Measuring*liver*iron*contentin* …...Heterogeneity*of*iron*concentraon* throughoutthe*liver* Sample...
40
Measuring liver iron content in thalassaemia and sickle cell disease Maciej Garbowski, MD, University College London
Transcript of Measuring*liver*iron*contentin* …...Heterogeneity*of*iron*concentraon* throughoutthe*liver* Sample...

Measuring liver iron content in thalassaemia and sickle cell disease
Maciej Garbowski, MD, University College London

What is liver iron? • Cellular FerriAn (not serum ferriAn) • Haemosiderin (old ferriAn, parAally degraded iron rich) • Labile iron pool (regulatory) • Iron in cellular enzymes, as prostheAc groups: heme, iron-‐sulfur cluster
– Mitochondria • <1.8mg/gdw normal range LIC (liver iron content)
Where is liver iron? • Hepatocyte (parenchymal): typically from gut
uptake of diet iron, also during redistribuAon from spleen – HFE haemochromatosis – Thalassaemia intermedia:
• As transferrin iron uptake±NTBI uptake • Hb-‐Haptoglobin uptake • Haem-‐haemopexin, methaemalbumin uptake
• Macrophage (Kupfer cells) – Transfusional haemosiderosis
• Hb-‐haptoglobin • As red cells aXere splenectomy BaYs K. Mod Pathol 2007

Why measure liver iron overload? • LIC predicts total body storage iron in TM1
• Absence of pathology – heterozygotes of HH where liver levels < 7 mg/g dry weight
• Liver pathology – abnormal ALT if LIC > 17 mg/g dry weight2 – liver fibrosis progression if LIC > 16 mg/g dry weight3
• Cardiac pathology at high levels
– Increased LIC linked to risk of cardiac iron in unchelated paAents 2,6
– LIC >15 mg/g dry weight associaAon with cardiac death • all of 15/53 TM paAents who died4 • improvement of subclinical cardiac dysfuncAon with venesecAon alone post-‐BMT5
1. Angelucci E, et al. N Engl J Med. 2000;343:327-‐31. 2. Jensen PD, et al. Blood. 2003;101:91-‐6. 3. Angelucci E, et al. Blood. 2002;100:17-‐21.
4. BriYenham GM, et al. N Engl J Med. 1994;331:567-73. 5. Mariog E, et al. Br J Haematol. 1998;103:916-‐21. 6. Buja LM, Roberts WC. Am J Med. 1971;51:209-‐21
ALT = alanine aminotransferase; BMT = bone marrow transplantaAon.

4
Body iron (mg/kg) = 10.6× hepaAc iron concentraAon (mg/g dry weight)
Sample <1 mg Dry Weight (n=23)
Body iron
stores (m
g/kg)
300
250
200
150
100
50
0
r=0.83
0 5 10 15 20 25 HepaAc iron concentraAon (mg/g dry weight)
Angelucci et al. N Engl J Med. 2000;343:327.
Liver Iron ConcentraAon Predicts Total Body Iron Stores
0 5 10 15 20 25
300
250
200
150
100
50
0
r=0.98
Body iron
stores (m
g/kg)
HepaAc iron concentraAon (mg/g dry weight)
Sample >1 mg Dry Weight (n=25)

Liver enzymes and iron overload
AST U/L
16.8mg/g dry wt
AL
T U/L
Jensen PD, et al. Blood. 2003;101:91-‐6

How to measure liver iron
• IntervenAonal – Biopsy
• Non-‐intervenAonal – SQUID – MRI – Serum markers?

Biopsy-‐measured LIC • Standard procedure 16 g needle under local anesthesia
typically into right lateral lobe • Small sample about 1g dry weight, up to 4g wet weight • Fresh/Fixed (PFA) • Allows for histology assessment, staging, grading • Semi-‐quanAtaAve Perl stain for iron and hepatocyte vs
Kupfer cell distribuAon • QuanAtaAve biochemical analysis of iron content per gram
Assue: – Dry weight: aXer drying – Wet weight – at biopsy before fixing with PFA or unfixed – Paraffin embedded for histology:
• Dewaxing causes fat deposits to be washed away with solvents
• Tissue weight is reduced, denominator is lower, LIC higher
2 cm

LIC by biopsy: Disadvantages • Coefficient of variability 19-‐40%
– Due to patchy iron distribuAon in the liver (distribuAon artefact)
– Small sample size – Effect of fibrosis
• no global LIC esAmaAon • Not standardized – colorimetric vs Atomic AbsorpAon • Wet/dry raAo in different labs • ComplicaAons • PaAent preference • Rarely used in chelaAon clinical trials

Heterogeneity of iron concentraAon throughout the liver
Sample size and type CV of LIC Pathology Source
Needle biopsy (< 4 mg dry weight)
19% Normal Emond, et al. 1999 Kreeftenberg, et al. 1984
Needle biopsy
(< 4 mg dry weight) > 40% End-stage
liver disease Emond, et al. 1999 Kreeftenberg, et al. 1984
Needle biopsy (9 mg dry weight)
9% Normal Barry, Sherlock. 1971
“Cubes” (200–300 mg wet weight)
17% 24%
β-thalassaemia
Non-cirrhotic
Ambu, et al. 1995
“Cubes” (1,000–3,000 mg wet weight),
19% β-thalassaemia Part-cirrhotic
Clark, et al. 2003
CV = coefficient of variaAon.
Ambu R, et al. J Hepatol. 1995;23:544-‐9; Barry M, Sherlock S. Lancet. 1971;1:100-‐3;
Clark PR, et al. Magn Reson Med. 2003;49:572-‐5; Emond MJ, et al. Clin Chem. 1999;45:340-‐6;
KreeXenberg HG, et al. Clin Chim Acta. 1984;144:255-‐62.

How to measure liver iron
• IntervenAonal – Biopsy
• Non-‐intervenAonal – Serum markers? – SQUID – MRI

Use serum ferriAn instead of LIC ? • Advantages
• Simple • Widely available • Serum ferriAn broadly correlated with body iron (macrophages) • Validated as predictor of complicaAons of iron overload in TM
• Disadvantages • Origin of serum ferriAn differs above values of 4K • Raised by inflammaAon or Assue damage (e.g. sickling crisis) • Lowered by vitamin C deficiency • RelaAonship of ferriAn to body iron varies in different diseases
• Low relaAve to LIC in Thal intermedia (hepatocellular > macrophages) • Higher and variable in SCD

Non-‐intervenAonal LIC measurement
• Serum markers: FerriAn – RelaAonship with LIC is different in SCD, TI and TDT
– Hepatocyte iron overload has disproporAonately low serum ferriAn unAl liver damage occurs and Assue ferriAn is released
– Kupfer cell and RES: transfusional iron overload is beYer marked by secreted ferriAn Origa, Hamatologica 2007, 92 583

How to measure liver iron
• IntervenAonal – Biopsy
• Non-‐intervenAonal – Serum markers? – SQUID=superconducAng quantum interference device
– MRI • R2* i.e. 1/T2* Anderson 2001 proof of concept • R2 i.e. 1/T2 (Ferriscan) St Pierre 2005

Principle of MR imaging for iron
• Iron overload shortens the Assue relaxaAon Ames in the longitudinal axis (T1) and transverse axis (T2) on which magneAc resonance imaging is based
• The decrease in the intensity of spin echo images (1/T2 or R2) with iron overload derives from shortening in the T2 relaxaAon Ames (Leung et al., 1984; Stark, 1991).
• This T2 shortening is mainly due to the paramagneAc properAes of ferriAn iron (Brown et al., 1985) (Stark, 1991)
• The spin echo can be detected in several ways, the shorter the echo Ame, the greater the sensiAvity
• The gradient echo relies on mulAple echos over a shorter acquisiAon Ame period than spin echo techniques

R2* = R2 + R2’
1/T2* = 1/T2 + 1/T2’
Intrinsic effects Tissue relaxaFon
Extrinsic effects MagneFc inhomogeneity
R2*
[Fe]
[Fe]
T2*

• Gradient echo (T2*) – Long first echo Ames (2-‐20ms) – not suitable for high LIC – MulAple breath-‐holds – Variable weights of biopsy specimens – BeYer calibraAon with non-‐fibroAc samples
• Normal liver T2* 33±7ms • LIC=0.0146(R2*)-‐0.45; T2* of 5ms=2.47mgFe/g dw • Main purpose to establish the relaAonship between Assue iron and T2* rather than exact quanAficaAon of iron
T2*LIC by Anderson et al.
Anderson L, et al. Eur Heart J 2001;22:2171-‐9.

T2*LIC by Anderson et al. • paper focused on cardiac iron • but this was the 1st report to show Proof of Concept that
Assue iron relates to Assue MR relaxivity (T2*)
• Cardiac T2* not related to heart Assue iron, • this relaAonship shown for liver iron in 30
paAents with beta thalassaemia, therefore • in general: Assue T2* relates to Assue iron
more iron
Anderson L, et al. Eur Heart J 2001;22:2171-‐9.

T2* RBH-‐UCLH • Updated T2* LIC method, used at UCLH, Heart Hospital, Bart’s and RBH – 50 liver biopsies from 25 paAents paired with MRI scan
– Newer T2* acquisiAon: shorter first echo Ame, more echo Ames
– Single laboratory biopsies as part of deferasirox registraAon studies (Renne, France)
Garbowski et al 2014, JCMR 16(1) p.40

T2*LIC RBH-‐UCLH • 1.5T Sonata MR scanner at Royal Brompton Hospital, London.
• Transverse slice through the centre of the liver using a mulA-‐echo single breath-‐hold gradient echo T2* sequence -‐ echo Ames TE 0.93-‐16.0ms, shorter and more closely spaced
• T2* decay was measured using Thalassaemia tools (Cardiovascular Imaging SoluAons, London, UK) from a region of interest (ROI) in an area of homogeneous liver Assue, avoiding blood vessels.
• To account for background noise, a truncaAon method was used for curve-‐figng.
• All T2* measurements were performed in triplicate by 2 independent observers choosing three separate ROIs to analyse.
• The Regions of Interest were chosen to be as large as possible in three separate areas (anterior, mid/lateral and posterior).
• Corrects Anderson T2*LIC by 220%: T2*=5 ms is now 2.47*2.2=5.43mgFe/g dry weight
Method
Garbowski et al 2014, JCMR 16(1) p.40

Other T2*LIC callibraAons
Wood JC, et al. Blood. 2005;106:1460-‐5.
HIC = hepaAc iron concentraAon.
Hankins JS, et al. Blood. 2009;113:4853-‐5.
1/T2*=R2*

Comparing T2*-‐LIC calibraiAons
Garbowski et al 2014, JCMR 16(1) p.40
1/T2*=R2*

R2-‐LIC Ferriscan • Transverse images with a mulA-‐slice single spin-‐echo (SSE) pulse
sequence • Slice thickness of 5 mm • 25 minute acquisiAon • Frequently employed in chelator clinical trials • Central reporAng in Perth, Australia • Validated regularly for inter-‐site reproducibility
St Pierre TG, et al. Blood. 2005;105:855-‐61

No iron overload
Thalassemia major
R2 (s-1)
R2 (s-1)
233
194
155
116
77
0
0 80 160 240 320 400
0 80 160 240 320 400
Voxels 500
400
300
200
100
0
R2-‐LIC Ferriscan
St Pierre TG, et al. Blood. 2005;105:855-‐61

24 St Pierre et al. Blood. 2005;105:855.
300
250
200
150
100
50
0 0 10 20 30 40
Biopsy iron concentraAon (mg/g dry Assue)
Mean transverse re
laxaAo
n rate R
2 (s-‐1)
HepaAAs
Hereditary hemochromatosis
Beta-‐thalassemia/hemoglobin E
Beta-‐thalassemia
St Pierre TG, et al. Blood. 2005;105:855-‐61.
RelaAonship between R2 and needle biopsy LIC (dry weight)

Comparing Ferriscan and T2*LIC • 92 scans in 54 paAents with transfusional
iron overload • Bland-‐Altman analysis showed
unacceptably wide limits of agreement • THEREFORE methods cannot be used
interchangeably when following LIC trends • One method should be used to follow
trends
Garbowski et al 2014, JCMR 16(1) p.40

Non-‐interchangeability of R2LIC and T2*LIC
• Poor agreement between T2* LIC and R2LIC – not derived from ROI-‐related and reproducibility-‐related variability of
both methods • T2*LIC and Ferriscan have excellent reproducibility
– likely stems from different sensiAvity of R2 and R2* to iron distribuAon in the Assue and to sources of noise.
– Further studies necessary

Case 1 • 30 yo TD Eβ-‐Thalassaemia paAent on DFX 30mg/kg/d, variable compliance historically, on
clinical trial with sotatercept (reported 2014 ASH abstract) • T2*LIC Jan 2015 25mg/gdw, no cardiac iron • Serum FerriAn trend 3000 down to 1400ug/L on DFX but drop in transfusion requirements
by 33%: ILR reduced from 0.32mgFe/kg/d to 0.22mgFe/kg/d • “SoX landing” with DFX as ferriAn approaching 1000ug/L – dose was to be reduced from 30
to 20mg/kg • Ferriscan was requested Oct 2015
– R2-‐LIC 23mg/gdw
• Is the LIC reduced? – Difficult to tell. SF trend suggests yes
• Should DFX dose be reduced? – But what about LIC ?
next management step?
Request T2*LIC to compare with baseline Ferriscan and T2*LIC don’t agree – poor agreement on Bland-‐Altman in the same paAent Longitudinal trends in LIC should be read using the same LIC method
S-‐ferriAn [ug/L]
ALT [IU
/L]
LIC=25 mg/g 23 mg/g

Case 2 • 28 yo TDT paAent on 25mg/kg/d DFX
approaching the “soX-‐landing” threshold for dose reducAon
• 3u PRBC/month ILR=0.4mgFe/kg/d • 16 Nov 2014 T2* LIC 4mg/gdw with SF
~1500ug/L, no cardiac iron • Develops acute kidney injury in Apr 2015
at SF 1100ug/L • DFX was stopped • S-‐creaAnine checked weekly,
normalized by Jul 2015 • Off-‐treatment 6 weeks • FerriAn increased>2000ug/L
• Restarted at DFX 0.5g/OD (10mg/kg/d) • Sep 2015 R2LIC 3.8mg/gdw and T2*LIC
6.0mg/gdw • LIKELY reached normal liver iron despite
SF>1000 when AKI occurred in Apr 2015
S-‐ferriAn [ug/L]
S-‐crea [u
mol/L]
LIC=4 mg/g 6 mg/g ??

FerriAn LIC?
• There is a disconnect between LIC and ferriAn in some paAents which may lead to problems with AtraAng chelator dose.

LIC and serum ferriAn use in chelaAon studies
• The primary outcome in establishing efficacy is typically LIC difference and typically measured by R2LIC (Ferriscan) or R2*LIC
• FerriAn trend is similarly useful • However absolute ferriAn value less so • FerriAn response vs LIC response problem (317paAents on DFX>1year)
– Serum ferriAn response • Occurs in 73% of paAents • Predicts LIC response in 80% of paAents • Is more likely to predict LIC response when baseline serum ferriAn is <4000 ng/mL
(88 vs 70%) • Closer correlaAon of ferriAn with LIC trends when ferriAn <4000ng/ml
– Serum ferriAn nonresponse • Occurs in 27% of paAents • Over half of these (52%) have a LIC response • Is more likely with
– Higher transfusional iron intake – Lower deferasirox dose
Porter et al 2014 ASH oral presentaAon 2014

Serum ferriAn response predicts an LIC response in more paAents when baseline serum ferriAn is <4000 ng/mL
88.7
52.6
70.3
50.0
0
10
20
30
40
50
60
70
80
90
100
Prop
orAo
n of paA
ents (%
)
Serum ferriAn nonresponders show a similar LIC response rate irrespecAve of baseline serum ferriAn
Serum ferriFn nonresponders
Serum ferriFn responders
31
Baseline serum ferriFn <4000 ≥4000 <4000 ≥4000
Porter et al 2014 ASH oral presentaAon 2014

Stronger correlaAon between serum ferriAn and LIC absolute change when baseline serum ferriAn <4000 ng/mL
LIC absolute change from
baseline
(mg Fe/g dw)
20
-‐30
-‐20
-‐10
0
10
-‐40
Serum ferriAn absolute change from baseline (ng/mL)
-‐12,000 8000 -‐8000 -‐4000 0 4000
32 Porter et al 2014 ASH oral presentaAon 2014

Conclusions • Tissue ferriAn and haemosiderin iron shortens MR relaxiviAes in the
Assue thus allowing for iron quanAficaAon by MRI • Biopsy based quanAficaAon of LIC is being replaced by MRI
methods • Ferriscan R2LIC is well established clinically and in research, longer
acquisiAon, reports available within a few days (Australia) • T2*LIC has been improved, acquisiAon is rapid and can be used
together with heart T2*, reports may be on the same day. • T2*LIC and Ferriscan R2LIC are not interchangeable – one method
needs to be used in following up trends • Serum ferriAn trend very useful and typically follows LIC trends but
there are discrepancies when ferriAn >4000ug/L • FerriAn-‐LIC relaAonship differs in SCD, TDT and NTDT

Thank you
QuesAons?

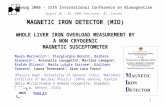
SQUID (liver susceptiometry)
• First validated non-invasive method for liver iron • Linear relationship to iron by biopsy • Only 4 operating machines in world • Expensive but room temperature devices being developed • Unclear about comparison between centres • Underestimated LIC in deferasirox studies Fischer R. In: Andra W, Nowak H, editors. MagneAsm in medicine: Berlin: Wiley-‐VCH; 1998. p. 286-‐301.
0
2,000
4,000
6,000
8,000
10,000
0 1,000 2,000 3,000 4,000 5,000 6,000 7,000 8,000 9,000
Liver: LIC < 5,000 μg/g Liver: LIC > 5,000 μg/g 2–4 fold biopsies Spleen Linear fit: LIC < 5,000 μg/g
LICblop = 1.03*LICBLS-‐33 R2 = 0.96
LIC from biomagneAc liver susceptometry (μg/gliv )
LIC from
biopsy (μg/g li
v)

LIC and cardiac iron • Poor predictor of cardiac iron and of cardiac complicaAons (arrhythmia and heart failure)
• Cardiac iron easily measured together with T2* LIC

LIC-‐ when to measure?
• Annually in TDT and transfused SCD • ?bi-‐annually in TI – no clear guidelines yet • In severe cardiac iron and other high risk paAents 3-‐6 monthly (together with cardiac T2*, LVEF, chamber sizes and mobility)
• ChelaAon is usually Atrated by ferriAn trend, however if there is no response in ferriAn there may be response in LIC in a substanAal proporAon of paAents

The cross secAonal relaAonship of serum ferriAn and LIC is less clear at high iron loads
38
Better correlation between baseline serum ferritin and LIC when serum ferritin is <4000 ng/mL and when LIC is <20 mg Fe/g dw
Baseline LIC (m
g Fe/g dw)
60
10
20
30
40
50
0
Baseline serum ferriAn (ng/mL)
0 18,000 2000 4000 6000 12,000 14,000 8000 10,000 16,000
Baseline LIC (m
g Fe/g dw)
60
10
20
30
40
50
0
Baseline serum ferriAn (ng/mL)
0 18,000 2000 4000 6000 12,000 14,000 8000 10,000 16,000
Baseline serum ferriAn category <4000 ng/mL ≥4000 ng/mL
Pearson correlaAon coefficient 0.59 0.19
Baseline LIC category <20 mg Fe/g dw ≥20 mg Fe/g dw
Pearson correlaAon coefficient 0.46 0.21
Porter et al 2014 ASH oral presentaAon 2014

Value of controlling serum ferriAn -‐ evidence in thalassaemia major
• Change in serum ferriAn over Ame
reflects change in LIC
– SequenAal evaluaAon of ferriAn
good index of chelaAon historya
• Maintenance of serum ferriAn < 2500 µg/L
– Over <me significantly correlates with
cardiac disease-‐free survivalb,c,d,e
a Olivieri NF, et al. N Engl J Med. 1994;331:574-‐578. B GabuK V and Piga A. Acta Haematol. 1996;95:26-‐36. C Telfer PT, et al. Br J Haematol. 2000;110:971-‐977. d Davis BA, et al. Blood. 2004 104: 263-‐9 e Borgna-‐PignaK et al. Haematologica; 89: 1187-‐1193
Survival Prob
ability
0 5 10 15
0
0.25
0.50
0.75
1.00
FerriFn >2500 μ/L on >1/3 of occasions
FerriFn <2500 μ/L on >2/3 of occasions
Years of Follow-‐Up
.
Maintenance of Lower Ferritin Levels a Positive Indicator for Survival at UCLH (unpublished data)

NonintervenAonal LIC measurement
• SQUID= superconducAng quantum interference device
• CT – under development • MRI
– R2* i.e. 1/T2* Anderson 2000 proof of concept – R2 i.e. 1.T2 (Ferriscan) St Pierre 2005