Maternal Physiological Changes during Pregnancy, Labor and Puerperium ASSOCIATE PROFESSOR IOLANDA...
178
Maternal Maternal Physiological Physiological Changes Changes during during Pregnancy Pregnancy , Labor and , Labor and Puerperium Puerperium ASSOCIATE PROFESSOR IOLANDA BLIDARU IOLANDA BLIDARU MD, PhD MD, PhD
-
Upload
roberta-norris -
Category
Documents
-
view
219 -
download
6
Transcript of Maternal Physiological Changes during Pregnancy, Labor and Puerperium ASSOCIATE PROFESSOR IOLANDA...

Maternal Maternal Physiological Physiological Changes Changes duringduring
PregnancyPregnancy, Labor and , Labor and PuerperiumPuerperium
ASSOCIATE PROFESSOR IOLANDA BLIDARUIOLANDA BLIDARU
MD, PhDMD, PhD

Pregnancy is a period of Pregnancy is a period of adaptation for :adaptation for :
• The needs of the fetus The needs of the fetus
• Meeting the stress of Meeting the stress of pregnancy and labourpregnancy and labour

THE THE GENITAL GENITAL
CHANGESCHANGES

(A) The whole (A) The whole uterusuterus

increase from increase from 7.5 x 5 x 2.5 7.5 x 5 x 2.5 cmcm in nonpregnant states in nonpregnant states to to 3366 x 25 x 20 cm x 25 x 20 cm at term at term i.e. the volume increase i.e. the volume increase
1000 time1000 time
11 - - SizeSize


increases from increases from 50 gm50 gm in nonpregnant state in nonpregnant state to to 1000 gm1000 gm at term at term
22 - - WeightWeight

pyriform in the nonpregnant state ,
becomes globular at 8th week, then ovoid by 16th
week till term .
33- - ShapeShape

with ascent from the pelvis , the uterus usually undergoes rotation
with tilting to the right (dextrorotation) due to the
presence of the rectosegmoid colon on the left side.
44 - - PositionPosition

5 - Consistency :5 - Consistency :
becomes progressively becomes progressively softer softer due to :due to :
11 - Increased vascularity - Increased vascularity 2 2 - Presence of amniotic fluid- Presence of amniotic fluid

from the first trimester from the first trimester onwards onwards , the uterus undergoes irregular , the uterus undergoes irregular
painless contractions painless contractions (Braxton Hicks contractions)(Braxton Hicks contractions) . .
They may cause some discomfort They may cause some discomfort late in pregnancy and may late in pregnancy and may
account for false labour pain .account for false labour pain .
66- - ContractilityContractility

7- Capacity7- Capacity
increases from increases from 4 ml4 ml in non-pregnant in non-pregnant
state to state to 44-5-5000 ml000 ml at term at term

(B) Myometrial (B) Myometrial changeschanges

1 - 1 - Hypertrophy Hypertrophy (estrogen (estrogen effect)effect) + + hyperplasia hyperplasia (progesterone effect)(progesterone effect)
2 - the fetus exerts a direct 2 - the fetus exerts a direct stretchstretch

2 - Formation of 2 - Formation of the the lower lower
uterine segmentuterine segment (L.U.S.) from the (L.U.S.) from the
isthmusisthmus

Formation of lower Formation of lower uterine segmentuterine segment
After 12 weeks, After 12 weeks, the isthmusthe isthmus (0.5cm)(0.5cm) starts to expand starts to expand
gradually to form the lower gradually to form the lower uterine segment which uterine segment which
measures measures 1010-11-11 cm cm in length at in length at termterm

Upper Uterine SegmentUpper Uterine Segment• PeritoneumPeritoneum: : Firmly-attachedFirmly-attached• Myometrium:Myometrium: 3 layers; outer 3 layers; outer
longitudinal, middle obliquelongitudinal, middle oblique (interlacing network)(interlacing network) and inner and inner circular. circular.
• The middle layer forms 8-shaped fibers The middle layer forms 8-shaped fibers around the blood vessels to control around the blood vessels to control
postpartum hemorrhagepostpartum hemorrhage

Upper Uterine SegmentUpper Uterine Segment
• Decidua:Decidua: Well-developedWell-developed
• Membranes:Membranes: Firmly-attachedFirmly-attached
• Activity:Activity: Active, contracts, Active, contracts, retracts and becomes thicker retracts and becomes thicker during labour.during labour.

Lower Uterine SegmentLower Uterine Segment
• PeritoneumPeritoneum: : Loosely-Loosely-attachedattached
• Myometrium Myometrium : : 2 layers; 2 layers; outer longitudinal and inner outer longitudinal and inner circular.circular.

Lower Uterine SegmentLower Uterine Segment
• DeciduaDecidua: : Poorly-developedPoorly-developed
• MembranesMembranes: : Loosely- Loosely- attached.attached.
• ActivityActivity:: Passive, dilates, Passive, dilates, stretches and becomes thinner stretches and becomes thinner during labourduring labour

The junction between the The junction between the upper uterine segment upper uterine segment
(U.U.S.) which is thick and the (U.U.S.) which is thick and the lower uterine segment which lower uterine segment which
is thin is called the is thin is called the physiologic contraction ringphysiologic contraction ring at the level of the symphysis pubis at the level of the symphysis pubis (not (not
seen or felt)seen or felt)

(C) Uterine (C) Uterine blood vesselsblood vessels

Uterine and vaginal blood supply

1 1 - - Uterine artery lumen:Uterine artery lumen:is doubled and its blood flow is doubled and its blood flow
increases 5 times increases 5 times 2 - 2 - Myometrial and decidual Myometrial and decidual
arteriesarteries (spiral arteries) undergo (spiral arteries) undergo fibrinoid degeneration due to 2 fibrinoid degeneration due to 2 waves of trophoblastic migration , waves of trophoblastic migration , so they become dilated to be the so they become dilated to be the uteroplacentaluteroplacental arteriesarteries

Trophoblast invasion

• Uterine blood flow Uterine blood flow increases increases
progressively and progressively and reaches about reaches about 500 500
ml / minute at termml / minute at term

(D) Changes in the cervix :(D) Changes in the cervix :
1 - 1 - It becomes It becomes hypertrophied , soft and hypertrophied , soft and bluishbluish in colour due to in colour due to oedema and increased oedema and increased
vascularity.vascularity.

2 - Soon after conception, a thick 2 - Soon after conception, a thick cervical secretion obstructs the cervical secretion obstructs the cervical canal forming a cervical canal forming a mucous plugmucous plug . .
3 - The endocervical epithelium 3 - The endocervical epithelium proliferates and proliferates and / / or evertor evertss forming cervical ectopy forming cervical ectopy (previously called erosion) (previously called erosion) (sometimes).(sometimes).

Cervical eversion (colposcopy)

4 - 4 - There are There are 33 principal principal structural components of the structural components of the cervix: cervix: smooth musclesmooth muscle (only (only 10%), 10%), collagencollagen and and connective connective tissuetissue or extracellular matrix or extracellular matrix (ground substance).(ground substance).

55 - -The cervical ripening processThe cervical ripening process -- changes in collagen changes in collagen ((breakdown breakdown and rearrangement of the fibersand rearrangement of the fibers)), , connective tissue and its ground connective tissue and its ground substancesubstance ( (alterations of the alterations of the various glycosaminoglycansvarious glycosaminoglycans))..
6 - 6 - In the ripening of uterine cervix In the ripening of uterine cervix there are involved: there are involved: PGPG E2 and PG E2 and PG F2 alphaF2 alpha,, EE, , PP and relaxin. and relaxin.

(E) Changes in fallopian tubes (E) Changes in fallopian tubes and round and round && broad ligaments : broad ligaments :
InactiveInactive , , elongatedelongated , , marked increase in marked increase in
vascularity vascularity There may be broad There may be broad
ligament ligament varicose veinsvaricose veins

(F) Changes in the vagina :(F) Changes in the vagina :
The vagina becomes The vagina becomes softsoft , , warmwarm , , moist moist with with
increased secretion and increased secretion and violetviolet in colour in colour
(Chadwick's sign)(Chadwick's sign) due to due to increased vascularityincreased vascularity

(G) Changes in the vulva :(G) Changes in the vulva :
•It becomes soft, violet in colour
• Oedema and varicosities may develop

(H) Changes in the ovaries(H) Changes in the ovaries
1 - Both ovaries are 1 - Both ovaries are enlarged due to increased enlarged due to increased vascularity and oedema vascularity and oedema particularly the ovary particularly the ovary
which conwhich conttains the corpus ains the corpus luteum .luteum .

(H) Changes in the ovaries(H) Changes in the ovaries
2 - Corpus luteum continues to 2 - Corpus luteum continues to grow till grow till 7 - 8 weeks7 - 8 weeks, then it , then it
stops growing. stops growing.
It becomes It becomes inactive and starts inactive and starts degeneration at 12 weeksdegeneration at 12 weeks
(degeneration is completed (degeneration is completed after labour) after labour)

Corpus luteum secretesCorpus luteum secretes
1.estrogen 1.estrogen 2.progesterone 2.progesterone
3.relaxin 3.relaxin
hormoneshormones

(H) Changes in the ovaries(H) Changes in the ovaries
3 - 3 - Ovulation ceases during Ovulation ceases during pregnancy due to pregnancy due to
pituitary inhibition by the pituitary inhibition by the high levels of oestrogen high levels of oestrogen
and progesteroneand progesterone

• RelaxinRelaxin is a protein is a protein hormone.hormone.
• Its complete role in Its complete role in pregnancy is debated. pregnancy is debated.
• It may induce It may induce softness and softness and effacementeffacement of the cervix. of the cervix.

II - Haematological II - Haematological ChangesChanges

(A) Blood volume(A) Blood volume
The total blood volume The total blood volume increasesincreases steadily from steadily from
early pregnancy to reach early pregnancy to reach a maximum of a maximum of 35-45 %35-45 % above the non-pregnant above the non-pregnant
level level at 32 weekat 32 week . .

Plasma volume :Plasma volume :
Increases fromIncreases from 2600 2600 ml by ± ml by ± 45 %45 % ( (12120000 in the 1st in the 1st
pregnancy) and pregnancy) and 1500 1500 ml in ml in subsequent pregnanciessubsequent pregnancies
After delivery, it decreases rapidly by 600-After delivery, it decreases rapidly by 600-800ml800ml..

Red blood cell massRed blood cell mass :
• Increases from Increases from 1400 ml1400 ml (nonpregnant) by (nonpregnant) by 3300 % % (± 450 (± 450
ml) due to increased production ml) due to increased production resulting from resulting from erythropoietin erythropoietin
action action
• The increase is steady till full The increase is steady till full term.term.

The increase in plasma The increase in plasma volume is more than the volume is more than the increase in red blood cell increase in red blood cell mass (Hb mass) resulting mass (Hb mass) resulting
in haemodilution in haemodilution
(physiologic (physiologic anemia)anemia)

However, the However, the minimal Hb. minimal Hb. accepted isaccepted is
10-11 gm%10-11 gm%

Changes in the blood volume

Values of increased blood volumeValues of increased blood volume
1 - Meets increased demands 1 - Meets increased demands for uterus, baby .... etc.for uterus, baby .... etc.
2 - Protects against supine 2 - Protects against supine hypotension syndrome.hypotension syndrome.
3 - Protects against fluid loss 3 - Protects against fluid loss at delivery.at delivery.

Increased blood volume Increased blood volume more than the increase more than the increase in red cell mass, leads in red cell mass, leads
to to decreased blood decreased blood viscosityviscosity which leads which leads
to to aa decrease in decrease in peripheral resistanceperipheral resistance

(B) Blood (B) Blood indicesindices

1 - Decreased Hb % and RBCs % :
• Erythrocytes decrease from Erythrocytes decrease from 4.5 million / mm3 to 3.7 4.5 million / mm3 to 3.7
million / mm3million / mm3 (due to the (due to the relative increase in plasma relative increase in plasma volume more than red cell volume more than red cell
mass). mass).

Hb concentrations Hb concentrations fallsfalls
from from 14 g / dl14 g / dl
ToTo
12 g / dl.12 g / dl.

2 - 2 - ReticulocytesReticulocytes : mild : mild 3 - 3 - E.S.R E.S.R :: from 12 to 50 from 12 to 50
mm / hourmm / hour((Erythrocyte Sedimentation RateErythrocyte Sedimentation Rate ))4 – 4 – FibrinogenFibrinogen: : from 200 from 200
- 400 mg / dl to 400 - 600 - 400 mg / dl to 400 - 600 mg / dl.mg / dl.

• All these changes are All these changes are reversed after labour with reversed after labour with
RBCs production (not RBCs production (not destruction)destruction) & the excess Fe & the excess Fe
is stored .is stored .

5 - 5 - White blood cells:White blood cells:
(from 7.000 / mm3 to 10.500 / (from 7.000 / mm3 to 10.500 / mm3 during pregnancy and up to mm3 during pregnancy and up to 16.000 / mm3 during labour16.000 / mm3 during labour..
6 - 6 - PNL & its enzymes. PNL & its enzymes.
(P(Polymorphonuclear Neutrophilic Leukocyteolymorphonuclear Neutrophilic Leukocyte))7 - Lymphocytes: no change.7 - Lymphocytes: no change.

8 - 8 - Platelets:
9 -Total plasma proteins: slightly
(mainly albumin) resulting in osmotic pressure.
10 - Increased plasma lipids

(C) Coagulation (C) Coagulation system system

• PlateletsPlatelets , , unchanged unchanged adhesivityadhesivity..
• FibrinogenFibrinogen doubled to 600 mg % doubled to 600 mg %
• Factor VIIIFactor VIII tripled . tripled .
• Factor VII & factor XFactor VII & factor X doubled doubled
• Factor XI & factor XIIIFactor XI & factor XIII slight slight
• Fibrinolytic activityFibrinolytic activity ..

• Therefore pregnancy is a Therefore pregnancy is a hypercoagulative statehypercoagulative state..
• After delivery, fibrinogen and After delivery, fibrinogen and plasminogen decrease and the plasminogen decrease and the
fibrinolytic activity fibrinolytic activity in thin thee plasma plasma increases.increases.

Ill - Cardiovascular Ill - Cardiovascular system changessystem changes

(A) Changes in the heart(A) Changes in the heart

As the diaphragm is elevated As the diaphragm is elevated progressively during pregnancy progressively during pregnancy the apex is the apex is displaced upwards displaced upwards
and to the leftand to the left so that it lies in the so that it lies in the 4th intercostal space outside the 4th intercostal space outside the
midclavicular line.midclavicular line.
Position:Position:

Pulse rate :Pulse rate :
- The resting pulse rate increases The resting pulse rate increases by by 8 beats / min.8 beats / min.
at at 8 weeks and 8 weeks and 16 beats / min16 beats / min. . at at full term.full term.
-- Some episodes of Some episodes of ectopic beats ectopic beats

Heart soundsHeart sounds• The first heart soundThe first heart sound become become
louder before midpregnancy louder before midpregnancy and splitting of this sound may and splitting of this sound may occur due to earlier closer of the occur due to earlier closer of the mitral than the tricuspid valvemitral than the tricuspid valve
• The intensity of the The intensity of the second second heart soundheart sound may increase. may increase.

Heart soundsHeart sounds• The third soundThe third sound becomes louder becomes louder
before mid-pregnancy and before mid-pregnancy and persists as such till one week persists as such till one week post partum. post partum.
• The fourth soundThe fourth sound may be may be detectable bydetectable by phonocardiography.phonocardiography.

MurmursMurmursSystolic functional murmursSystolic functional murmurs
develop in most of women, usually develop in most of women, usually early systolicearly systolic, but , but mid systolic mid systolic
murmursmurmurs may occur and heard over may occur and heard over the left sternal edge,the left sternal edge,
they are thought to be due to they are thought to be due to functional tricuspid regurgitationfunctional tricuspid regurgitation

ECG CHANGESECG CHANGES• The main features of ECG may be The main features of ECG may be
attributed to the changes in the attributed to the changes in the position of the heart.position of the heart.
• The axisThe axis undergoes undergoes left shift by 15 - left shift by 15 - 28°. 28°.
• The The QRSQRS complexes become of complexes become of low low voltagevoltage, and , and T waveT wave becomes becomes flattenedflattened. .

(B) Haemodynamic (B) Haemodynamic changeschanges

1 - Cardiac output 1 - Cardiac output (C.O.P.)(C.O.P.)

Cardiac output:Cardiac output:
increases mainly by increased increases mainly by increased stroke volume rather than stroke volume rather than
increased heart rate reaching a increased heart rate reaching a maximum of 40%maximum of 40% above the non- above the non-pregnant level pregnant level at 20 weeksat 20 weeks to be to be
maintained till termmaintained till term..Cardiac outputCardiac output = = stroke volumestroke volume x x heart rateheart rate

Cardiac outputCardiac outputDistribution :Distribution :
• 400 ml400 ml to the to the uterusuterus, , • 300300 ml ml to the to the kidneyskidneys,,• 300 ml300 ml to to skinskin,,• 300 ml300 ml to to gastrointestinal gastrointestinal
tracttract, , breast breast & & heartheart

• Roles: Distributes extra 02 • During labour:
Cardiac outputCardiac output increases more increases more particularly during the second particularly during the second
stage due to stage due to pain , uterine pain , uterine contractions, and expulsive contractions, and expulsive
effortsefforts pushing the blood into the pushing the blood into the general circulationgeneral circulation

• Postpartum :
the increased the increased CCARDIAC ARDIAC OOUTUTPPUTUT is is maintained for up to maintained for up to 4 4
daysdays and then and then declines rapidlydeclines rapidly

2 - Arterial blood 2 - Arterial blood pressurepressure

Although Although CCARDIAC ARDIAC OOUTUTPPUTUT inc incrrease, yet ease, yet
Arterial Blood Arterial Blood Pressure is Pressure is decreaseddecreased in in
midtrimestermidtrimester to to increase again in 3rd increase again in 3rd
trimestertrimester

This is due to:1- - Decreased Peripheral Decreased Peripheral
resistanceresistance : :
(mainly affect diastolic B.P.) (mainly affect diastolic B.P.) due to :due to : vasodilatation + vasodilatation + increased metabolism + increased metabolism +
arterio-venous shunt at the arterio-venous shunt at the level of placenta .level of placenta .

2.2.- - Supine hypotensiSupine hypotensive syndromeve syndrome::
may develomay developp in late pregnancy while in late pregnancy while lying supine lying supine compression on compression on the the
IInferior nferior VVena ena CCavaava by the large by the large pregnant uteruspregnant uterus decreased venous decreased venous return return decreased Cardiac Output decreased Cardiac Output
and low B.P. to the extent that and low B.P. to the extent that fainting fainting may occurmay occur..
TreatmentTreatment: lateral recumbent position : lateral recumbent position

Vena Cava SyndromeVena Cava Syndrome

3. -3. - Decreased Decreased sensitivity of blood sensitivity of blood
vesselsvessels to to angiotensin II angiotensin II which is vasoconstrictorwhich is vasoconstrictor

• The posture of the pregnant The posture of the pregnant woman affects arterial blood woman affects arterial blood pressure. pressure.
• Typically, it is Typically, it is highest when she highest when she is sittingis sitting, , lowest when lying in lowest when lying in the lateral recumbent positionthe lateral recumbent position and intermediate when supine.and intermediate when supine.

Peripheral Peripheral VasodilatationVasodilatation

Regional blood flows Regional blood flows
- - the utero-placentalthe utero-placental flow, flow,
- - the renal bloodthe renal blood flow, flow,
- - the skinthe skin, particularly in the , particularly in the hands and feet + hands and feet + mammary mammary
glandgland
Peripheral VasodilatationPeripheral Vasodilatation

Renal blood flow → Renal blood flow → glomerular glomerular filtration increasefiltration increase favoring the oxygen favoring the oxygen supply and the amplification of some supply and the amplification of some
active processesactive processes..
The increase of glomerular filtration The increase of glomerular filtration contributes to the explanation of contributes to the explanation of
glycosuria, aminoaciduriaglycosuria, aminoaciduria and to the and to the increase of water-soluble vitamin increase of water-soluble vitamin
excretionexcretion..
Peripheral VasodilatationPeripheral Vasodilatation

blood flow to the skin, blood flow to the skin, particularly in the hands particularly in the hands and feet generally giving and feet generally giving the pregnant women a the pregnant women a
feeling of warmthfeeling of warmth
Peripheral VasodilatationPeripheral Vasodilatation

Peripheral VasodilatationPeripheral Vasodilatation
Increases the congestion of Increases the congestion of nasal mucosa leading to nasal mucosa leading to a common complaint of a common complaint of nasal obstruction and nasal obstruction and bleeding bleeding (epistaxis).(epistaxis).

3 - Venous pressure3 - Venous pressure

Increased venous pressure in Increased venous pressure in the lower limbs due to:the lower limbs due to:
1. 1. Back pressure from the compressed Back pressure from the compressed IInferior nferior VVena ena CCavaava by the pregnant by the pregnant uterus .uterus .
2.Mechanical pressure of the uterus on 2.Mechanical pressure of the uterus on pelvic veins .pelvic veins .
3.Increased venous return from internal 3.Increased venous return from internal iliac veins → increased pressure in iliac veins → increased pressure in external iliac veins .external iliac veins .

Increased venous pressure Increased venous pressure in the lower limbsin the lower limbs
Predisposes to:Predisposes to:
Oedema,Oedema,
varicose veinsvaricose veins
and pilesand piles

Oedema and varicose veins in the Oedema and varicose veins in the lower limbs & vulva are due tolower limbs & vulva are due to
1. - 1. - Venous pressure. Venous pressure.
2. - Relaxation of the smooth muscles in 2. - Relaxation of the smooth muscles in the wall of the veins by progesterone the wall of the veins by progesterone
3. - 3. - Osmotic pressure in blood. Osmotic pressure in blood.
4. - 4. - Capillary permeability (due to Capillary permeability (due to progesterone and aldosterone).progesterone and aldosterone).
5. - 5. - Interstitial pressure (Na retention). Interstitial pressure (Na retention).

IV - Respiratory IV - Respiratory systemsystem

(A) Anatomically:(A) Anatomically:
The enlarged The enlarged uterus displaces uterus displaces the diaphragmthe diaphragm up up
to 4 cm .to 4 cm .

This results in :This results in :1. 1. The diaphragmatic mobility The diaphragmatic mobility
is reduced and is reduced and respiration respiration becomes mainly thoracicbecomes mainly thoracic..
2. 2. Widen the subcostal angleWiden the subcostal angle and increases the transverse and increases the transverse diameter of the chest.diameter of the chest.

Respiratory functionsRespiratory functions
The respiratory rateThe respiratory rate
does not increase during does not increase during pregnancy from its pregnancy from its
normal rate of normal rate of 14 - 15 / 14 - 15 / minute.minute.

Overbreathing
(deep respiration)
occurs due to the effect of excess progesterone

Shortness of breathShortness of breath (the need to breath becomes a (the need to breath becomes a
conscious one)conscious one) and and dyspneadyspnea are common are common complaints of the pregnant complaints of the pregnant
women which may be due to women which may be due to unfamiliarity with low C02 unfamiliarity with low C02
tension in the alveolar tension in the alveolar capillariescapillaries . .

The vital capacityThe vital capacity
1.The inspiratory capacity1.The inspiratory capacity (Tidal volume + (Tidal volume +
inspiratory volume) inspiratory volume) is is decreased decreased in late in late
pregnancy pregnancy

2.The expiratory reserve 2.The expiratory reserve volumevolume
(maximum amount of air (maximum amount of air which can be expired after which can be expired after
normal expiration) is normal expiration) is reducedreduced
3.The residual volume3.The residual volume is is reducedreduced . .

The reduction in:The reduction in:1.The inspiratory capacity1.The inspiratory capacity 2.The expiratory reserve 2.The expiratory reserve
volumevolume
3.The residual volume3.The residual volume is not significantis not significant ..

4.4.The tidal volumeThe tidal volume : :
(amount of gas inspired (amount of gas inspired or expired in each or expired in each respiration) respiration) risesrises
through out pregnancy through out pregnancy by about 40 % .by about 40 % .

Hyperventilation is due Hyperventilation is due to increased tidal to increased tidal
volume not respiratory volume not respiratory raterate
►►a respiratory alkalosis a respiratory alkalosis takes placetakes place

V - Urinary systemV - Urinary system

(A) Kidney and kidney (A) Kidney and kidney function testsfunction tests
• Renal blood flow and glomerular filtration rate
increases by 50 %. This leads to increased
excretion

• Blood Tests:Blood Tests:1.1. There is There is serum creatinine serum creatinine (due to (due to
creatinine cleareance) creatinine cleareance)
serum uric acidserum uric acid..3. 3. blood urea blood urea..
4. 4. kidney excretion of glucose is due kidney excretion of glucose is due
to to filtration load and filtration load and renal renal threshold leading to threshold leading to renal renal glucosuria. glucosuria.

Therefore , in interpretating Therefore , in interpretating the results of kidney the results of kidney
function test you should function test you should take into consideration that take into consideration that
the lowest normal values the lowest normal values in non-pregnant statein non-pregnant state = =
the highest normal the highest normal values in pregnancyvalues in pregnancy

(B) Ureters(B) Ureters Dilatation of the ureters and renal Dilatation of the ureters and renal
pelvis due to:pelvis due to:1.1.Relaxation of the ureters Relaxation of the ureters by the effect of by the effect of
progesterone.progesterone.
2. 2. Pressure against the pelvic brim by the Pressure against the pelvic brim by the uterus uterus particularly on the right side due to particularly on the right side due to dextroposed uterus and dilatation of the dextroposed uterus and dilatation of the right ovarian vesselsright ovarian vessels

(C) Bladder and urethra(C) Bladder and urethra
• Frequency of micturitionFrequency of micturition
in early pregnancy due to:in early pregnancy due to: - Pressure on the bladder - Pressure on the bladder
by the enlarged uterus.by the enlarged uterus. - Congestion of the bladder - Congestion of the bladder
muscosa.muscosa.

VI - Gastrointestinal VI - Gastrointestinal tract tract
& liver& liver

1 - Gingivitis :1 - Gingivitis :
There is increased vascularity and tendency
for bleeding as well as hypertrophy of the
interdental papillae

• The gums may become The gums may become hyperemic and soft and may hyperemic and soft and may
bleedbleed when mildly traumatized, when mildly traumatized, as with a tooth brush. as with a tooth brush.
• Epulis of pregnancyEpulis of pregnancy
may develop.may develop.
Treated by dental hygiene and Treated by dental hygiene and cryosurgery for severe casescryosurgery for severe cases.

2 - Ptyalism:2 - Ptyalism:
• It is excessive salivation which is It is excessive salivation which is more common in association with more common in association with oral sepsis . oral sepsis .
• It is due to It is due to failure to swallowfailure to swallow saliva saliva and not due to increase in amount. and not due to increase in amount.
• Smoking is stopped and Smoking is stopped and anticholinergic drugs may helpanticholinergic drugs may help..

3 - Nausea and vomiting3 - Nausea and vomiting
Nausea (morning sickness) Nausea (morning sickness) and vomiting and vomiting
(emesis gravidarum) (emesis gravidarum) occur in early monthsoccur in early months

4 - Appetite changes4 - Appetite changes (longing or craving) (longing or craving)

• The pregnant woman dislikes The pregnant woman dislikes some foods and odours while some foods and odours while desires others desires others
• Reduced sensitivity of the Reduced sensitivity of the taste budstaste buds during pregnancy during pregnancy creates the desire for creates the desire for markedly sweet, sour, or salt markedly sweet, sour, or salt foods .foods .

(pica)(pica)Deviation may be so Deviation may be so
extreme to the extreme to the extent of eating extent of eating
blackboard chalk, blackboard chalk, coal or mudcoal or mud

5 - Indigestion 5 - Indigestion and flatulenceand flatulence

This is probably due to :This is probably due to :
1. - Decreased gastric acidity 1. - Decreased gastric acidity caused by regurgitation of caused by regurgitation of alkaline secretion from the alkaline secretion from the intestine to the stomach . intestine to the stomach .
2. - Decreased gastric motility 2. - Decreased gastric motility (progesterone effect).(progesterone effect).

6 - 6 - Pyrosis (Heart burnHeart burn)
Due to reflux of acidic Due to reflux of acidic gastric contents to the gastric contents to the
oesophagus oesophagus

The treatment includes :The treatment includes :
(a) (a) small frequent mealssmall frequent meals to to prevent overdistension of prevent overdistension of the stomach. The evening the stomach. The evening meal should be taken at meal should be taken at
least 3 hours before going least 3 hours before going to bed. to bed.

(b) (b) avoidavoid fatty foods, fatty foods, chocolate, and smoking, as chocolate, and smoking, as
these relax the lower these relax the lower esophageal sphincter. esophageal sphincter.
(c) the (c) the bed should be raisedbed should be raised at the head (15-20 cm), and at the head (15-20 cm), and
an extra pillow is used. an extra pillow is used.

(d) (d) Antacid Antacid PreparationsPreparations
containing aluminium containing aluminium hydroxide are hydroxide are
favoured.favoured.

7 - Constipation7 - Constipation
Due to:1. - Reduced motility of large 1. - Reduced motility of large
intestine intestine (progesterone effect).(progesterone effect).
2. - Increased water reabsorption 2. - Increased water reabsorption from large intestine from large intestine (aldosterone effect).(aldosterone effect).

7 - Constipation7 - Constipation
3. - Pressure on the pelvic colon by the pregnant uterus.
4. - Sedentary life during pregnancy .

It is treated byIt is treated by
(a) evacuation of the (a) evacuation of the bowel at the same bowel at the same
time each day time each day (bowel training)(bowel training)

(b) (b) diet rich in fiberdiet rich in fiber in in the form of vegetables, the form of vegetables, fruits, and bran fruits, and bran
(c) (c) milkmilk and avoid and avoid dehydration by dehydration by increasing fluid intake.increasing fluid intake.

(d) (d) minimize coffee and minimize coffee and teatea as they are diuretics as they are diuretics and cause dehydration.and cause dehydration.
(e) (e) increase physical increase physical activityactivity and avoid and avoid sedentary life. sedentary life.

(f) a (f) a mild laxativemild laxative may may be needed. be needed.
Liquid paraffin is better avoided Liquid paraffin is better avoided as it prevents absorption of fat as it prevents absorption of fat
soluble vitaminssoluble vitamins. .

In some women In some women iron iron
supplementationsupplementation may be the causemay be the cause

8 - Gall stones8 - Gall stones
More tendency to stone More tendency to stone formation due to atony formation due to atony and delayed emptying and delayed emptying
of the gall bladderof the gall bladder

9 - Haemorroids9 - Haemorroids

due to :due to :
1. - Mechanical pressure on the pelvic veins.
2. - Laxity of the walls of the veins by progesterone
3. - Constipation.

10 - Appendix10 - Appendix
Is displaced upwards and laterally (pain and tenderness due to
appendicitis is higher than in nonpregnant state)

AppendixAppendix

LiverLiver1. - Decreased albumin and Decreased albumin and
increased globulin resulting increased globulin resulting in in decreased A/G ratio decreased A/G ratio
2. - Increased heat labile 2. - Increased heat labile serum alkaline phosphatase .serum alkaline phosphatase .

Therefore both Therefore both A/G ratioA/G ratio and and heat labile alkaline heat labile alkaline
phosphatasephosphatase are not are not reliable as liver function reliable as liver function tests during pregnancytests during pregnancy
The functional disorders The functional disorders are minimal.are minimal.

VII - Metabolic VII - Metabolic changeschanges

(A) Weight gain
The average The average weight gain in weight gain in pregnancy is pregnancy is
10 - 12 kg10 - 12 kg

The increase The increase occurs mainly in occurs mainly in the second and the second and
third trimester at a third trimester at a rate of rate of 350 - 400 350 - 400
gm/ weekgm/ week

Out of the 11 kg weight gainOut of the 11 kg weight gain
6 kg is 6 kg is composed ofcomposed of maternal tissuesmaternal tissues (breasts, (breasts,
fat, blood and uterine fat, blood and uterine tissues), and tissues), and
5 kg of fetal tissue, placenta 5 kg of fetal tissue, placenta and amniotic fluid and amniotic fluid

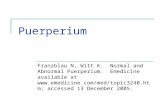
Maternal TissuesMaternal TissuesIncreases during weeks of Pregnancy
0
200
400
600
800
1000
1200
1400
1600
10 wk 20 wk 30 wk 40 wk
UterusMammary GlandPlasma Volume
King JC. Am J Clin Nutr 71 (5(S));2000.

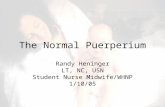
Products of ConceptionProducts of ConceptionIncreases during weeks of PregnancyIncreases during weeks of Pregnancy
0
500
1000
1500
2000
2500
3000
3500
10 wk 20 wk 30 wk 40 wk
FetusPlacentaAmniotic Fluid
King JC. Am J Clin Nutr 71 (5(S));2000.

Out of the 11 kg Out of the 11 kg weight gainweight gain::
77 kg are waterkg are water,,33 kg fat andkg fat and11 kg proteinkg protein

)B) Water metabolismB) Water metabolism
There is tendency to There is tendency to water retention water retention secondary to secondary to
sodium retentionsodium retention

(C) Protein metabolism(C) Protein metabolism
There is tendency for There is tendency for nitrogen retention nitrogen retention
(+ nitrogen balance)(+ nitrogen balance) for fetal and maternal for fetal and maternal
tissue formation tissue formation

(D) Carbohydrate metabolism(D) Carbohydrate metabolism
Pregnancy is potentially Pregnancy is potentially diabetogenicdiabetogenic
- - Alimentary glucosuriaAlimentary glucosuria may may occur in occur in earlyearly pregnancy. pregnancy.
- - Renal glucosuriaRenal glucosuria may occur in may occur in the the middlemiddle of pregnancy. of pregnancy.

(E) Fat metabolism(E) Fat metabolism
There is increase of plasma lipids with
tendency to acidosis (Human Placental Lactogen action)

(F) Mineral metabolism
There is increased There is increased demand for iron, demand for iron,
calcium, phosphate calcium, phosphate and magnesium and magnesium

IX - Endocrine IX - Endocrine systemsystem

1 - Anterior pituitary1 - Anterior pituitary

1. - Increase in size 1. - Increase in size more than increase in more than increase in
vascularity vascularity This renders anterior This renders anterior
pituitary liable for pituitary liable for ischaemia.ischaemia.

22. - . - Prolactin levelProlactin level increases increases up to 150 ng /ml at term to up to 150 ng /ml at term to ensure lactation.ensure lactation.
3. 3. The ACTH and MSH The ACTH and MSH secretion increases.secretion increases.

2 - Posterior pituitary2 - Posterior pituitary
Does not hypertrophy, Does not hypertrophy, but increase its but increase its
oxytocinoxytocin release near release near term.term.
OXT is synthesized in the hypothalamus (supraoptic and
paraventricular nuclei).

3 - Thyroid gland3 - Thyroid gland
There is diffuse There is diffuse slight slight enlargement enlargement
of the glandof the gland

Gland activity is Gland activity is as as evidenced by normal free T4 evidenced by normal free T4 (although total T4 (although total T4 ) due to ) due to thyroid binding globulin thyroid binding globulin
(TBG) , (TBG) ,
BBasal asal MMetabolism etabolism RRateate (20 (20 %),%), total T3 total T3, , protein protein bound iodine andbound iodine and TSHTSH

4 - Parathyroid gland4 - Parathyroid gland
Hypertrophy due to Hypertrophy due to increased demand increased demand
for Calciumfor Calcium

5 - Suprarenal gland5 - Suprarenal gland
HypertrophyHypertrophy particularly the particularly the cortex cortex resulting in increased resulting in increased glucocorticoids glucocorticoids (cortisone)(cortisone)
and increased and increased mineralocorticoids mineralocorticoids
(aldosterone)(aldosterone)

5 - Suprarenal gland5 - Suprarenal gland
• Under the influence of estrogens, Under the influence of estrogens, transcortin (cortisol-binding transcortin (cortisol-binding
globulin) levels rise and, together globulin) levels rise and, together with cortisol, produce a slight with cortisol, produce a slight
hypercorticismhypercorticism.. • As early as 15 weeks of normal pregnancy, the maternal adrenal secretes considerably increased
amounts of aldosterone.

6 - Insulin6 - Insulin
increased mainly increased mainly due to HPL due to HPL (anti - (anti - insulin hormone)insulin hormone)

7 -Ovaries7 -Ovaries
corpus luteum of corpus luteum of pregnancypregnancy
functions till 8-12 wks. functions till 8-12 wks. when its function is taken when its function is taken
by the placentaby the placenta

4 4 - Pigmentation- Pigmentation
Due to melanocyte Due to melanocyte stimulating hormone stimulating hormone

• In the faceIn the face = = chloasma chloasma gravidarum = mask of gravidarum = mask of
pregnancypregnancy a butterfly pigmentation a butterfly pigmentation
on the cheeks and nose. on the cheeks and nose. It usually disappears few It usually disappears few
months after labourmonths after labour. .

Linea nigraLinea nigra

•In abdomenIn abdomen::
Linea Nigra=Linea Nigra= pigmentation in pigmentation in
midline below the midline below the umbilicus umbilicus

Stria gravidarumStria gravidarum
pigmentation in the lower pigmentation in the lower abdomen ,abdomen ,
flanks , inner thighs , flanks , inner thighs , buttocks & breast and buttocks & breast and increase as pregnancy increase as pregnancy
advancesadvances


It starts bluish It starts bluish (stria rubra)(stria rubra) , , then becomes pale to become then becomes pale to become
white white (stria albicans)(stria albicans) after after delivery , which persists delivery , which persists
(primigravida has stria rubra (primigravida has stria rubra only, while multigravida has only, while multigravida has
both S.R and S.A) both S.R and S.A)

It is due mainly not to It is due mainly not to mechanical stretchingmechanical stretching but to but to
increased glucocorticoidsincreased glucocorticoids which results in rupture of which results in rupture of
the elastic fibres in the the elastic fibres in the dermis and exposure of the dermis and exposure of the
vascular subcutaneous vascular subcutaneous tissuestissues

5 - Secretions5 - Secretions
increase in sweat increase in sweat and sebaceous and sebaceous glands activityglands activity

(B) Breast signs(B) Breast signs

Breast changesBreast changes

1. – Early pregnancy :1. – Early pregnancy :
increased size & vascularity increased size & vascularity (dilated veins)(dilated veins), mastodynia , mastodynia
may be present which ranges may be present which ranges from tingling to frank pain from tingling to frank pain
due to hormonal responses of due to hormonal responses of the mammary ducts and the mammary ducts and
alveolar systemalveolar system

2. – end of I trim. :2. – end of I trim. :
increased pigmentation of the increased pigmentation of the nipple & areola and nipple & areola and
prominence of prominence of Montgomery Montgomery tubercles -tubercles - nonpigmented nonpigmented
nodules around the nodules around the primary primary areola (12 - 20)areola (12 - 20)
enlarged sebaceous glandsenlarged sebaceous glands

3. - 3. - Midpregnancy:Midpregnancy: secretion of secretion of colostrumcolostrum
(thick yellowish (thick yellowish fluid) which can be fluid) which can be expressed from the expressed from the
nipplenipple

4. - 4. - Midpregnancy:Midpregnancy:
a pigmented area a pigmented area appears around the appears around the
primary areola called primary areola called the the secondary areolasecondary areola

XII. Neurologic XII. Neurologic SystemSystem

1. 1. HeadacheHeadache
It is relatively common, and It is relatively common, and attributed to intracranial attributed to intracranial vasodilatation caused by vasodilatation caused by
oestrogen and oestrogen and progesteroneprogesterone

2. 2. FaintingFainting
It results from lowering It results from lowering of blood pressure due to of blood pressure due to
vasodilatation which vasodilatation which occur in pregnancyoccur in pregnancy

3. 3. InsomniaInsomnia
During pregnancy some During pregnancy some women are sleepy and women are sleepy and
depressed, others may be depressed, others may be irritable and suffer irritable and suffer
insomniainsomnia

LEUCORRHEALEUCORRHEA
The normal vaginal The normal vaginal discharge increases discharge increases
during pregnancy because during pregnancy because of excess oestrogen and of excess oestrogen and may form a complaint may form a complaint

However, a pathological However, a pathological discharge, e.g., discharge, e.g.,
monilial infectionsmonilial infections which is common in which is common in pregnancy must be pregnancy must be
excluded.excluded.