Me Sent Eric Ischemia
39
Acute Mesenteric Ischemia Acute Mesenteric Ischemia Scott Q. Nguyen, M.D. Scott Q. Nguyen, M.D. Celia M. Divino, M.D. Celia M. Divino, M.D. Mount Sinai School of Medicine Mount Sinai School of Medicine Department of Surgery Department of Surgery
-
Upload
igorcotaga -
Category
Documents
-
view
219 -
download
0
description
ccc
Transcript of Me Sent Eric Ischemia

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 1/39
Acute Mesenteric IschemiaAcute Mesenteric Ischemia
Scott Q. Nguyen, M.D.Scott Q. Nguyen, M.D.
Celia M. Divino, M.D.Celia M. Divino, M.D.
Mount Sinai School of MedicineMount Sinai School of MedicineDepartment of SurgeryDepartment of Surgery
7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 2/39
Mrs. MittyMrs. Mitty
• An ! year"old #oman is $rought to the
%& $y am$ulance from her nursing home#' a ( hour history of severe diffuse
a$dominal pain and distention..

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 3/39
)istory
*hat other points of the history doyou #ant to +no#

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 4/39
)istory, Mrs. Mitty)istory, Mrs. Mitty
• Characteri-ation of
symptoms
• emporal se/uence
• Alleviating '
%0acer$ating factors1
• 2ertinent 2M), &3S,
M%DS.
• Associated signs and
symptoms
• &elevant family h0.
Consider the 4ollo#ing

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 5/39
)istory, Mrs. Mitty
• Characteri-ation of Symptoms1Characteri-ation of Symptoms1 Sudden onset diffuse a$dominal pain and distention (
hours ago. 2ain not locali-ed to any /uadrant.
• Alleviating ' %0acer$ating factors1Alleviating ' %0acer$ating factors1 2ain is e0cruciating, it5s the #orse she5s ever e0perienced Nothing alleviates it
• Associated signs'symptoms1Associated signs'symptoms1 She vomits 67 of feculent emesis on arrival to %&. 7ast 8M 9 hours ago, loose

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 6/39
3ther )istory
• 2M)2M) Atrial 4i$rillation " d05d 6 month ago, anticoagulation
contraindicated #ith history of massive :I $leed C)4, CAD, DM
• 2S)2S) Cholecystectomy, left hemicolectomy for diverticular
disease
• M%DS digo0in, metoprolol, insulin

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 7/39
3ther )istory
• Social )istory 3ccasional #ine,
;< pac+"yr smo+er, /uit 9 yrs ago
• 4amily )istory 2atient una$le to give
7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 8/39
*hat is your DifferentialDiagnosis

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 9/39
Differential Diagnosis8ased on )istory and 2resentation
• Small 8o#el 3$struction3$struction
• Acute MesentericAcute MesentericIschemiaIschemia
• 2erforated Diverticulitis2erforated Diverticulitis
• Ischemic ColitisIschemic Colitis
• 2erforated 2eptic =lcer
Disease• Acute 2ancreatitis
• Acute Cholecystitis
• :astroenteritis• Acute Appendicitis

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 10/39
2hysical %0amination
*hat #ould you loo+ for

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 11/39
2hysical %0amination
• >ital Signs1 ? !.;, 2 ? 6<!, 82 ? 6(<';, && ? 9
• Appearance1 thin , in severe distress, legs pulled up to chest,
moaning
• )eart1 irregularly irregular • 7ungs1 mild rales at $ases
• A$domen1 decreased 8S, very distended, mildly tender
diffusely, no guarding're$ound tenderness, no hernias
• &ectal1 loose stool in vault, strea+ed #' fresh $lood
&emaining %0amination findings non"contri$utory

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 12/39
*ould you li+e to revise your
Differential Diagnosis

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 13/39
7a$oratory
*hat #ould you o$tain

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 14/39
• 74s " *N7
• Amylase'7ipase " @'@;" @'@;
• 2'2 " 6!.<'!!.<2'2 " 6!.<'!!.<
• A8: " .!6'!<'B@'6B" .!6'!<'B@'6B
• 7actate .@.@
6!! 6<6
(.@ 6@
6(
(9
(<;!<
6.9
6 9(<
7a$s ordered, Mrs. Mitty
; 2MN5s 99 8ands

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 15/39
7a$ &esults, Discussion
• 7eu+ocytosis "" acute processacute process,, possi$ly infectious possi$ly infectious
• %lectrolytes " elevated 8=N indicating dehydration or" elevated 8=N indicating dehydration or
!rd spacing.!rd spacing.
• Anion gap acidosis " intravascular depletion," intravascular depletion,
Meta$olic acidosis lactic acidosisMeta$olic acidosis lactic acidosis
• Coags Ea$normal coags may reflect sepsis. 2t. not onCoags Ea$normal coags may reflect sepsis. 2t. not on
anticoagulation for Afi$.anticoagulation for Afi$.• Normal 74s' pancreatic en-ymes " no signs of" no signs of
hepatic'pancreatic insulthepatic'pancreatic insult

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 16/39
Interventions at this point

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 17/39
Consider the follo#ing Interventions
• Admit to the hospital'IC=
• Aggressive resuscitation
• Start I> #ith isotonic crystalloid solution NS or 7&
• Insert 4oley catheter
•Monitor response to resuscitation
• Administer $road spectrum anti$iotics
• 7i+ely intra"a$dominal septic process

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 18/39
Studies
*hat further studies #ould you #antat this time

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 19/39
Studies, Mrs. Mitty
• A$dominal F"rays
• 4lat ' =pright4lat ' =pright
• Acute A$dominal Series may include chest at someAcute A$dominal Series may include chest at some
institutionsinstitutions

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 20/39

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 21/39
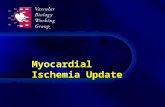
Studies E &esults
• 2lain a$dominal films
Diffuse dilation of small $o#el #' air fluidlevels on upright vie#. Some air in 7eft
colon and &ectum. N3 free air

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 22/39
*hat is the differential
diagnosis at this point

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 23/39
&evised Differential Diagnosis
6 Acute Mesenteric Ischemia
99 Strangulated small $o#el o$structionStrangulated small $o#el o$struction!! Diverticulitis #' contained perforationDiverticulitis #' contained perforation

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 24/39
*hat ne0t

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 25/39
*hat ne0t
• Mesenteric Angiogram or C
Angiogram

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 26/39
Discussion
• *ith the sudden onset of symptoms, h'o Afi$,and Gpain out of proportion to physical e0am,Hacute mesenteric ischemia should $e high on
the Differential Diagnosis• A mesenteric angiogram #ill allo#
visuali-ation of the visceral vessels celiac,
SMA, IMA

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 27/39
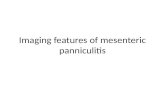
Mesenteric AngiogramMesenteric Angiogram
Note complete lac+ of contrast in mesenteric vessels in A2 vie# left. he
occluded origins of the celiac a0is and superior mesenteric artery are demonstrated
in the 7ateral vie# right.
7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 28/39
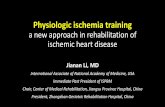
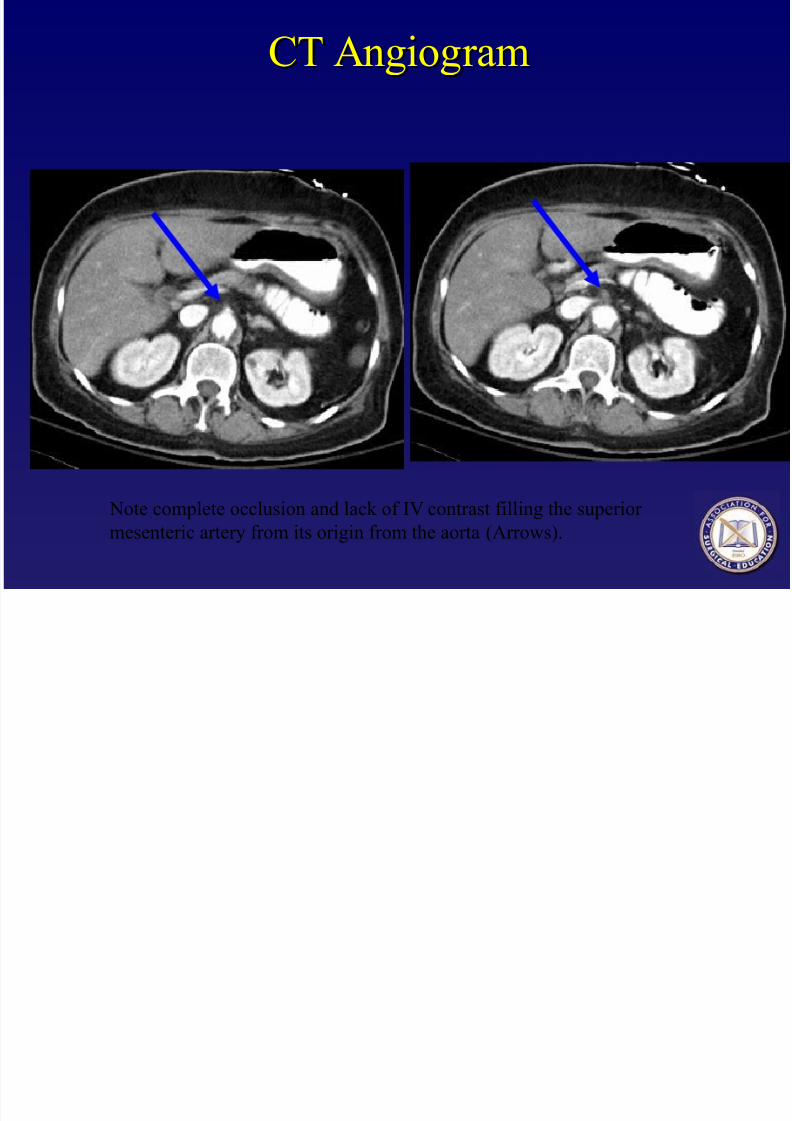
C AngiogramC Angiogram
Note complete occlusion and lac+ of I> contrast filling the superior
mesenteric artery from its origin from the aorta Arro#s.

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 29/39
3ther studies
C angiogram ' M& angiogram
• sensitivity ;, specificity 6<< for em$oli
• additionally can detect thic+ened, distended
$o#el loops
• more sensitive for Mesenteric >enous
hrom$osis

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 30/39
Management
*hat should $e done ne0t

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 31/39
Management
• 2re"operative preparation2re"operative preparation• Assure ade/uate resuscitationAssure ade/uate resuscitation
• MonitoringMonitoring
• 4oley Catheter 4oley Catheter
• =rgent e0ploration=rgent e0ploration
• Surgical em$olectomySurgical em$olectomy
• Assess $o#el via$ilityAssess $o#el via$ility

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 32/39
Management
• 2re"operative preparation• Assure ade/uate resuscitationAssure ade/uate resuscitation
• MonitoringMonitoring• Non"invasive1 %J:, 82, 2ulse 30imetry, foley catheter Non"invasive1 %J:, 82, 2ulse 30imetry, foley catheter
• Consider invasive monitoring1 Central venous catheter, 2AConsider invasive monitoring1 Central venous catheter, 2ACatheter Arterial lineCatheter Arterial line
• 3perative echni/ue' =rgent e0ploration• Midline 7aparotomyMidline 7aparotomy
• &elevant Anatomy&elevant Anatomy• Surgical %m$olectomySurgical %m$olectomy
• Assess $o#el via$ilityAssess $o#el via$ility

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 33/39
Surgical %m$olectomySurgical %m$olectomy
• 2ac+ $o#el to &ight, %0pose2ac+ $o#el to &ight, %0pose
SMASMA
• ArteriotomyArteriotomy
• 2ass $alloon em$olectomy2ass $alloon em$olectomy
catheter catheter
• Assess $o#el via$ilityAssess $o#el via$ility
• &esect if necessary&esect if necessary
Necrotic $o#el from
mesenteric ischemia.

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 34/39
Discussion
Acute mesenteric ischemia is a vascular emergency #ith overall mortality B<"<. here are four main pathophysiologic processes #hich have the samecommon endpoint, $o#el necrosis, a$dominal sepsis, and death. Mesentericarterial anatomy is nota$le for rich collateral flo# $et#een the celiac trun+,superior mesenteric artery, and inferior mesenteric artery. :radual occlusion of9 of the ! vessels is tolera$le as rich collateral $ranches form $et#een these.
Acute occlusion of any of the vessels or their $ranches causes acute intestinalischemia and necrosis..

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 35/39
Discussion
The four processes:
1) Acute arterial embolus -usually from cardiogenic embolusin pts w/ Afib or valvular disorders. !A is the commonvessel affected as it has a less acute ta"e off from aorta
#) Acute arterial thrombosis - chronic atherosclerotic pla$ueat origin of vessel acutely thromboses
%) &hronic mesenteric ischemia - atherosclerosis of visceralvessels results in abdominal pain 'intestinal angina)during times of increased blood demand 'digestion)
() Acute venous occlusion - venous thrombosis causes
cessation of venous outflow from intestines *on-occlusive mesenteric ischemia can also be seen in low-flow states
Di iDi i

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 36/39
DiscussionDiscussion
DiagnosisDiagnosis -- re/uires high degree of suspicion. Classically presents asre/uires high degree of suspicion. Classically presents asGpain out of proportion to physical e0amH or severe pain #'o peritonealGpain out of proportion to physical e0amH or severe pain #'o peritoneal
signs. he history of Cardiac disease, valvular disease, or Afi$ shouldsigns. he history of Cardiac disease, valvular disease, or Afi$ should
alert one to an em$olic disease. :old standard for diagnosis is mesentericalert one to an em$olic disease. :old standard for diagnosis is mesenteric
angiogram, $ut C angiogram is more and more $eing used.angiogram, $ut C angiogram is more and more $eing used.
TreatmentTreatment "" re/uires aggressive resuscitation and hemodynamicre/uires aggressive resuscitation and hemodynamic
monitoring as patients $ecome critically ill very /uic+ly. =rgent surgerymonitoring as patients $ecome critically ill very /uic+ly. =rgent surgery
#' viseral revasculari-ation em$olectomy, throm$ectomy,#' viseral revasculari-ation em$olectomy, throm$ectomy,
endarterectomy, or $ypass is re/uired. After this, evaluation of via$ilityendarterectomy, or $ypass is re/uired. After this, evaluation of via$ility
of $o#el segments should $e performed #ith resection of any necroticof $o#el segments should $e performed #ith resection of any necrotic portions. portions.

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 37/39
Q=%SI3NS
7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 38/39
&eferences
• o#nsend CM. Sa$iston e0t$oo+ of Surgery.o#nsend CM. Sa$iston e0t$oo+ of Surgery.6th %dition6th %dition
• Cameron K7. Current Surgical herapy. thCameron K7. Current Surgical herapy. th
%dition%dition
• 3lden$urg et al. Acute Mesenteric Ischemia.3lden$urg et al. Acute Mesenteric Ischemia.
Arch Intern Med 6B(16<;("B9. 9<<(Arch Intern Med 6B(16<;("B9. 9<<(

7/21/2019 Me Sent Eric Ischemia
http://slidepdf.com/reader/full/me-sent-eric-ischemia 39/39
Ac"nowledgment
The preceding educational materials were made available through the
A+&,AT,+* + 0,&A 2D&AT,+*A+&,AT,+* + 0,&A 2D&AT,+*
In order to improve our educational materials wewelcome your comments/ suggestions at: