Mast Cells: Potential Positive and Negative Roles in Tumor ...Masters of Immunology Mast Cells:...
12
Masters of Immunology Mast Cells: Potential Positive and Negative Roles in Tumor Biology Thomas Marichal 1 , Mindy Tsai 1 , and Stephen J. Galli 1,2 Abstract Mast cells are immune cells that reside in virtually all vascularized tissues. Upon activation by diverse mechanisms, mast cells can secrete a broad array of biologically active products that either are stored in the cytoplasmic granules of the cells (e.g., histamine, heparin, various proteases) or are produced de novo upon cell stimulation (e.g., prostaglandins, leukotrienes, cytokines, chemokines, and growth factors). Mast cells are best known for their effector functions during anaphylaxis and acute IgE-associated allergic reactions, but they also have been implicated in a wide variety of processes that maintain health or contribute to disease. There has been particular interest in the possible roles of mast cells in tumor biology. In vitro studies have shown that mast cells have the potential to influence many aspects of tumor biology, including tumor development, tumor-induced angiogenesis, and tissue remodeling, and the shaping of adaptive immune responses to tumors. Yet, the actual contributions of mast cells to tumor biology in vivo remain controversial. Here, we review some basic features of mast cell biology with a special emphasis on those relevant to their potential roles in tumors. We discuss how using in vivo tumor models in combination with models in which mast cell function can be modulated has implicated mast cells in the regulation of host responses to tumors. Finally, we summarize data from studies of human tumors that suggest either beneficial or detrimental roles for mast cells in tumors. Cancer Immunol Res; 1(5); 269–79. Ó2013 AACR. Disclosure of Potential Conflicts of Interest No potential conflicts of interest were disclosed. CME Staff Planners' Disclosures S.J. Galli has an ownership interest in Atossa Genetics, Inc., for which he serves on the board of directors. No potential conflicts of interest were disclosed by the other authors. Learning Objectives Upon completion of this activity, the participant should acquire a basic knowledge of the heterogeneity of macrophages, their roles in homeostasis, infection, and in the maintenance of organ integrity. A better understanding of the cellular ontogeny and tissue regulation of this group of circulating and tissue-resident hematopoietic cells of myeloid origin, how they balance between promoting immune tolerance during steady state, and responding to tissue damage and inflammation during infection will lead to the development of more specific and effective therapeutics. Acknowledgment of Financial or Other Support This activity does not receive commercial support. General Aspects of Mast Cell Biology Paul Ehrlich described mast cells in his doctoral thesis in 1878, identifying them in human tissues as connective tissue cells containing purple intracellular granules when stained with aniline blue; Ehrlich also reported that mast cells were particularly abundant in some tumors (1). In 1891, Ehrlich's student, Westphal, observed that in certain human tumors, mast cells were mainly present at the periphery of the tumor (2). These early observations have been confirmed and extend- ed many times since then (Fig. 1), suggesting that mast cells may be involved in tumor biology. Today, mast cells are mainly thought of as critical effector cells in antigen-induced anaphylaxis and other acute IgE- dependent allergic reactions, responses initiated when antigen crosslinks antigen-specific IgE antibodies bound to high-affin- ity FceRI receptors on the mast cell surface, thereby triggering mast cell activation (3). However, mast cells are also thought to represent versatile cells that can have effector or immuno- modulatory functions in both innate and adaptive immunity, Authors' Affiliations: Departments of 1 Pathology and 2 Microbiology and Immunology, Stanford University School of Medicine, Stanford, California Corresponding Author: Stephen J. Galli, Department of Pathology, L-235, Stanford University School of Medicine, 300 Pasteur Drive, Stanford, CA 94305-5324. Phone: 650-723-7975; Fax: 650-725-6902; E-mail: [email protected] doi: 10.1158/2326-6066.CIR-13-0119 Ó2013 American Association for Cancer Research. Cancer Immunology Research www.aacrjournals.org 269 on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Transcript of Mast Cells: Potential Positive and Negative Roles in Tumor ...Masters of Immunology Mast Cells:...

Masters of Immunology
Mast Cells: Potential Positive and Negative Roles in TumorBiology
Thomas Marichal1, Mindy Tsai1, and Stephen J. Galli1,2
AbstractMast cells are immune cells that reside in virtually all vascularized tissues. Upon activation by diverse
mechanisms, mast cells can secrete a broad array of biologically active products that either are stored in thecytoplasmic granules of the cells (e.g., histamine, heparin, various proteases) or are produced de novo upon cellstimulation (e.g., prostaglandins, leukotrienes, cytokines, chemokines, and growth factors). Mast cells are bestknown for their effector functions during anaphylaxis and acute IgE-associated allergic reactions, but they alsohave been implicated in a wide variety of processes that maintain health or contribute to disease. There has beenparticular interest in the possible roles of mast cells in tumor biology. In vitro studies have shown that mast cellshave the potential to influence many aspects of tumor biology, including tumor development, tumor-inducedangiogenesis, and tissue remodeling, and the shaping of adaptive immune responses to tumors. Yet, the actualcontributions of mast cells to tumor biology in vivo remain controversial. Here, we review some basic features ofmast cell biology with a special emphasis on those relevant to their potential roles in tumors. We discuss howusing in vivo tumor models in combination with models in which mast cell function can be modulated hasimplicated mast cells in the regulation of host responses to tumors. Finally, we summarize data from studiesof human tumors that suggest either beneficial or detrimental roles formast cells in tumors. Cancer Immunol Res;1(5); 269–79. �2013 AACR.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
CME Staff Planners' Disclosures
S.J. Galli has an ownership interest in Atossa Genetics, Inc., for which he serves on the board of directors. No potential conflicts of interest
were disclosed by the other authors.
Learning ObjectivesUpon completion of this activity, the participant should acquire a basic knowledge of the heterogeneity of macrophages, their roles in
homeostasis, infection, and in themaintenance of organ integrity. A better understanding of the cellular ontogeny and tissue regulation of
this group of circulating and tissue-resident hematopoietic cells of myeloid origin, how they balance between promoting immune
tolerance during steady state, and responding to tissue damage and inflammation during infection will lead to the development of more
specific and effective therapeutics.
Acknowledgment of Financial or Other SupportThis activity does not receive commercial support.
General Aspects of Mast Cell BiologyPaul Ehrlich described mast cells in his doctoral thesis in
1878, identifying them in human tissues as connective tissuecells containing purple intracellular granules when stainedwith aniline blue; Ehrlich also reported that mast cells were
particularly abundant in some tumors (1). In 1891, Ehrlich'sstudent, Westphal, observed that in certain human tumors,mast cells were mainly present at the periphery of the tumor(2). These early observations have been confirmed and extend-ed many times since then (Fig. 1), suggesting that mast cellsmay be involved in tumor biology.
Today, mast cells are mainly thought of as critical effectorcells in antigen-induced anaphylaxis and other acute IgE-dependent allergic reactions, responses initiated when antigencrosslinks antigen-specific IgE antibodies bound to high-affin-ity FceRI receptors on the mast cell surface, thereby triggeringmast cell activation (3). However, mast cells are also thought torepresent versatile cells that can have effector or immuno-modulatory functions in both innate and adaptive immunity,
Authors' Affiliations: Departments of 1Pathology and 2Microbiology andImmunology, Stanford University School of Medicine, Stanford, California
CorrespondingAuthor:Stephen J.Galli, Department of Pathology, L-235,Stanford University School of Medicine, 300 Pasteur Drive, Stanford, CA94305-5324. Phone: 650-723-7975; Fax: 650-725-6902; E-mail:[email protected]
doi: 10.1158/2326-6066.CIR-13-0119
�2013 American Association for Cancer Research.
CancerImmunology
Research
www.aacrjournals.org 269
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

and a wide variety of additional possible mast cell functionshave been proposed, spanning many aspects of health, hostdefense, and disease (4–6).
Mast cells are long-lived secretory cells derived fromhematopoietic precursors that ordinarily are found only insmall numbers in the blood but that complete their differen-tiation andmaturation in the microenvironments of almost allvascularized tissues (7–9). Like cells in the monocyte lineage,mast cells can proliferate after appropriate stimulation (10). Inaddition, increased recruitment, survival, and maturation ofmast cell progenitors may also contribute to the local expan-sion of mast cell populations in the tissues (8). Mature mastcells are particularly abundant in tissues and organs exposedto the external environment, such as the skin, the lung, and thegut, and are often located close to potential targets of theirmediators, such as epithelia and glands, smooth muscle cells,fibroblasts, blood and lymphatic vessels, and nerves (8).
During IgE-associated biologic responses, the antigen-dependent cross-linking of antigen-specific IgE bound to FceRIon the plasmamembrane ofmast cells induces the aggregationof FceRI, thereby activating downstream signaling events thatlead to the secretion of biologically active products implicatedin allergic reactions (11). Following antigen binding, mast cellsvery rapidly release into the extracellular space mediatorsprestored in their cytoplasmic granules, for example, vasoac-tive amines (histamine and serotonin), neutral proteases(tryptase, chymase, and carboxypeptidase), proteoglycans(heparin), and some cytokines and growth factors by a process
called degranulation. A second class of secreted products isgenerated by de novo synthesis of proinflammatory lipidmediators, such as prostaglandins and leukotrienes. Finally,mast cells are also able to synthesize and secrete a largenumber of growth factors, cytokines, and chemokines, manyof which have been implicated in tumor biology [e.g., VEGF,angiopoietin-1, TGF-b, interleukin (IL)-1, IL-6, TNF-a, and IL-10; refs. 12–14]. Notably, mast cells can be activated not only byIgE and specific antigen but by a long list of stimuli, includingphysical agents, products of diverse pathogens, endogenousdanger signals, certain endogenous peptides, and componentsof venoms, and several products of innate and adaptiveimmune responses, including some chemokines and cytokinesand products of complement activation (8).
Mast cells express high levels of the tyrosine kinase receptorKit (CD117), which is also expressed by other cell types suchas hematopoietic stem cells, melanocytes, germ cells, andintestinal interstitial cells of Cajal (15). Kit expression can beupregulated in tumor cells and mutations in c-kit have beenshown to be a primary event in the development of somenonhematopoietic tumors, such as gastrointestinal stromaltumors, and in neoplastic disorders associated with the devel-opment of abnormal expansionofmast cells (suchas the variousforms of mastocytosis and mast cell leukemia; refs. 15–17).
Stem cell factor (SCF), the ligand for Kit, is produced bystructural cells in the tissues (and also by mast cells) and playsa crucial role inmast cell development, survival, migration, andfunction (7, 18). SCF can be expressed by several types of tumor
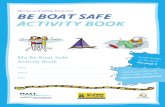
20 µm
Figure 1. High-power photomicrograph of a specimen of infiltrating ductal carcinoma of the breast stained by immunohistochemistry to detect tryptase,which identifies mast cells as cells with brown-stained cytoplasm. The section depicts at least 4 mast cells (solid arrows) in the tumor stroma, neargroups of infiltrating carcinoma cells (the edges of these groups of carcinoma cells are indicated with solid arrowheads). Scale bar, 20 mm(photomicrograph by Matt van de Rijn).
Marichal et al.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology Research270
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

cells and tissues (19–22). SCF can induce mast cell migrationin vitro (20, 21), and inhibition of the SCF/Kit axis in vivohas been shown to inhibit the migration of mouse bonemarrow–derived cultured mast cells (BMCMC) to tumors ina transplanted tumor model in mice (21).
The Notion of Mast Cell PlasticityMany key characteristics of mast cells, such as proliferation,
survival, and ability to store and/or secrete various products, aswell as the magnitude and nature of their secretory responsesto particular activation signals, can be regulated or "tuned" bymany environmental and genetic factors (8). The properties ofindividual mast cells thus may be different depending on thegenetic background of the host and/or the local or systemiclevels of factors that affect various aspects of mast cell bio-logy. This "plasticity" ofmultiple aspects of themast cell pheno-type can result in the development of phenotypically distinctpopulations of mast cells in different anatomic sites (or indifferent animal species). It also may result in the inducedalteration of mast cell phenotypes during various biologicresponses in vivo, and is called mast cell heterogeneity.The extent to which it is useful to use differences in the
phenotype of mast cells to "subclassify" the cells into distinctsubtypes, and the extent to which such phenotypic differencesare "fixed" as opposed to malleable, has been a matter ofdebate. However, mast cells in some animal species can beplaced into "subpopulations" based on readily identifiablefeatures such as differences in the ability of the mast cells tosynthesize and store various proteases or proteoglycans. Inhumans, mast cells have been classified into those containingmainly tryptase and those containing both tryptase and chy-mase (23). In mice, connective tissue-type mast cells (CTMC)are distinguished from mucosal mast cells (a population thatis more dependent on T-cell–dependent modulation than areCTMCs) according to their anatomic localization,morphology,and content of heparin and proteases (7–9). No matter whatcriteria are used to identify the subpopulations of mast cellsthat are present at a particular time in an individual anatomiclocation, the concept of mast cell plasticity is of particularimportance in the context of tumors, as the phenotype (andtherefore the function) of mast cells may be influenced by thetumor microenvironment and may change in important waysduring disease progression.
Possible Mast Cell Functions in Tumor BiologyTumors are complex tissues whose fate depends on the
levels of pro- versus antitumorigenic signals that are providedby the tumor cells, by the local tumor microenvironment(including by resident and recruited immune cells), and bythe host systemically. In particular, the proliferation andsurvival of tumor cells, angiogenesis, and other aspects oftissue remodeling, metastasis and distant growth of tumorcells, and the ability of tumors tomodulate the immune systemare especially important for the progression of tumors. All ofthese processes can potentially be negatively or positivelyregulated by individual products released by mast cells. Forinstance, the granule-associated mediator heparin can inter-fere with the growth of human breast cancer cells (24).
Histamine can inhibit the proliferation of human primarymelanoma cells, an effect that is enhanced by IL-6 (25). Angio-genesis is central to tumor development, and tumors oftenexhibit enhanced vascular permeability and the developmentof abnormal blood vessels. Notably, the proangiogenic VEGF,which was first described as a potent enhancer of vascularpermeability (26), can be produced by mouse and humanmastcells (27, 28). VEGF expression has been detected in mast cellswithin different types of human tumors (29–32). Several pro-teases released by mast cells [MMP-9 (33) and the serineproteases chymase and tryptase (34–36)] are proangiogenic;they can degrade components of the extracellular matrix andcontribute to tumor invasiveness. In addition, host immunityplays a central role in cancer development (elegantly reviewedin ref. 37), and several mouse studies have provided evidencethat mast cells have the ability to modulate adaptive immuneresponses, including effects on the biology of regulatory T cells(Tregs) and immunologic tolerance, thereby potentially mod-ulating the fate of tumors (38–40).
Functions of Mast Cells in Tumor Development:Lessons from Mouse Models
Many biologic functions of mast cells have been discoveredusing mouse models in which the activities and/or numbers ofmast cells can be altered. Each model has its advantages andlimitations (5, 6, 41), and mutant mice that specifically lack allmast cell populations as their sole abnormality have not yetbeen reported. Moreover, to our knowledge, there are nopharmacologic agents that can solely and selectively suppressmast cell activation (5). These points need to be kept in mindwhen interpreting data derived from studies using suchapproaches.
Mast cell–deficient mice with mutations affecting c-kitstructure or expression, especially WBB6F1-Kit
W/W-v (KitW/W-v)and C57BL/6-KitW-sh/W-sh (KitW-sh/W-sh) mice, have been usedextensively to study the functions ofmast cells in vivo (5). Thesemice are profoundly deficient in mast cells but also exhibitseveral other Kit-dependent phenotypic abnormalities (42, 43),and differences in the biologic responses of such "Kit-mutantmice" compared with the corresponding wild-type (WT) micemight, in principle, be due to any one of their abnormalities,not solely their deficit in mast cells. However, the lack of mastcells in Kit-mutant mice can be selectively repaired by theadoptive transfer of genetically compatible, in vitro-derivedmast cells to create so-called mast cell "knock-in" mice (44).These mast cell knock-in mice then can be used to assess theextent to which abnormalities in the biologic responses ofKit-mutant mice can be "normalized" by the adoptive transferof WT versus genetically altered mast cells. Such genetic andmast cell engraftment approaches have been widely used, inassociation with tumormodels, to investigate the roles of mastcells in tumor development in mice.
Examples of such studies are summarized in Table 1.Highlighting the potential complexity of the roles of mast cellsin tumors, a study by Pittoni and colleagues assessed thecontribution of mast cells in prostate cancer (45). Well-differ-entiated prostate adenocarcinoma cells [derived from transgen-ic TRAMP (transgenic adenocarcinoma of the mouse prostate)]
Mast Cells in Tumor Biology
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013 271
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

Tab
le1.
Exa
mplesof
pro-ve
rsus
antitum
origen
icfunc
tions
ofmas
tce
llsbas
edon
invivo
mou
sestud
ies
Tum
ormodel
Mutan
tmiceus
edFe
atures
analyz
edMainfind
ings/co
nclusions
Referen
ces
Tran
splant
mod
elof
B16
-BL6
melan
omace
llsSystemically
BM-eng
rafted
(106
)or
loca
llyBMCMCs-en
grafted
(107
)KitW
/W-vmice
—nu
mber
oftumor-bea
ringmice
with
amac
rosc
opic
angiog
enic
resp
onse
(this
resp
onse
couldalso
have
reflec
tedaco
ntrib
utionof
increa
seblood
flow
)—nu
mber
ofsp
ontane
ouslung
metas
tase
s
—Param
eterslower
inKitW
/W-v
than
inBM-or
BMCMCs-
engraftedKitW
/W-vmiceor
WTmice
—MCsco
ntributed
tothe
angiogen
ican
dmetas
tatic
resp
ons
e
(106
,107
)
Tran
sgen
icK14
-HPV16
mice:
amod
elof
dyn
amic
epith
elial
carcinog
enes
is(epidermal
hyperplasia,
angiog
enic
dys
plasia,
inva
sive
SCC)
K14
-HPV16
miceon
theKitW
/W-v
andco
rres
pon
dingWT
bac
kgroun
d
—MC
numbersan
dtryp
tase
/ch
ymas
eac
tivity
—ke
ratin
ocyteproliferation
—histolog
icev
alua
tionof
blood
vess
els
—MC
numbersan
dch
ymas
e/tryp
tase
activ
ityincrea
sedin
angiog
enic
dys
plastic
lesion
sin
WTK14
-HPV16
mice
—KitW
/W-vK14
-HPV16
mou
sewas
deficien
tinMCs,ha
dreduc
edke
ratin
ocyteprolife
ratio
nan
dsm
allq
uies
cent
blood
vess
els
—MCsco
ntributed
tothe
proce
ssofpremaligna
ntne
ova
scularizationvia
releas
eofpro-ang
iogen
icproteas
es
(34)
1,2-DMH-ind
uced
colonic
epith
elialn
eoplasm
sBM-eng
rafted
KitW
/W-vmice
—MC
numbers
—nu
mber
oftumor-bea
ringmice
—nu
mber
andsize
oftumors
—KitW
/W-vwereless
susc
eptib
leto
tumor
dev
elop
men
tthan
BM-eng
rafted
KitW
/W-vmice
orco
rres
pon
dingWTmice
—Increa
sedMCnu
mbersintumor
tissu
eco
rrelated
with
tumor
size
—MCs(and
/orother
hematopoieticce
llsdefi
cien
tin
KitW/W
-vmice)
may
contributeto
the
growth
ofsu
chch
emically
induc
edintestinal
tumor
(108
)
(Con
tinue
don
thefollo
wingpag
e)
Marichal et al.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology Research272
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

Tab
le1.
Exa
mplesof
pro-ve
rsus
antitum
origen
icfunc
tions
ofmas
tce
llsbas
edon
invivo
mou
sestud
ies
(Con
t'd)
Tum
ormodel
Mutan
tmiceus
edFe
atures
analyz
edMainfind
ings/co
nclusions
Referen
ces
Myc
-ind
uced
panc
reatic
islet
tumors(b-celltum
ors)
C57
BL/6-KitW
-sh/W
-sh
mice
Cromolyn
trea
tmen
tof
WTmice
—pa
ncreaticislettum
orex
pan
sion
(histology
,cellp
roliferation,
insu
linex
pression)
—intratum
orce
lldea
th,h
ypox
iaan
dva
scular
expan
sion
—Cromolyn
-treated
WTmicean
dC57
BL/6-KitW
-sh/W
-shmice
displaye
dlower
pan
crea
ticisletc
elltum
orex
pan
sion
than
(untreated
)WTmice,
aphe
nomen
onas
sociated
with
increa
seddea
thof
b-ce
lls,
hypox
ia,a
nddim
inishe
dan
giog
enes
is
–MCsarerequiredfor
angiogen
esisan
dex
pan
sion
ofsu
chMyc
-ind
uced
pan
crea
ticislettumors
(109
)
Tran
sgen
icC57
BL/6/J-APCMin/þ
mice:
amod
elof
early
-stage
intestinal
aden
omas
C57
BL/6/J-APCMin/þ
miceon
the
WTan
dC57
BL/6-KitW
-sh/W
-sh
bac
kgroun
ds
—MC
number
—tumor
size
—ap
optosis
—T-ce
ll,eo
sino
phil,an
dne
utroph
ilinfiltration
—C57
BL/6/JAPCMin/þ;
KitW
-sh/W
-shmicedisp
laye
dincrea
sedtumor
size
asso
ciated
with
dec
reas
edeo
sino
phils
anddec
reas
edap
optosisco
mpared
toco
ntrols
—MCsca
nplayaprotectiverole
inthegrowth
ofsu
chintestinal
tumors
(110
)
Tran
splant
mod
elof
well-
differen
tiatedprostate
aden
ocarcino
mace
llsderived
from
TRAMPmice:
amod
elof
prostateca
ncer
MCkn
ock-inC57
BL/6-KitW
-sh/W
-sh
mice(som
een
graftedwith
WTor
Mmp9�
/�BMCMCs)
—MC
number
andMMP9
express
ion
—nu
mber
oftumor-bea
ringmice
—tumor
size
—Tu
mor
cells
failedto
grow
robus
tlyin
C57
BL/
6-KitW
-sh/W
-shmice,
even
after
engraftm
entwith
Mmp9
�/�
BMCMCs,
but
did
grow
strong
lyin
WTmiceor
inC57
BL/6-KitW
-sh/W
-shmice
egrafted
with
WTBMCMCs
—MCsan
dMC-d
erived
MMP9co
ntributeto
the
dev
elopmen
tofsu
chwell-
differen
tiated
prostate
tumors
(45)
(Con
tinue
don
thefollo
wingpag
e)
Mast Cells in Tumor Biology
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013 273
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

Tab
le1.
Exa
mplesof
pro-ve
rsus
antitum
origen
icfunc
tions
ofmas
tce
llsbas
edon
invivo
mou
sestud
ies
(Con
t'd)
Tum
ormodel
Mutan
tmiceus
edFe
atures
analyz
edMainfind
ings/co
nclusions
Referen
ces
Tran
sgen
icTR
AMPmice:
amod
elof
prostateca
ncer
TRAMPmiceon
theC57
BL/
6-KitW
-sh/W
-shba
ckgrou
ndor
C57
BL/6-TR
AMPmicetrea
ted
with
crom
olyn
—inciden
ceof
anap
lastic
tumors
—ge
neex
pressionprofile
ofthe
tumors
—TR
AMPmiceon
theC57
BL/
6-KitW
-sh/W
-shbac
kgroun
d,
orC57
BL/6-TR
AMPmice
trea
tedwith
crom
olyn
displaye
dahigh
inciden
ceof
aggres
sive
canc
erva
riants
charac
teriz
edbya
neuroe
ndoc
rinesign
ature
—MCsmay
playaprotectiverole
inprostatene
uroen
docrine
tumorigen
esis
(45)
Tran
splant
mod
elof
MB49
bladde
rca
rcinom
ace
llsMCkn
ock-inC57
BL/6-KitW
-sh/W
-sh
mice
—MC
number
andmicrova
scular
den
sity
—tumor
size
andsu
rvival
—T-ce
llinfiltration
—C57
BL/6-KitW
-sh/W
-shmiceare
moreresistan
tto
tumor
dev
elop
men
ttha
nMCkn
ock-
inC57
BL/6-KitW
-sh/W
-shor
WT
mice,
aneffect
that
isTce
lldep
enden
t—
MCsca
nco
ntributeto
tumor
inva
sive
ness
inthis
model
byim
pairing
the
dev
elopmen
tofprotective
anti-tumorim
mun
ity
(111
)
Tran
splanted
T-ce
lllympho
ma
EL4
cells
C57
BL/6-KitW
-sh/W
-shmicean
dinduc
ible
MC-defi
cien
tMcp
t5-
Cre/iD
TRþmice
—tumor
volume/area
—Bothstrainsof
MC-defi
cien
tmicedisplaylower
tumor
grow
th—
MCspromote
thegrowth
of
EL4
tumors
invivo
(58)
NOTE
:K14
-HPV16
mice,
miceex
pressingea
rlyregion
gene
sof
human
pap
illom
aviru
stype16
under
theco
ntrolo
fthe
promoter
oftheke
ratin
ocyte-as
sociated
keratin
14ge
ne;
Cromolyn
,anag
entkno
wnto
"stabilize
"ce
rtainroden
tmas
tcells(M
C),althou
ghits
effectiven
essan
dse
lectivity
asan
inhibito
rofm
astc
ellactivationrece
ntlyha
sbee
nque
stione
din
mice(112
).APCMin/þ
mou
se,the
Min(m
ultip
leintestinalne
oplasia)mou
seistheresu
ltof
asing
lege
rmlinemutationinthetumor
suppress
orge
nead
enom
atou
spolyp
osisco
li(APC):
APCMin/þ
micede
velopmultip
leintestinalad
enom
as;M
cpt5-C
re/iD
TRþmice,cros
sbetwee
ninduc
iblediphteriatoxinrece
ptor-flox
edmicean
dtran
sgen
icmiceex
pressingtheCre
reco
mbinas
eun
der
theco
ntrolo
ftheMC-ass
ociatedMcp
t5prom
oter
(diphteria
toxintrea
tmen
tresu
ltsin
nearly
complete
ablatio
nof
perito
neal
mas
tce
lls).
Abbreviations
:BM,b
onemarrow;D
MH,d
imethy
lhyd
razine
;SCC,s
qua
mou
sce
llca
rcinom
a.
Marichal et al.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology Research274
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

failed to grow in mast cell-deficient C57BL/6-KitW-sh/W-sh micebut grew normally in WT controls, as well as in C57BL/6-KitW-sh/W-sh mice engrafted with WT BMCMCs. The authorsshowed that these effects weremediated byMMP-9, as engraft-ment of C57BL/6-KitW-sh/W-sh mice with Mmp9-deficientBMCMCs did not restore tumor growth (45). These resultsare consistent with the conclusion that mast cells and mastcell–derived MMP-9 contribute to the development ofwell-differentiated prostate tumors in this model and maytherefore represent attractive therapeutic targets. In contrast,the same report showed that when TRAMPmice were crossedwith C57BL/6-KitW-sh/W-sh mice that genetically lack mast cells(and which exhibit other abnormalities independent of themast cell deficiency), or when TRAMP mice were treated withcromolyn, a drug thought to suppress certain mast cell func-tions but that also affects other cell types, suchmice developeda high incidence of aggressive but rare cancer variants char-acterized by a neuroendocrine signature and c-kit expression.These experiments suggested that mast cells might have aprotective role in the development of these aggressive types ofprostate tumors. Taken together, these findings from Pittoniand colleagues suggest that mast cells can exert different (andindeed opposite) functions in the development of cancers inthis model, depending on the stage and subtype (epithelial vsneuroendocrine) of the particular tumor (45).Other approaches have been used to identify contributions
ofmast cells to tumor development. By generating polyp-prone(APCD468) chimeric mice bearing bone marrow derived fromWT mice or mice deficient in genes important for mast celldevelopment or trafficking, Gounaris and colleagues providedevidence suggesting that mast cells (and/or other bone mar-row-derived cell types also influenced by these mutations)were essential hematopoietic components that favored thedevelopment of intestinal polyps (46). Using this mousemodel,the same group investigated cross-talk between Tregs andmast cells and reported that mast cells can induce phenotypicchanges in classical immunosuppressive and anti-inflamma-tory Tregs, causing them to become a "proinflammatory Treg"population that can promote tumor growth (47–49).Evidence of the importance of mast cells and tumor-derived
SCF in the development of plexiform neurofibromas has beenprovided by Clapp and colleagues (20, 50, 51). Plexiformneurofibromas, tumors comprising many cell types includingSchwann cells and infiltrating mast cells, are pathognomonicfor neurofibromatosis type 1 (NF1), which results from muta-tions in the Nf1 gene (52). Zhu and colleagues (53) developeda mouse model of plexiform neurofibroma and studiedthe mechanisms underlying the formation of these tumors.Notably, in addition to loss-of-function mutations in bothcopies of the Nf1 gene in Schwann cells, optimal growth ofthe neurofibromas also required haploinsufficiency of NF1in Kit–dependent bone marrow–derived cells (which theauthors concluded probably represented mast cells) withinthe tumor microenvironment (50). The proposed mechanismis that Nf1�/� Schwann cells secrete high levels of SCF thatcan enhance mast cell migration within the tumor (20). Fur-thermore, Nf1þ/� mast cells are more potent than WT mastcells in proliferating, surviving and secreting proinflamma-
tory cytokines within the tumor, therefore promoting tumordevelopment (20).
In 2011, four different groups generated new "Kit-indepen-dent" constitutive or inducible models of mast cell deficiency(5, 54–57). While these models do not exhibit abnormalitiesrelated to mutations affecting c-kit structure or expression,each model has other limitations that should be consideredwhen used for studies of mast cell biology in vivo (5). Never-theless, these newmodels represent additional tools to analyzepossible roles of mast cells in tumor biology in vivo (58).
In summary, studies in mice have provided evidence thatmast cells may exert either protumorigenic or antitumori-genic functions in different tumor models. Results obtainedin an individual tumor model probably depend on such factorsas: (i) the type and stage of the tumor (and other features ofthe "tumor model," such as whether the tumor developedspontaneously or was transplanted); (ii) the signals in thetumor microenvironment (or generated systemically) that canmodulate mast cell phenotype and function; and (iii) theapproaches used to manipulate mast cell numbers and/orfunctions.
Studies Linking Mast Cells to Tumors in HumansIt has long been known that mast cells can accumulate at
sites of tumors in humans (1, 2). But what are their functions inhuman tumor biology, and can features of the mast cellresponse to tumors, such as their numbers, phenotype, oranatomic distribution, be used to predict tumor behavior orprognosis in patients with cancer? The answers to thesequestions have not yet been fully resolved, but are likely tobe complex. Indeed, as in mice, studies in humans havesuggested that mast cells can have either protective or dele-terious roles in host responses to tumors.
Increased numbers of mast cells have been associated withunfavorable disease features or outcomes (e.g., high tumorgrade, increased metastases, and low overall or progression-free survival). The deleterious roles ofmast cells were identifiedin studies of neoplasms affecting the skin, including malignantmelanoma (30, 59, 60), Merkel cell carcinoma (61), and primarycutaneous lymphoma (58). Increased numbers of mast cellswere also found in pancreatic adenocarcinomas (62–64); squa-mous cell carcinomas (SCC) of the esophagus (65), mouth (66),and lip (67); and in a long list of hematologic neoplasms (e.g.,Hodgkin lymphoma; refs. 68, 69, B-cell chronic lymphocyticleukemia; refs. 70, 71, myelodysplastic syndromes; ref. 72,follicular lymphoma; ref. 73, B-cell non-Hodgkin lymphoma;ref. 74, and multiple myeloma; ref. 75). In many of thesestudies (29, 30, 58–60, 62, 64–66, 71, 75), the extent of angio-genesis, as assessed by staining of microvessels (in most casesby immunohistochemistry using anti-human CD31 or CD34antibodies), was positively correlated with the numbers ofmast cells per unit area of tissue. In some of these studies,mast cells were shown to express VEGF (29, 30). Such findingshave suggested that mast cells may contribute to tumorprogression by supporting angiogenesis. However, in an anal-ysis of Hodgkin lymphoma (68, 69), high numbers of eithermicrovessels or mast cells were associated with a poor prog-nosis, but high numbers of microvessels did not correlate
Mast Cells in Tumor Biology
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013 275
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

significantly with high numbers of mast cells, suggesting thatmast cells may contribute to tumor progression in thesesettings by mechanisms unrelated to angiogenesis.
Studies correlating the presence of mast cells in prostatecancer (76–78), colorectal cancer (79–84) and non–small celllung cancer (32, 85–88) have led to more nuanced interpreta-tions. In prostate cancer, Nonomura and colleagues reportedthat the number of tryptaseþmast cells (that in this study wereonly observed around but not within the cancer foci) positivelycorrelated with a high Gleason score and an advanced clinicalstage of the prostate tumor, indicating that high numbers ofsuch mast cells represent a poor prognostic factor for survivalfollowing treatment (76). However, Fleischmann and collea-gues used tissue microarrays to count numbers of Kitþ mastcells in more than 2,300 prostate cancer specimens frompatients who underwent prostatectomy at the same insti-tution and found that high intratumoral mast cell density(i.e., number of mast cells per unit area within the tumor)was associated with a good prognosis in prostate cancer(77). A third study, by Johansson and colleagues, of patientswith prostate cancer who underwent prostatectomy, showedthat mast cell densities within the tumors were an inde-pendent favorable prognostic factor, whereas high numbersof peritumoral mast cell were associated with a poor prog-nosis (78). The findings of Johansson and colleagues there-fore suggest that the discrepancy observed in the twopreceding studies might be due to the different anatomiclocation (peritumoral vs. intratumoral) of the mast cellsanalyzed and that the function(s) of mast cells in this cancermay be strongly dependent on the cells' distribution withinthe tumor or in its local microenvironment.
Results similar to those in prostate cancer were reported byFisher and colleagues in 1989 that in colorectal cancer highnumbers of mast cells at the tumor border correlated withdecreased survival and represented an independent poorprognostic parameter (79). In accord with this finding, subse-quent studies have shown that mast cells positively correlatedwith microvessel density in colorectal cancers, a parameterthat independently was associated with a poor prognosis (82–84). However, in 1999, Nielsen and colleagues showed in a studyof more than 500 samples from patients with colorectal cancerthat high numbers of tryptaseþ mast cells within the submu-cosal area with the highest density of inflammatory cells at theboundary zone between the tumor and normal tissue signif-icantly correlated with a favorable prognosis (80). The latterfinding is consistent with observations by Tan and colleagues(81), in which the authors correlated the number of chymaseþ
and tryptaseþ mast cells within the most abundant inflam-matory infiltrates with various clinicopathologic factors (his-tologic grade, depth of invasion, metastasis) and survival, andshowed that patients with a low level of mast cell infiltrationhad a significantly deeper invasion and lower overall survival(81). Increased numbers of mast cells also have been shown tocorrelate with either a good (85, 87, 88) or poor (32, 86)prognosis in non–small cell lung cancer, and the reasons forthese discrepancies may reflect the following factors: (i) dif-ferences in the type and the stage of tumors included in thesestudies (pulmonary adenocarcinoma only; ref. 85, all types of
non–small cell lung cancer; refs. 86, 87, or stage I of non–smallcell lung cancer; refs. 32, 88; (ii) the location of the mast cellsanalyzed (lung parenchyma; ref. 85, regions of highestmast cellinfiltration and vascularization; ref. 86, intratumoral stroma;ref. 32, tumor cell islets; ref. 87, or peritumoral zone; ref. 88; and(iii) the methods used to assess and quantify the mast cells(alcian blue and safranin O; ref. 85, tryptase; refs. 32, 86, 87, ortryptase and chymase; ref. 88).
In breast carcinomas, most (89–92) but not all (93, 94)studies have linked mast cells to a good prognosis. In 2004,Dabiri and colleagues used tissue microarrays to study 348cases of invasive breast carcinoma (each specimen analyzedwas from an invasive region of the carcinoma) using immu-nohistochemical staining of several markers that were thencorrelated to patient outcome (90). Interestingly, the presenceof Kitþ mast cells in the stroma (the authors did not observeany Kit expression in the tumor cells, although it has beenreported in other studies; ref. 95) correlated with improvedsurvival. This study confirmed previous findings (89) support-ing an important favorable role for mast cells in breast carci-nomas (90). The same authors then extended their findings byconducting a large microarray study of 4,444 cases of breastcancer and confirmed by immunohistochemical staining ofKit that the presence of any number of mast cells is anindependent marker of a good prognosis in invasive breastcarcinomas (91).
Mast cells may herald a favorable prognosis in other tumorsas well. For example, high numbers of tumor-associatedtryptaseþ mast cells have been reported to be an independentfavorable prognostic factor for survival after surgery in patientswith malignant pleural mesothelioma (96). Another studyreported that high numbers of tryptaseþ mast cells in tumortissue in patients with diffuse large B-cell lymphoma whounderwent chemotherapy [mainly CHOP (cyclophosphamide,doxorubicin, oncovin, and prednisone)] were positively corre-lated with a favorable prognosis (97).
Notably, a study of mast cells in samples from various typesof renal cell carcinoma showed that toluidine blueþ mast cellswere more abundant in tumor tissues and at tumor bordersthan in healthy tissues, and that the number of mast cellscorrelated positively with the presence of CD31þmicrovessels;however, no correlationwas found between eithermast cells ormicrovessels and the clinicopathologic features of the disease,including survival (98). It is possible that observations like thisalso may have been made by other groups investigating othertypes of tumors, but have not been published given the"negative" findings.
Concluding ThoughtsAs reviewed briefly above and by others (e.g., refs. 99–102),
the literature abounds with studies correlating the presence ofmast cells with tumors but it has been challenging to drawsimple conclusions from such studies. As we have outlined,both studies of mouse models and observations in humancancer suggest that, depending on the circumstances, includ-ing the tumor model (in mice) or the type of tumor (inhumans), mast cells can have either favorable or unfavorablenet effects on host responses to tumors. Why this is so remains
Marichal et al.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology Research276
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

to be determined. However, mast cells certainly are not theonly type of hematopoietic cells that can have disparate effectson host responses in different types of tumors, as the same hasbeen reported for macrophages (103–105). And while it iscorrect to point out that both mast cell populations andtumors (and their component neoplastic cells) can exhibitheterogeneity of phenotype, defining mechanistically howmast cells interfere with or promote the survival and progres-sion of particular types of tumors is likely to continue torepresent a challenge. This may turn out to be a rewardingchallenge to address, however, as advancing understanding inthis area holds the promise of determining whether criticalfunctions ofmast cells might even be harnessed (or restrained)to provide therapeutic benefit to patients with cancer.
Authors' ContributionsConception and design: T. Marichal, S.J. GalliAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): S.J. GalliWriting, review, and/or revision of the manuscript: T. Marichal, M. Tsai,S.J. Galli
AcknowledgmentsThe authors thank Matt van de Rijn for his critical reading of the manuscript
and for providing the photomicrographs depicted in Fig. 1 and on the cover.
Grant SupportT. Marichal is supported by a Marie Curie International Outgoing Fellowship
for Career Development (grant agreement no. 299954), and S.J. Galli and M. Tsaihave been supported by NIH grants AI023990, CA072074, and AI070813.
Received August 8, 2013; accepted September 3, 2013; published onlineNovember 4, 2013.
References1. Ehrlich P. Beitr€age zur Theorie und Praxis der Histologischen
F€arbung [Thesis]. Leipzig, Germany: Leipzig University; 1878.2. Westphal E. Uber Mastzellen. Berlin: Hirschwald Press; 1891.3. Galli SJ, Tsai M. IgE andmast cells in allergic disease. Nat Med 2012;
18:693–704.4. Galli SJ, Grimbaldeston M, Tsai M. Immunomodulatory mast cells:
negative, as well as positive, regulators of immunity. Nat Rev Immu-nol 2008;8:478–86.
5. Reber LL, Marichal T, Galli SJ. New models for analyzing mast cellfunctions in vivo. Trends Immunol 2012;33:613–25.
6. RodewaldHR, FeyerabendTB.Widespread immunological functionsof mast cells: fact or fiction? Immunity 2012;37:13–24.
7. Gurish MF, Austen KF. Developmental origin and functional special-ization of mast cell subsets. Immunity 2012;37:25–33.
8. Galli SJ, Kalesnikoff J, Grimbaldeston MA, Piliponsky AM, Wil-liams CM, Tsai M. Mast cells as "tunable" effector and immuno-regulatory cells: recent advances. Annu Rev Immunol 2005;23:749–86.
9. Kitamura Y. Heterogeneity of mast cells and phenotypic changebetween subpopulations. Annu Rev Immunol 1989;7:59–76.
10. Galli SJ, BorregaardN,Wynn TA. Phenotypic and functional plasticityof cells of innate immunity: macrophages,mast cells and neutrophils.Nature Immunol 2011;12:1035–44.
11. GilfillanAM,Rivera J. The tyrosine kinasenetwork regulatingmast cellactivation. Immunol Rev 2009;228:149–69.
12. Detoraki A, Granata F, StaibanoS, Rossi FW,MaroneG,GenoveseA.Angiogenesis and lymphangiogenesis in bronchial asthma. Allergy2010;65:946–58.
13. MetzM,GrimbaldestonMA,NakaeS,PiliponskyAM, TsaiM,Galli SJ.Mast cells in the promotion and limitation of chronic inflammation.Immunol Rev 2007;217:304–28.
14. Kalesnikoff J, Galli SJ. New developments in mast cell biology. NatImmunol 2008;9:1215–23.
15. Pittoni P, Piconese S, Tripodo C, Colombo MP. Tumor-intrinsic and-extrinsic roles of c-Kit:mast cells as the primary off-target of tyrosinekinase inhibitors. Oncogene 2011;30:757–69.
16. Valent P, Akin C, Sperr WR, Mayerhofer M, Fodinger M, Fritsche-Polanz R, et al. Mastocytosis: pathology, genetics, and currentoptions for therapy. Leuk Lymph 2005;46:35–48.
17. Rubin BP, HeinrichMC, Corless CL. Gastrointestinal stromal tumour.Lancet 2007;369:1731–41.
18. Galli SJ, Tsai M, Wershil BK, Tam SY, Costa JJ. Regulation of mouseand human mast cell development, survival and function by stemcell factor, the ligand for the c-kit receptor. Int Arch Allergy Immunol1995;107:51–3.
19. Bellone G, Smirne C, Carbone A, Buffolino A, Scirelli T, Prati A, et al.KIT/stemcell factor expression in premalignant andmalignant lesionsof the colon mucosa in relationship to disease progression andoutcomes. Int J Oncol 2006;29:851–9.
20. Yang FC, Ingram DA, Chen S, Hingtgen CM, Ratner N, Monk KR,et al. Neurofibromin-deficient Schwann cells secrete a potentmigratory stimulus for Nf1þ/� mast cells. J Clin Invest 2003;112:1851–61.
21. Huang B, Lei Z, Zhang GM, Li D, Song C, Li B, et al. SCF-mediatedmast cell infiltration and activation exacerbate the inflammation andimmunosuppression in tumor microenvironment. Blood 2008;112:1269–79.
22. Zhang W, Stoica G, Tasca SI, Kelly KA, Meininger CJ. Modulationof tumor angiogenesis by stem cell factor. Cancer Res 2000;60:6757–62.
23. Craig SS, Schwartz LB. Tryptase and chymase, markers of distincttypes of human mast cells. Immunol Res 1989;8:130–48.
24. Samoszuk M, Kanakubo E, Chan JK. Degranulating mast cells infibrotic regions of human tumors and evidence that mast cell heparininterferes with the growth of tumor cells through a mechanisminvolving fibroblasts. BMC Cancer 2005;5:121.
25. Lazar-Molnar E, Hegyesi H, Pallinger E, Kovacs P, Toth S, FitzsimonsC, et al. Inhibition of human primary melanoma cell proliferation byhistamine is enhanced by interleukin-6. Eur J Clin Invest 2002;32:743–9.
26. Sitohy B, Nagy JA, Dvorak HF. Anti-VEGF/VEGFR therapy for cancer:reassessing the target. Cancer Res 2012;72:1909–14.
27. Boesiger J, Tsai M, Maurer M, Yamaguchi M, Brown LF, Claffey KP,et al. Mast cells can secrete vascular permeability factor/vascularendothelial cell growth factor and exhibit enhanced release afterimmunoglobulin E-dependent upregulation of fc e receptor I expres-sion. J Exp Med 1998;188:1135–45.
28. Grutzkau A, Kruger-Krasagakes S, Baumeister H, Schwarz C, KogelH, Welker P, et al. Synthesis, storage, and release of vascularendothelial growth factor/vascular permeability factor (VEGF/VPF)by human mast cells: implications for the biological significance ofVEGF206. Mol Biol Cell 1998;9:875–84.
29. SawatsubashiM,YamadaT, FukushimaN,MizokamiH, TokunagaO,Shin T. Association of vascular endothelial growth factor and mastcells with angiogenesis in laryngeal squamous cell carcinoma. Virch-ows Archiv 2000;436:243–8.
30. Toth-Jakatics R, Jimi S, Takebayashi S, Kawamoto N. Cutaneousmalignant melanoma: correlation between neovascularization andperitumor accumulation of mast cells overexpressing vascular endo-thelial growth factor. Hum Pathol 2000;31:955–60.
31. Aoki M, Pawankar R, Niimi Y, Kawana S. Mast cells in basal cellcarcinoma express VEGF, IL-8 and RANTES. Int Arch Allergy Immu-nol 2003;130:216–23.
32. Imada A, Shijubo N, Kojima H, Abe S. Mast cells correlate withangiogenesis and poor outcome in stage I lung adenocarcinoma.Eur Respir J 2000;15:1087–93.
33. BaramD, Vaday GG, Salamon P, Drucker I, Hershkoviz R, Mekori YA.Human mast cells release metalloproteinase-9 on contact with
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013 277
Mast Cells in Tumor Biology
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

activated T cells: juxtacrine regulation by TNF-a. J Immunol 2001;167:4008–16.
34. Coussens LM, Raymond WW, Bergers G, Laig-Webster M, Beh-rendtsen O, Werb Z, et al. Inflammatory mast cells up-regulateangiogenesis during squamous epithelial carcinogenesis. GenesDev1999;13:1382–97.
35. Huang C, Sali A, Stevens RL. Regulation and function of mast cellproteases in inflammation. J Clin Immunol 1998;18:169–83.
36. Blair RJ, Meng H, MarcheseMJ, Ren S, Schwartz LB, Tonnesen MG,et al. Humanmast cells stimulate vascular tube formation. Tryptase isa novel, potent angiogenic factor. J Clin Invest 1997;99:2691–700.
37. Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integratingimmunity's roles in cancer suppression and promotion. Science2011;331:1565–70.
38. Galli SJ, Nakae S, Tsai M. Mast cells in the development of adaptiveimmune responses. Nat Immunol 2005;6:135–42.
39. Lu LF, Lind EF, GondekDC, Bennett KA,GleesonMW,Pino-LagosK,et al. Mast cells are essential intermediaries in regulatory T-celltolerance. Nature 2006;442:997–1002.
40. Dalton DK, Noelle RJ. The roles of mast cells in anticancer immunity.Cancer Immunol Immunother 2012;61:1511–20.
41. Rao KN, Brown MA. Mast cells: multifaceted immune cells withdiverse roles in health and disease. Ann N Y Acad Sci 2008;1143:83–104.
42. Chervenick PA, Boggs DR. Decreased neutrophils and megakaryo-cytes in anemic mice of genotype W/W. J Cell Physiolo 1969;73:25–30.
43. Nigrovic PA, Gray DH, Jones T, Hallgren J, Kuo FC, Chaletzky B, et al.Genetic inversion in mast cell-deficient Wsh mice interrupts corinand manifests as hematopoietic and cardiac aberrancy. Am J Pathol2008;173:1693–701.
44. Tsai M, Grimbaldeston MA, Yu M, Tam SY, Galli SJ. Using mast cellknock-in mice to analyze the roles of mast cells in allergic responsesin vivo. Chem Immunol Allergy 2005;87:179–97.
45. Pittoni P, Tripodo C, Piconese S, Mauri G, Parenza M, Rigoni A, et al.Mast cell targeting hampers prostate adenocarcinoma developmentbut promotes the occurrence of highly malignant neuroendocrinecancers. Cancer Res 2011;71:5987–97.
46. Gounaris E, ErdmanSE,RestainoC,GurishMF, FriendDS,Gounari F,et al. Mast cells are an essential hematopoietic component for polypdevelopment. Proc Natl Acad Sci U S A 2007;104:19977–82.
47. Gounaris E, Blatner NR, Dennis K, Magnusson F, Gurish MF, StromTB, et al. T-regulatory cells shift from a protective anti-inflammatoryto a cancer-promoting proinflammatory phenotype in polyposis.Cancer Res 2009;69:5490–7.
48. Blatner NR, Bonertz A, Beckhove P, Cheon EC, Krantz SB, StrouchM, et al. In colorectal cancer mast cells contribute to systemicregulatory T-cell dysfunction. Proc Natl Acad Sci U S A 2010;107:6430–5.
49. Colombo MP, Piconese S. Polyps wrap mast cells and Treg withintumorigenic tentacles. Cancer Res 2009;69:5619–22.
50. Yang FC, Ingram DA, Chen S, Zhu Y, Yuan J, Li X, et al. Nf1-dependent tumors require a microenvironment containing Nf1þ/�
- and c-kit-dependent bone marrow. Cell 2008;135:437–48.51. Yang FC, Chen S, Clegg T, Li X, Morgan T, Estwick SA, et al. Nf1þ/�
mast cells induce neurofibroma like phenotypes through secretedTGF-beta signaling. Hum Mol Genet 2006;15:2421–37.
52. Staser K, Yang FC, Clapp DW. Mast cells and the neurofibromamicroenvironment. Blood 2010;116:157–64.
53. Zhu Y, Ghosh P, Charnay P, Burns DK, Parada LF. Neurofibromas inNF1: Schwann cell origin and role of tumor environment. Science2002;296:920–2.
54. DudeckA,Dudeck J, Scholten J, PetzoldA, SurianarayananS, KohlerA, et al. Mast cells are key promoters of contact allergy that mediatethe adjuvant effects of haptens. Immunity 2011;34:973–84.
55. Lilla JN, Chen CC, Mukai K, BenBarak MJ, Franco CB, Kalesnikoff J,et al. Reducedmast cell and basophil numbers and function inCpa3-Cre; Mcl-1fl/fl mice. Blood 2011;118:6930–8.
56. Feyerabend TB, Weiser A, Tietz A, StassenM, Harris N, Kopf M, et al.Cre-mediated cell ablation contests mast cell contribution in models
of antibody- and T cell-mediated autoimmunity. Immunity 2011;35:832–44.
57. Otsuka A, Kubo M, Honda T, Egawa G, Nakajima S, Tanizaki H,et al. Requirement of interaction between mast cells and skindendritic cells to establish contact hypersensitivity. PLoS ONE2011;6:e25538.
58. Rabenhorst A, Schlaak M, Heukamp LC, Forster A, Theurich S, vonBergwelt-Baildon M, et al. Mast cells play a protumorigenic role inprimary cutaneous lymphoma. Blood 2012;120:2042–54.
59. Ribatti D, Ennas MG, Vacca A, Ferreli F, Nico B, Orru S, et al. Tumorvascularity and tryptase-positive mast cells correlate with a poorprognosis in melanoma. Eur J Clin Invest 2003;33:420–5.
60. Ribatti D, Vacca A, Ria R, Marzullo A, Nico B, Filotico R, et al.Neovascularisation, expression of fibroblast growth factor-2, andmast cells with tryptase activity increase simultaneously with path-ological progression in human malignant melanoma. Eur J Cancer2003;39:666–74.
61. Beer TW,Ng LB,MurrayK.Mast cells haveprognostic value inMerkelcell carcinoma. Am J Dermatopathol 2008;30:27–30.
62. Esposito I, Menicagli M, Funel N, Bergmann F, Boggi U, Mosca F,et al. Inflammatory cells contribute to the generation of an angiogenicphenotype in pancreatic ductal adenocarcinoma. J Clin Pathol2004;57:630–6.
63. Strouch MJ, Cheon EC, Salabat MR, Krantz SB, Gounaris E, Mel-strom LG, et al. Crosstalk between mast cells and pancreatic cancercells contributes to pancreatic tumor progression. Clin Cancer Res2010;16:2257–65.
64. Cai SW, Yang SZ, Gao J, Pan K, Chen JY, Wang YL, et al.Prognostic significance of mast cell count following curativeresection for pancreatic ductal adenocarcinoma. Surgery 2011;149:576–84.
65. ElpekGO,Gelen T, AksoyNH,ErdoganA,Dertsiz L, DemircanA, et al.The prognostic relevance of angiogenesis and mast cells in squa-mous cell carcinoma of the oesophagus. J Clin Pathol 2001;54:940–4.
66. Iamaroon A, Pongsiriwet S, Jittidecharaks S, Pattanaporn K, Pra-payasatok S, Wanachantararak S. Increase of mast cells and tumorangiogenesis in oral squamous cell carcinoma. J Oral Pathol Med2003;32:195–9.
67. Rojas IG, Spencer ML, Martinez A, Maurelia MA, Rudolph MI. Char-acterization of mast cell subpopulations in lip cancer. J Oral PatholMed 2005;34:268–73.
68. Glimelius I, Edstrom A, Fischer M, Nilsson G, Sundstrom C, Molin D,et al. Angiogenesis and mast cells in Hodgkin lymphoma. Leukemia2005;19:2360–2.
69. Molin D, EdstromA,Glimelius I, Glimelius B, NilssonG, SundstromC,et al. Mast cell infiltration correlates with poor prognosis in Hodgkin'slymphoma. Br J Haematol 2002;119:122–4.
70. Molica S, Vacca A, Crivellato E, Cuneo A, Ribatti D. Tryptase-positivemast cells predict clinical outcome of patients with early B-cellchronic lymphocytic leukemia. Eur J Haematol 2003;71:137–9.
71. Ribatti D, Molica S, Vacca A, Nico B, Crivellato E, Roccaro AM, et al.Tryptase-positive mast cells correlate positively with bone marrowangiogenesis in B-cell chronic lymphocytic leukemia. Leukemia2003;17:1428–30.
72. Ribatti D, Polimeno G, Vacca A, Marzullo A, Crivellato E, Nico B, et al.Correlation of bone marrow angiogenesis and mast cells with tryp-tase activity in myelodysplastic syndromes. Leukemia 2002;16:1680–4.
73. Taskinen M, Karjalainen-Lindsberg ML, Leppa S. Prognostic influ-ence of tumor-infiltrating mast cells in patients with follicular lym-phoma treated with rituximab and CHOP. Blood 2008;111:4664–7.
74. Ribatti D, Vacca A, Marzullo A, Nico B, Ria R, Roncali L, et al.Angiogenesis and mast cell density with tryptase activity increasesimultaneously with pathological progression in B-cell non-Hodg-kin's lymphomas. Int J Cancer 2000;85:171–5.
75. Ribatti D, Vacca A, Nico B, Quondamatteo F, Ria R, Minischetti M,et al. Bone marrow angiogenesis and mast cell density increasesimultaneously with progression of human multiple myeloma. Br JCancer 1999;79:451–5.
Cancer Immunol Res; 1(5) November 2013 Cancer Immunology Research278
Marichal et al.
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

76. Nonomura N, Takayama H, Nishimura K, Oka D, Nakai Y, Shiba M,et al. Decreased number of mast cells infiltrating into needle biopsyspecimens leads to abetter prognosis of prostate cancer. Br JCancer2007;97:952–6.
77. Fleischmann A, Schlomm T, Kollermann J, Sekulic N, Huland H,Mirlacher M, et al. Immunological microenvironment in prostatecancer: high mast cell densities are associated with favorable tumorcharacteristics and good prognosis. Prostate 2009;69:976–81.
78. JohanssonA,RudolfssonS,HammarstenP,Halin S, PietrasK, JonesJ, et al. Mast cells are novel independent prognostic markers inprostate cancer and represent a target for therapy. Am J Pathol2010;177:1031–41.
79. Fisher ER, Paik SM, Rockette H, Jones J, Caplan R, Fisher B.Prognostic significance of eosinophils andmast cells in rectal cancer:findings from the National Surgical Adjuvant Breast and BowelProject (protocol R-01). Hum Pathol 1989;20:159–63.
80. Nielsen HJ, Hansen U, Christensen IJ, Reimert CM, Brunner N,Moesgaard F. Independent prognostic value of eosinophil and mastcell infiltration in colorectal cancer tissue. J Pathol 1999;189:487–95.
81. Tan SY, Fan Y, Luo HS, Shen ZX, Guo Y, Zhao LJ. Prognosticsignificance of cell infiltrations of immunosurveillance in colorectalcancer. World J Gastroenterol 2005;11:1210–4.
82. Acikalin MF, Oner U, Topcu I, Yasar B, Kiper H, Colak E. Tumourangiogenesis and mast cell density in the prognostic assessment ofcolorectal carcinomas. Dig Liver Dis 2005;37:162–9.
83. Yodavudh S, Tangjitgamol S, Puangsa-art S. Prognostic significanceof microvessel density and mast cell density for the survival of Thaipatients with primary colorectal cancer. J Med Assoc Thai2008;91:723–32.
84. GulubovaM, Vlaykova T. Prognostic significance ofmast cell numberand microvascular density for the survival of patients with primarycolorectal cancer. J Gastroenterol Hepatol 2009;24:1265–75.
85. Tomita M, Matsuzaki Y, Onitsuka T. Correlation between mast cellsand survival rates in patients with pulmonary adenocarcinoma. LungCancer 1999;26:103–8.
86. Takanami I, Takeuchi K, Naruke M. Mast cell density is associatedwith angiogenesis and poor prognosis in pulmonary adenocarcino-ma. Cancer 2000;88:2686–92.
87. Welsh TJ, Green RH, RichardsonD,Waller DA, O'Byrne KJ, BraddingP. Macrophage and mast-cell invasion of tumor cell islets confers amarkedsurvival advantage in non-small-cell lungcancer. JClinOncol2005;23:8959–67.
88. Carlini MJ, Dalurzo MC, Lastiri JM, Smith DE, Vasallo BC, PuricelliLI, et al. Mast cell phenotypes and microvessels in non-small celllung cancer and its prognostic significance. Hum Pathol 2010;41:697–705.
89. AaltomaaS, Lipponen P, PapinahoS, KosmaVM.Mast cells in breastcancer. Anticancer Res 1993;13:785–8.
90. Dabiri S, Huntsman D, Makretsov N, Cheang M, Gilks B, Bajdik C,et al. The presence of stromal mast cells identifies a subset ofinvasive breast cancers with a favorable prognosis. Mod Pathol2004;17:690–5.
91. Rajput AB, Turbin DA, Cheang MC, Voduc DK, Leung S, Gelmon KA,et al. Stromal mast cells in invasive breast cancer are a marker offavourable prognosis: a study of 4,444 cases. Breast Cancer ResTreat 2008;107:249–57.
92. della Rovere F, Granata A, Familiari D, D'Arrigo G, Mondello B, BasileG. Mast cells in invasive ductal breast cancer: different behavior inhigh and minimum hormone-receptive cancers. Anticancer Res2007;27:2465–71.
93. Xiang M, Gu Y, Zhao F, Lu H, Chen S, Yin L. Mast cell tryptasepromotes breast cancer migration and invasion. Oncol Rep 2010;23:615–9.
94. Ribatti D, FinatoN, Crivellato E, Guidolin D, LongoV,Mangieri D, et al.Angiogenesis and mast cells in human breast cancer sentinel lymphnodes with and without micrometastases. Histopathology 2007;51:837–42.
95. Palmu S, SoderstromKO, Quazi K, Isola J, Salminen E. Expression ofC-KIT and HER-2 tyrosine kinase receptors in poor-prognosis breastcancer. Anticancer Res 2002;22:411–4.
96. Ali G, Boldrini L, Lucchi M, Mussi A, Corsi V, Fontanini G. Tryptasemast cells in malignant pleural mesothelioma as an independentfavorable prognostic factor. J Thorac Oncol 2009;4:348–54.
97. HedstromG, BerglundM,Molin D, FischerM,NilssonG, ThunbergU,et al. Mast cell infiltration is a favourable prognostic factor in diffuselarge B-cell lymphoma. Br J Haematol 2007;138:68–71.
98. Tuna B, Yorukoglu K, Unlu M, Mungan MU, Kirkali Z. Association ofmast cells with microvessel density in renal cell carcinomas. Eur Urol2006;50:530–4.
99. Dimitriadou V, Koutsilieris M. Mast cell-tumor cell interactions: for oragainst tumour growth and metastasis? Anticancer Res 1997;17:1541–9.
100. Theoharides TC, Conti P. Mast cells: the Jekyll and Hyde of tumorgrowth. Trends Immunol 2004;25:235–41.
101. Galinsky DS, Nechushtan H. Mast cells and cancer–no longer justbasic science. Crit Rev Oncol Hematol 2008;68:115–30.
102. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflam-mation. Nature 2008;454:436–44.
103. Mantovani A, Locati M. Tumor-associated macrophages as aparadigm of macrophage plasticity, diversity, and polarization:lessons and open questions. Arterioscler Thromb Vasc Biol2013;33:1478–83.
104. Biswas SK, Mantovani A. Macrophage plasticity and interaction withlymphocyte subsets: cancer as a paradigm. Nat Immunol 2010;11:889–96.
105. Qian BZ, Pollard JW. Macrophage diversity enhances tumor pro-gression and metastasis. Cell 2010;141:39–51.
106. Starkey JR, Crowle PK, Taubenberger S. Mast-cell-deficient W/Wvmice exhibit a decreased rate of tumor angiogenesis. Int J Cancer1988;42:48–52.
107. Crowle PK, Starkey JR. Mast cells and tumor-associated angiogen-esis. In:Galli SJ, Austen KF, editors. Mast cell and basophil differen-tiation and function in health and disease. New York, NY: RavenPress, Ltd; 1989. p. 307–15.
108. Wedemeyer J, Galli SJ. Decreased susceptibility of mast cell-defi-cient KitW/KitW-vmice to the development of 1, 2-dimethylhydrazine-induced intestinal tumors. Lab Invest 2005;85:388–96.
109. Soucek L, Lawlor ER, Soto D, Shchors K, Swigart LB, Evan GI.Mast cells are required for angiogenesis and macroscopic expan-sion of Myc-induced pancreatic islet tumors. Nat Med 2007;13:1211–8.
110. Sinnamon MJ, Carter KJ, Sims LP, Lafleur B, Fingleton B, MatrisianLM. A protective role of mast cells in intestinal tumorigenesis. Car-cinogenesis 2008;29:880–6.
111. Wasiuk A, DaltonDK,SchperoWL,Stan RV, Conejo-Garcia JR, NoelleRJ. Mast cells impair the development of protective anti-tumorimmunity. Cancer Immunol Immunother 2012;61:2273–82.
112. Oka T, Kalesnikoff J, Starkl P, Tsai M, Galli SJ. Evidence questioningcromolyn's effectiveness and selectivity as a 'mast cell stabilizer' inmice. Lab Invest 2012;92:1472–82.
www.aacrjournals.org Cancer Immunol Res; 1(5) November 2013 279
Mast Cells in Tumor Biology
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from

2013;1:269-279. Cancer Immunol Res Thomas Marichal, Mindy Tsai and Stephen J. Galli Mast Cells: Potential Positive and Negative Roles in Tumor Biology
Updated version
http://cancerimmunolres.aacrjournals.org/content/1/5/269
Access the most recent version of this article at:
Cited articles
http://cancerimmunolres.aacrjournals.org/content/1/5/269.full#ref-list-1
This article cites 109 articles, 24 of which you can access for free at:
Citing articles
http://cancerimmunolres.aacrjournals.org/content/1/5/269.full#related-urls
This article has been cited by 11 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerimmunolres.aacrjournals.org/content/1/5/269To request permission to re-use all or part of this article, use this link
on February 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from