Maxillofacial Trauma Dr. Fuad AbulJadayel BDS, DPH, MSc, Jord. Board.e Maxillofacial Specialist.
30
Maxillofacial Trauma Dr. Fuad AbulJadayel BDS, DPH, MSc, Jord. Board.e Maxillofacial Specialist
Transcript of Maxillofacial Trauma Dr. Fuad AbulJadayel BDS, DPH, MSc, Jord. Board.e Maxillofacial Specialist.
Maxillofacial Trauma
Dr. Fuad AbulJadayel
BDS, DPH, MSc, Jord. Board.e
Maxillofacial Specialist
Aetiology
Interpersonal violence tends to be the most common aetiology in the UK.
Road traffic accidents.
Falls.
Sports injuries.
Industrial injuries.
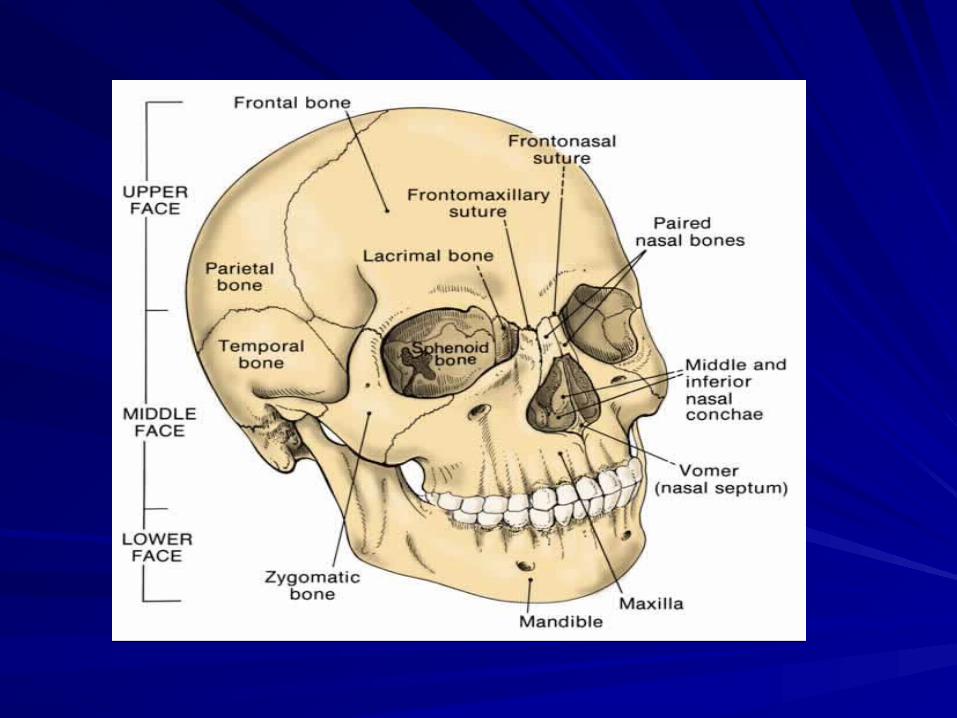
Surgical Anatomy
The upper facial skeleton (The Frontal Bone).
The middle facial skeleton (MFS).
The lower facial skeleton (The mandible).
Surgical Anatomy of MFS- Boundary: zygomaticofrontal suture Zygomaticofrontal
suture occlusal plane of the upper teeth.
The MFS is made up of the Following Bones:
1. Two maxillae.
2. Two zygomatic bones.
3. Two zygomatic processes of the temporal bones.
4. Two palatine bones.
5. Two Nasal bones
6. Two lacrimal bones
7. The vomer
8. The Ethmoid and its attached conchae
9. Two inferior conchae
10.The pterygoid plates of the sphenoid.
Death from trauma has a trimodal distribution
The first peak
Within seconds or minutes of the injury, due major damage to brain, spinal cord, heart, aorta, or other large vessels.
The second death peak
Minutes to hours after injury “golden hour.”
Death is usually due to subdural haematoma, ruptured spleen, pelvic #.
The third death peak
Days to weeks after injury.
Death due to sepsis and organ failure.
Management of Trauma
Initial Assessment:
-Primary Survey (A,B,C,D,E).
-Secondary Survey (GCS).
Eye opening.
Motor response.
Verbal response.
Definitive care phase.
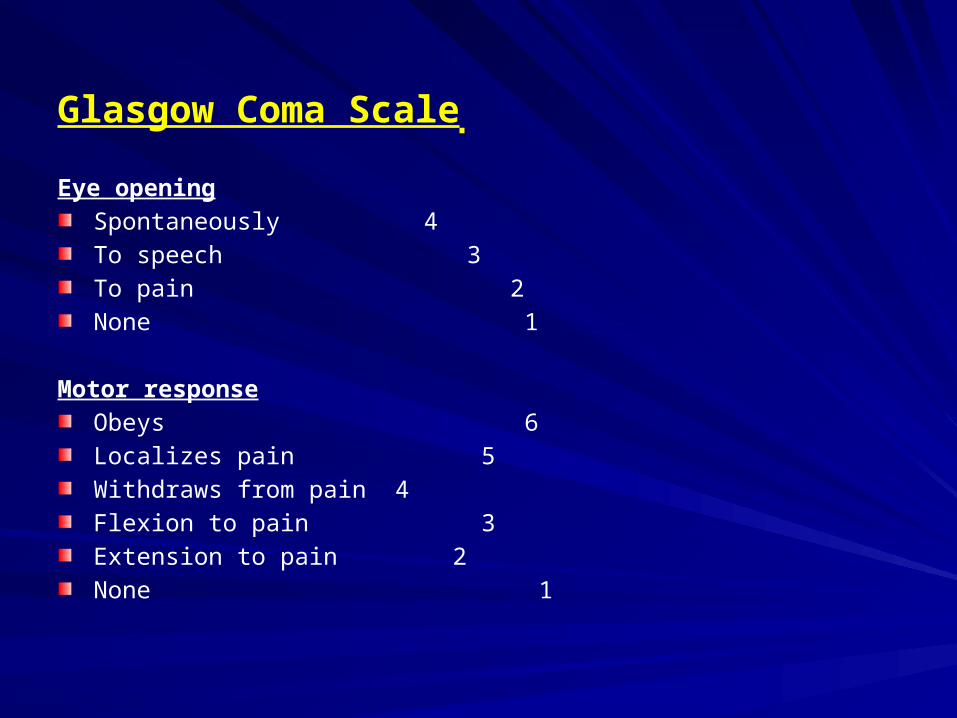
Glasgow Coma Scale
Eye opening
Spontaneously 4
To speech 3
To pain 2
None 1
Motor response
Obeys 6
Localizes pain 5
Withdraws from pain 4
Flexion to pain 3
Extension to pain 2
None 1
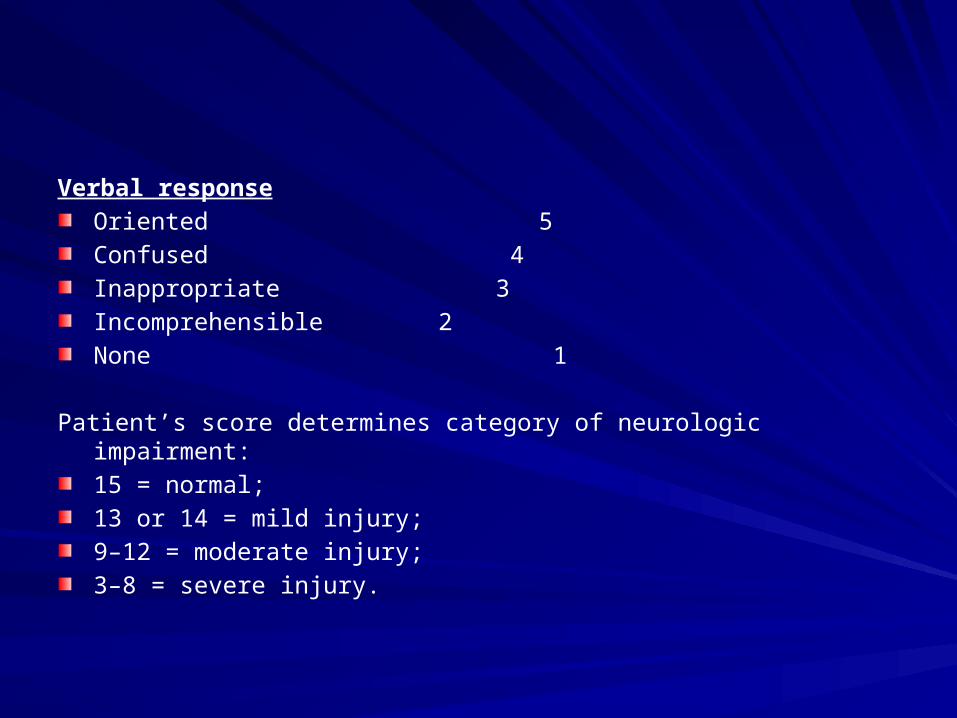
Verbal response
Oriented 5
Confused 4
Inappropriate 3
Incomprehensible 2
None 1
Patient’s score determines category of neurologic impairment:
15 = normal;
13 or 14 = mild injury;
9–12 = moderate injury;
3–8 = severe injury.
Management of Trauma
3 mandatory radiographs:
C1-T1
Chest x-ray
Pelvic x-ray
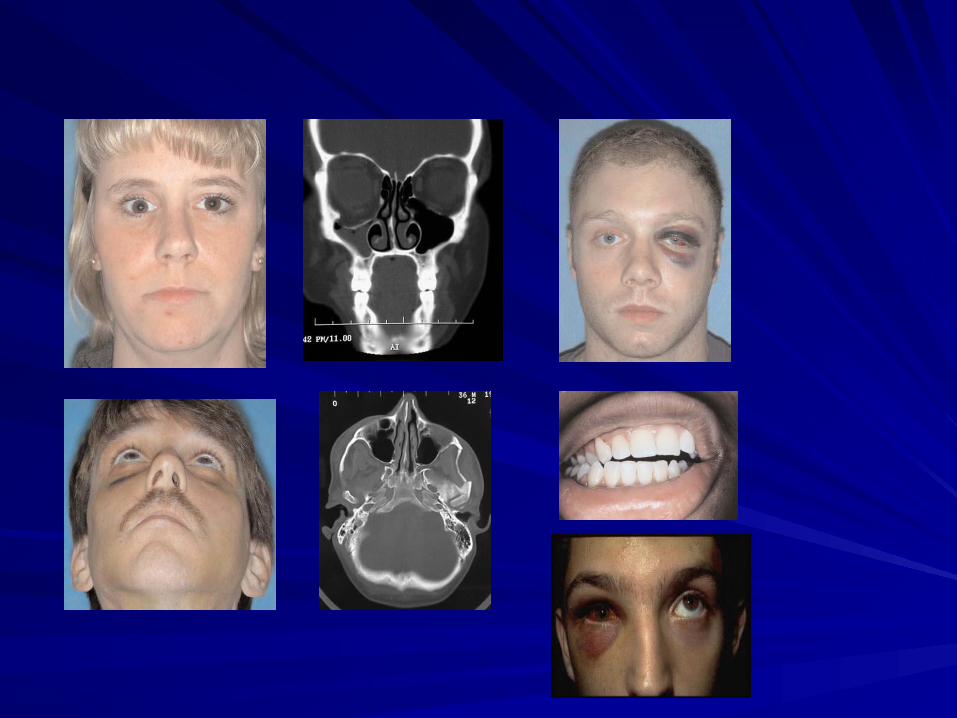
Facial examination
Inspect from the front, profile, and also from above by standing behind, look for deformity, contours, asymmetry, flattening, depression, raccoon’s eyes, battle’s sign, dish face, telecanthus.
Eyes: pupils (reflexes , symmetry), subconjunctival haemorrhage (from direct trauma to globe, or fracture zygoma & orbital wall fracture), epiphora, enophthalmus, proptosis.

Facial examination
Nose: deformity, swelling, obstruction, bleeding and CSF leak, septal hematoma.
Ears: bleeding and CSF leak, hemotympanum.
Mouth: teeth, haematoma (especially sublingual haematoma), intra-oral lacerations, and malocclusion.

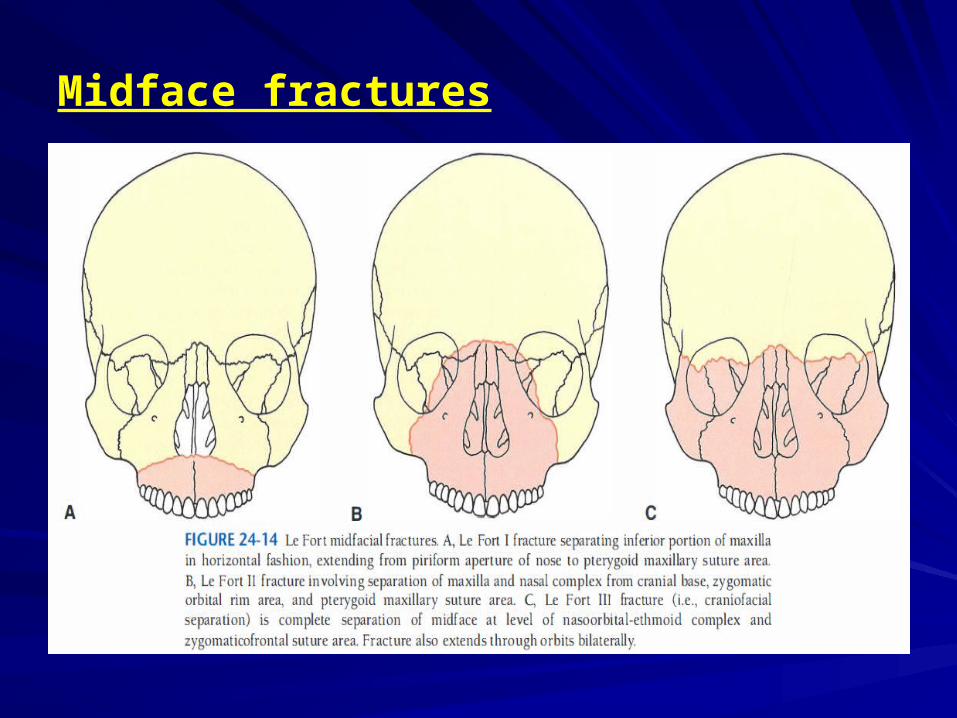
Midface fractures
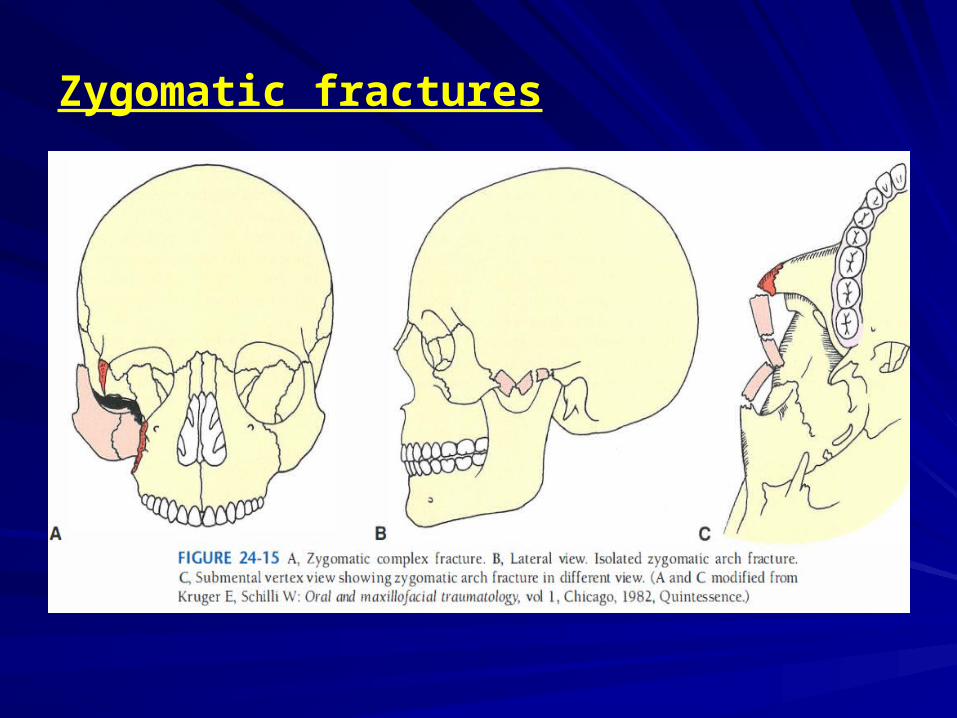
Zygomatic fractures
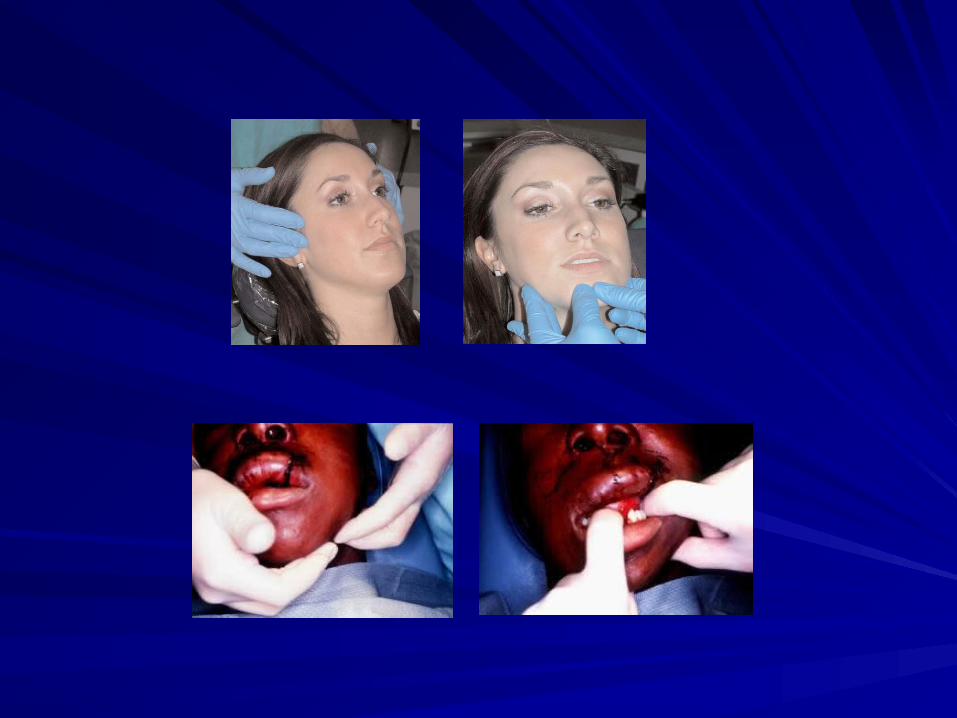
Cont…Examination
Palpate bones to elicit tenderness, crepitus or depression
Feel for step defects, all butresses
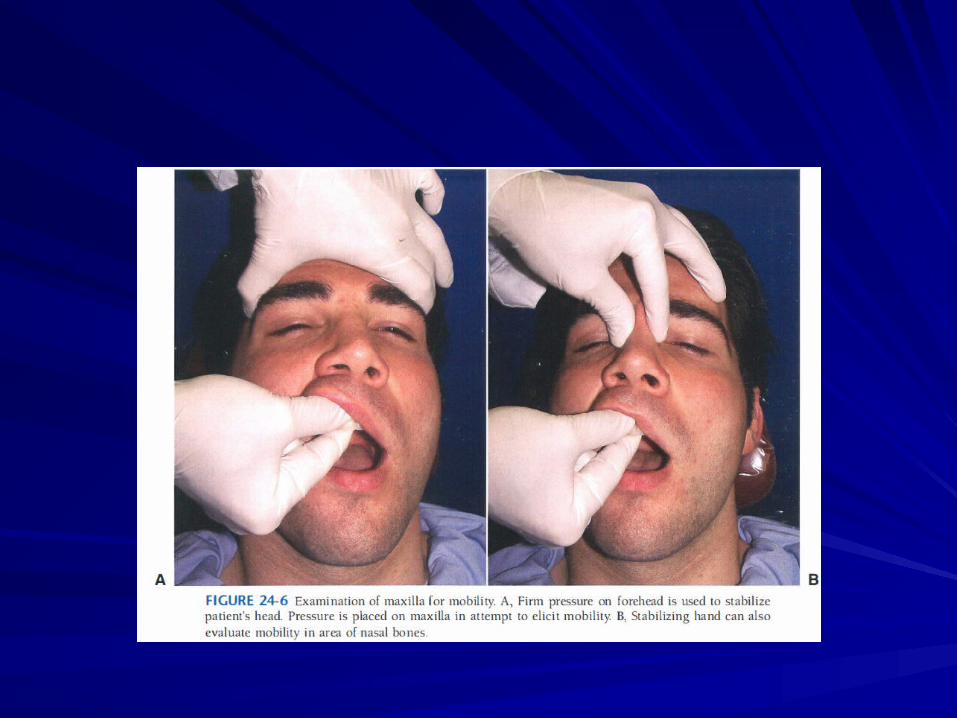
Maxillary mobility, range of mandibular motion, deviation on opening, palpate condyles during motion, test for nondisplaced#
Surgical emphysema.
Visual aquity, visual fields, ocular motility, canthal integrity, eyelid and lacrimal integrity.
Diplopia
Neurologic (II,III,IV,VI,V sensory and VII motor)
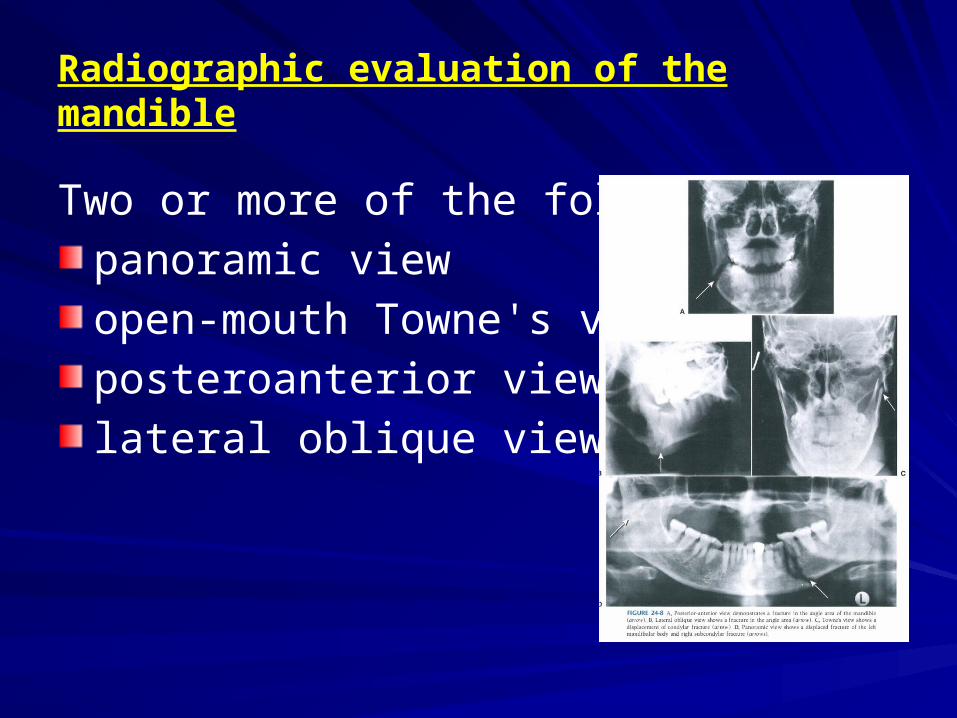
Radiographic evaluation of the mandible
Two or more of the following:
panoramic view
open-mouth Towne's view
posteroanterior view
lateral oblique views
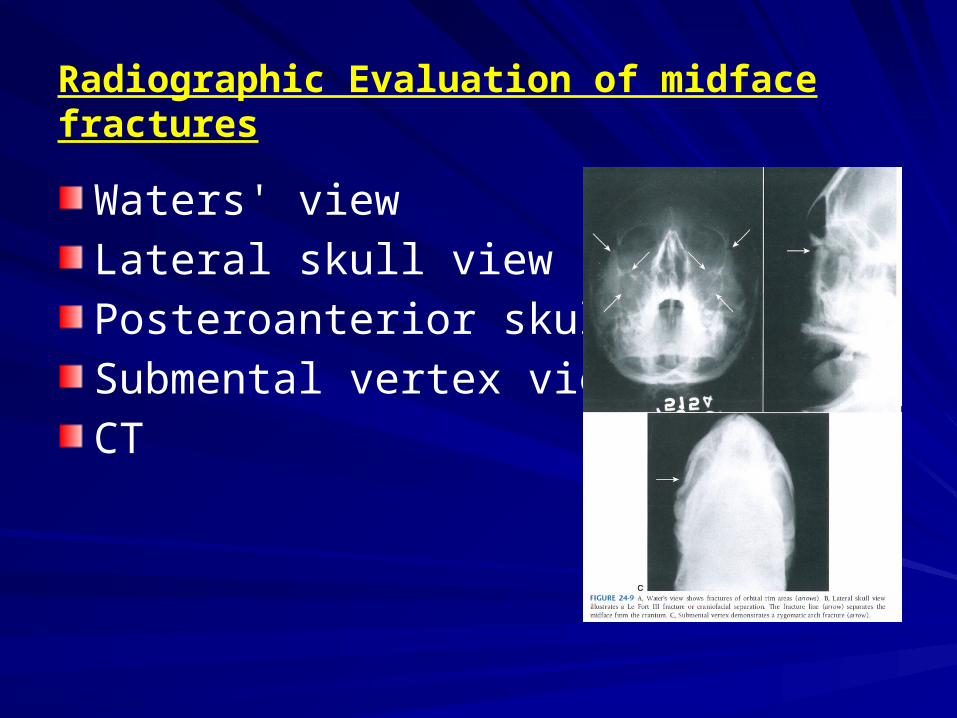
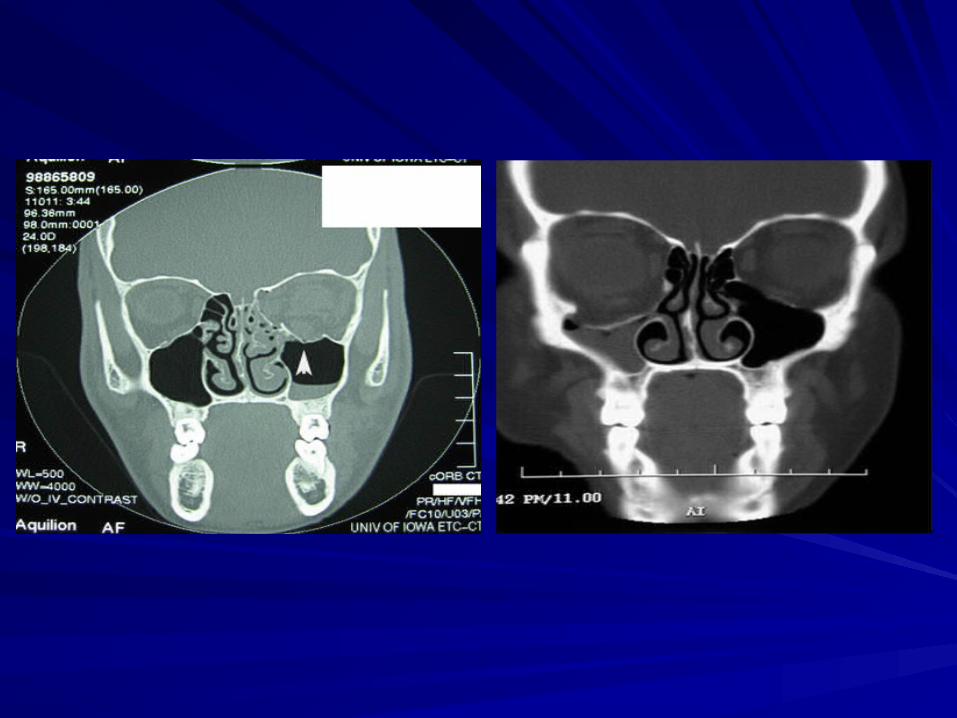
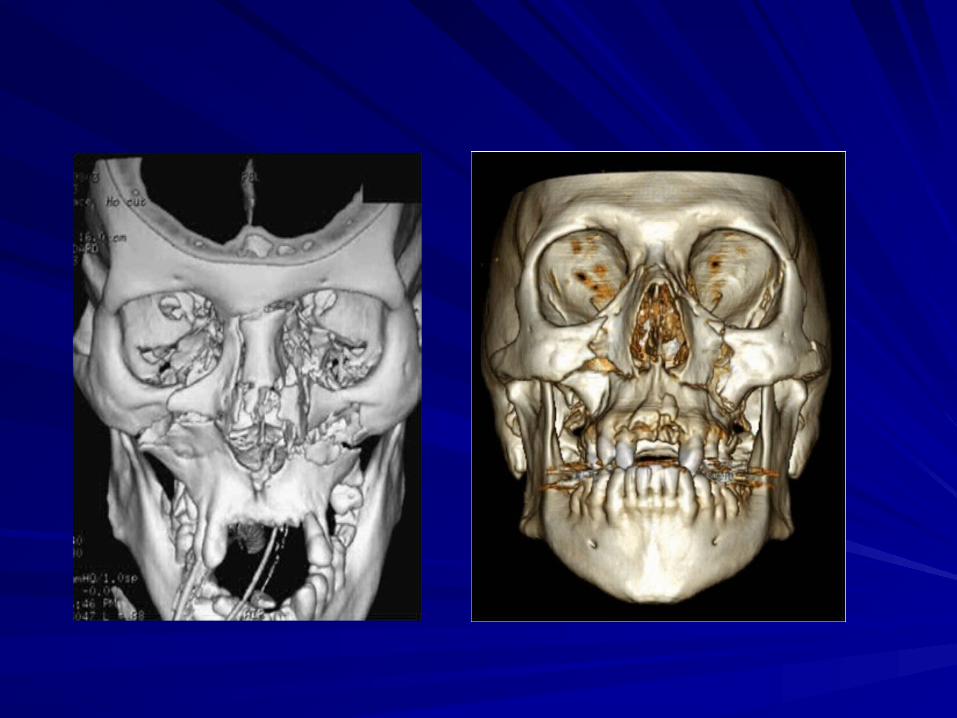
Radiographic Evaluation of midface fractures
Waters' view
Lateral skull view
Posteroanterior skull view
Submental vertex view
CT
Goals of treatment
Rapid bone healing Return of normal appearance Masticatory and nasal function Restoration of speech Minimal complications
Basic surgical principles
Reduction of the fracture Fixation of the bony segment Stabilization of the bony segment Immobilization of segments Preoperative occlusion must be
restored
THANK YOU