • SEPTEMBER 2009 VOL 54 NO 9 1241

crossover trial by Scopesi and colleagues suggested that inthe weaning phase, volume guarantee in modes that sup-port every breath may be more effective than a combina-tion of SIMV plus volume guarantee.15
The protective effects of volume guarantee are high-lighted by the trial done by Lista et al, in which 53 pre-mature infants with RDS were randomized to receive ei-ther PSV alone or PSV plus volume guarantee.16 A VT of5 mL/kg was targeted for all study patients. Tracheal as-pirates were obtained on days of life 1, 3, and 7, andpro-inflammatory cytokines interleukin 6 (IL-6), IL-8, andtumor necrosis factor alpha were measured. Statisticallysignificant elevations in IL-6 and IL-8 were found in pa-tients who received only PSV, compared to PSV plus vol-ume guarantee. The volume-guarantee group also had lowerairway pressures and decreased duration of ventilation,though the latter did not reach statistical significance. Nev-ertheless, this study suggests that volume-targeted venti-lation may reduce ventilator-induced lung injury.
A subsequent study by Lista and colleagues examinedthe inflammatory effects of ventilation with variable vol-umes.17 The targeted volume of 5 mL/kg used in theirearlier study was compared to a smaller 3.5 mL/kg vol-ume. Interestingly, the lower volume had a statisticallysignificant increase in cytokine levels. Duration of venti-lation was also prolonged for the low-VT group (9.2 d vs16.8 d, P � .05). It was hypothesized that these findingsresulted from atelectrauma.
Lista et al most recently compared volume guarantee(5 mL/kg) with high-frequency oscillatory ventilation.18
This analysis revealed higher pro-inflammatory cytokineconcentrations and longer oxygen dependence in patientsreceiving high-frequency oscillatory ventilation, comparedto those receiving assist-control plus volume guarantee.These findings raise more questions regarding optimal mo-dalities and what constitutes the ideal VT.
Clinical studies of conventional ventilation have thusfar used target VT of 3–6 mL/kg.19 However, it is unlikelythat “one size fits all,” and more research is warranted inthis area.20
Pressure-Regulated Volume Control
The evidence for pressure-regulated volume control ven-tilation is quite sparse. Piotrowski and colleagues com-pared pressure-regulated volume control to time-cycledpressure-limited intermittent mandatory ventilation in arandomized controlled trial.21 Sixty patients with RDS orcongenital pneumonia requiring ventilatory support, weigh-ing � 2,500 g, were enrolled in this study. Primary out-comes included the duration of ventilation and the inci-dence of BPD. No statistically significant differences werefound between the 2 groups; however, subgroup analysisof infants � 1,000 g revealed a significant decrease in both
the duration of ventilation and hypotension in the pres-sure-regulated volume-control group compared to the time-cycled pressure-limited ventilation group (P � .05). Ad-ditional outcomes included a statistically significantdecrease in the incidence of severe (grade 3–4) intraven-tricular hemorrhage in the pressure-regulated volume-con-trol group (11% vs 35%, P � .05). Air leaks were also lessfrequent in the pressure-regulated volume-control group,although this did not reach statistical significance.
D’Angio and colleagues compared pressure-regulatedvolume control to time-cycled pressure-limited SIMV.22
They studied 213 infants who required mechanical venti-lation and were at least 24 weeks gestational age andweighed 500–1,249 g at birth. Primary outcome analysisrevealed no statistically significant differences betweenthe 2 groups for the number of infants who were alive andextubated at 14 and 28 days of life, and at 36 weekspost-menstrual age. There was no difference in the inci-dence of BPD at 36 weeks post-menstrual age. The authorsnoted that infants in the pressure-regulated volume-controlgroup were less likely to fail their assigned modality thanthose in the SIMV group (relative risk 0.61, 95% CI 0.38–0.97). The authors concluded that pressure-regulated vol-ume control did not provide any clear benefits over time-cycled pressure-limited SIMV.
Meta-analysis
There has been one meta-analysis comparing volume-targeted to pressure-limited ventilation in the neonate thusfar.23 Four of the trials discussed above, consisting of 178patients, met the inclusion criteria for this meta-analy-sis.7,12,16,22 The 2 primary outcome measures were hospitalmortality, and death or need for supplemental oxygen ateither 28 days of life or 36 weeks post-conceptual age.There were no statistically significant differences noted inthe first outcome measure. As for secondary outcomes,there was a significant reduction in the mean number ofdays of intermittent positive-pressure ventilation in thevolume-targeted group (weighted mean difference �2.93,with a 95% CI of �4.28 to �1.57). This volume groupalso had a lower incidence of pneumothorax (relative riskof 0.23, with a 95% CI of 0.07 to 0.76). Grade 3–4 intra-ventricular hemorrhage was less common in the volume-targeted group (relative risk of 0.32, 95% CI of 0.11 to0.9). Furthermore, there was a trend toward decreased BPDin the volume-targeted group that approached—but didnot reach—statistical significance (relative risk 0.34,95% CI of 0.11 to 1.05). The authors concluded that sta-tistically significant effects favoring volume-targeting wereshown, but further trials are still needed. When the studyby Singh et al8 is added to these trials, there is a statisti-cally significant reduction in the duration of ventilationand the incidence of pneumothorax, and the relative risk of
MECHANICAL VENTILATION OF THE NEONATE: SHOULD WE TARGET VOLUME OR PRESSURE?
1242 RESPIRATORY CARE • SEPTEMBER 2009 VOL 54 NO 9

BPD is 0.7 (95% CI 0.5 to 1.05) (personal communication,Peter G Davis, Department of Paediatrics, Royal Women’sHospital, Parkville, Australia).
Why Does It Work?
The revival of volume-targeted ventilation in the treat-ment of neonatal respiratory failure and its early successraises questions about mechanisms of efficacy. While it isreasonable to believe that faster reduction in pressure mightobviate both barotrauma and volutrauma, other factors areno doubt involved.
A recent study by Swamy and colleagues24 examinedthe patients in the Singh et al trial.8 They looked at dif-ferences in VT delivery in babies assigned to either VCVor time-cycled pressure-limited ventilation. Although themedian VT was quite similar, there was a statistically sig-nificant reduction in the variability of VT delivery for ba-bies receiving VCV. This could explain why they wereable to be weaned faster and perhaps why there was lesslung injury.
In a study of adult patients, Kallet and colleagues25
showed differences in the work of breathing among pa-tients randomized to VCV (1.09 � 0.59 J/L), pressure-control ventilation (1.27 � 0.58 J/L), and pressure-regu-lated volume control (1.35 � 0.60 J/L). While comparabledata do not exist yet for neonatal patients, it does suggestanother mechanism of benefit.
Summary
In summary, volume-targeted ventilation of newbornswith respiratory failure leads to small but clinically im-portant improvements in short-term pulmonary outcomes,including BPD. Further investigation is warranted to bettercomprehend and refine the technique and to determine theoptimal clinical applications. These should also include anassessment of clinically relevant long-term outcomes.
REFERENCES
1. Bandy KP, Nicks JJ, Donn SM. Volume-controlled ventilation forsevere neonatal respiratory failure. Neonatal Intensive Care 1992;5(3):70-73.
2. Sinha SK, Donn SM. Volume-controlled ventilation. In: GolsmithJP, Karotkin EH, editors. Assisted ventilation of the neonate, 4thedition. Philadelphia: WB Saunders; 2003:171-182.
3. Donn SM, Bandy KP. Volume-controlled ventilation. In: Donn SM,Sinha SK, editors. Manual of neonatal respiratory care, 2nd edition.Philadelphia: Mosby-Elsevier; 2006:206-209.
4. Keszler M, Abubakar KM. Volume guarantee ventilation. Clin Peri-natol 2007;34(3):107-116.
5. Bushell MK. Servo-i ventilator. In: Donn SM, Sinha SK, editors.Manual of neonatal respiratory care, 2nd edition. Philadelphia: Mosby-Elsevier; 2006:273-278.
6. Becker MA, Donn SM. Bird VIP Gold ventilator. In: Donn SM,Sinha SK, editors. Manual of neonatal respiratory care, 2nd edition.Philadelphia: Mosby-Elsevier; 2006:249-255.
7. Sinha SK, Donn SM, Gavey J, McCarty M. Randomised trial ofvolume controlled versus time cycled, pressure limited ventilation in
preterm infants with respiratory distress syndrome. Arch Dis Child1997;77(3):F202-F205.
8. Singh J, Sinha SK, Clarke P, Byrne S, Donn SM. Mechanical ven-tilation of very low birth weight infants: is volume or pressure abetter target variable? J Pediatr 2006;149(3):308-313.
9. Singh J, Sinha S, Alsop E, Gupta S, Misra A, Donn S; Heart of EnglandNHS Foundation Trust. Long term follow up of VLBW infants from aneonatal volume versus pressure mechanical ventilation trial. Arch DisChild Fetal Neonatal Ed, 2009. Mar 25 [Epub ahead of print].
10. Cheema IU, Ahluwalia JS. Feasibility of tidal volume-guided ven-tilation in newborn infants: a randomized, crossover trial using thevolume guarantee modality. Pediatrics 2001;107(6):1323-1328.
11. Herrera CM, Gerhardt T, Claure N, Everett R, Musante G, ThomasC, Bancalari E. Effects of volume-guaranteed synchronized intermit-tent mandatory ventilation in preterm infants recovering from respi-ratory failure. Pediatrics 2002(3):110:529-533.
12. Keszler M, Abubakar K. Volume guarantee: stability of tidal volumeand incidence of hypocarbia. Pediatr Pulmonol 2004;38(3):240-245.
13. Cheema IU, Sinha AK, Kempley ST, Ahluwalia JS. Impact of vol-ume guarantee ventilation on arterial carbon dioxide tension in new-born infants: a randomised controlled trial. Early Hum Devel 2007;83(3):183-189.
14. Abubakar K, Keszler M. Effect of volume guarantee combined withassist/control vs synchronized intermittent mandatory ventilation. JPerinatol 2005;25(10):638-642.
15. Scopesi F, Calevo MG, Rolfe P, Arioni C, Traggiai C, Risso FM,Serra G. Volume targeted ventilation (volume guarantee) in the wean-ing phase of premature newborn infants. Pediatr Pulmonol 2007;42(10):864-870.
16. Lista G, Colnaghi M, Castoldi F, Condo V, Reali R, Compagnoni G,Mosca F. Impact of targeted-volume ventilation on lung inflamma-tory response in preterm infants with respiratory distress syndrome(RDS). Pediatr Pulmonol 2004;37(4):510-514.
17. Lista G, Castoldi F, Fontana P, Reali R, Reggiani A, Bianchi S,Compagnoni G. Lung inflammation in preterm infants with respira-tory distress syndrome: effects of ventilation with different tidalvolumes. Pediatr Pulmonol 2006;41(4):357-363.
18. Lista G, Castoldi F, Bianchi S, Battaglioli M, Cavigioli F, BosoniMA. Volume guarantee versus high-frequency ventilation: lung in-flammation in preterm infants. Arch Dis Child Fetal Neonatal Ed2008;93(4):F252-F256.
19. Polimeni V, Claure N, D’Ugard C, Bancalari E. Effects of volume-targeted synchronized intermittent mandatory ventilation on sponta-neous episodes of hypoxemia in preterm infants. Biol Neonate 2006;89(1):50-55.
20. Keszler M. Volume guarantee and ventilator-induced lung injury:Goldilocks’ rules apply. Pediatr Pulmonol 2006;41(4):364-366.
21. Piotrowski A, Sobala W, Kawczynski P. Patient-initiated, pressure-regulated, volume-controlled ventilation compared with intermittentmandatory ventilation in neonates: a prospective, randomised study.Intensive Care Med 1997;23(9):975-981.
22. D’Angio CT, Chess PR, Kovacs SJ, Sinkin RA, Phelps DL, KendigJW, et al. Pressure-regulated volume control ventilation vs synchro-nized intermittent mandatory ventilation for very low-birth-weightinfants: a randomized controlled trial. Arch Pediatr Adolesc Med2005;159(9):868-875.
23. McCallion N, Davis PG, Morley CJ. Volume-targeted versus pres-sure-limited ventilation in the neonate. Cochrane Database Syst Rev2005;(3):D003666.
24. Swamy R, Gupta S, Singh J, Donn SM, Sinha SK. Tidal volumedelivery and peak inspiratory pressure in babies receiving volumetargeted or time cycled, pressure limited ventilation: a randomizedcontrolled trial. J Neonatal-Perinatal Med 2008;1(2):239-243.
25. Kallet RH, Hemphill JC III, Dicker RA, Alonso JA, Campbell AR,et al. The spontaneous breathing pattern and work of breathing ofpatients with acute respiratory distress syndrome and acute lunginjury. Respir Care 2007;52(8):989-995.
MECHANICAL VENTILATION OF THE NEONATE: SHOULD WE TARGET VOLUME OR PRESSURE?
RESPIRATORY CARE • SEPTEMBER 2009 VOL 54 NO 9 1243