Maximum tolerable doses of intravenous zidovudine in combination ...
7
Annals of Oncology 8: 539-545, 1997. © 1997 Kluwer Academic Publishers. Printed in the Netherlands. Original article Maximum tolerable doses of intravenous zidovudine in combination with 5-fluorouracil and leucovorin in metastatic colorectal cancer patients Clinical evidence of significant antitumor activity and enhancement of zidovudine-induced DNA single strand breaks in peripheral nuclear blood cells A. Falcone, 1 M. Lencioni, 1 I. Brunetti, 1 E. Pfanner, 1 G. Allegrini, 1 A. Antonuzzo, 1 M. Andreuccetti, 2 G. Malvaldi, 2 R. Danesi, 3 M. Del Tacca 4 & P. F. Conte 1 l U.O. Oncologia Medica, Ospedale S. Chiara, 2 Dipartimento di Biomedicina, Sezione di Patologia Generate, Universita di Pisa, 3 Scuola Supenore di Sludi Universitan e di Perfezwnamenlo S Anna; 4 Istituto Farmacologia Medica, Universita di Pisa, Pisa, Italy Summary Background: Experimental studies have demonstrated that 5-fluorouracil (5-FU) enhances zidovudine (AZT)-induced DNA strand breaks and cytotoxicity. Phase I studies have demonstrated that the maximum tolerable dose (MTD) of AZT is 8000 mg/sqm when administered i.v. over two hours after weekly 5-FU + 1-leucovorin (LV), and that this combina- tion has promising antitumor activity. The purpose of this study was therefore to evaluate the antitumor activity of weekly bolus 5-FU + LV + AZT, administered at its MTD, and to determine whether 5-FU enhances AZT-induced DNA strand breaks in blood nuclear cells. Patients and methods: Twenty-nine chemotherapy-naive metastatic colorectal cancer patients with measurable disease entered the study to evaluate the activity of a weekly 5-FU 500 mg/m 2 i.v. bolus + LV 250 mg/m 2 i.v. two-hour infusion + AZT 8000 mg/m 2 i.v. two-hour infusion. In 10 different patients, who during three different weeks received 5-FU + LV, AZT and 5-FU + LV + AZT, DNA strand breaks in blood nuclear cells were determined by a fluorescent analysis of DNA unwinding. Results: Treatment was generally well tolerated and WHO grades III— IV toxicities, consisting mostly of diarrhea (17%), were uncommon. One patient died of severe diarrhea with consequent hypokalemia and cardiac arrhythmia. All patients were considered evaluable for response, and 3 (10%) complete and 10 (35%) partial responses were observed, for an objective response rate of 45% (95% confidence limit interval 26%- 64%). Both 5-FU + LV and AZT decreased the percentage of double stranded DNA in nuclear blood cells. The greatest effect was observed with 5-FU + LV + AZT, which reduced the percentage of double stranded DNA to 50% and 36% after 24 and 48 hours, respectively, and this interaction between 5-FU + LV and AZT was found to be cumulative. Conclusions: These studies demonstrate that the present dose and schedule of AZT in combination with 5-FU + LV has significant activity in metastatic colorectal cancer and that the combination of 5-FU + LV with AZT increases the amount of DNA damage. Therefore, AZT in combination with 5-FU + LV warrants further study in colorectal cancer. Key words: AZT, DNA, fluorouracil, phase II, strand breaks, zidovudine Introduction Zidovudine (AZT) is a toxic thymidine analogue which was mainly developed as an antiretroviral agent and has shown significant activity in vitro against the human immunodeficency virus-1 (HIV-1) and clinical utility in patients with AIDS and AIDS-related diseases [1-3]. AZT is phosphorylated intracellularly by thymidine kinase (TK) and can be ultimately incorporated into DNA as AZT triphosphate (AZTTP) where it blocks chain elongation [2]. AZTTP is a more favourable sub- strate for HIV reverse transcriptase than for human DNA polymerase and is, therefore, more efficiently in- corporated into viral than into cellular DNA, resulting in important anti-HIV activity and negligible cytotoxic- ity [1, 2, 4]. More recently, several experimental studies by our group as well as others have demonstrated that AZT incorporation into DNA, AZT-induced DNA strand breaks and AZT cytotoxicity in cancer cells can be markedly enhanced when AZT is combined with agents that inhibit de novo thymidylate (dTMP) syn- thesis, such as 5-fluorouracil (5-FU), methotrexate (MTX), hydroxyurea and ZD1694 [5-12]. In fact, these agents, by depleting intracellular thymidine triphos- phate (dTTP) pools, facilitate the utilisation of AZTTP in DNA synthesis [7, 8, 13]. We have also demonstrated that this effect is evident also in vivo in nude mice bearing xenografts of the human colorectal cancer cell line HCT-8 [7]. These studies also demonstrated that the enhancement of AZT incorporation into DNA was relatively specific for cancer cells and that this reflects biochemical differences between 'normal'and neoplastic cells with regard to thymidine salvage capacity and transport [7, 14-21], Downloaded from https://academic.oup.com/annonc/article-abstract/8/6/539/197888 by guest on 02 April 2018
-
Upload
truongxuyen -
Category
Documents
-
view
216 -
download
0
Transcript of Maximum tolerable doses of intravenous zidovudine in combination ...

Annals of Oncology 8: 539-545, 1997.© 1997 Kluwer Academic Publishers. Printed in the Netherlands.
Original article
Maximum tolerable doses of intravenous zidovudine in combination with5-fluorouracil and leucovorin in metastatic colorectal cancer patientsClinical evidence of significant antitumor activity and enhancement of zidovudine-inducedDNA single strand breaks in peripheral nuclear blood cells
A. Falcone,1 M. Lencioni,1 I. Brunetti,1 E. Pfanner,1 G. Allegrini,1 A. Antonuzzo,1
M. Andreuccetti,2 G. Malvaldi,2 R. Danesi,3 M. Del Tacca4 & P. F. Conte1
lU.O. Oncologia Medica, Ospedale S. Chiara, 2Dipartimento di Biomedicina, Sezione di Patologia Generate, Universita di Pisa, 3Scuola Supenoredi Sludi Universitan e di Perfezwnamenlo S Anna; 4Istituto Farmacologia Medica, Universita di Pisa, Pisa, Italy
Summary
Background: Experimental studies have demonstrated that5-fluorouracil (5-FU) enhances zidovudine (AZT)-inducedDNA strand breaks and cytotoxicity. Phase I studies havedemonstrated that the maximum tolerable dose (MTD) ofAZT is 8000 mg/sqm when administered i.v. over two hoursafter weekly 5-FU + 1-leucovorin (LV), and that this combina-tion has promising antitumor activity. The purpose of thisstudy was therefore to evaluate the antitumor activity ofweekly bolus 5-FU + LV + AZT, administered at its MTD,and to determine whether 5-FU enhances AZT-induced DNAstrand breaks in blood nuclear cells.
Patients and methods: Twenty-nine chemotherapy-naivemetastatic colorectal cancer patients with measurable diseaseentered the study to evaluate the activity of a weekly 5-FU 500mg/m2 i.v. bolus + LV 250 mg/m2 i.v. two-hour infusion +AZT 8000 mg/m2 i.v. two-hour infusion. In 10 differentpatients, who during three different weeks received 5-FU +LV, AZT and 5-FU + LV + AZT, DNA strand breaks in bloodnuclear cells were determined by a fluorescent analysis ofDNA unwinding.
Results: Treatment was generally well tolerated and WHOgrades III—IV toxicities, consisting mostly of diarrhea (17%),were uncommon. One patient died of severe diarrhea withconsequent hypokalemia and cardiac arrhythmia. All patientswere considered evaluable for response, and 3 (10%) completeand 10 (35%) partial responses were observed, for an objectiveresponse rate of 45% (95% confidence limit interval 26%-64%). Both 5-FU + LV and AZT decreased the percentage ofdouble stranded DNA in nuclear blood cells. The greatesteffect was observed with 5-FU + LV + AZT, which reducedthe percentage of double stranded DNA to 50% and 36% after24 and 48 hours, respectively, and this interaction between5-FU + LV and AZT was found to be cumulative.
Conclusions: These studies demonstrate that the presentdose and schedule of AZT in combination with 5-FU + LVhas significant activity in metastatic colorectal cancer and thatthe combination of 5-FU + LV with AZT increases theamount of DNA damage. Therefore, AZT in combinationwith 5-FU + LV warrants further study in colorectal cancer.
Key words: AZT, DNA, fluorouracil, phase II, strand breaks,zidovudine
Introduction
Zidovudine (AZT) is a toxic thymidine analogue whichwas mainly developed as an antiretroviral agent and hasshown significant activity in vitro against the humanimmunodeficency virus-1 (HIV-1) and clinical utility inpatients with AIDS and AIDS-related diseases [1-3].AZT is phosphorylated intracellularly by thymidinekinase (TK) and can be ultimately incorporated intoDNA as AZT triphosphate (AZTTP) where it blockschain elongation [2]. AZTTP is a more favourable sub-strate for HIV reverse transcriptase than for humanDNA polymerase and is, therefore, more efficiently in-corporated into viral than into cellular DNA, resultingin important anti-HIV activity and negligible cytotoxic-ity [1, 2, 4]. More recently, several experimental studiesby our group as well as others have demonstrated that
AZT incorporation into DNA, AZT-induced DNAstrand breaks and AZT cytotoxicity in cancer cells canbe markedly enhanced when AZT is combined withagents that inhibit de novo thymidylate (dTMP) syn-thesis, such as 5-fluorouracil (5-FU), methotrexate(MTX), hydroxyurea and ZD1694 [5-12]. In fact, theseagents, by depleting intracellular thymidine triphos-phate (dTTP) pools, facilitate the utilisation of AZTTPin DNA synthesis [7, 8, 13]. We have also demonstratedthat this effect is evident also in vivo in nude micebearing xenografts of the human colorectal cancer cellline HCT-8 [7]. These studies also demonstrated that theenhancement of AZT incorporation into DNA wasrelatively specific for cancer cells and that this reflectsbiochemical differences between 'normal'and neoplasticcells with regard to thymidine salvage capacity andtransport [7, 14-21],
Downloaded from https://academic.oup.com/annonc/article-abstract/8/6/539/197888by gueston 02 April 2018

540
On the basis of these preclinical observations, werecently conducted a phase I study with intravenousAZT in combination with weekly 5-FU 500 mg/m2 andthe 1-isomer form of leucovorin (LV) 250 mg/m2 inchemotherapy-naive metastatic colorectal cancer pa-tients [22]. In this trial, in contrast to previous studies, ashort intravenous infusion of AZT was used to reachpeak plasma levels similar to those previously found tobe effective in experimental murine models [7, 8]. Resultsdemonstrated that AZT doses ^ 6 g/m2 i.v. over 90-120 minutes were able to produce peak plasma concen-trations (Cmax) and area under the concentration/timecurve (AUC) values similar to those previously demon-strated to be effective in murine tumor models andthat the maximum tolerable AZT dose (MTD) was 8 g/m2,with hypotension being its dose-limiting toxicity.Furthermore, this combination with 5-FU + LV + AZTdemonstrated promising activity, with an objective re-sponse rate of 44% (95% confidence interval 27% to62%) and with a trend toward an increased responserate with higher AZT doses.
The aim of the present phase II study was, therefore,to determine the activity of weekly 5-FU + LV + AZTwith AZT given at its MTD of 8 g/m2 in previouslyuntreated metastatic colorectal cancer patients. Further-more, a second objective was to elucidate the biologicalinteraction between 5-FU and AZT in humans and, inparticular, to investigate if the enhancement of AZT-induced DNA strand breaks by 5-FU, previously dem-onstrated in preclinical experimental models [5], couldbe confirmed also clinically in peripheral nuclear bloodcells of metastatic colorectal cancer patients.
Patients and methods
Drugs and chemicals
AZT (Retrovir) was generously provided by Glaxo-Wellcome (Becke-nam, UK) in 200 mg vials. All chemicals were obtained from SigmaChemical Co. (St. Louis, MO, USA).
Patient selection
Different patients were accrued to determine the activity of 5-FU + LV+ AZT or the effects on DNA of peripheral nuclear cells. In the phaseII study, where the main purpose was to determine the activity of AZTat its MTD in combination with 5-FU + LV, the main elegibilitycriteria included: histologically confirmed diagnosis of colorectaladenocarcinoma with metastatic disease, Eastern Cooperative Oncol-ogy Group (ECOG) performace status <2 , measurable disease, noprevious adjuvant or palliative chemotherapy, leukocyte count^3500/mm3 , platelet count > 100.000/mm3, serum creatinine =£1.5mg/dl, serum bilirubin $1.5 mg/dl and transaminases $2.5 timesnormal values. Patients with a history of other malignant tumor(except in situ carcinoma of the cervix or non-melanoma skin cancer),symptomatic cardiac disease or recent history of myocardial infarctionor arrhythmia, active infections or cerebral metastases were excluded.To determine the effects of 5-FU + LV, AZT and 5-FU + LV + AZTonDNA strand-breaks of peripheral mononuclear blood cells, the sameselection criteria were used, but also patients with non-measurableor non-evaluable metastatic disease could be included in the study
Approval for these studies was obtained from the local EthicalCommittee; patients were informed of the nature of the study, gavetheir informed consent and were pre-registered before entry into thestudy.
Treatment and study design
In the phase II study, 5-FU was administered as i.v. bolus (3-5 minutes)at a dose of 500 mg/m2 in the middle of a 2-hour i.v. infusion of the 1isomer form of leucovorin 250 mg/m2. AZT 8 g/m2 was diluted inapproximately 1.5 L of sodium chloride 0.9% and given i.v. over 120minutes starting after the end of the LV infusion. Treatment wasrepeated every week at full doses if WBC > 2000 mm3, PLT Jt 75.000mm3, there was no persistent diarrhea or stomatitis > grade 1 and ifWHO grades II I—IV toxicities had not occurred. In instances of WBC<2000, PLT < 75.000 or persistent diarrhea or stomatitis > grade 1treatment was delayed one week. If grade III non-haematologicaltoxicity had occurred, treatment was continued, after recovery, withthe 5-FU and AZT doses reduced by 20% (the LV dose was notmodified). In the presence of grade 4 toxicity chemotherapy wasdefinitively discontinued, or continued with the 5-FU and AZT dosesreduced by 50%. Treatment was continued for a maximum of 26weekly cycles or until the advent of progressive disease or intolerabletoxic effects. If a further improvement was noticed after 26 cycles,treatment was continued for a total of 34 weekly cycles.
In the separate group of patients in whom DNA strand breaks weredetermined in peripheral nuclear blood cells, 5-FU 500 mg/m2, LV250 mg/m2 and AZT 8 g/m2 were administered as in the phase IIstudy, but patients received three separate weekly courses of 5-FU +LV without AZT or AZT alone or 5-FU + LV + AZT. The sequence ofadministration of the three different treatments was randomly deter-mined on the hypothesis that a cumulative effect on DNA damagecould be observed. After the three weeks of treatment with 5-FU + LV,AZT and 5-FU + LV + AZT patients were treated with 5-FU 370 mg/m2 + LV 100 mg/m2 i.v. bolus for five consecutive days every 28 daysfor 6-8 months or until disease progression
Assessability, toxicity and response criteria
Pretreatment evaluation included history and physical examination,performance status assessment, complete blood cell with differentialand platelet counts, complete blood profile, carcinocmbryonic antigen(CEA), urine analysis, electrocardiogram, chest X-ray or computedtomography (CT) scan, abdominal CTscan and/or sonogram and anyother appropriate diagnostic procedure appropriate for evaluatingmetastatic sites. During treatment, a physical examination and com-plete blood cell count were repeated every week, blood profile, urineanalysis and CEA every four weeks, and sites of metastatic diseasewere evaluated every eight weeks with radiographs or CTscan. A chestX-ray and/or an abdominal sonogram were repeated every six monthsif there was no evidence of lung or abdominal disease. Toxicity andresponses were scored according to standard WHO criteria [23] Inparticular, complete response (CR) was defined as the complete dis-appearance of all known disease demonstrated at two separate exami-nations performed at least eight weeks apart; partial response (PR), a50% or greater decrease in total tumor area demonstrated at twoseparate examinations performed at least eight weeks apart; minorresponse (MR), a 25%-50% decrease in total tumor area; stabledisease (SD), when neither a < 25% decrease nor a < 25% increase intotal tumor area had been demonstrated for at least eight weeks;progressive disease (PD), the appearance of any new lesion not pre-viously identified or a > 25% increase of one or more existing lesions.Durations of response were calculated from the first day of treatmentto the date of first observation of progressive disease or last examina-tion.
Downloaded from https://academic.oup.com/annonc/article-abstract/8/6/539/197888by gueston 02 April 2018

541
Analysis of DNA strand breaks
Single strand breaks (SSB) in DNA from peripheral blood nucleatedcells were measured before, and 24 and 48 hours after the start oftreatment with AZTor 5-FU + LVor5-FU + LV + AZT. A fluorescentanalysis of DNA unwinding, previously described and modified forwhole blood cellular populations by collection in heparinized tubesand lysis of erythrocytes without further separation of cells, was usedto evaluate the percentage of double-stranded and single-strandedDNA [24]. Briefly, blood samples (10 ml) from patients were collectedin heparinized tubes and were mixed with 9 ml of solution A (0.87%NH4CI, 10 mM Tns-HCI (pH 7.2)) and held at 0°C for 20-30 minuntil lysis of erythrocytes was complete. The suspension was centri-fuged (0 °C, 20 min, 400 g), the pellet suspended in 3 ml of solution Aand cells were again centrifuged for 10 min. This pellet was suspendedin 2 7 ml of solution B (0.25 M myo-inositol, 10 mM sodium phos-phate, lmM MgCl2) to give a total WBC concentration of 5-10 x106 ml. Aliquots of this suspension (0.2 ml) were distributed into 12disposable glass tubes designated T, P or B in groups of 4. T tubes wereused to estimate the total fluorescence (double-stranded DNA + con-taminants), P tubes to estimate the unwinding rate of DNA and Btubes (blank) to estimate the contribution to fluorescence by compo-nents other than double-stranded DNA. For this purpose, 0.2 ml ofsolution C (9 M urea, 10 mM NaOH, 2 5 mM cyclohexanediaminetetraacetate, and 0.1% sodium dodecylsulfate {SDS)) was added toeach tube and incubated at 0°C for 10 min. After this time, duringwhich cell lysis and chromatin disruption occurred, 0.1 ml of solutionD (45% of solution B and 55% 0.2 N NaOH) and 0.1 ml of solution E(40% of solution C and 60% of 0.2 N NaOH) were gently added to theP and B tubes. After incubation at 0°C for a further 30 min duringwhich the alkali diffused into the lysate to give a final pH of approxi-mately 12.8, the contents of the B tubes were sonicated for 1-2 s toensure rapid denaturation of the DNA in the alkaline solution; P and Btubes were further incubated at 15 °C for 60 min and then denaturationwas stopped by chilling to 0°C and adding 0.4 ml of solution F (1 Mglucose, and 14 mM p-mercaptoethanol) which lowered the pH toapproximately 11.0 The lysates were briefly sonicated to render themhomogeneous, diluted with 1.5 ml of solution G (ethidium bromide 6.7ug/ml, and 13 3 mM NaOH) and their fluorescence was read at roomtemperature in a Perkin-Elmer spectrofluorometer (excitation wave-length 520 nm and emission 590 nm). The T tubes differed from the Ptubes in that the neutralizing solution E was added before the alkalineC and D solutions so that the DNA was never exposed to a denaturingpH. The extent of DNA unwinding after a given time of exposure ofcell extracts to alkali was calculated from the fluorescence values of theT, P and B samples. The percent of double stranded DNA is given bythe formula (P-B)/(T-B) x 100 where (P-B) provides an estimate of theamount of double-stranded DNA remaining after exposure to alkalifor 60 min, and (T-B) an estimate of the amount of double-strandedDNA in the cell extracts. Up to the point at which solution D wasadded, all steps were carried out under ordinary room illumination;after this, manipulations were carried out in the dark and incubationswere in a covered bath. All solutions were kept at 0 °C except solutionsC and G which were stored at room temperature
Statistical analysis
In the phase II trial, the optimal two-stage sequential sampling designdescribed by Simon [25] was used to determine the number of patientsto be included. Because responses with 5-FU bolus alone are observedin 10%-ll% of patients and with 5-FU bolus modulated by LV orMTX in approximately !9%-23% of patients [26, 27], a response rateof 30% or greater with a 5-FU bolus-based regimen should be consid-ered promising. Therefore, the design parameters pO (response rate innull hypothesis), and pi (response rate in alternative hypothesis)selected were 0.10 and 0.30, respectively. Considering also an errorprobability a of 0.05 and p of 0.20, the first stage of the study required10 patients and, if at least one objective response was observed, thesecond stage required a total of 29 patients. If at least five patients
responded after the second accrual stage the treatment was consideredpromising unless other considerations indicated otherwise.
The interaction between 5-FU + LV and AZT on DNA-inducedsingle strand breaks of peripheral nuclear blood cells was analysedusing a multiplicative model, as previously described [28, 29]. Briefly,the multiplication of the fraction of double stranded DNA remainingafter treatment with 5-FU + LV or AZT (DS-DNAS.FU + LV or DS-DNAAZTT) w a s compared with the observed result after treament with5-FU + LV + AZT. If DS-DNAJ.FU + LV + AZT < (DS-DNA5.FU + LV xDS-DNAAZT) the interaction is synergistic, if D S - D N A 5 . F ( J + LV + AZT= (DS-DNA 5 -FU + LV x DS-DNAAZT) the interaction is cumulative,and if DS-DNA5.FU + LV + AZT > (DS-DNA5.FU + LV x DS-DNAAZT)it is antagonistic.
Results
Phase II study
From September 1994 to December 1995, 29 patientsentered into this clinical trial. As shown in Table 1 wherethe patient characteristics are summarized, the medianECOG PS was 0 (range 0-1), the predominant site ofmetastasis was the liver and 11 patients had multiplemetastatic sites. A total of 585 weekly cycles of 5-FU +LV + AZT were administered with a median of 20 cyclesper patient (range 4-34). All patients are evaluable for
Table I. Patients' characteristics.
Characteristic
No. of patientsMale/femaleAge
MedianRange
ECOG performance status01
PrimaryColonRectum
GradingG 1G 2G3/4Unknown
Previous surgery on primary tumorNumber of metastatic sites
SingleMultiple
Sites of diseaseLiverLungPeritoneumRetroperitoneumSpleenBonePelvis
CEA (ng/ml)MedianRange
LDH (U/L)MedianRange
2920/9
6037-74
219
236
41384
29
1811
25752111
131-850
365171-980
Downloaded from https://academic.oup.com/annonc/article-abstract/8/6/539/197888by gueston 02 April 2018

542
toxicity, which consisted of diarrhea, stomatitis, nauseaand vomiting, leukopenia, dermatitis, conjunctivitis andhypotension. As shown in Table 2, toxicities were usuallymild or moderate (WHO grade 1-2); grades III-IVtoxicities, consisting of diarrhea (17%), nausea and vom-iting (7%), stomatitis (3%), fever (3%) and leukopenia(3%). were uncommon. One patient, who had sufferedan episode of myocardial infarction four years beforestudy entry, died of a cardiac arrhytmia which occurredfive days after the fourth weekly cycle as a consequenceof grade IV diarrhea associated with hypokalemia.Nineteen patients required treatment delays (^ 1 week)or 5-FU and AZT dose reductions because of toxicity,with the median 5-FU and AZT dose intensities being,respectively, 442 mg/m2/week (range 280-500) and 6880mg/m2/week (range 4480-8000). According to the in-tent to treat analysis, all entered patients were includedfor evaluation of response. Two additional patients, inwhom disease was not actually reevaluated, were con-sidered treatment failures (Table 3); one of these was thepatient who died of toxicity after the fourth cycle and theother was one who was lost to follow-up after the fifthcycle and died, presumably of disease progression, fourmonths after treatment start. Overall 3 (10%) completeand 10 (35%) partial responses were observed, for anobjective response rate of 45% (95% confidence limitinterval 26%-64%). Significant subjective improvementwas observed in four of nine patients who initially haddisease-related symptoms. The median time to responsewas two months (range 2 to 4) and the median durationof response eight months (range 2 to 17). Responses
Table 2. Overall worst toxicity (29 evaluable patients).
Adverse event
Nausea /vomitingStomatitisDiarrheaDermatitisLeukopeniaHypotensionFeverConjuntivitisAlopecia
WHO grade (%)
1
383438244114173810
2
31212717210
2124
7
3
73
10030300
4
007000000
Table 3. Objective responses.
Response (WHO) No. pts (%)
Complete responsePartial responseComplete + partialMinor responseStable diseaseTreatment failure
Total
3(10%)10(35%)13(45%)6(21%)5(17%)5(17%)
29(100%)
occurred in liver (10), lung (3), spleen (1) and retroper-itoneum (1). Of the remaining patients 6 (20%) hadminor responses, 5 (17%) stable disease and 5 (17%)were treatment failures (three had documented diseaseprogression) (Table 3). The median time to progressionand median survival times were 7.5 and 14 months,respectively.
Analysis ofDNA strand breaks in peripheral nuclearblood cells
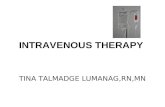
Because previous studies have suggested that 5-FUenhances AZT cytotoxicity by increasing AZT incorpo-ration into DNA and therefore by increasing AZT-induced DNA single-strand breaks [5, 7, 13], 10 patientswere studied for the frequency of DNA single-strandbreaks in peripheral nuclear blood cells 24 and 48 hoursafter treatment with AZT 8 g/m2, 5-FU 500 mg/m2 +LV 250 mg/m2 and 5-FU + LV + AZT. All patients hadmetastatic colorectal cancer (six non-evaluable meta-static disease) and were chemotherapy-naive. Othercharacteristics included median age of 61 years, medianECOG PS of 0, nine were males and the most frequentmetastatic sites were peritoneum and liver. Treatmentswere administered in three separate weeks in differentsequences that were randomly determined. Resultsindicate that after treatment with AZT the mean valuesof double-stranded DNA decreased from approximately93% to 70% and 59% after 24 and 48 hours, respectively.Similar effects on DNA were observed after treatmentwith 5-FU + LV, but the greatest effect was observedafter treatment with 5-FU + LV + AZT which reducedthe percentage of double stranded DNA to 50% and36% after 24 and 48 hours, respectively (Figure 1). Sevendays after treatment with AZT, 5-FU + LVand 5-FU +LV + AZT, no significant residual DNA damage wasobserved and the mean values of double-stranded DNAhad returned to > 90%. The effect of combining 5-FU +LV with AZT on DNA was analysed using the multi-plicative model previously described, and it was foundto be additive. Of the four patients with evaluable dis-ease one obtained a partial response.
Discussion
Despite the increased accumulation in recent decades ofknowledge about the biology and treatment of cancer,the prognosis of metastatic colorectal cancer patientswith unresectable disease remains very poor, with amedian survival of only 10-12 months, and with fewerthan 10% of its victims surviving longer than 36 months[26, 27, 30]. 5-FU has been in use for more than 30 yearsand is still the drug most often administered. However,5-FU alone, given as an i.v. bolus, induces responses inonly 10%-ll% of patients [26, 27]; many attempts havebeen made to combine it with other agents or to modifythe scheduling of its administration in an effort tobiochemically modulate its cytotoxicity [31]. Although
Downloaded from https://academic.oup.com/annonc/article-abstract/8/6/539/197888by gueston 02 April 2018

543
100
« 30-(L
20-
10-
- • - 5-FU+LV
-OAzr-W- 5-FU+LV+AZT
24
Hours
48
Figure I Percentage of double stranded DNA of peripheral nuclearblood cells in 10 metastatic colorectal cancer patients before, 24 and 48hours after treatment with 5-FU 500 mg/m2 + LV 250 mg/m2, AZT 8g/m2 and 5-FU + LV + AZT. Points represent means with SDs shownas vertical lines.
clinical improvement has been obtained by combining5-FU with LV or MTX or by administering 5-FU inprotracted continuous infusion, survival has been onlymarginally improved and results remain unsatisfactory[26, 27, 32, 33]. More recently, new studies [34-41] havereported promising results from the use of high doses of5-FU given as a 24-48-hour continuous infusion, or bycombining a 5-FU continuous infusion with a 5-FUbolus + MTX, or by administering 5-FU as a circadianmodulated continuous infusion, or with new agents suchas tomudex, irinotecan, doxifluridine and oxaliplatin,and further study is warranted.
Recent experimental and clinical studies have sug-gested that a new approach to improving the treatmentof colorectal cancer might be to combine a toxic thymi-dine analogue, such as AZT, with an inhibitor of dTMPsynthesis such as 5-FU, MTX, tomudex and others[5-12]. Indeed, these agents facilitate the incorporationof AZTTP into DNA by lowering intracellular dTTPpools and thus enhancing DNA damage and cytotoxic-ity [7, 8, 13]. Interestingly, experimental studies havedemonstrated that this effect is more evident in colorec-tal cancer cells because of an elevated thymidine kinase
activity (which activates AZT to AZTTP) and the lackof an efficient concentrative nucleoside transport forthymidine, since thymidine competes with AZT forphosphorylation and incorporation into DNA [7, 14-21]. In initial phase I studies [42, 43] AZT, in combina-tion with 5-FU and LV, was administered orally or inprotracted (48 hours) intravenous infusions that did notrender possible attainment of plasma AZT concentra-tions that had been demonstrated to be effective in nudemice bearing tumour xenografts (0.5-1 mmol/L) [7, 8].Subsequent phase I studies, therefore, have used shorterintravenous infusions of high doses of AZT which haveallowed achievement of peak plasma concentrationssimilar to those previously obtained in preclinical ani-mal models and rendered possible a promising activityin previously untreated metastatic colorectal cancerpatients [22, 44, 45]. However, these studies did notdemonstrate an activity for 5-FU + LV + AZT in heavilypretreated metastatic colorectal cancer patients resist-ant to 5-FU [42, 43, 45]. This is not surprising, not onlybecause heavily pretreated patients with bulky diseaseand chemoresistant tumours very rarely respond to anyfurther chemotherapy, but also because the mechanismof action of the 5-FU + AZT combination requires that5-FU possess some degree of activity. Indeed, if thymi-dylate synthase (TS) is not inhibited and therefore dTTPpools are not lowered, AZT incorporation into DNA isnegligible and does not lead to a detectable clinicalactivity [13]. Of interest is the fact that these phase Istudies [42, 43] demonstrated a dose-dependent biologiceffect of AZT manifested by an increase in DNA strandbreaks in peripheral nuclear blood cells. However, thepossible enhancement by 5-FU of AZT incorporationinto DNA and therefore of AZT-induced DNA singlestrand breaks, was not investigated.
In the present study, we evaluated the activity of acombination of 5-FU bolus+LV with high doses ofintravenous AZT, administered at its MTD as a short(120') intravenous infusion, in chemotherapy-naivemetastatic colorectal cancer patients, and we also inves-tigated whether the enhancement of AZT-induced DNAstrand breaks by 5-FU, previously demonstrated inexperimental models, could be confirmed clinically inperipheral nuclear blood cells. Leucovorin was added to5-FU to enhance TS inhibition, and therefore the deple-tion of dTTP pools, and AZT was administered starting60' after 5-FU to ensure that high AZT tumour concen-trations were present when TS was inhibited [46].Although the response rate observed in this trial has awide 95% confidence limit interval (26%-64%), theantitumor activity of this new combination appearspromising; in fact, it compares favourably with that ofsimilar regimens with weekly bolus 5-FU plus LV with-out AZT (response rates 20%-25%) [26], and it is in thesame range as that of more demanding regimens inwhich 24-48-hour or protracted infusions of 5-FU orchronomodulated infusions of 5-FU plus oxaliplatinhave been used [34-37]. These results, therefore, confirmthe elevated activity of 5-FU + LV + AZT already
Downloaded from https://academic.oup.com/annonc/article-abstract/8/6/539/197888by gueston 02 April 2018

544
observed in the previous phase I studies in chemother-apy-naive patients [22, 45]. This study also demonstratesthat the combination of 5-FU + LV with AZT increasesthe amount of DNA damage and this might reflect anincreased incorporation of AZT into DNA; neverthe-less, because 5-FU + LV alone also induced DNA strandbreaks, other mechanisms could be involved. Interest-ingly, the effect of combining 5-FU + LV with AZT onDNA was only additive and not synergistic as previouslyobserved in colorectal cancer cells in experimental mod-els [5]. A possible explanation is that blood cells, despitehaving an elevated TK activity, also possess an activethymidine transport that could partially protect themfrom the cytotoxic effects of AZT due to the competitionbetween thymidine and AZT, [7,18, 19]. Therefore, it willbe important to study the induction of DNA damage incancer cells of colorectal cancer patients after treatmentwith 5-FU + LV and AZT to determine whether theseeffects on DNA are similar to those observed in bloodcells or, as demonstrated in experimental models, aremore pronounced and the interaction between 5-FU +LVand AZT is synergistic.
In conclusion, because of these and previous findingswith 5-FU + LV + AZT in metastatic colorectal cancer,further studies are warranted. In particular, these resultswill require confirmation in randomized trials in whichthe effects of this new combination on survival will alsobe determined. Furthermore, because of recent experi-mental findings demonstrating that AZT might circum-vent cisplatinum resistance and synergistically poten-tiate the cytotoxicity of cisplatinum + 5-FU [47], andalso that alfa-interferon enhances AZT cytotoxicity [48],phase I—II studies clinically testing these observationsshould be performed. Some have already been initiated[49-51]. Most notably, a phase I study in 12 patients withmetastatic gastrointestinal carcinomas demonstrates thefeasibility of a combination with 5-FU + LV + AZT andcisplatin, and some activity also in chemotherapy-pre-treated patients [51]; furthermore, a phase II study inHTLV-1 associated adult T-cell leukemia-lymphomawith a combination of AZT and alfa-interferon demon-strates a significant activity for this combination, witheight of nine patients obtaining an objective response[49]. Finally, it will be of interest to combine AZT with5-FU administered in continuous infusion because of itsmore specific effect on TS when compared with 5-FUbolus [52]; similarly, it will be interesting to combineAZT with the new folate-based TS inhibitors such astomudex which, being very specific and effective inhibi-tors of TS, might enhance AZT antitumor activity evenmore efficiently than 5-FU.
Acknowledgement
The work was partially supported by a grant from theAssociazione Italiana per la Ricerca sul Cancro(A.I.R.G), Milano, Italy and M.UR.S.T 60%.
References
1. Wilde MI, Langtry HD. Zidovudine. An update of its pharmaco-dynamic and pharmacokinetic properties and therapeutic effi-cacy. Drugs 1993; 46: 515-78.
2. Furman PA, Fyfe JA, St. Clair MH et al. Phosphorylation of 3'-azido-3'-deoxythymidine and selective interaction of the 5'-tri-phosphate with human immunodeficiency virus reverse transcrip-tase. Proc Natl Acad Sci USA 1986; 83: 8333-7.
3. Fischl MA, Richmann DD, Grieco MH et al. The efficacy ofazidothymidine in the treatment of patients with AIDS andAIDS-related complex. N Engl J Med 1987; 317: 185-91.
4. Horowitz JP, Chua J, Noel MJ. Nucleosides. V. The monomesy-lates of l-(2'-deoxy-beta-D-lyxofuranosyl)thymidine. J Org Chem1964; 29: 2076-8.
5. Andreuccetti M, Allegrini G, Antonuzzo A et al. Azidothymidinein combination with 5-fluorouracil in human colorectal cell lines:'In vitro' synergistic cytotoxicity and DNA-induced strandbreaks. Eur J Cancer 1996; 32A: 1219-26.
6. Szekeres T, Findenig G, Fritzer M et al. Synergistic cytotoxiceffects of 5-fluorouracil with AZT in human colon carcinomacells. Proc Am Ass Cancer Res 1995; 36: 297.
7. Brunetti I, Falcone A, Calabresi P et al. 5-Fluorouracil enhancesazidothymidine cytotoxicity: In vitro, in vivo, and biochemicalstudies. Cancer Res 1990, 50. 4026-31.
8. Tosi P, Calabresi P, Goulette FA et al. Azidothymidine-inducedcytotoxicity and incorporation into DNA in the human colontumor cell line HCT-8 is enhanced by methotrexate in vitro and invivo. Cancer Res 1992; 52: 4069-73.
9. Tosi P, Visani G, Ottaviani E et al. Hydroxyurea enhances 3'-azido-3'-deoxythymidine (AZT) cytotoxicity in human chronicmyeloma leukemia models. Eur J Haematol 1994; 52: 291-5.
10. Weber G, Nagai M, Prajda N et al. AZT: A biochemical responsemodifier of methotrexate and 5-fluorouracil cytotoxicity inhuman ovarian and pancreatic carcinoma cells. Cancer Commun1991; 3- 127-32.
11. Weber G, Ichikawa S, Nagai M et al. Azidothymidine inhibitionof thymidine kinase and synergistic cytotoxicity with methotrex-ate and 5-fluorouracil in rat hepatoma and human colon cancercells. Cancer Commun 1990; 2: 129-34.
12. Pressacco J, Mitrovski B, Erlichman C. Cytotoxic consequencesof combining zidovudine with D1694 in MGH-U1 and HCT-8cells. Proc Am Assoc Cancer Res 1993; 34: 299.
13. Darnowski JW, Goulette FA. 3'-Azido-3'-deoxythymidine cyto-toxicity and metabolism in the human colon tumor cell lineHCT-8. Biochem Pharmacol 1994, 48. 1797-805.
14. Weber G, Lui MS, Takeda E et al. Enzymology of human colontumors. Life Sci 1980; 27: 793-9.
15. Sakamoto S, Sagara T, Iwama T et al. Increased activity ofthymidine kinase isozymes in human colon polyp and carcinoma.Carcinogenesis 1985; 6: 917-9.
16. Denton JE, Lui MS, Aoki Tet al. Enzymology of pyrimidine andcarbohydrate metabolism in human colon carcinomas. CancerRes 1982; 42: 1176-83.
17. Herzfeld A, Legg MA, Greengard O. Human colon tumors.Enzymic and histological characteristics. Cancer 1978; 42:1280-3.
18. Wohlhueter RM, Marz R, Plagemann PGW. Thymidine transportin cultured mammalian cells. Kinetic analysis, temperaturedependence and specificity of the transport system. BiochemBiophys Acta 1979; 553: 262-83.
19. Paterson ARP, Kolassa N, Cass CE. Transport of nucleosidedrugs in animal cells. Pharmacol Ther 1981; 12: 516-36.
20. Belt JA, Vijayalakshmi D. Sodium-dependent nucleoside trans-port in mouse intestinal epithelial cells: Two transporters withdiffering substrate specificities. Proc Am Assoc Cancer Res 1988;29: 13.
21. Dagnino L, Bennett LL, Paterson ARP. Concentrative transportof nucleosides in L1210 mouse leukemia cells. Proc Am AssocCancer Res 1987; 28: 15.
Downloaded from https://academic.oup.com/annonc/article-abstract/8/6/539/197888by gueston 02 April 2018

545
22 Falcone A, Danesi R, Dargenio F et al. Intravenous azidothymi-dine with fluorouracil and lcucovorin. A phase I—II study inpreviously untreated metastatic colorectal cancer patients. J ClinOncol 1996; 14. 729-36.
23. Miller AB, Hoogstraten B, Staquet M et al. Reporting results ofcancer treatment. Cancer 1981; 47: 207-14.
24. Birnboim HC, Jevcak JJ. Fluorometric method for rapid detec-tion of DNA strand breaks in human blood cells produced by lowdose of radiation. Cancer Res 1981; 41: 1889-92
25. Simon R. Optimal two-stage designs for phase II clinical trials.Controlled Clin Trials 1989; 10: 1-10.
26 Advanced Colorectal Cancer Meta-Analysis Project. Modulationof fluorouracil by leucovorin in patients with advanced colorectalcancer: Evidence in terms of response rate. J Clin Oncol 1992; 10:896-903.
27. Advanced Colorectal Cancer Meta-Analysis Project. Meta-anal-ysis of randomized trials testing the biochemical modulation offluorouracil by methotrexate in metastatic colorectal cancer. JClin Oncol 1994; 12. 960-9.
28. Sayers TJ, Wiltrout TA, McCormick K et al. Antitumor effects ofot-interferon and y-interferon on a munne renal cancer (Renca) invitro and in vivo. Cancer Res 1990; 50: 5414-20.
29. Falcone A, Danesi R, Zaccaro L et al. Synergistic antiprolif-erative activity of suramin and a2A-interferon against humancolorectal adenocarcinoma cell lines: In vitro studies. Eur JCancer 1994; 30A: 516-20.
30. Ahlgren JD. Colorectal cancer: Chemotherapy In Ahlgren JD,Macdonald JS (eds): Gastrointestinal Oncology. Philadelphia.J.B. Lippincott Company 1992; 339-57.
31. Sotos GA, Grogan L, Allegra J. Preclimcal and clinical aspects ofbiomodulation of 5-fluorouracil. Cancer Treat Rev 1994, 20:
32 Bertino JR. Ode to methotrexate J Clin Oncol 1993; 115-14.33. Lokich JJ, Ahlgren JD, Gullo JJ et al. A prospective randomized
comparison of continous infusion fluorouracil with a conven-tional bolus schedule in metastatic colorectal carcinoma: A mid-atlantic oncology program study. J Clin Oncol 1989, 7: 425-32.
34. Ardalan B, Chua L, Tian E et al A phase II study of weekly24-hour infusion with high-dose fluorouracil with leucovorin incolorectal carcinoma. J Clin Oncol 1991; 9: 625-30.
35. Rubio ED, Aranda E, Campus C et al. A phase II study of weekly48-hour infusions with high-dose fluorouracil in advanced color-ectal cancer: An alternative to biochemical modulation. J Infu-sional Chemother 1994; 4- 58-61.
36. Sobrero AF, Aschele C, Guglielmi AP et al. Schedule selectivebiochemical modulation of 5-fluorouracil: A phase II study inadvanced cancer. Clin Cancer Res 1995; 1: 955-60.
37. Levi FA, Zidani R, Vannetzel JM et al. Chronomodulated versusfixed-infusion-rate delivery of ambulatory chemotherapy withoxaliplatin, fluorouracil, and fohnic acid in patients with colorec-tal cancer metastases: A randomized multi-institutional trial. JNatl Cancer Inst 1994; 86: 1608-17.
38. Seitz JF, Cunningham D, Rath U et al. Final results and survivaldata of a large randomized trial of tomudex in advanced color-ectal cancer confirm comparable efficacy to 5-fluorouracil +leucovorin. Proc Am Soc Clin Oncol 1996; 15: 201.
39. Rothenberg ML, Eckardt JR, Kuhn JG et al. Phase II trial of
irinotecan in patients with progressive or rapidly recurrent color-ectal cancer. J Clin Oncol 1996; 14:1128-35.
40. Falcone A, Pfanner E, Ricci S et al. Oral doxifluridine in elderlypatients with metastatic colorectal cancer: A multicenter phase IIstudy. Ann Oncol 1994; 5: 760-2.
41. Baietta E, Colleoni M, Di Bartolomeo M et al. Doxifluridine andleucovorin: An oral treatment combination in advanced color-ectal cancer. J Clin Oncol 1995; 13' 2613-9.
42. Posner MR. Darnowski JW, Calabresi P et al. Oral zidovudine,continous infusion fluorouracil, and oral leucovorin calcium: Aphase I study. J Natl Cancer Inst 1990; 82: 1710-4.
43. Posner MR, Darnowski JW,Weitberg AB et al. High-dose intra-venous zidovudine with 5-fluorouracil and leucovorin. A phase Itrial. Cancer 1992; 70. 2929-34.
44 Beitz JB, Darnowski JW, Cummings FJ et al. A phase I andpharmacologic analysis of fluorouracil + leucovorin combinedwith infused high-dose zidovudine Proc Am Assoc Cancer Res1992; 33: 427.
45. Posner M, Darnowski J, Tessitore J et al. A phase I trial of highdose intravenous zidovudine and 5-fluorouracil/leucovorin. ProcAm Soc Clin Oncol 1993; 12. 162.
46. Spears CP, Gustavsson BG, Berne M et al. A mechanism ofinnate resistance to thymidylate synthase inhibition after 5-flu-orouracil. Cancer Res 1988; 48. 5894-900.
47. Andreuccetti M, Allegrini G, Antonuzzo A et al. Azidothymidineenhances 'in vitro 'cisplatin and cisplatin + 5-fluorouracil cytotox-icity against the human colorectal cancer cell line COLO-320DM.Proc Am Assoc Cancer Res 1996, 37: 292
48. Darnowski JW, Goulette FA. Synergistic cytotoxicity with alpha-interferon and azidothymidine in HCT-8 cells reflects increasedazidothymidine incorporation in DNA Proc Am Assoc CancerRes 1994, 35: 334.
49. Hermine O, Bouscary D, Gessain A et al. Treatment of HTLV-1associated adult T-cell leukemia-lymphoma with a combinationof zidovudine and interferon-alpha. Blood 1995; 86 (Suppl 1).931a.
50. Tosi P, Gherhnzoni F, Visani G et al. Zidovudine as an antineo-plastic agent in the treatment of HIV related high-grade non-Hodgkin lymphoma. Blood 1994; 84 (Suppl 1): 518a.
51 Anand A, Ellis M, Tessitore J et al. A phase I study of intermittenthigh-dose zidovudine, 5-fluorouracil/leucovonn and cisplatin.Proc Am Soc Clin Oncol 1995; 14. 481.
52. Sobrero AF, Aschele C, Guglielmi AP et al. Synergism and lackof cross-resistance between short-term and continuous exposureto fluorouracil in human colon adenocarcinoma cells. J NatlCancer Inst 1993; 85: 1937-^4.
Received 10 October 1996; accepted 19 February 1997.
Correspondence to:Alfredo Falcone, MDU.O. Oncologia MedicaOsp. S. ChiaraVia Roma, 6756126 PisaItaly
Downloaded from https://academic.oup.com/annonc/article-abstract/8/6/539/197888by gueston 02 April 2018