
Measuring self-report obsessionality in anorexia nervosa: Maudsley obsessive–compulsive inventory...
8
RESEARCH ARTICLE Measuring Self-Report Obsessionality in Anorexia Nervosa: Maudsley Obsessive–Compulsive Inventory (MOCI) or Obsessive–Compulsive Inventory-Revised (OCI-R)? Marion Roberts 1 , Anna Lavender 2 & Kate Tchanturia 1 * 1 Institute of Psychiatry, Department of Psychological Medicine, King’s College London, UK 2 Institute of Psychiatry, Department of Psychology, King’s College London, UK Abstract Self-report measures are often used in research and clinical practise as they efficiently gather a large amount of information. With growing numbers of self-report measures available to target single constructs, it is important to revisit one’s choice of instrument to be sure that the most valid and reliable measure is employed. The Maudsley Obsessive–Compulsive Inventory (MOCI) and the Obsessive–Compulsive Inventory-Revised (OCI-R) were admi- nistered to 223 female participants: 30 inpatients with anorexia nervosa (AN), 62 community cases with AN, 69 community cases weight restored from AN and 62 healthy controls. Both measures distinguished between clinical and healthy groups; however, the OCI-R showed superior internal reliability. Additionally, the OCI-R measures six (to the MOCI’s four) obsessive–compulsive constructs, and uses a more sensitive response format (likert scale vs. categorical). It is recommended that the OCI-R be employed as the self-report instrument of choice for assessing obsessive–compulsive pathology in those with AN. Copyright # 2010 John Wiley & Sons, Ltd and Eating Disorders Association. Keywords anorexia nervosa; obsessive–compulsive disorder; MOCI; OCI-R; psychometrics *Correspondence Dr Kate Tchanturia, PhD, Eating Disorders Unit PO59, Institute of Psychiatry, King’s College London, De Crespigny Park, London SE5 8AF, UK. Tel: 0044 207 848 0134. Fax: 0044 207 848 0181. Email: [email protected] Published online 28 December 2010 in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/erv.1072 Introduction The high level of comorbidity and symptomalogical overlap between anorexia nervosa (AN) and obsessive– compulsive disorder (OCD) has long been acknowl- edged. Co-morbidity estimates of the proportion of AN sufferers with co-morbid OCD vary widely, from 17.5% (Godart et al., 2003) to 66% (Fornari, Kaplan, Sandberg, Matthews, Skolnick, & Katz, 1992). This considerable variation may in part be due to the wide range of measurement instruments employed to measure comorbid OCD in the AN literature. Clinically, high obsessive–compulsive symptomatology has been associated with poor treatment outcome (Rastam, Gillberg, & Wentz, 2003; Thomsen, 1994) and increased severity of eating disorder psychopathology (Jimenez-Murcia et al., 2007). The complexity of this picture underlines the need to be able to assess obsessive–compulsive symptoms in eating disorder patients quickly and easily in routine clinical practice (e.g. Davies, Liao, Campbell, & Tchanturia, 2009). In brief, reliable measurement Eur. Eat. Disorders Rev. 19 (2011) 501–508 ß 2010 John Wiley & Sons, Ltd and Eating Disorders Association. 501
-
Upload
marion-roberts -
Category
Documents
-
view
214 -
download
2
Transcript of Measuring self-report obsessionality in anorexia nervosa: Maudsley obsessive–compulsive inventory...

RESEARCH ARTICLE
Measuring Self-Report Obsessionality in AnorexiaNervosa: Maudsley Obsessive–Compulsive Inventory(MOCI) or Obsessive–Compulsive Inventory-Revised(OCI-R)?Marion Roberts1, Anna Lavender2 & Kate Tchanturia1*
1Institute of Psychiatry, Department of Psychological Medicine, King’s College London, UK
2Institute of Psychiatry, Department of Psychology, King’s College London, UK
Abstract
Self-report measures are often used in research and clinical practise as they efficiently gather a large amount of
information. With growing numbers of self-report measures available to target single constructs, it is important to
revisit one’s choice of instrument to be sure that the most valid and reliable measure is employed. The Maudsley
Obsessive–Compulsive Inventory (MOCI) and the Obsessive–Compulsive Inventory-Revised (OCI-R) were admi-
nistered to 223 female participants: 30 inpatients with anorexia nervosa (AN), 62 community cases with AN, 69
community cases weight restored from AN and 62 healthy controls. Both measures distinguished between clinical
and healthy groups; however, the OCI-R showed superior internal reliability. Additionally, the OCI-R measures six
(to the MOCI’s four) obsessive–compulsive constructs, and uses a more sensitive response format (likert scale vs.
categorical). It is recommended that the OCI-R be employed as the self-report instrument of choice for assessing
obsessive–compulsive pathology in those with AN. Copyright# 2010 John Wiley & Sons, Ltd and Eating Disorders
Association.
Keywords
anorexia nervosa; obsessive–compulsive disorder; MOCI; OCI-R; psychometrics
*Correspondence
Dr Kate Tchanturia, PhD, Eating Disorders Unit PO59, Institute of Psychiatry, King’s College London, De Crespigny Park, London SE5 8AF,
UK. Tel: 0044 207 848 0134. Fax: 0044 207 848 0181.
Email: [email protected]
Published online 28 December 2010 in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/erv.1072
Introduction
The high level of comorbidity and symptomalogical
overlap between anorexia nervosa (AN) and obsessive–
compulsive disorder (OCD) has long been acknowl-
edged. Co-morbidity estimates of the proportion of AN
sufferers with co-morbid OCD vary widely, from 17.5%
(Godart et al., 2003) to 66% (Fornari, Kaplan,
Sandberg, Matthews, Skolnick, & Katz, 1992). This
considerable variation may in part be due to the wide
range of measurement instruments employed to
measure comorbid OCD in the AN literature.
Clinically, high obsessive–compulsive symptomatology
has been associated with poor treatment outcome
(Rastam, Gillberg, &Wentz, 2003; Thomsen, 1994) and
increased severity of eating disorder psychopathology
(Jimenez-Murcia et al., 2007).
The complexity of this picture underlines the need
to be able to assess obsessive–compulsive symptoms
in eating disorder patients quickly and easily in
routine clinical practice (e.g. Davies, Liao, Campbell,
& Tchanturia, 2009). In brief, reliable measurement
Eur. Eat. Disorders Rev. 19 (2011) 501–508 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association. 501

of obsessive–compulsive symptoms in patients with an
eating disorder enables more comprehensive and
individualised assessment and treatment planning,
enhancing outcome assessment. Such a measure is also
of use as a research tool, allowing efficient gathering of
data with minimal researcher input. With growing
numbers of self-report measures available to target
single constructs, it is important to revisit one’s
choice of instrument in order to be sure that the most
valid and reliable measure is employed.
The Maudsley Obsessive–Compulsive Inventory
(MOCI; Hodgson & Rachman, 1977) is a 30-item
self-report scale with a yes/no response format. It
produces a total score in addition to scores for its four
subscales: Checking, washing, doubting and slowness. It
is a well-validated instrument (Dent & Salkovskis, 1986;
Sternberger & Burns, 1990) and has been used in
numerous studies of obsessionality in various popu-
lations (Alegret, Junque, Valldeoriola, Vendrell, Marti,
& Tolosa, 2001; Kano, Ohta, Nagai, Pauls, & Leckman,
2004; Li & Chen, 2007). However, use of the MOCI
within the eating disorder population has produced
equivocal results. While some papers report favourable
discriminant validity between eating disorder and
OCD/anxiety participants (Emmelkamp, Kraaijkamp,
& van den Hout, 1999; Jimenez-Murcia et al., 2007),
others have reported no difference in MOCI score
between these populations (Fahy, 1991).
The Obsessive–Compulsive Inventory-Revised
[OCI-R; (Foa et al., 2002)] is an 18-item self-report
scale with a five-point likert scale format. Like the
MOCI, it yields both a total score and individual
scores for each of its six subscales: Checking, washing,
obsessing, neutralising, ordering and hoarding.
The OCI-R has exhibited good-to-excellent internal
reliability among clinically anxious (total scale
0.81–0.93; Foa et al., 2002) and non-anxious control
participants for all subscales but neutralising (total scale
a¼ 0.88; Hajcak, Huppert, Simons, & Foa, 2004).
Hajcak and colleagues (2004) provide strong support
for good test–retest reliability (r¼ .70), and convergent
and divergent validity of the OCI-R in a college sample.
The OCI-R has been further validated in both clinical
and subclinical populations (Abramowitz & Deacon,
2006; Huppert et al., 2007; Roberts & Wilson, 2008).
As the OCI-R appeared in the anxiety literature only
8 years ago (compared to the MOCI’s 30-year
presence), research using the OCI-R in the eating
disorder field is just beginning to emerge. Recent
studies have reported effect sizes of up to 1.9 (very large
effect) when comparing OCI-R scores of AN and
healthy control (HC) groups (Lopez et al., 2008).
Numerous studies exist in the literature exploring
the impact of clinical variables on obsessive–compul-
sive characteristics in the eating disorder population
(Altman & Shankman, 2009; Crane, Roberts, &
Treasure, 2007). This paper does not attempt a
comprehensive analysis of this topic. Rather, the aim
of this study was to determine the most appropriate
self-report measure for obsessive–compulsive traits in
the AN population by assessing their relative psycho-
metric properties, specifically discriminant validity and
internal reliability, content validity in relation to eating
disorders, and any additional aspects of the MOCI
and OCI-R which may influence their utility with
individuals with AN.
Method
Participants
Participants were 223 female volunteers between the
ages of 14 and 67. The first group were inpatients
currently in a specialist eating disorder ward for severe
AN (n¼ 30). The second group were a community
AN sample recruited from the Maudsley section of
eating disorders’ volunteer database. Volunteers that
met criteria for a lifetime diagnosis of AN based on the
Eating Disorder Diagnostic Scale (Stice, Telch, & Rizvi,
2000) were included in the study. This group was split
into those with a current BMI< 18 (AN community,
ANC; n¼ 62) and those with a current BMI� 18 (AN
community weight restored, ANC-WR; n¼ 69).
Finally, a HC general population group was collected
as a comparison (n¼ 62).
Measures
TheMaudsley Obsessive–Compulsive Inventory (MOCI)
(Hodgson & Rachman, 1977) and the Obsessive–
Compulsive Inventory-Revised (OCI-R) (Foa et al.,
2002).
Procedure
The MOCI and OCI-R were posted to all participants
on the Maudsley volunteer database (approximately
800 individuals) as part of a larger study, along with
a pre-paid return envelope. Inpatients were approached
on the ward to ask for their participation. HC were
502 Eur. Eat. Disorders Rev. 19 (2011) 501–508 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association.
Measuring Self-Report Obsessionality in AN M. Roberts et al.

recruited from a volunteer research pool at the Institute
of Psychiatry (MindSearch) and through Masters level
Psychology students. HC were not included in the
study if they endorsed disordered eating or obsessive–
compulsive traits as measured by self-report on the
overview page of the SCID-I (First, Gibbon, Spitzer, &
Williams, 1997). Participation was voluntary, and no
payment was given. The study was approved by the
local ethics committee and all participants gave
informed written consent.
Statistical methods
Data was entered into SPSS 16.0 for analysis using a
significance level of 0.05. As data was normally
distributed, differences in demographic and clinical
characteristics between groups were assessed using
ANOVA (Tukey post hoc) and Cohen’s d effect size.
Effect sizes are described as negligible (<0.15), small
(0.15–0.39), moderate (0.40–0.74), large (0.75–1.14)
and very large (>1.15). Discriminant validity was also
assessed using ANOVA and Cohen’s d to compare
group means across OCI-R and MOCI full scale and
subscale scores. Cronbach’s alpha was used as the
measure of internal reliability. Participants with
missing data (OCI-R items; MOCI items; BMI) were
excluded from the dataset (n¼ 42).
Results
Clinical characteristics
Groups differed significantly by age (F(3,221)¼ 5.64,
p¼ 0.001), where the AN inpatient group (M¼ 27.33,
SD¼ 8.88) was significantly younger than both ANC
(M¼ 36.23, SD¼ 12.78; d¼ 0.76) and ANC-WR
(M¼ 37.55, SD¼ 12.85, d¼ 0.85) groups but not the
HC group (M¼ 32.06, SD¼ 13.60, d¼ 0.39). Current
BMI for the AN inpatient group ranged between 12.0
and 17.5 (M¼ 15.36, SD¼ 1.27). This was comparable
to ANC group, range 10.1–17.6 (M¼ 14.98, SD¼ 2.02;
d¼ 0.21). BMI for the ANC-WR group (M¼ 20.98,
SD¼ 2.69) was significantly lower than that of HC
(M¼ 22.82, SD¼ 3.06; d¼ 0.61). Inpatient AN, ANC
and ANC-WR groups had comparable lowest ever
BMI’s (M¼ 12.11, SD¼ 1.41; M¼ 11.97, SD¼ 2.07;
M¼ 14.85, SD¼ 12.80; p¼ 0.13). The AN inpatient
group had a shorter duration of illness in years
(M¼ 8.20, SD¼ 5.20), compared to both ANC
(M¼ 17.03, SD¼ 7.09; d¼ 1.35) and ANC-WR
(M¼ 12.96, SD¼ 10.32; d¼ 0.53) with moderate to very
large effects. Self-report anxiety and depression as
measured by the Hospital Anxiety and Depression Scale
(Zigmond & Snaith, 1983) were both high in the inpatient
AN group (anxiety M¼ 15.5, SD¼ 3.94; depression
M¼ 13.77, SD¼ 5.99). Levels of self-report obsessive–
compulsive symptoms were high across all three clinical
groups, most notably in the inpatient AN sample and
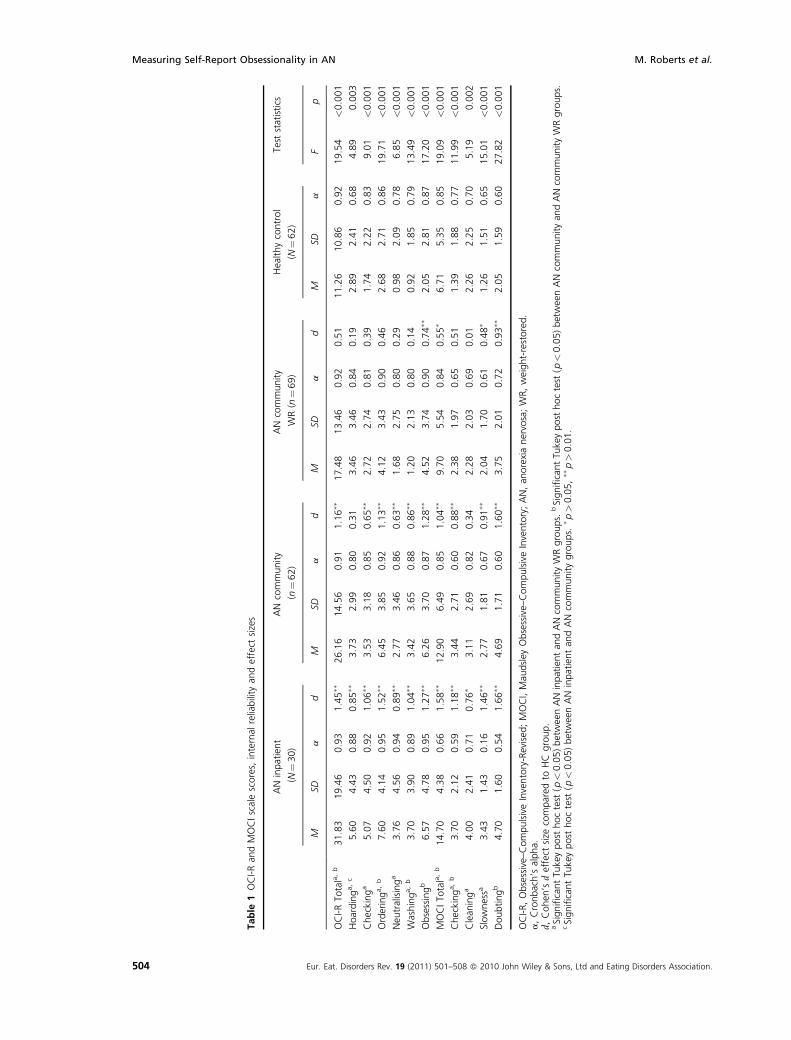
decreasing in parallel with illness severity (see Table 1).
Discriminant validity
As seen in Table 1, both the OCI-R and MOCI total
scale scores discriminated between clinical and HC
groups, with the exception of the ANC-WR and HC
group comparison on the OCI-R (p¼ 0.06). Compar-
able effect sizes were seen across full-scale group
comparisons, decreasing in magnitude from very large
effects for AN inpatient/HC, to large for ANC/HC
comparisons, to moderate for ANC-WR/HC compari-
sons. This is likely due to the moderate correlation
between BMI and both OCI-R (r(220)¼�0.37,
p< 0.001) and MOCI (r(220)¼�0.35, p< 0.001)
scale totals. Though total and subscale scores for both
the OCI-R and MOCI trend higher in the ANC-WR
group compared to HC, both measures were poor at
discriminating significantly between these two groups.
The hoarding subscale of the OCI-R was the only
subscale across both measures to discriminate signifi-
cantly between inpatient AN and ANC groups, where
a moderate effect (d¼ 0.53) was found.
Internal reliability
Acceptable Cronbach’s alphas (a>0.7) were achieved
for the total score and all subscale scores across all
participant groups for the OCI-R. High Cronbach’s
alphas (>0.8) were observed on all but three of the 28
potential scale total and subscale scores across groups,
indicating a high level of internal reliability. For the
MOCI, such high levels of internal reliability (Cron-
bach’s alphas> 0.8) were only observed for three of four
total scores (ANC, ANC-WR and HC), and the cleaning
subscale for ANC. The majority of MOCI subscale scores
showed poor internal reliability (<0.70).
Discussion
This study aimed to evaluate the utility of the MOCI
and OCI-R within an AN population on the basis of
Eur. Eat. Disorders Rev. 19 (2011) 501–508 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association. 503
M. Roberts et al. Measuring Self-Report Obsessionality in AN
Table
1OCI-Ran
dMOCIscalescores,
internal
reliability
andeffect
sizes
AN
inpatient
(N¼30)
AN
community
(n¼62)
AN
community
WR(n
¼69)
Healthycontrol
(N¼62)
Test
statistics
MSD
ad
MSD
ad
MSD
ad
MSD
aF
p
OCI-RTo
tala,b
31.83
19.46
0.93
1.45��
26.16
14.56
0.91
1.16��
17.48
13.46
0.92
0.51
11.26
10.86
0.92
19.54
<0.001
Hoardinga,c
5.60
4.43
0.88
0.85��
3.73
2.99
0.80
0.31
3.46
3.46
0.84
0.19
2.89
2.41
0.68
4.89
0.003
Checkinga
5.07
4.50
0.92
1.06��
3.53
3.18
0.85
0.65��
2.72
2.74
0.81
0.39
1.74
2.22
0.83
9.01
<0.001
Orderinga,b
7.60
4.14
0.95
1.52��
6.45
3.85
0.92
1.13��
4.12
3.43
0.90
0.46
2.68
2.71
0.86
19.71
<0.001
Neu
tralisinga
3.76
4.56
0.94
0.89��
2.77
3.46
0.86
0.63��
1.68
2.75
0.80
0.29
0.98
2.09
0.78
6.85
<0.001
Washinga,b
3.70
3.90
0.89
1.04��
3.42
3.65
0.88
0.86��
1.20
2.13
0.80
0.14
0.92
1.85
0.79
13.49
<0.001
Obsessingb
6.57
4.78
0.95
1.27��
6.26
3.70
0.87
1.28��
4.52
3.74
0.90
0.74��
2.05
2.81
0.87
17.20
<0.001
MOCITo
tala,b
14.70
4.38
0.66
1.58��
12.90
6.49
0.85
1.04��
9.70
5.54
0.84
0.55�
6.71
5.35
0.85
19.09
<0.001
Checkinga,b
3.70
2.12
0.59
1.18��
3.44
2.71
0.60
0.88��
2.38
1.97
0.65
0.51
1.39
1.88
0.77
11.99
<0.001
Clean
inga
4.00
2.41
0.71
0.76�
3.11
2.69
0.82
0.34
2.28
2.03
0.69
0.01
2.26
2.25
0.70
5.19
0.002
Slownessa
3.43
1.43
0.16
1.46��
2.77
1.81
0.67
0.91��
2.04
1.70
0.61
0.48�
1.26
1.51
0.65
15.01
<0.001
Doubtingb
4.70
1.60
0.54
1.66��
4.69
1.71
0.60
1.60��
3.75
2.01
0.72
0.93��
2.05
1.59
0.60
27.82
<0.001
OCI-R,Obsessive–CompulsiveInventory-Revised
;MOCI,Mau
dsley
Obsessive–CompulsiveInventory;AN,an
orexianervosa;WR,weight-restored.
a,Cronbach’s
alpha.
d,Cohen
’sdeffect
size
compared
toHC
group.
aSignificantTu
keypost
hoctest
(p<0.05)betwee
nANinpatientan
dANcommunityWRgroups.
bSignificantTu
keypost
hoctest
(p<0.05)betwee
nANcommunityan
dANcommunityWRgroups.
cSignificantTu
keypost
hoctest
(p<0.05)betwee
nAN
inpatientan
dAN
communitygroups.
� p>0.05,��p>0.01.
504 Eur. Eat. Disorders Rev. 19 (2011) 501–508 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association.
Measuring Self-Report Obsessionality in AN M. Roberts et al.

three main factors. These were (1) their relative
psychometric properties, specifically discriminant
validity and internal reliability, (2) their content
validity in relation to AN and (3) other features of
the instruments relevant to their routine use within an
AN population.
Psychometrics
Both the MOCI and the OCI-R total scores discrimi-
nated well (moderate to very large effect sizes) between
the clinical and HC groups, suggesting that both
measures have a high overall level of discriminant
validity. The ability of the MOCI to discriminate
reliably between AN and HC groups is contrary to
Fahy’s (1991) finding, and lends support to the MOCI’s
utility in this context.
Considering the results at a subscale level, five of the
six OCI-R subscales and three of the four MOCI
subscales discriminated between inpatient AN and
ANC-WR groups, suggesting that the measures showed
broadly comparable discriminative validity in this
respect. Similarly, three of the OCI-R and two of
the MOCI subscales discriminated between the ANC
and ANC-WR groups, again suggesting broadly
comparable ability to discriminate between these
groups. Neither measure discriminated well between
the ANC-WR group and the healthy controls, with only
the hoarding subscale of the OCI-R discriminating
between the two low-weight AN groups (discussed
below). Taken together, these results suggest that
neither measure stands out as possessing superior
discriminant validity within this population.
In contrast, the internal reliabilities of the MOCI and
OCI-R differed substantially. While the OCI-R showed
high Cronbach’s alphas on all but three of the 28
potential total and subscale scores, the equivalent
alphas for the MOCI were much less satisfactory with
only four of the potential 20 total or subscale scores
being above 0.8, and 12 being below 0.7, in the
unacceptable range. This suggests that the OCI-R is a
more internally reliable measure of obsessive–compul-
sive symptoms in the AN population than the MOCI.
Content validity
Two of the MOCI and OCI-R’s subscales, cleaning
(MOCI) and washing (OCI-R) are conceptually
matched. The content of the cleaning/washing subscales
is very similar, and although within the OCI-R the
factor has been labelled ‘cleaning’ rather than ‘washing’,
washing is mentioned in two of the three items within
the OCI-R subscale. Both measures have similar
properties in terms of ability to discriminate between
groups, although the MOCI did not discriminate
between ANC and the ANC-WR groups, suggesting
some benefit of using the OCI-R in this context.
The checking subscales are also similar in content,
with the exception of two questions within the MOCI
checking subscale that have a lower factor loading than
the others. With the checking subscales, the reverse
picture is seen from the washing/cleaning subscales, in
that the two measures perform similarly except that the
OCI-R does not discriminate between ANC and ANC-
WR groups, suggesting some benefit for the MOCI
within this domain.
An examination of the MOCI doubting items (e.g. ‘I
tend to get behind in my work because I repeat things
over and over again’; ‘I have a very strict conscience’)
indicates similarities between this construct and that of
clinical perfectionism, a key component in the cognitive
conceptualisation of eating disorders (Fairburn,
Cooper, & Shafran, 2003; Schmidt & Treasure, 2006).
Individuals with AN score higher than those with OCD
on the perfectionism subscale of the Obsessive Beliefs
Questionnaire (Lavender, Shubert, de Silva, & Treasure,
2006), and high perfectionism in AN is a consistent and
robust finding (Anderluh, Tchanturia, Rabe-Hesketh,
Collier, & Treasure, 2009; Bardone-Cone et al., 2007;
Goldner, Cockell, & Srikameswaren, 2002). Given
that the aim of a measure of obsessive–compulsive
complaints in this population is to identify symptoms
additional to those that are central to and to be expected
in an AN group, the inclusion of a subscale very similar
to the construct of perfectionism may be redundant.
It could also be anticipated that high scores on the
doubting subscale that reflect high levels of perfection-
ism would artificially elevate the MOCI total score for
this group.
Considering the final MOCI subscale, slowness in
individuals with OCD (e.g. ‘I am often late because
I can’t seem to get through everything on time’) may be
understood to be a result of their neutralising, which
can be extremely time consuming and may best be
conceptualised as an epiphenomenon of the disorder,
rather than a core feature. While this may be useful
to measure, two OCI-R subscales (neutralising and
ordering) provide a more direct measure of the
Eur. Eat. Disorders Rev. 19 (2011) 501–508 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association. 505
M. Roberts et al. Measuring Self-Report Obsessionality in AN

cognitive and behavioural underpinnings of slowness in
OCD, the specificity of which may be valuable when
assessing an eating disorder cohort.
Two items on the MOCI, ‘I find that almost every
day I am upset by unpleasant thoughts that come into
my mind against my will’ and ‘I frequently get nasty
thoughts and have difficulty in getting rid of them’,
relate to the experience of intrusive thoughts, or what
the scale authors refer to as ‘obsessional rumination’.
These items appear on both the checking and
slowness subscales, positively and negatively loaded,
respectively. The MOCI authors explain that these two
questions originally formed a fifth component, which
they ignored because it contained only two items. More
recent cognitive models of OCD (Salkovskis, 1999)
emphasise, indeed centralise, the importance of
intrusive thoughts in understanding the disorder. This
is reflected in the newer OCI-R, which contains an
obsessing subscale within which two of the three items
are nearly identical to the MOCI items above. Thus it
may make sense to include a subscale specifically
designed to measure this construct.
Finally, the OCI-R includes a hoarding subscale not
seen in the MOCI. High levels of hoarding have been
reported in the AN literature, with no difference in the
frequency of hoarding obsessions found between eating
disorder and OCD samples as measured by the clinical
rated Yale–Brown Obsessive–Compulsive Scale (Halmi
et al., 2003). Hoarding has also been found to be
elevated in a sub-clinical eating disorder population
(Roberts, 2006). It therefore seems appropriate for a
measure of OCD used in the eating disorder population
to include a hoarding component or subscale. As noted
above, the hoarding subscale of the OCI-R was the only
one across both measures to discriminate between the
inpatient AN and low weight ANC sample. It might be
that hoarding is a particular difficulty for severely ill
inpatient groups, a proposition that could usefully be
explored further. Hoarding is currently being intensively
studied and debated in the OCD literature with respect
to potential classification of ‘hoarding disorder’ as a
stand-alone diagnosis to OCD (Mataix-Cols et al., 2010).
It is, therefore, pertinent to increase our understanding of
this domain within the eating disorder population.
Other features
As noted in the introduction, the MOCI and OCI-R
differ in terms of their response formats (categorical vs.
5-point Likert scale, respectively). An advantage of the
latter in clinical practice is that it allows for gradations
of response, enabling the assessor a clearer picture of
the relevance of individual items or domains than a
dichotomous format permits. Another advantage of the
OCI-R over the MOCI for both clinical and research
purposes is that it is a shorter instrument, with 18
compared to 30 items, making its administration
quicker, easier and less demanding for the participant.
Additionally, the information gathered is richer given
that the OCI-R measures six rather than four subscales.
Limitations
The current study had a number of limitations. The first
of these was the heterogeneity of our community AN
sample, who were at various stages within their eating
disorder including some who at the time of the study
did not meet diagnostic criteria for AN. We addressed
this difficulty by dividing the community group into
those with a currently low weight, and those whose
weight had been restored. However, in the absence of
clinical diagnoses for these individuals, this remains a
limitation. Another limitation was the relatively smaller
sample of inpatient participants compared with the
community AN and HC groups. This limitation was a
consequence of the clinical reality that there are many
fewer inpatients than outpatients within our service. A
third limitation was the absence of a formal OCD
diagnostic assessment within the samples. This may
have masked scores elevated due to comorbidity with
Axis I OCD, across the groups.
Conclusion
This study aimed to evaluate the utility of the MOCI
and OCI-R within four female samples: inpatients with
current AN, community participants with lifetime
AN and a current low BMI (<18), community
participants with lifetime AN and a current healthy
weight and a healthy control group. While discriminant
validity was broadly similar between the measures,
when taking into account the findings for internal
reliability, content validity and other factors relevant
to assessing OCD in the AN population, the OCI-R
emerged as the superior measure.
The MOCI and the OCI-R are both valuable
instruments and each has its merits in the assessment
of obsessive–compulsive symptoms. TheMOCI is time-
tested and, being the more widely employed measure,
506 Eur. Eat. Disorders Rev. 19 (2011) 501–508 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association.
Measuring Self-Report Obsessionality in AN M. Roberts et al.

its use particularly for research purposes enables cross
comparison of data more easily than the newer OCI-R.
However, for the assessment of obsessive–compulsive
symptoms in individuals with AN, the OCI-R offers a
number of advantages. Higher internal reliability within
the AN population in addition to the length and format
of the OCI-R offer clear benefits over the MOCI.
Additionally, an analysis of both measures’ scale/
subscale content suggests that the OCI-R offers a more
useful approach for the assessment of a broader range of
obsessive–compulsive symptoms in the AN population.
We, therefore, suggest that the OCI-R be used in place
of the MOCI when a short, reliable self-report measure
of OCD is required in the AN population.
Acknowledgements
M. Roberts was funded by a Nina Jackson Fellowship
(RIED) with the Psychiatry Research Trust. Data were
part of the BIAL funded project awarded to K. Tchan-
turia (grant numbers 88/02, 61/04). The authors wish to
acknowledge students Mandy Dimmer, Thomas Liao
and Laura Prytherch for assistance with data collection.
References
Abramowitz, J. S., & Deacon, B. J. (2006). Psychometric
properties and construct validity of the Obsessive-
Compulsive Inventory–Revised: Replication and
extension with a clinical sample. Journal of Anxiety
Disorders, 20, 1016–1035.
Alegret, M., Junque, C., Valldeoriola, F., Vendrell, P.,
Marti, M., & Tolosa, E. (2001). Obsessive-compulsive
symptoms in Parkinson’s disease. Journal of Neurol-
ogy, Neurosurgery & Psychiatry, 70, 394–396.
Altman, S. E., & Shankman, S. A. (2009). What is the
association between obsessive-compulsive disorder
and eating disorders? Clinical Psychology Review, 29,
638–646.
Anderluh, M., Tchanturia, K., Rabe-Hesketh, S., Collier,
D., & Treasure, J. (2009). Lifetime course of eating
disorders: Design and validity testing of a new strategy
to define the eating disorders phenotype. Psychological
Medicine, 39, 105–114.
Bardone-Cone, A. M., Wonderlich, S. A., Frost, R. O.,
Bulik, C. M., Mitchell, J. E., & Uppala, S., et al. (2007).
Perfectionism and eating disorders: Current status
and future directions. Clinical Psychology Review,
27, 384–405.
Crane, A. M., Roberts, M. E., & Treasure, J. (2007). Are
Obsessive-compulsive personality traits associated
with a poor outcome in anorexia nervosa? A
systematic review of randomised controlled trials
and naturalistic outcome studies. International Journal
of Eating Disorders, 40, 581–588.
Davies, H., Liao, P. C., Campbell, I. C., & Tchanturia, K.
(2009). Multidimensional self reports as a measure of
characteristics in people with eating disorders. Eat
Weight Disord, 14, e84–e91.
Dent, H. R., & Salkovskis, P. M. (1986). Clinical measures
of depression, anxiety and obsessionality in non-
clinical populations. Behaviour Research and Therapy,
24, 689–691.
Emmelkamp, P., Kraaijkamp, H., & van den Hout, M.
(1999). Assessment of obsessive-compulsive disorder.
Behavior Modification, 23, 269–279.
Fahy, T. A. (1991). Obsessive-compulsive symptoms in
eating disorders. Behaviour Research and Therapy, 29,
113–116.
Fairburn, C. G., Cooper, Z., & Shafran, R. (2003). Cog-
nitive behaviour therapy for eating disorders: A
‘‘transdiagnostic’’ theory and treatment. Behaviour
Research and Therapy, 41, 509–528.
First, M. B., Gibbon, M., Spitzer, R. L., & Williams, J. B.
W. (1997). Structured clinical interview for DSM-IV
axis I disorders - patient edition (SCID-I/P, 2/2001
revision). New York, NY: Biometrics Research
Department.
Foa, E. B., Huppert, J. D., Leiberg, S., Langner, R., Kichic,
R., & Hajcak, G., et al. (2002). The obsessive-
complusive inventory: Development and validation
of a short version. Psychological Assessment, 14,
485–495.
Fornari, V., Kaplan, M., Sandberg, D. E., Matthews, M.,
Skolnick, N., & Katz, J. L. (1992). Depressive and
anxiety disorders in anorexia nervosa and bulimia
nervosa. International Journal of Eating Disorders,
12, 21–29.
Godart, N. T., Flament, M. F., Curt, F., Perdereau, F.,
Lang, F., & Venisse, J. L., et al. (2003). Anxiety
disorders in subjects seeking treatment for eating
disorders: A DSM-IV controlled study. Psychiatry
Research, 117, 245–258.
Goldner, E. M., Cockell, S. J., & Srikameswaren, S. (2002).
Perfectionism and eating disorders. In G. L. Flett, & P.
L. Hewitt (Eds.), Perfectionism: Theory, research, and
treatment. Washington, DC: American Psychological
Association, 319–340.
Hajcak, G., Huppert, J. D., Simons, R. F., & Foa, E. B.
(2004). Psychometric properties of the OCI-R in a
college sample. Behaviour Research and Therapy, 42,
115–123.
Halmi, K. A., Sunday, S. R., Klump, K. L., Strober, M.,
Leckman, J. F., & Fichter, M., et al. (2003). Obses-
sions and compulsions in anorexia nervosa subtypes.
International Journal of Eating Disorders, 33, 308–
319.
Hodgson, R. J., & Rachman, S. (1977). Obsessional-com-
pulsive complaints. Behaviour Research and Therapy,
15, 389–395.
Huppert, J. D., Walther, M. R., Hajcak, G., Yadin, E., Foa,
E. B., & Simpson, H., et al. (2007). The OCI-R:
Validation of the subscales in a clinical sample. Journal
of Anxiety Disorders, 21, 394–406.
Jimenez-Murcia, S., Fernandez-Aranda, F., Raich, R. M.,
Alonso, P., Krug, I., & Jaurrieta, N., et al. (2007).
Obsessive-compulsive and eating disorders: Compari-
son of clinical and personality features. Psychiatry and
Clinical Neurosciences, 61, 385–391.
Kano, Y., Ohta, M., Nagai, Y., Pauls, D. L., & Leckman, J.
F. (2004). Obsessive-compulsive symptoms in parents
of Tourette syndrome probands and autism spectrum
disorder probands. Psychiatry and Clinical Neuro-
sciences, 58, 348–352.
Lavender, A., Shubert, I., de Silva, P., & Treasure, J.
(2006). Obsessive-compulsive beliefs and magical
ideation in eating disorders. British Journal of Clinical
Psychology, 45, 331–342.
Li, C-s. R., & Chen, S.-H. (2007). Obsessive-compulsive-
ness and impulsivity in a non-clinical population of
adolescent males and females. Psychiatry Research,
149, 129–138.
Lopez, C., Tchanturia, K., Stahl, D., Happe, F., Booth, R.,
& Holliday, J., et al. (2008). An investigation of
central coherence in women with anorexia nervosa.
International Journal of Eating Disorders, 41, 143–
152.
Mataix-Cols, D., Frost, R. O., Pertusa, A., Clark, L. A.,
Saxena, S., & Leckman, J. F., et al. (2010). Hoarding
disorder: A new diagnosis for DSM-V? Depression and
Anxiety, 27, 556–572.
Eur. Eat. Disorders Rev. 19 (2011) 501–508 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association. 507
M. Roberts et al. Measuring Self-Report Obsessionality in AN

Rastam, M., Gillberg, C., & Wentz, E. (2003). Outcome
of teenage-onset anorexia nervosa in a Swedish
community-based sample. European Child & Adoles-
cent Psychiatry, 12, I78–I90.
Roberts, M. E. (2006). Disordered eating and obsessive-
compulsive symptoms in a sub-clinical student
population. New Zealand Journal of Psychology, 35,
45–54.
Roberts, M. E., & Wilson, M. S. (2008). Factor structure
and response bias of the Obsessive-Compulsive
Inventory-Revised (OCI-R) in a female under-
graduate sample from New Zealand. New Zealand
Journal of Psychology, 37, 2–7.
Salkovskis, P. M. (1999). Understanding and treating
obsessive-compulsive disorder. Behaviour Research
and Therapy, 37, S29–S52.
Schmidt, U., & Treasure, J. (2006). Anorexia nervosa:
Valued and visible. A cognitive-interpersonal main-
tenance model and its implications for research
and practice. British Journal of Clinical Psychology,
45, 343–366.
Sternberger, L. G., & Burns, G. L. (1990). Compulsive
activity checklist and the Maudsley obsessional-
compulsive inventory: Psychometric properties
of two measures of obsessive-compulsive disorder.
Behaviour Research and Therapy, 21, 117–127.
Stice, E., Telch, C. F., & Rizvi, S. L. (2000). Development
and validation of the Eating Disorder Diagnostic Scale:
A brief self-report measure of anorexia, bulimia, and
binge-eating disorder. Psychological Assessment, 12,
123–131.
Thomsen, P. H. (1994). Obsessive-compulsive disorder in
children and adolescents: A 6-22-year follow-up study:
Clinical descriptions of the course and continuity of
obsessive-compulsive symptomatology. European
Child & Adolescent Psychiatry, 3, 82–96.
Zigmond, A. S., & Snaith, R. P. (1983). The hospital
anxiety and depression scale. Acta Psychiatrica Scan-
dinavica, 67, 361–370.
508 Eur. Eat. Disorders Rev. 19 (2011) 501–508 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association.
Measuring Self-Report Obsessionality in AN M. Roberts et al.


















