Measles Eradication: The Role of the Anthropologist...tine measures had been implemented in response...
19
Measles Eradication: The Role of the Anthropologist Item Type Article Authors McCombie, S.C. Publisher University of Arizona, Department of Anthropology Journal Atlatl Download date 18/06/2021 18:20:44 Link to Item http://hdl.handle.net/10150/113404
Transcript of Measles Eradication: The Role of the Anthropologist...tine measures had been implemented in response...
-
Measles Eradication: The Role of the Anthropologist
Item Type Article
Authors McCombie, S.C.
Publisher University of Arizona, Department of Anthropology
Journal Atlatl
Download date 18/06/2021 18:20:44
Link to Item http://hdl.handle.net/10150/113404
http://hdl.handle.net/10150/113404
-
MEASLES ERADICATION:THE ROLE OF THEANTHROPOLOGIST
S.C. McCombie
INTRODUCTION
In the Western response to infectious disease, priorityhas been given to preventive medicine and particularly toimmunizations. The number of available vaccines ismultiplying rapidly, and research directed at developing aneven wider range of prophylactic agents is accelerating.Infectious disease continues to be the most importantpublic health problem in the developing world, and vaccine—preventable disease is a cause of significant mortalityand morbidity in these areas. Because the World HealthOrganization has called for the provision of immunizationsto all of the world's children by 1990, it is likely thatmore anthropologists will be called upon to facilitatecommunity acceptance of such programs. In addition tofunctioning as community mediators, anthropologists haveother responsibilities with respect to immunization theoryand practice. These include evaluating cost analyses,considering the legal and ethical aspects of immunizations,and examing the consequences of changes in epidemiologicalpatterns in an evolutionary framework. It is also impor-tant to study the development of Western disease theory andassociated practices in cultural and historical contexts.
HISTORY OF MEASLES AND VACCINATION
Over time, significant changes in human behavior haveresulted in an increase in exposure to some diseases anddecrease in incidence of others. The abandonment of anomadic hunting and gathering lifestyle put populations inconstant proximity to human wastes and other reservoirs ofdisease. Pastoralism brought humans into close contactwith animals that transmit diseases which can becomeestablished in human populations. The development ofagriculture and subsequent environmental modificationcreated environments suitable for the multiplication ofvarious disease vectors. Finally, urbanization and itsassociated high population density allowed the evolution ofacute infectious diseases that are transmitted by person toperson contact.
Measles belongs to this last category of disease. Theinitial measles attack generally confers a life—longimmunity. Hence, even in a large urban community, epi—
23
-
24
demics have a relatively short lifespan, subsiding as thepopulation of susceptible hosts decreases as a result ofmortality and recovery. Only when new hosts such asinfants and young children are available does the diseasereach epidemic proportions again, attaining the status of a'childhood' disease. However, when these diseases areintroduced into virgin populations, all age groups areaffected and morbidity and mortality increase drastically.
The attempt to trace the history of measles in ancienttimes is plagued by uncertainty, due to the difficulty ofmaking conclusive diagnoses from the varying types ofinformation given in historical texts. Measles was firstdistinguished from smallpox in 860 A.D. by Rhazes, althoughconfusion between these two diseases persisted for cen—tunes. There are numerous reports of devastating epi-demics in the New World during the conquest and colonialperiods. Despite the fact that trans-Atlantic contactbegan relatively recently, the identification of thediseases involved in particular epidemics is frequently asubject of debate. Difficulty in diagnosis sometimesarises from the fact that many infectious diseases showdifferent clinical manifestations when they attack virginpopulations. With measles and smallpox, many individualsdie before the eruption of the characteristic rashes.Measles probably reached the New World in 1531, a decadeafter the arrival of smallpox (Dobyns, 1963:497).
Although the idea of contagion is ancient, and quaran-tine measures had been implemented in response to a numberof epidemic diseases, the germ theory of disease did notgain acceptance in Western medical theory until the late19th century. As early as 1546 Fracastoro gave priority tothe theory of contagion, but the miasmatic theory, whichattributed disease to polluting vapors that arose fromswamps or decaying corpses, continued to prevail (Wain,1970:95, McNeill, 1976:265).
In 1846, Peter Ludwig Panum observed a measles epidemicon the Faroe Islands. The unique circumstances provided byan island population that had been free of the disease for65 years allowed him to make important conclusions aboutthe epidemiology of measles. He determined that theincubation period was 13 or 14 days and that no casesoccurred among those previously exposed. One of his mostimportant conclusions was that measles was a contagious andnot a miasmatic disease. Panum also describes some unsuc-cessful measles inoculation attempts he undertook inEdinburgh (Panum, 1940:94). As early as 1758, Frances Home
-
25
had performed similar experiments with measles inoculationin Scotland (Waterson and Wilkinson, 1978:148).
The history of inoculation lends support to the ideathat medical practice proceeds on an empirical line ofdevelopment distinct from theories of disease. Deliberateexposure as a means of minimizing the mortality of aninfectious disease has a long history. In China, threethousand years ago, an aerosolized smallpox 'vaccine'operated on the same principle as modern immunization. Apowder was prepared from the scabs of an individualrecovering from smallpox and introduced into the nostrilsof a susceptible individual, a process known as varlo—lation. The variolated individual would usually get amilder form of the disease followed by life—long immunity.Unfortunately, these individuals were contagious and couldpass on the disease in its more severe form.
Variolation reached Europe in 1717 when the wife of theBritish ambassador to Turkey returned to England andintroduced the practice. In 1796, Edward Jenner, himselfvariolated at age 8, performed an experiment which is seenas a hallmark in preventive medicine. Using material fromthe hand of a dairymaid infected with cowpox, he inoculateda susceptible young boy. He subsequently variolated theboy, who failed to develop smallpox, thus demonstrating theefficacy of the new technique which came to be calledvaccination. The principles that allowed this technique towork were not understood at the time, although Jenner knewof the folk belief that those who got cowpox wouldn'tget smallpox.
It was almost a century before the bacteriological workof Pasteur and Koch validated the germ theory of disease.Although the immunological principles underlying Jennerianvaccination remained undiscovered at this time, thedemonstrated efficacy of the technique, combined with newknowledge of disease—causing organisms, gave rise to anumber of attempts to develop prophylactic agents for otherdiseases. These attempts sometimes proceeded successfullyin the absence of knowledge of the disease agents them-selves. Pasteur himself developed and administered avaccine for rabies in 1885, in spite of the fact that hewas unable to isolate the infectious agent or grow it invitro. The properties of filterable viruses were notunderstood for many years following successful vaccina-tions. The first virus was grown in tissue culture in1913, and it was not until 1939 that the developmentof the electron microscope allowed these pathogens to bevisualized (Hughes, 1977:77)
-
26
Knowledge about measles virus grew slowly in the firsthalf of the 20th century. The fact that the virus isdifficult to isolate from the infectious host (Fenner andWhite, 1976:394) was probably an important factor in thisslow development. Credit for measles virus isolation hasbeen attributed to Plotz in 1938 (Schmidt, 1959:292) andEnders and Peebles in 1954 (Fraser and Martin, 1978:1).
In current viral taxonomy, measles is assigned to genusfamily Paramyxoviridae. Like other members
uf the Paramyxoviridae; mumps, rinderpest, and distemper,measles is composed of a single strand of RNA. Antigenicand epidemiological characteristics of current measlesstrains have been used in attempts to reconstruct itsorigin. Because of the large population size needed tosustain measles transmission, most authors feel thatmeasles is a relatively recent addition to the humanrepertoire of disease, appearing sometime after theagricultural revolution allowed substantial increases inpopulation size and density. The range of possible earliestdates is extensive, and ranges from 10,000 BP (Cockburn,1971:51) to 4500 BP (Black, 1982:398). Most authors feelthat measles virus arose in the recent past and began withaccidental transmission from the domestic animals that nowexhibit closely related infections. Cockburn (1971:51)feels that canine distemper and rinderpest (cattle) are thelikely culprits. The close morphological and antigenicrelationships between these viruses and measles supportsthis interpretation. However, this evidence is ambiguous,since it also supports the hypothesis that as they becamedomesticated, the animals in question acquired thesediseases from human. An implicit bias toward finding thecause of disease in 'nature' rather than in humans isevident in the philosophy of Western scientists.
CLINICAL ASPECTS OF MEASLES AND MEASLES IMMUNIZATION
Although measles produces highly consistent signs andsymptoms, a number of host factors have been cited ascausing clinical variation. As with most diseases, thedeterminants of clinical variation are not well under-stood. Age is the most important variable, with thehighest fatality ratios and incidence of encephalitis beingseen in infants and adults. Unlike many viral infections,measles has a higher mortality rate in malnourishedpopulations (Fraser and Martin, 1978:3). Mortalityrates as high as have been recorded in West Africa, andthere is evidence that the malnourished host is infectivefor a longer period of time (Morley, 1980:119, 125).
-
27
An attack of measles depresses cellular immunity, andmay activate latent tuberculosis. The virus apparently hasthe ability to remain latent in the body for long periodsof time. In a small number of individuals subacutescierosing panencephalitis (SSPE), a chronic fatal infec-tion of the brain, appears years after the initial infec-tion of measles. Further mystery surrounds the possiblerelationship of measles virus to multiple sclerosis.Elevated measles antibody levels in MS patients wereobserved as early as 1962 (Shelley and Dean, 1981:74) butattempts to associate measles virus with this disease havenot been totally successful. In recent experiments, partsof the measles virus genome have been isolated from onlyone in four MS patients (Haase, et.al., 1981:672). Someresearchers have suggested that MS results from exposure tocanine distemper (Norman, et.al., 1983).
The first measles vaccine to be developed was a killedvaccine, which approximately 800,000 people in the UnitedStates received before 1968 (Fulginitti, 1982:116).Recipients of this vaccine developed a high risk ofsuffering from a severe atypical measles syndrome whenexposed to the natural disease or the live vaccine which isnow in use, because the inactivated vaccine sensitized thehostts immune system so it reacted to the live virus in anunusual manner.
The development and widespread use of an effective livevaccine has resulted in a dramatic decrease in reportedmeasles in the United States. The risk of complicationsfrom the vaccine is estimated to be one case of encepha-litis per 1,000,000 doses versus one per 2,000 cases of thedisease (MMWR, 5/7/82:217,221). Cases of SSPE have alsooccurred after vaccination, but at a lower rate than withnatural disease. It is not clear whether the risk ofcomplication rises with age and poor nutritional status asit does with the actual disease.
Because of the existence of maternal antibodies,problems in establishing immunity in infants have beenencountered. Measles vaccine is now administered at 15months of age in the United States, and individuals whohave been immunized prior to 12 months of age are con-sidered inadequately immunized. However, in the developingworld, the average child acquires measles much earlier, andmany severe infections occur before age one. Because ofthe high mortality due to measles in the developingworld, vaccination must be performed as early as 6 monthsto significantly reduce mortality (Ogunmekan et.al.
-
28
1981:177). When vaccine is administered this early, alarge percentage will fail to develop immunity. Revaccina—tion does not appear to solve this problem, as recentresearch has shown that children vaccinated at 12 months oryounger did not respond well to revaccination, perhapsbecause of some immunological sensitization similarto that encountered with the killed vaccine (Black et.al.,1984).
IMMUNIZATION IN THE DEVELOPING WORLD
The success of the smallpox eradication program has gen-erated additional enthusiasm for vaccination in a medicaltechnology that has already placed an enormous emphasis onthis form of disease control. In the United States,children are routinely immunized against diphtheria,pertussis, tetanus, polio, measles, mumps, and rubella.Additional prophylactics that may be recommended forinternational travel or high risk groups include typhoid,cholera, yellow fever, influenza, tuberculosis, hepatitisB, and plague vaccines. Other vaccines are in use or arein various stages of development, and a number of diseaseshave been suggested as candidates for control by immuniza-tion, including malaria, leprosy, schistosomiasis, herpes,AIDS, and cancer. Immunization is often considered whenother methods fail to control a disease or are too costly.The appearance of malarial vectors that are resistant tovarious insecticides, as well as Plasmodia that are resis-tant to the effects of chloroquine, is well known. Malariais not considered a good candidate for control by immuñiza—tion because it can cause a persistent infection and theparasite changes its antigenic structure fairly rapidly.However, attempts continue to be made, and work on aleprosy vaccine has been accelerated by the fact thatMycobacterium leprae has developed resistance to one of thedrugs that was most effective against it.
Most of the immunization programs in the developingworld have the prevention of disease as their major goal.The rationale for such prevention has humanitarian as wellas practical aspects. High rates of morbidity and mortali-ty from infectious diseases are a significant barrier toeconomic development. Immunizations are considered one ofthe easiest health services to deliver (Creese andHenderson, 1980:494) and a successful program is believedto have a number of economic benefits. The followingquotation illustrates this point of view.
-
29
"It is widely accepted that successful vaccine programs,such as the one which essentially eliminated polio in theU.S.A., resulted in a ratio of $100.00 saving of publictax money per year for every dollar of expense ofdeveloping the vaccine, (i.e., based on estimated cost ofhospitalization and institutional care for persons whowould have otherwise developed polio in the absence ofthe vaccine, and the tax revenue obtained fromindividuals who reach maturity, had gainful employment,and thus became a taxpayer rather than a recipient."
(Friedman, 1978:223)
Immunization programs have also been seen as having animportant role in the acceptance of family planningprograms. A guarantee of better infant survival is seen asa prerequisite for persuading people to have fewer children(World Health Organization, 1975:1).
Scientists interested in genetic variation between humanpopulations have used immunizations to study the biologicalresponse to disease. Debate has centered around thereasons for the high mortality rates in virgin populationsintroduced to epidemic diseases. Some authors havestressed the role of social factors, pointing to the socialdisorganization and breakdown of patient care that occurswhen everyone becomes sick at once. Others feel thatgenetic susceptibilities are responsible for high mortali-ty. A number of researchers have administered measlesvaccine to virgin populations of South American Indiansin order to test these hypotheses (Neel et. al., 1970;Neel, 1982; Black et.al., 1982). Because the vaccine is inwidespread use as a preventive measure, these experimentsare not considered unethical. A small case of measlesgenerally follows the injection, and the clinical andserological responses are recorded and compared to those ofWestern populations. However, this research has not yetresolved the issue of genetic susceptibilities.
Populations outside the developed world have often beeninvolved in vaccine trials. Because new vaccines must betested in the presence of the diseases they are to prevent,endemic areas must be used as test sites. Isolation fromdiseases is another criterion used in selecting a communityas a test population. Some of the island populations inMicronesia have participated in studies to demonstrate thepersistence of measles antibodies over time in the absenceof the disease (Brown et. al., 1965; Brown and Gajdusek,1970).
-
30
A number of epidemiological, geographical, technologi-cal and cultural factors can create difficulties in theadministration of immunization programs in the developingworld. Most vaccines have specific temperature require-ments and lose their potency if subjected to temperaturesthat are either too low or too high. It is difficult tomaintain the cold chain in areas where adequate refrigera-tion is lacking. Nomadic and migratory groups are diff i—cult to locate and immunize adequately, especially whenthey cross national borders. Even in urban areas, identify-ing and locating migrant workers and other temporaryresidents present problems for immunization program staff.
A crucial determinant of the success of an immunizationprogram is community acceptance. If a significantproportion of individuals do not receive immunizations, aprogram will fail regardless of how effectively logisticproblems are handled. This is an area where anthropolo-gists can play an important role. One prerequisite forcommunity acceptance of a preventive health service iseffective communication with the target population. Theselection of appropriate channels of communication musttake into account cultural and socioeconomic factors. InNigeria, a mass media program failed because many womenwere engaged in trading and were not at home when theprograms were scheduled (Odumosu, 1982:108).
Even with adequate communication, immunization rates mayfall below desirable levels because individuals do not wantto be immunized. Mackland and Durand (1976) have produceda profile of the factors relating to inadequate immuniza-tion in the United States. Their profile, based oninterviews with parents, shows that a number of factors arecorrelated with low rates of vaccination. These are: lowperception of disease seriousness, low perception ofindividual risk, inadequate knowledge of efficacy ofvaccine, inadequate knowledge of length of protection,younger ages, lower education, larger families, less mediaexposure, and a greater percentage of non—whites.
In the developing world, studies of the characteristicsof inadequately immunized populations have shown thatMackland's and Durand's profile does not havecross-cultural applicability. In Thamaga, South Africa,education of parents was not related to the child'simmunization status, and lack of understanding of thereasons for immunization was prevalent in both the im-munized and inadequately immunized groups. Many of thosewho had one immunization but failed to return for boostersbelieved that the practice was a ritual that would have
-
31
lasting protective powers against all illness (THin andUlin, 1981). The inability to understand why a healthychild should receive an injection showed a failure todistinguish between preventive and therapeutic healthservices, which is often cited as a factor in low accept-ance of immunization. On the other hand, the successfuluse of penicillin against yaws in New Guinea generatedsupport for a number of other injections (Radford,1980:328). Undoubtedly there have been a number ofinstances around the world in which the belief thatinjections are beneficial facilitated acceptance ofimmunizations. Low immunization rates have also been attri-buted to distrust of free services and the belief that thepractice is dangerous because of the fever and skineruptions that sometimes follow the shots.
The administration of any vaccine involves a small riskof complications. Some vaccines create problems forindividuals with allergies to eggs and other substancesthat may be present in small quantities in the vaccine.Often immunological sensitivities cannot be determinedprior to vaccine administration. The occurrence of anallergic reaction or other vaccine—related complication inone individual in a small community may destroy the entirecommunity's confidence in all immunizations. The determi-nants of participation in an immunization program arecomplex, and vary according to a number of differentsocial, cultural, and historical factors. Methods forgenerating acceptance of immunizations must reflect thenature of these factors in each target population.
In addition to functioning as a troubleshooter concernedwith increasing community participation in an immunizationprogram, the anthropologist has a role to play in programevaluation. Funds for immunization programs are oftenjustified on the basis of cost—benefit andcost—effectiveness analyses. A number of indirect andintangible benefits are quantified in cost-benefit analy-ses. Many factors render such analyses inappropriate incertain situations, for instance the difficulty of quanti-fying intangibles, the complexity and interdependence ofthe variables used, socioeconomic change, and differingepidemiological circumstances (McCarthy, 1979:410). Theremay be problems inherent in the application of cost-benefitanalyses based on Western economic theory to non—Westernsocieties in which values and economic circumstances aremuch different. Cost—effectiveness analyses simply measurethe efficiency of competing programs and are preferred bysome authors (McCarthy, 1979:411). By virtue of theirclose association with the communities involved and their
-
32
understanding of daily activities related to economicproductivity, ethnographers are in a position to evaluatethe use of cost analyses in specific social settings.
For the applied anthropologist who acts as a communityadvocate and is concerned with establishing free choiceand self—direction for the study population, the legal andethical aspects of immunization are important considera-tions. Even in the developed world, there is controversyregarding this aspect of vaccine administration. Questionsrelating to the rights of individuals and the rights andresponsibilities of those implementing immunizationprograms remain unanswered. The widespread use of immuni-zation protects the population but puts a small number ofindividuals at risk for vaccine—caused disease and disabi-lity. Yet, when a significant number of individuals refuseimmunization, the entire population may be susceptible todevastating epidemics that circulate among individuals whohave not been adequately immunized or whose immunity haswaned. Some of the legal and ethical questions that ariseinclude the following: What type of informed consent isnecessary? How are the possible risks to be explained toindividuals with varying educational and medical back-grounds? Should individuals be compensated by society forcomplications caused by the administration of vaccines?Should parents who withhold immunizations from theirchildren be penalized for negligence? There is no consen-sus about how to deal with the legal and ethical questionsraised by vaccine administration.
MEASLES ERADICATION
The global eradication of smallpox graphically illus-trates the power of human practices to affect the evolutionof disease. In this case, the end result was the extinc-tion of the variola virus. Because of the epidemiologicalsimilarities between measles and smallpox, some havesuggested that measles may ultimately face a similarfate. However, most authors agree that the global eli.mina—tion of measles, if it is at all possible, will be muchmore difficult than smallpox eradication because of avery important difference between the two viruses. Measlesis one of the most contagious diseases known and itsintrinsic reproductive rate (Ro) is much higher than thatof smallpox. This means that a much higher level ofimmunity must be attained to break the chain of transmis-sion.
The resilience of this disease is illustrated by thedifficulties encountered in eliminating measles from the
-
33
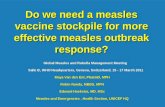
United States in spite of high levels of immunity. InOctober 1978 a goal was set to eliminate indigenousmeasles from the U.S. by October 1, 1982. This goal wasnot attained, and no future target date has been set.
MEASLES INCIDENCE - UNITED STATES
Year Total Indigenous Imported
1978 26,871 N/A N/A1979 13,597 N/A N/A1980 13,506 N/A N/A1981 3,124 N/A N/A1982 1,728 N/A N/A1983 1,436 1,136 3001984 2,534 2,239 295
Source: Morbidity and Mortality Weekly Reports. Atlanta,Georgia, Center for Disease Control.
College campuses are frequently the focal points ofepidemics. Individuals of college age grew up when measlestransmission was decreasing because of use of the vaccine.Consequently their chances of acquiring the disease duringchildhood were low.
The number of people who remain susceptible to measlesinfection is not known. The group includes individuals whowere not immunized because of refusal or medical pro-blems. Immunized individuals may also remain susceptiblebecause of vaccine failure, which can result from improperstorage or administration (i.e., before maternal or otherpassively acquired antibodies have disappeared). Even withproper administration, the overall effectiveness of measlesvaccine is reported at varying rates from 90% (MMWR,12/17/82:659) to 95% (MMWR, 5/7/82:219). Consequent-ly, even with 100% immunization coverage, 5-10% of thepopulation may not be prqtected. Infants are consideredprotected against measles until 6 months of age because ofmaternal antibodies. No one has addressed the issue ofwhat will happen when the vaccine cohort begins reproducing(as it already has) and infants fail to acquire passiveantibodies from their still—susceptible mothers.
In the United States during the first 26 weeks of 1984,51.6% of the individuals who acquired measles had been vac-cinated before the first birthday, which is no longerconsidered adequate. These cases, along with 54 recruits
-
34
at a Naval training station who were considered immunebecause of positive laboratory assays for measles antibody,were classifed as "non—preventable" (MMWR, 9/7/84:504)In spite of this, the Public Health Service's analysis andrecommendations state only that efforts should be directedat increasing immunization coverage.
Controversy is beginning to surface over whether measlescases in vaccinees results from initial vaccine failure orfrom waning immunity (Black, 1982:413). If the vaccinedoes not confer a solid life—long immunity, currentimmunization policies providing a single dose will need tobe altered. Otherwise, when the first generation ofvaccine recipients reaches old age, if measles has not beentotally eradicated, it may emerge as a geriatric disease,where it is likely to be particularly severe.
The question of waning immunity is also important inevaluating the possible epideiniological effects of subclin-ical cases. The fact that the decline in antibody titers isgreater in the absence of epidemic measles illustrates thatsubclinical infections do take place (Fraser and Martin,1978:3). While such infections are not generally con-sidered communicable, research in Nigeria has suggestedthat subclinical infections in adults may be transmitted tosusceptible children (Harry, 1981:172). If this phenomenondoes occur, it can be expected to increase in populationswhere antibody titers are low because of waning artificialimmunity
It is clear that immunization has had an effect on theepidemiology of measles. The disease has 'evolved' in theU.S., where it has been transformed from a common childhoodillness into a disease which causes sporadic epidemicsamong young adults. This is a result of the fact thatvaccination imposes selection pressures on the pathogensthat infect human beings. Disease agents such as measlesvirus, which are viable only in the human organism, areparticularly susceptible to such selective pressures.However, when a disease agent has a high reproductivecapacity, the outcome of selection may not be extinction,but evolution.
A conservative estimate of the rate of spontaneousmutation in viruses is one per 1,000,000 replications.Because replication occurs several million times in asingle host, mutations occur during each episode of a viraldisease, including subclinical infections (Fenner andWhite, 1976:72). Under natural conditions most of themutations that arise have to compete with the established
-
35
form of the disease. Such competition is unsuccessfulunless the variant possesses a selective advantage.When the original form is unable to succeed in establishinginfection in new hosts because of immunity, forms that caninvade and multiply in spite of host defenses will befavored. Mutations that increase a virus' invasiveability, alter its antigenic structure, or suppress immuneresponses may emerge. Optimism about the elimination ofmeasles is based on the assumption that the virus isantigenically stable. However, immunoselection usingmonoclonal antibodies has shown that antigenic variants ofmeasles virus arise spontaneously in the laboratory(Birrer et.al., 1981).
CONCLUSION
A final responsibility of anthropologists involvesinvestigating the customs and practices of our own socie-ty. This field of study has not received the attention itdeserves. We must recognize that modern medicine is acultural system, and as such operates on the sameprinciples as the cultural systems of other societies. Sucha system is associated with a number of customs andpractices that have evolved in response to variousstresses. The form these practices take is determined byhistorical precedent as well as economic and practicalconsideration. A cultural system does not have foresight,and some of its 'adaptive responses' may not be favorablein the long term.
The logical outcome of the widespread use of vaccinationmay be to produce a pathogen that can interfere with thehost's immune response in some manner. The idea of acommunicable disease agent that can literally 'turn off' anindividual's immune system is no longer hypothetical. Sucha disease has already reached alarming proportions in theUnited States, where it has been diagnosed in 8215 peopleand caused 3929 deaths (as of February 4, 1985) . Therecent appearance of this new disease, presently termedAcquired Immune Deficiency Syndrome (AIDS), and the linkingof many viruses to malignancies, suggests that demographictransition theorists need to start over. The battleagainst infectious disease has not been won. In fact, itmay have just begun.
"Infectious disease which antedatedthe emergence of humankind will lastas long as humanity itself, and willsurely remain as it has been
-
hitherto, one of the fundamentalparameters and determinants of humanhistory."
(McNeill, 1976:291)
36
-
37
REFERENCES
Bass, Joh. Hermann1971 History of Medicine. Huntington: Robert
E. Krieger Publishing Company (orig. 1889).
Birrer, Michael J. et.al.1981 "Antigenic Variants of Measles Virus,"
Nature. Vol 293:67—9.
Black, Francis L.1982 "Meales," In Viral Infections of Humans.
Ed. A.S. Evans, New York. Plenum Medical BookCompany, pp. 397-418.
Black, Francis L. et.al.1982b "Genetic Correlates of Enhanced Measles
Susceptibility in Amazon Indians," MedicalAnthropology, Vol. 6, No. 1:37-46.
1984 "Inadequate immunity to measles in childrenvaccinated at an early age: effect ofrevaccination." Bulletin of the World HealthOrganizaiton 62(2) :315—319.
Brown, Paul, et.al.1965 "Response to Live Attenuated Measles Vaccine
in Susceptible Island Populations inMicronesia." American Journal ofEpidemiology. Vol. 28, No.2:115—22.
Brown, Paul, and 0. Carleton Gajdusek.1970 "Disease Patterns and Vaccine Response
Studies in Isolated Micronesian Populations,"American Journal of Tropical Medicine andHygiene. Vol. 19, No. 1:170—5.
Cockburn, T. Aidan1971 "Infectious Diseases in Ancient Populations,"
Current Anthropology. Vol.12, No. 1:45-62.
Creese, A.L., and R.H. Henderson.1980 "Cost—Benefit Analysis and Immunization
Programs in Developing Countries,"Bulletin of the World Health Organization.—Vol. 58, No. 3:491—7.
-
38
Dobyns, Henry F.1963 "An Outline of Andean Epidemic History to
1720." Bulletin of the History of Medicine.—Vol. 36, No. 6:493—515.
Fenner, Frank J. and David 0. White1976 Medical Virology. New York: Academic Press.
Fraser, K.B. and S.J. Martin1978 Measles Virus and its Biology. London:AcademiC
Press.
Friedman, H.1978 "Cholera Vaccines," in New Trends and
ments in Vaccines. Ed. A. Voller andH. Friedman, Baltimore:UniVersity Park Press.
Fuiginitti, Vincent A.,1982 Immunization in Clinical Practice.
Philadelphia: J.B. Lippincott.
Haase, A.T. et.al.1981 "Measles Virus Nucleotide Sequences: Detection
by Hybridization in situ", Science. Vol. 21—2:672—5.
Harry, T.O.1981 "Anti-Measles 1GM in healthy adult Nigerians",
Journal of Tropical Medicine and Hygine.Vol. 84:171—3.
Hughes, Sally Smith1977 The Virus: A History of the Concept.
London: Heinemann Educational Books.
Mackland, Robert E. and Douglas E. Durand1976 "An Investigation of
Factors Affecting Infant Immunization",American Journal of Public Health. Vol. 66,No. 2:168—70.
McCarthy, Neville, J.,1979 "Benefit—Cost and Cost—Effectiveness
Analysis: Theory and Application", ination: Benefit vs. Risk Factors. Basel,Switzerland: S. Karger.
McNeill, William H.1967 Plagues and Peoples. Garden City: Anchor
Press.
-
39
Morbidity and Mortality Weekly Report. U.S. Department ofHHS Atlanta: Center for Disease Control.
Morley, David.1980 "Severe Measles:, in Changing Disease Patterns
and Human Behavior. Ed. N.F. Stanley andR.A. Joske, London: Academic Press.
Neel, James V. et.al.1970 "Notes on the Effect of Measles and Measles
Vaccine in a Virgin—soil population of SouthAmerican Indians", American Journal ofEpidemiology. Vol. 91, No. 4:418-29.
Neel, James V.1982 "Infectious Disease Among Amerindians",
Medical Anthropology. Vol 6, No. 1:47—55.
Norman, James E. Jr. et.al.1983 "Household pets among veterans with multiple
sclerosis and age—matched controls," Archivesof Neurology. Vol. 40, 4:213—4.
Odumosu, Modupe 0.,1982 "Mass Media and Immunization Awareness of
Pregnant Women in a Nigerian Community,"Canadian Journal of Public Health. Vol. 73,No. 2:105—8.
Ogunmekan, D.A. et.al.1981 "A sero-epidemiological study of measles
infection in normal and handicapped persons inLagos, Nigeria," Journal of Tropical Medicineand Hygiene. Vol 84:175-8.
Panum, Peter Ludwig1940 Observations made during the epidemic of
measles on the Faroe Islands in the year1846. New York: F.H.Newton.
Radford, Anthony J.1980 "The Inverse Care Law in Papua New Guinea." in
Changing Disease Patterns and Human Behav4.or.—Ed. N.F. Stanley and R.A. Joske, London:Acade—mic Press.
Schmidt, J.E.1959 Medical Discoveries. Springfield: Charles
C. Thomas, Publisher.
-
40
Shelley, Emer and Geoffrey Dean1981 "Multiple Sclerosis," i.n Western Diseases:—
Their Emergence and Prevention. Ed.H.C. Trowell and D.P. Burkitt, London: EdwardArnold, pp. 71-82.
tJlin, Pricilla R., and Richard 0. Ulin1981 "The Use and Non—use of Preventive Health
Services in a Southern Africa Village."national Journal of Health Education. Vol. 24,No. 1:45—53.
Wain, Harry1970 A History of Preventive Medicine. Springfield:
Charles C. Thomas, Publisher.
Waterson, A.P. and Lise Wilkinson1978 An Introduction to the History of Virology.
Cambridge: Cambridge University Press.
World Health Organization1980 The Global Eradication of Smallpox.
Geneva: World Health Organization.
World Health Organization1975 First WHO Seminar on Expansion of the Use of
Immunization in Developing Countries.Geneva: World Health Organization.