
Maternal hypertensive disorders during pregnancy and the mental ...
10/4/2017
1
Maternal Mental Health—Pharmacology for Primary Care
Debra Scrandis, PhD, CRNP‐PMHAssociate ProfessorUniversity of Maryland School of NursingBaltimore, MD [email protected]
Objectives
1. Prescribe psychotropic medications for anxiety and depression in postpartum women
2. Analyze existing evidence on psychotropic medication use in lactation
3. Identify appropriate timing for psychiatric referral for postpartum women
Who’s at Risk?
• Disorder in pregnancy
• Personal history
• Family history
• Biological Processes
• Adverse life events
Biaggi et al, J Affect Disord.2016; 191:62–77; Yim et al. Annu Rev Clin Psychol. 2015. 11:99–137
10/4/2017
2
Postpartum Mood Disorders
• Major Depressive Disorder
• Bipolar Disorder
• Psychotic Disorder
What’s the difference from Postpartum Blues?
Major Depressive Disorder• Depressed mood, lack of interest in activities
• Sleep & appetite disturbances, weight changes, low energy, poor concentration, hopelessness, suicidal ideation
I was so excited to have a baby girl. I couldn’t shake the tears and sadness that got deeper and darker every day. I had a non existent appetite but forced myself since I was nursing. I lost 30 lbs. in the first month. I couldn’t sleep. I wanted to run away. I thought I was the worst mother on the face of the earth.
Brain and Psychiatric Disorders
Monoamine hypothesis
– Deficiency of individual neurotransmitters
– Serotonin (5HT), Norepinephrine (NE), Dopamine (DA)
Gene expression
– Neurotransmitter receptors, downregulation
– Decreased neurotransmitters upregulation of postsynaptic neurotransmitter receptors
Brain circuitry
– Different neurotransmitters depending on patient symptoms
10/4/2017
3
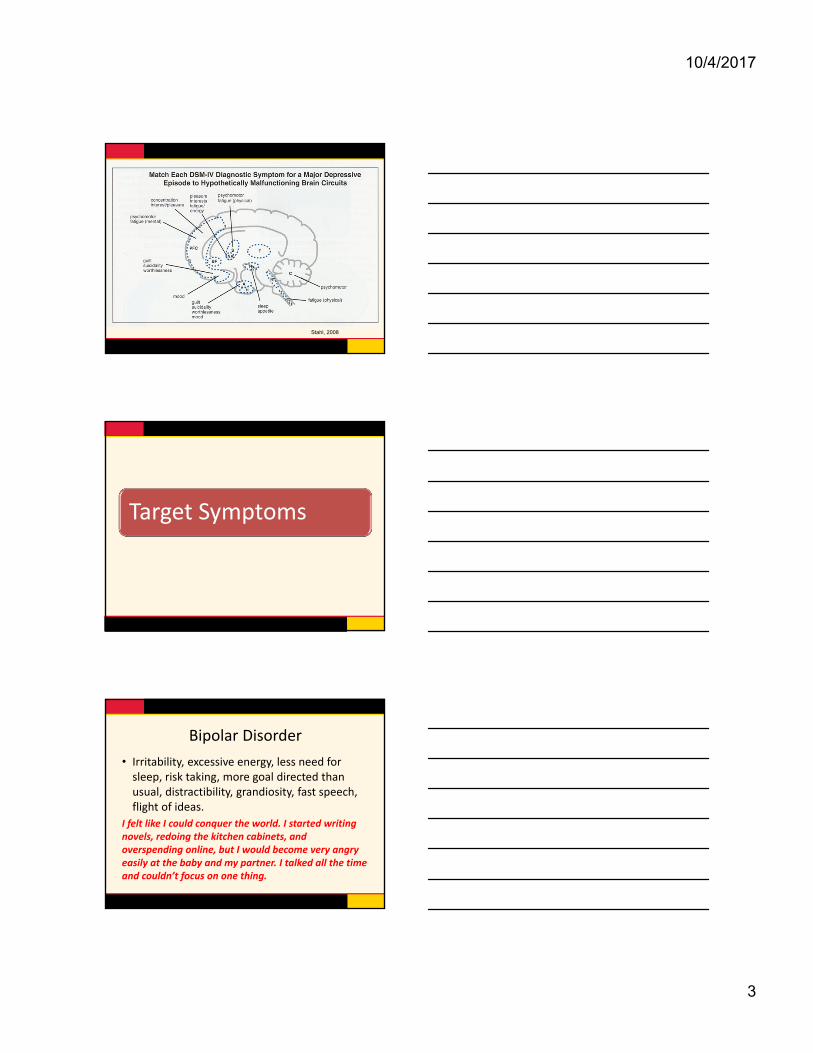
Stahl, 2008
Target Symptoms
Bipolar Disorder
• Irritability, excessive energy, less need for sleep, risk taking, more goal directed than usual, distractibility, grandiosity, fast speech, flight of ideas.
I felt like I could conquer the world. I started writing novels, redoing the kitchen cabinets, and overspending online, but I would become very angry easily at the baby and my partner. I talked all the time and couldn’t focus on one thing.
10/4/2017
4
Psychotic Disorder
• Visual or auditory hallucinations
• Delusional thinking about need to kill baby
My wife began to withdraw into her own world. She became less communicative, more confused and suspicious. I had to practically carry her to get help.
Screening and History
• Edinburgh Postnatal Depression Scale
• How often have you felt this way since your baby was born?
– 5 point scale—never to always
– Depressed mood, felt hopeless, and slowed down
• Consider the Mood Disorder Questionnaire– www.dbsalliance.org/pdfs/MDQ.pdf
Cox et al, Br J Psychiatry. 1987;150, 782-786 ; O’Hara et al, J Womens Health. 2012; 21(12): 1237-1243.
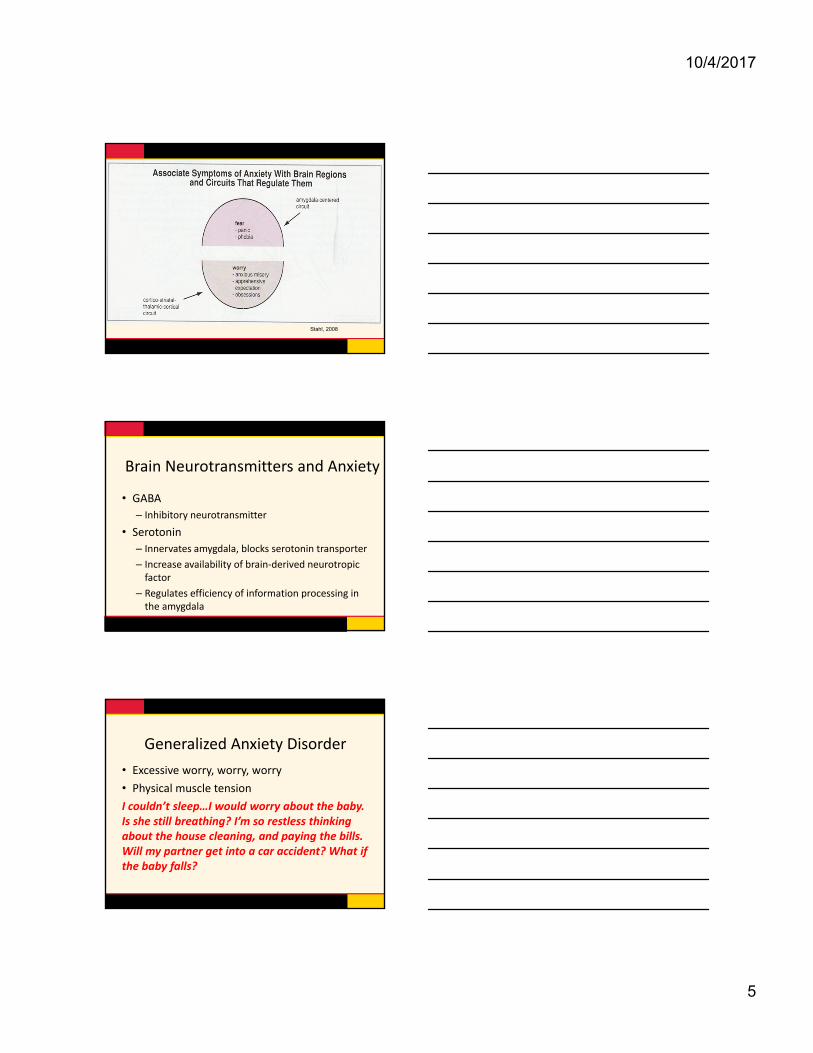
Postpartum Anxiety
• Generalized Anxiety Disorder (worry)
• Panic Disorder (fear)
• Obsessive Compulsive Disorder (worry)
• Posttraumatic Stress Disorder (fear)
10/4/2017
5
Stahl, 2008
Brain Neurotransmitters and Anxiety
• GABA
– Inhibitory neurotransmitter
• Serotonin
– Innervates amygdala, blocks serotonin transporter
– Increase availability of brain‐derived neurotropic factor
– Regulates efficiency of information processing in the amygdala
Generalized Anxiety Disorder
• Excessive worry, worry, worry
• Physical muscle tension
I couldn’t sleep…I would worry about the baby. Is she still breathing? I’m so restless thinking about the house cleaning, and paying the bills. Will my partner get into a car accident? What if the baby falls?
10/4/2017
6
Panic Disorder• Physical symptoms (SOB, nausea, palpitations) “out of the blue”
• Avoidance behaviors
• Fear of dying and subsequent panic attacks
At 3 weeks postpartum, I stopped leaving the house except for pediatrician appointments. I was afraid to have panic attacks in the store and not be able to care for my baby.
Obsessive Compulsive Disorder• Intrusive, repetitive, and persistent thoughts or mental pictures, often about hurting or killing the baby
• Tremendous sense of horror and disgust about these thoughts.
Each time I went to the balcony I would clutch the baby tightly until I was in a room with the door closed. Only then did I know he was safe one more time from me dropping him over.
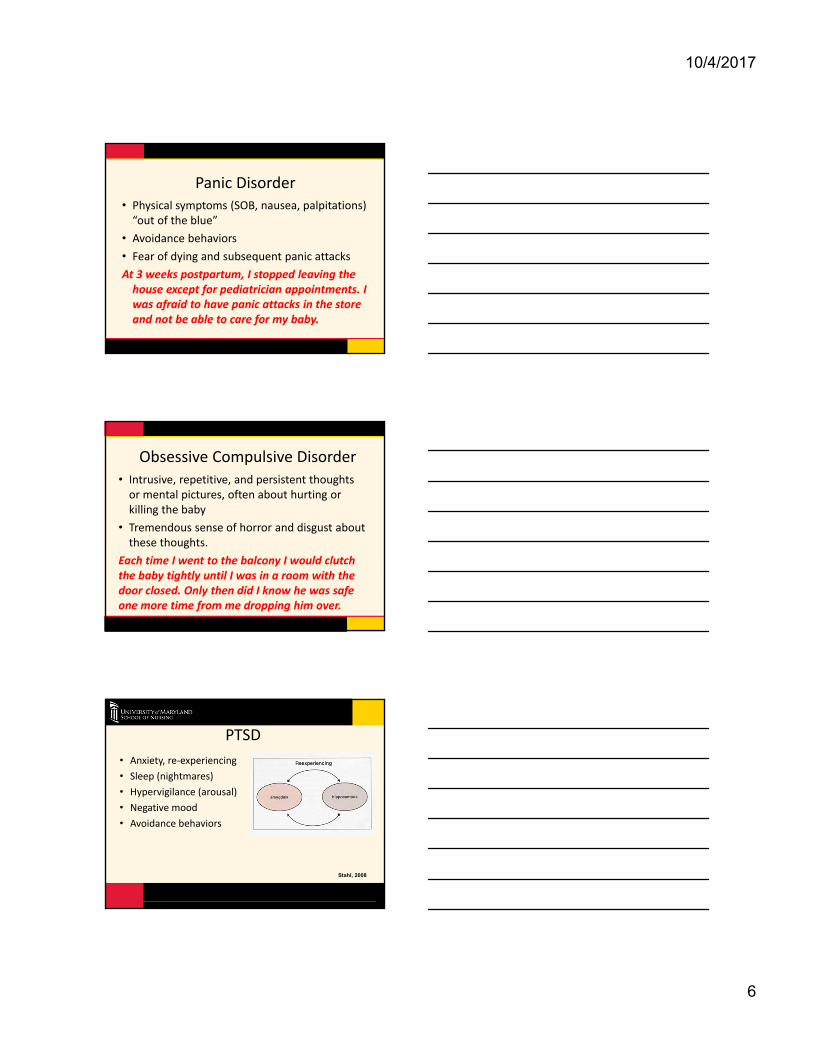
• Anxiety, re‐experiencing
• Sleep (nightmares)
• Hypervigilance (arousal)
• Negative mood
• Avoidance behaviors
PTSD
Stahl, 2008
10/4/2017
7
Anxiety Screens
• How often have you felt this way since your baby was born? 5 point scale—never to always
– panicky, restless, problems sleeping
• GAD‐Q‐IV
– 9 questions (5 yes/no, 2 open ended, 2 severity)
– Range 0‐12– https://adaa.org/screening‐generalized‐anxiety‐disorder‐gad
GAD-Q-IV=Generalized Anxiety Disorder Questionnaire; O’Hara et al. J Womens Health. 2012; 21(12): 1237-1243.Pierson et al. Psychol Assess. 2017: http://dx.doi.org/10.1037/pas0000443
FDA ApprovedSSRIs
– fluoxetine (Prozac), sertraline (Zoloft), paroxetine (Paxil), fluvoxamine (Luvox), citalopram (Celexa), escitalopram (Lexapro)
– All selective & potent inhibition of 5HT reuptake
– Auto receptor downregulation
– Side effects related to acute actions of 5HT
– Targets negative mood symptoms well
Bold approved for anxiety disordersSSRIs=Selective Serotonin Reuptake Inhibitors5HT=serotonin
SSRIs Side Effects
• Stimulation of different 5HT receptors• Basal ganglia—motor movements
• Spinal cord—sexual dysfunction
• Brainstem—sleep disturb slow wave sleep
• Mesocortical pleasure centers—decrease DA—decrease libido
• Hypothalamus or brainstem—nausea and vomiting
• Attenuate over time
SSRIs=Selective Serotonin Reuptake Inhibitors; 5HT=Serotonin; DA=Dopamine
10/4/2017
8
Not All Are Same
• Fluoxetine (Prozac)
– 5HT2C receptor antagonist and NE/DA disinhibiting
– Generally activating (hypersomnia, apathy, fatigue)
– Long half life 2‐3 days
• Sertraline (Zoloft)
– DA transporter inhibition
– Sigma 1 receptor binding (anxiolytic actions)
– Short half life
NE=Norepinephine; DA=Dopamine
• Paroxetine (Paxil)
– Muscarinic anticholinergic and NET inhibitory (anxiety symptoms)
– Withdrawal symptoms
• Fluvoxamine (Luvox)
– Sigma 1 receptor binding properties
– Anxiolytic properties
NET = Norepinephrine Transporter
• Citalopram (Celexa)
– Mild antihistamine properties
• Escitalopram (Lexapro)
– Removes antihistamine properties
– Pure SERT inhibition
– Fewest CYP 450 drug interactions
SERT=serotonin transporter; CYP=Cytochrome
10/4/2017
9
Selective Norepinephrine Reuptake Inhibitors
Combines SERT inhibition and inhibition of the NET increasing DA in PFC
• Venlafaxine XR (Effexor)
• Desvenlafaxine XR (Pristiq)
• Duloxetine (Cymbalta): anxiety disorders; lower incidence of HTN
SERT=serotonin transporter; DA=dopamine; PFC=prefrontal cortex; HTN=hypertension
Side Effects SNRIs
• Cerebellum—motor activation/tremor
• Brainstem—alter blood pressure
• Heart—pulse rate
SNRIs=selective norepinephrine reuptake inhibitors
NE and DA Reuptake Inhibitors
• Bupropion (Wellbutrin)
– Improvements in loss of happiness, joy interest, pleasure, energy, enthusiasm, alertness and self confidence
– Avoid in highly anxious patients
NE=norepinephrine; DA=dopamine
10/4/2017
10
Alpha 2 antagonist and SNDIsMirtazapine (Remeron)
– Release of 5HT and NE through alpha 2 receptors
– Release of dopamine
– Not cause sexual side effects
– NE and DA disinhibitor
– Improve insomnia, anxiety
– Weight gain, drowsiness more likely with H1 antihistamine properties
5HT=serotonin; NE=norepinephrine; H1=histamine 1
Newer Medications
• Vortioxetine (Trintellix)
– No sedation, long ½ life
• Vilazdone (Viibryd)
• Initial activation
• Co morbid anxiety
Trazodone
• Block 5HT 2A and 2 C receptors and reuptake
• High doses for antidepressant
• Low dose for insomnia
5HT=serotonin
10/4/2017
11
Tricyclic Antidepressants
Imipramine, nortriptyline
– Sedation, weight gain—blockade of H1 receptors
– Dry mouth, blurred vision, urinary retention, constipation—blockade of muscarinic cholinergic receptors
– Orthostatic hypotension, dizziness—alpha 1 adrenergic receptors.
H1= histamine 1
L‐methylfolate
• Derived from folate
• Regulator of trimonoamine neurotransmitter synthesis
• Only form of folate passes into the brain
How to Choose?
• Presenting symptoms
• Treatment history
• Does side effects help with symptoms?
• Breastfeeding considerations
10/4/2017
12
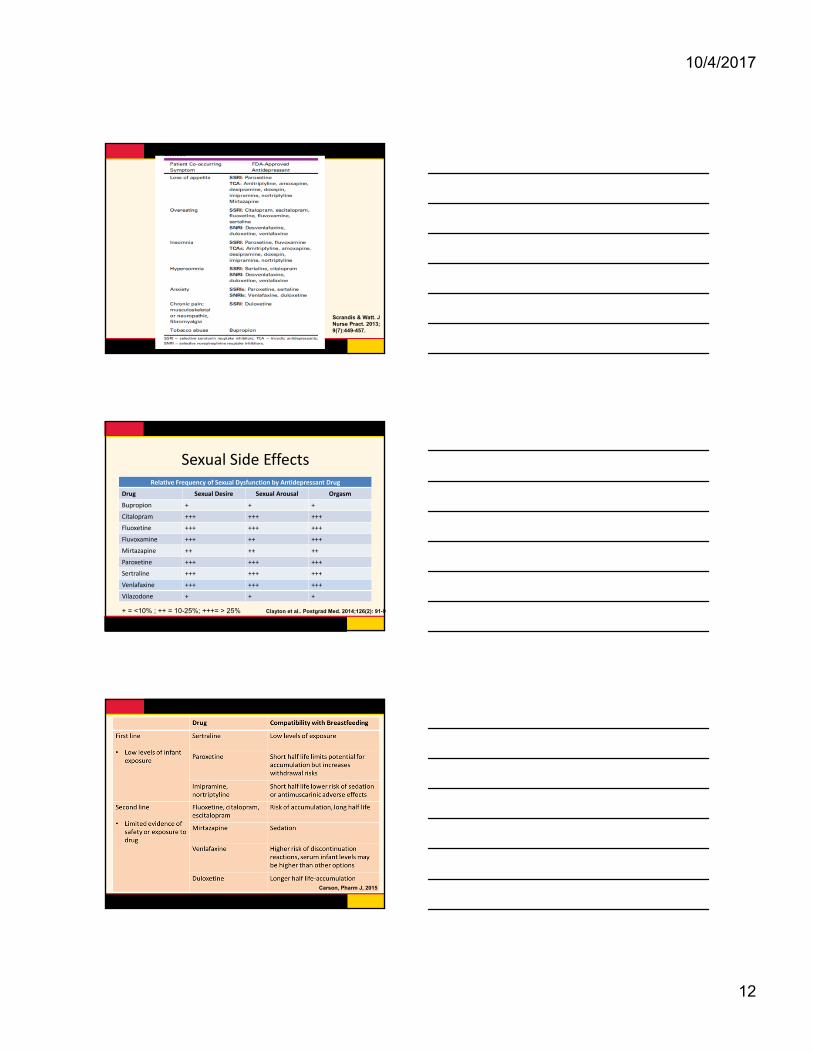
Scrandis & Watt. J Nurse Pract. 2013; 9(7):449-457.
Sexual Side EffectsRelative Frequency of Sexual Dysfunction by Antidepressant Drug
Drug Sexual Desire Sexual Arousal Orgasm
Bupropion + + +
Citalopram +++ +++ +++
Fluoxetine +++ +++ +++
Fluvoxamine +++ ++ +++
Mirtazapine ++ ++ ++
Paroxetine +++ +++ +++
Sertraline +++ +++ +++
Venlafaxine +++ +++ +++
Vilazodone + + +
+ = <10% ; ++ = 10-25%; +++= > 25% Clayton et al.. Postgrad Med. 2014;126(2): 91-9
Carson, Pharm J, 2015
10/4/2017
13
CZ 23 year old G2P2 married Jewish
• Feels overwhelmed with caring for 3 year old & 5 month old infant for the past 3 months‐teary, depressed mood, poor appetite, anhedonia, irritable with children.
• Difficulty with concentration. Denies SI but wishes she could “get away”.
• Feels guilt for being upset with children. Anxious. Poor sleep, especially onset. Husband reports “she complains a lot”.
Therapy weekly & exclusively breastfeeding
CZ
FH: anxiety in mother
Past psych: denies with first child
MDD single episode, moderate with anxious distress
Paroxetine 20mg dailyMDD= major depressive disorder
1 month follow up
• Still depressed, slight improvement. Overwhelmed and anxious. Ongoing irritability
• Too much sedation and lack of energy
• Wean paroxetine and changed to sertraline 50mg x 7 days then increase to 75 mg daily
• Added clonazepam 0.5mg as needed at bedtime
• 2 week follow‐up—increased to 100mg daily
10/4/2017
14
Augmentation
Benzodiazepines
•Short half life and no active metabolites
– Lorazepam
– Clonazepam
– Avoid diazepam (Valium)
•Primary concern—withdrawal, sedation
•USE SHORT TERM
HypnoticsFortinguerra et al. Pediatr. 2009; 124:e547.
Phone call from husband• Reports patient with elevated mood, not sleeping, spending money online
• “She is acting different”.
• Reports previous episodes in past. Uncle with Bipolar disorder
Refer**Therapy (CBT)
•Medical emergency—psychotic disorder
•Bipolar manic/hypomanic episode
•Suicidal, poor judgment
•OCD, PTSD
•Atypical symptoms (irritability, distractibility, agitation)
•Failed 2 adequate doses and adequate trials of antidepressants
Hofmann et al. Cognit Ther Res. 2012;26(5): 427-440.
10/4/2017
15
Maryland• Develop up to date evidence based information for health care facilities and providers
• Identify and develop training programs that improve identification of postpartum depression and other mood/anxiety disorders
• Expand the existing BHIPP program to assist specific providers in addressing emotional and mental health needs of pregnant and postpartum women
BHIPP=Behavioral Health Integration in Pediatric Primary Care (www.mdbhipp.org)
ReferencesBennett, S.S. & Indman P. (2003). Beyond the blues: A guide to understanding and treating prenatal and postpartum depression. San Jose, CA: Moodswings.
Carson, N. (2015). Antidepressant use during breastfeeding. Pharm J. Retrieved at pharmaceutical‐joujnral.com/learning/learning‐article/antidepressant‐use‐during‐breastfeeding/20069296.article.
Clayton AH, Croft HA, Handiwala L. Antidepressants and sexual dysfunction: mechanisms and clinical implications. Postgrad Med. 2014; 126(2): 91‐99.
Cox, J.L., Holden, J.M., & Sagovsky, R. Detection of postnatal depression: Development of the 10‐item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987;150, 782‐786 .
Fortinguerra F, Clavenna, A, & Bonati M.. Psychotropic drug use during breastfeeding: A review of the evidence. Pediatr. 2009; 124, e547.
Hofmann SG, Asnaani A, Vonk IJJ et al. The efficacy of cognitive behavioral therapy: A review of meta‐analyses. Cognit Ther Res. 2012; 26(5): 427‐440.
ReferencesKimmel MC, Meltzer‐Brody S. (2017). Safety of infant exposure to antidepressants and benzodiazepines through breastfeeding. UpToDate. Topic 1720, version 29.0
O’Hara M.W, Stuart S, Watson D, Dietz P.M, Farr SL, D’Angelo D. Brief scales to detect postpartum depression and anxiety symptoms. J Womens Health. 2012; 21(12): 1237‐1243.
Pierson ME, Prenoveau JM, Craske, MG, Netsi E & Stein A. (2017, February 20). Psychometric properties of the generalized anxiety disorder questionnaire‐IV (GAD‐Q‐IV) in postpartum mothers. Psychol Assess: Advance online publication. http://dx.doi.org/10.1037/pas0000443
Scrandis DA, Watt M. Antidepressant medication management in primary care: Not just another pill. J Nurse Pract. 2013; 9(7):449‐457.
Stahl, S.M. (2008). Stahl’s essential psychopharmacology: Neuroscientific basis and practical applications. 3rd
ed. New York: Cambridge.


















