McCallum Lecture for FOM Annual Scientific Meeting at ... · McCallum Lecture for FOM Annual...
38
McCallum Lecture for FOM Annual Scientific Meeting at Royal College of Physicians 28 th May, 2014 "Observation and Experiment : an appreciation of Bradford Hill" Professor Sir Anthony Newman Taylor CBE, FRCP, FFOM, FMedSci Imperial College London 1
-
Upload
duonghuong -
Category
Documents
-
view
213 -
download
0
Transcript of McCallum Lecture for FOM Annual Scientific Meeting at ... · McCallum Lecture for FOM Annual...

McCallum Lecture for FOM Annual Scientific Meeting
at Royal College of Physicians
28th May, 2014
"Observation and Experiment : an appreciation of Bradford Hill"
Professor Sir Anthony Newman Taylor CBE, FRCP, FFOM, FMedSci
Imperial College London
1

3

1950
Bradford Hill
TB is curable
Lung cancer is preventable
4

5

After being bedbound for nearly two years
and having an artificial pneumothorax, a lung
abscess and two years of convalescence, I
emerged to complete (at this time of writing)
nearly 66 years of (officially) 100% disability.
from A. Bradford Hill
in ‘A pilot in the First World War’
BMJ 1983;287:1947-1949
6

7
Bradford Hill
Pre 1950
Increased death rates recorded in 1910-1943 from cancer
of lung (5x) and skin (25x) in chemical factory workers
exposed to inorganic As compounds.
Increased death rates from cancer of lung (5x) and nasal
sinuses (150x) in nickel refinery workers in S. Wales
employed before 1923.
1937 Principles of Medical Statistics. Initially series of
articles in Lancet. Subsequently published as book. 11th
edition in 1984

Fig 1 Hospital for Consumption and Diseases of the Chest, Brompton.
Green M BMJ 2011;343:bmj.d7505
©2011 by British Medical Journal Publishing Group

The role of the physician is to
amuse his patients, while nature
takes its course
Voltaire

Cod liver oil and tuberculosis
Standard treatment Standard treatment
plus cod liver oil
Number of patients 542 535
Improved 60.8% 63.1%
Arrested 5.6% 18.1%
Deteriorated or died 33.3% 18.8%
From First Medical Report of the Hospital for
Consumption and Diseases of the Chest, Brompton 1848
10

11
0
1000
2000
3000
4000
5000
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80
Deaths from TB in England and Wales, 1930
Number
of deaths
Age (yrs)
Cause of largest number
of deaths ages 10 to 45yrs

MRC Streptomycin trial
Ethical considerations
Only small amounts of Streptomycin available at time
in UK (foreign exchange not available to buy more)
Ethical use of limited supplies
(1) Miliary and meningeal TB (otherwise invariably fatal)
(2) What remained sufficient for only small proportion of
cases of TB, “it would have been unethical not to have
seized the opportunity to design a strictly controlled
trial which could speedily and effectively reveal the
value of treatment”. Hill A. B.
12

13
Clinical trial
“To one group is given that treatment
from one group it is witheld”
A. Bradford Hill

MRC Streptomycin in Pulm TB trial
Patients Patients with “acute progressive bilateral
pulmonary tuberculosis, of presumably
recent origin, bacteriologically proved,
unsuitable for collapse therapy, age group
15-25 (later extended to 30)
Intervention Streptomycin
Control Bed rest
Outcome Improvement on CXR
Reduction in mortality rate
Time 6 months
(later extended to 3 years)
14

R.C.T. Streptomycin in pulmonary TB
6 months
n Considerable Death
improvement
Bed rest 52 4 14
Bed rest +
Sm 4 hrly 55 27 4
15
MRC, 1948

MRC Streptomycin trial
Landmarks
1. Random (concealed) allocation
2. Strict criteria for patient selection into trial
3. Events recorded unbiased by knowledge of treatment received:
(1) Counting as end points only in indisputable events e.g. death
(2) Blinding investigator and patient to patients‟ treatment allocation
(3) Events requiring subjective judgement (e.g. CXR change)
determined by person ignorant of patients‟ treatment allocation
4. Ethical considerations
16

Bias in Treatment Effects in Controlled Trials
Peto – non randomised trials exaggerate treatment benefit by 30%
Methodological issue Exaggeration of odds ratio (%)
Concealment of treatment
allocation:
Inadequate 40%
Unclear 30%
Trial not double blind 17%
After Saluz et al, 1995
17

R.C.T. Streptomycin in pulmonary TB
n Deaths from TB
6mths 3yrs
Bed rest 52 14 32
Bed rest +
Sm 4 hrly 55 4 35
From Florey, 1961
18

19
RCT‟s Streptomycin v Streptomycin + PAS in pulmonary TB
6 months 3 years
Treatment n Deaths Streptomycin Alive
resistance
†Streptomycin 55 4 33/49 (67%) 40%
*Streptomycin 53 1 5/48 (10.4%) 80%
+ PAS
† MRC, 1948
*MRC, 1950
20
0
1000
2000
3000
4000
5000
6000
1921 1925 1930 1935 1940 1945
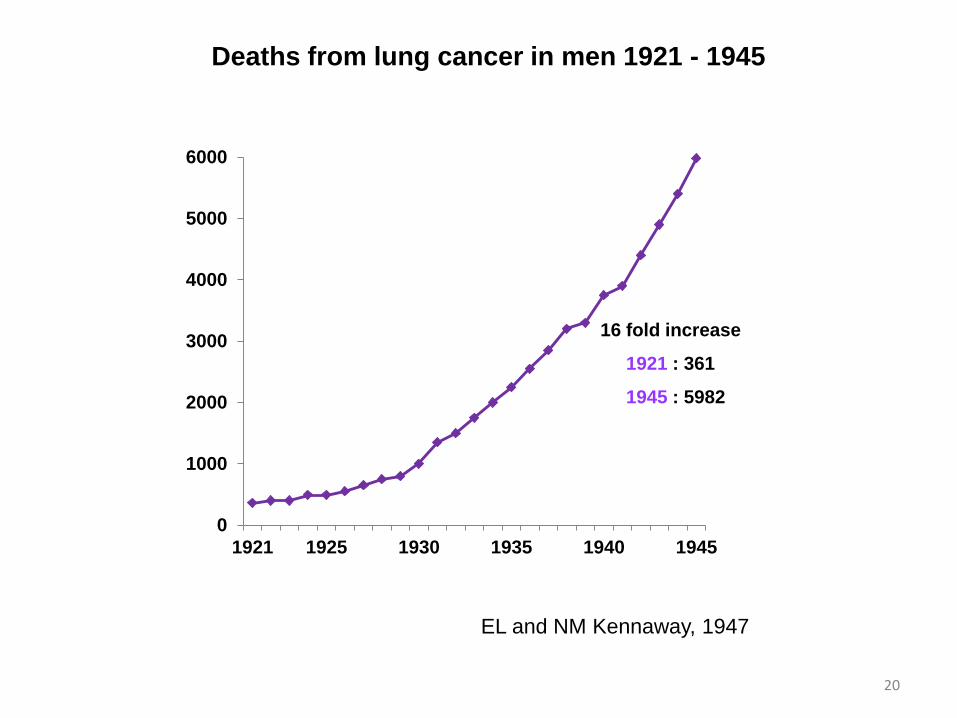
Deaths from lung cancer in men 1921 - 1945
16 fold increase
1921 : 361
1945 : 5982
EL and NM Kennaway, 1947

Aetiology of lung cancer
Knowledge before 1950
Lung cancer incidence in the UK :
Progressive increase since World War I
Men >> Women
Towns > Country
Putative causes :
Cars Exhaust fumes
Tar on roads
Cigarettes
21

You ask me what is needed to
win this war. I answer tobacco,
as much as bullets. We must
have thousands of tons of it
without delay.
General Pershing, 1917
22

23
Retrospective study
Patients with lung cancer (cases) questioned about
previous smoking habits.
Smoking histories in cases compared with smoking
histories in patients without lung cancer (controls)

Case control study of lung cancer in cigarette smokers
Cigarette Lung cancer
smoking Cases Controls Total
+ 1350 1296 2646
- 7 61 68
Odds ratio = 9
After Doll and Bradford Hill, 1952 24
0
50
100
150
200
250
Non-smoker 1-14g 15-24g >25g
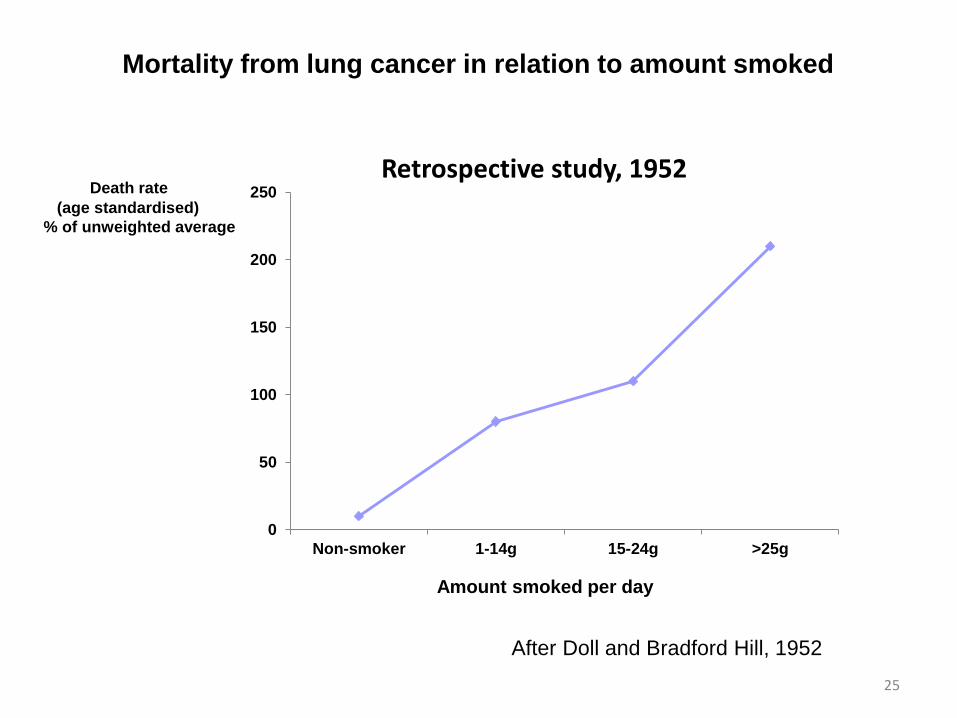
Retrospective study, 1952
Amount smoked per day
Death rate
(age standardised)
% of unweighted average
Mortality from lung cancer in relation to amount smoked
After Doll and Bradford Hill, 1952
25

26
“to determine the frequency with which the disease
lung cancer appeared in the future among groups
whose smoking habits were already known”
Bradford Hill
Doctors in UK on medical register
Willing to report smoking accurately
Easy to follow up because of need to remain on medical register
Usable replies from ⅔
20 years later : Peto + Doll able to determine vital status of 99.7%
Prospective study

0
20
40
60
80
100
120
140
160
180
200
Non-smoker 1-14g 15-24g >25g
Prospective study, 1954
Amount smoked per day
Death rate
(age standardised)
% of unweighted average
Mortality from lung cancer in relation to amount smoked
After Doll and Bradford Hill, 1954
27

0
50
100
150
200
250
Non-smoker 1-14g 15-24g >25g
Retrospective study, 1952 Prospective study, 1954
Amount smoked per day
Death rate
(age standardised)
% of unweighted average
Mortality from lung cancer in relation to amount smoked
After Doll and Bradford Hill, 1952, 1954
28

British doctors (40,000) 10 years on
0
1
2
3
4
5
6
7
8
9
10
All causes Coronary heartdisease
Lung cancer Chronicbronchitis
Non smokers
Cigarette smokers
Cigarette smokers >25g/day
Death
per 105 yr
Cause of death
After Doll and Bradford Hill, 1964 29
Standardised death rate / 100,000

30
Death rate from lung cancer
0
0.5
1
1.5
2
2.5
3
3.5
5 10 15 20 25 30 35 40 45
Death rate from lung cancer
Average No of cigarettes smoked daily
Annual
death rate/1000 men
Doll and Bradford Hill, 1964

31
Death rate from lung cancer
0
0.5
1
1.5
0 5 10 15 20 25 30
Death rate from lung cancer
Annual
death rate/1000 men
Years stopped smoking
Corresponding rate for non-smokers = 0.07/103 men
Doll and Bradford Hill, 1964
„Expected results‟ from retrospective study
Higher mortality in :
(1) Smokers than non-smokers
(2) Heavy smokers than light smokers
(3) Cigarette smokers than pipe smokers
(4) Those who continued to smoke than in those who gave it up
In each case “expected result has
appeared in this prospective study”
Doll R and Hill AB, 1956
32

0
20
40
60
80
100
0 40 50 60 70 75 80 85 90 95 100
Age (years)
0
20
40
60
80
100
0
20
40
60
80
100
57
85
58
80
58
75
Non-smokers
Cigarette smokers
After Doll et al, 2004
UK male doctors : Survival from age 35 years
Doctors
Born
1900 - 1909
Doctors
Born
1910 - 1919
Doctors
Born
1920 - 1929

34
UK cigarette consumption, 1890-2008
0
2
4
6
8
10
1900 1920 1940
Cigarettes per day
(per adult aged 15+)
1950 1960 1980 2000
10
8
6
4
2
0

35
Excess mortality attributable to smoking in India
Respiratory disease ⅓
(chiefly TB RR4.5)
Vascular disease ⅓
„Smoking is a cause and an important cause of death from tuberculosis‟. Gajalakshmi V, Peto R et al, 2003
„Smoking is a factor and an important factor in the production of carcinoma of the lung‟.
Doll and Bradford Hill, 1950

Environment and disease : association or causation?
1. Strength Relative risk
2. Consistency Similar results from different studies
3. Biological gradient Risk increases with increasing exposure
4. Time relationship Exposure always precedes the
outcome
5. Specificity Association limited to specific disease
6. Biological plausibility Depends on biological knowledge of the day
(e.g. John Snow and cholera)
7. Experiment Risk reduces with reducing exposure
8. Coherence Does it all hang together
9. Reasoning by analogy e.g. Effects of drugs + viruses on developing foetus
following rubella and thalidomide
Is there any other way of explaining the set of facts before us, is there any other answer more likely than cause and effect?
Bradford Hill, 1965 36

Bradford Hill : Influence on Medical Science
Lancet articles on medical statistics Principles of Medical Statistics
Development of epidemiological methods to investigate
causes of non-infectious disease with guidelines for
deciding whether observed association is causal
Introduction of randomisation for conduct of clinical trials
„The greatest medical statistician of the 20th century
despite
the fact held no degree in either medicine or statistics‟
Doll R, 1992
37

38
End