Mast cell disorders
109
Mast Cell Disorders By Wat Mitthamsiri, MD. Allergy and Clinical Immunology Fellow King Chulalongkorn Memorial Hospital
-
Upload
chulalongkorn-allergy-and-clinical-immunology-research-group -
Category
Health & Medicine
-
view
546 -
download
5
description
Mast Cell Disorders Presented by Watt Mitthamsiri, MD. September05, 2014
Transcript of Mast cell disorders

Mast Cell Disorders By
Wat Mitthamsiri, MD.Allergy and Clinical Immunology FellowKing Chulalongkorn Memorial Hospital

Previous issues
• How long is the life span of mast cells in circulation (not in tissue)?
J Hallgren and MF Gurich, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p14-28.

Previous issues
• What is non-pathological, physiological role of mast cell?– One of the first responder in innate defense
against infections• Location• Arrays of innate sensors:
– PRRs: TLR1-7 and TLR9, NLRP3– Complement products receptors– CRP, LPS-binding proteins, pentraxins, collectins– Sensors for other peptide signals from other cells
CP Shellburne and SN Abraham, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p162-185.

Ligands that can activate MCs
CP Shellburne and SN Abraham, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p162-185.

Ligands that can activate MCs
CP Shellburne and SN Abraham, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p162-185.

Microbial sensors of MCs
CP Shellburne and SN Abraham, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p162-185.

Previous issues
• What is non-pathological, physiological role of mast cell?– One of the first responder in innate defense
against infections• Arrays of weapons:
– Mediators– Cytokines– Antimicrobial peptides: Beta-defensins, cathelicidin
• Powerful response: Neutrophil recruitment
CP Shellburne and SN Abraham, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p162-185.

Previous issues
• What is non-pathological, physiological role of mast cell?– Protection against toxic substances• MC’s carboxypeptidase is required to limit effect of:
– Endothelin-1 (ET-1) peptide from peritonitis– Pit viper venom– Honeybee (Apis mellifera) venom
• MC’s proteases limit toxic effect of neurotensin, IL-6
CP Shellburne and SN Abraham, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p162-185.

Previous issues
• What is non-pathological, physiological role of mast cell?– Enhance adaptive immune response• MC-deficient mice had impaired T-cell activation and
had reduced DC migration• MCs remotely enhance lymphocytes sequestration in
lymph nodes by using TNF-a• Using MC-activating compound as an adjuvant with
some Ag can elicit protective immunity to the corresponding pathogen only in host with normal MC• MC activating compound can increase IgA secretion in
mucosal challangeCP Shellburne and SN Abraham, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p162-185.

Summary of MC’s defense model
CP Shellburne and SN Abraham, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p162-185.

Summary of MC’s defense model
CP Shellburne and SN Abraham, Mast Cell Biology: Contemporary and Emerging Topic, Springer Science+Business Media, 2011, p162-185.

Mast Cell Disorders By
Wat Mitthamsiri, MD.Allergy and Clinical Immunology FellowKing Chulalongkorn Memorial Hospital

Outline
• Classification and epidemiology• Pathogenesis• Clinical features• Pathology• Approach for diagnosis• Treatment• Prognosis

Classificationand
Epidemiology

Diseases of mast cells
P Bradding, H Saito., Middleton’s Allergy 8th edition, 2013, 228-251.DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
Excessive mast cell no/Fn • Localized
mastocytosis• Systemic
mastocytosis
Mast cell deficiency• Never been found

Localized mastocytosis
• Cutaneous mastocytosis – Urticaria pigmentosa/maculopapular cutaneous
mastocytosis (UP/MPCM)– Diffuse cutaneous mastocytosis (DCM)– Solitary mastocytoma
• Extracutaneous mastocytoma
Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Systemic mastocytosis• Indolent Systemic Mastocytosis (ISM)• Systemic Mastocytosis with Associated Clonal,
Hematologic Non–Mast Cell Lineage Disease (SM-AHNMD)
• Aggressive Systemic Mastocytosis (ASM)• Mast Cell Leukemia (MCL)• Mast Cell Sarcoma (MCS)• Monoclonal mast cell activation syndrome
(MMAS)• Mast cell activation syndrome (MCAS)Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Epidemiology• Unknown prevalence– Estimated 20,000-30,000 in the USA
• Male/female ratio of 1 : 1 to 1 : 3• Found in all ethnic backgrounds– More frequently reported in Caucasians
• May occur at any age• Familial occurrence is unusual
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Pathogenesis

Pathogenesis
KIT-dependent
Apoptosis inhibition
Other modifying mutation
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

KIT-dependent
AM Gilfillan and C Tkaczyk, Nature Reviews Immunology, 2006, 6:218-230

KIT-dependent
J Lennartsson and L Rönnstrand, Physiological ReviewsPublished 1 October 2012Vol. 92no. 4,1619-1649.AM Gilfillan and C Tkaczyk, Nature Reviews Immunology, 2006, 6:218-230
Other names:• Mast/stem cell growth
factor receptor (SCFR)• Proto-oncogene c-Kit• Tyrosine-protein kinase
Kit• CD117

KIT-dependent
J Lennartsson and L Rönnstrand, Physiological ReviewsPublished 1 October 2012Vol. 92no. 4,1619-1649.Chromosome image: http://ghr.nlm.nih.gov/gene/KIT
Chromosome4Position 12
(4q12)

KIT-dependent
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.Chromosome image: http://ghr.nlm.nih.gov/gene/KIT
• Most common mutation = ASP 816 VAL (D816V)• Inheriable to next generation? No
evidence• Other mutations:• V560G (MCL cell line)• D816Y, D816F, D816H, E839K (pediatric
mastocytosis)• F522C• R815K, D820G, V533D, V559A, del419,
K509I, and A533D (Exceedingly rare <1%)

Apoptosis inhibition
FIP1L1-PDGFRA fusion
PRKG2-PDGFRB fusion
Anti-apoptotic proteins
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

FIP1L1-PDGFRA
Oncogene in pluripotential hematopoietic progenitor cells
Results from ~800-kb interstitial deletion of chromosome 4q12
Patients:• ↑ Mast cells• Peripheral eosinophilia• ↑ Serum tryptase levels
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

PRKG2-PDGFRB
Systemic mastocytosis
Chronic basophilic leukemia
Rare
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Anti-apoptotic proteins
AB Gustafsson and RA Gottlieb, American Journal of Physiology - Cell Physiology,1 January 2007Vol. 292no. 1, C45-C51

Clinical features

Clinical features
Systemic symptoms
Dermatologic symtoms
GI symtoms
Musculoskeletal symptoms
Hepatosplenic symptoms
Neuropsychiatric sypmtomsDD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Systemic symptoms
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Caused by mast cell’s mediators

Systemic symptoms
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Caused by mast cell’s mediators

Systemic symptoms
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Flushing and episodic hypotension• Hypotension may be provoked by– Alcohol– Aspirin– Insect stings– Infection– Exposure to iodinated contrast materials
• No increased risk in bacterial, fungal, or viral infections

Dermatologic symptoms
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Urticaria pigmentosa (UP)/maculopapular cutaneous mastocytosis (MPCM)– Most common pattern of skin involvement in both
adults and children– Found in >90% of ISM patients– Found in ~50% of SM-AHNMD or ASM patients

DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Urticaria pigmentosa
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
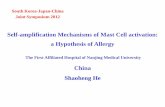
• Tend to spare palms, soles, face, and scalp• Rubbing the lesions => urtication and erythema
over and around the macules (Darier sign)• May be associated with pruritus exacerbated by:– Changes in temperature– Local frictionIngestion of hot beverages or spicy foods– Ethanol– Drugs
• Petechiae, ecchymoses, or telangiectasias may be present in or adjacent to UP lesions

Darier sign
http://www.allergikos.gr/%CE%BC%CE%B1%CF%83%CF%84%CE%BF%CE%BA%CF%85%CF%84%CF%84%CE%AC%CF%81%CF%89%CF%83%CE%B7/

Diffuse cutaneous mastocytosis
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Both UP and DCM
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• May have bullous eruptions with hemorrhage
• Blisters may erupt spontaneously or in association with infection or immunization

Solitary mastocytomas
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
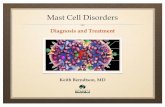
• Fairly common cutaneous variant• May be present at birth but usually before age
3 months• Usually spontaneously involute during
childhood• Solitary extracutaneous mastocytomas of the
lung have been reported in adults

Solitary mastocytomas
(http://dermaamin.com/site/images/clinical-pic/m/mastocytoma-solitary_mastocytoma/mastocytoma-solitary_mastocytoma1.jpg
)
DM Thappa,B. Jeevankumar, Indian Pediatrics 2005; 42:390

Mast cell sarcomas
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Exceedingly rare• Characterized by a tumor consisting of highly
atypical immature mast cells• Distant spread is possible• Leukemia phase may occur

Telangiectasia macularis eruptiva perstans (TMEP)
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Found <1% of mastocytosis patients• Reported only in adults• Characteristic skin lesion– Telangiectatic, red macule on a tan-brown
background– 2-6 mm in diameter– No sharply defined borders
• Pruritus, purpura, blister -> Uncommon• May become edematous when rubbed• Occasionally coexist with UP

Telangiectasia macularis eruptiva perstans (TMEP)
Ahmet Altiner MD, Julia Tzu MD, Rishi Patel MD, Shane Meehan MD, Miguel Sanchez, et al., Dermatology Online Journal 17 (10): 7

Telangiectasia macularis eruptiva perstans (TMEP)
Ahmet Altiner MD, Julia Tzu MD, Rishi Patel MD, Shane Meehan MD, Miguel Sanchez, et al., Dermatology Online Journal 17 (10): 7

GI symptoms
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• 80% of patients had significant GI symptoms• Abdominal pain = Most common GI symptom– Followed by diarrhea and N/V– 70% of patients with dyspeptic pain had evidence
of gastric acid hypersecretion– PU occured in 4-44% of all patients– Plasma concentration of histamine correlated with
basal acid output• GI bleeding -> Uncommon

GI symptoms
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Diarrhea, from:– Altered intestinal secretion– Structural disease of the small intestinal mucosa– Hypermotility or transit disorder
• Malabsorption– Found in 31% of patients– Usually not severe– Primarily occurred as mild steatorrhea with
impaired absorption of d-xylose or vitamin B12– Diffuse, small intestinal mucosal dysfunction has
been proposed as the cause

Musculoskeletal symptoms
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Uncertain etiology– Unless associated with osteopenia or osteoporosis
• Osteoporosis leading to pathologic fractures– Back pain from osteoporosis– Vertebral compression fractures– May be the initial manifestation of mastocytosis

Hepatosplenic symptoms
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• ~60% of patients had evidence of liver disease– 24% -> Hepatomegaly – 54% -> Elevated ALP and GGT• ALP levels correlated with GGT levels, hepatomegaly,
splenomegaly, and liver mast cell infiltration and fibrosis
• In SM-AHNMD or ASM patients– Elevated ALP -> More frequently– Reported 5 cases of ascites or portal hypertension
• Severe liver disease is uncommon– Except in patients with aggressive disease

Neuropsychiatric symptoms
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• In adults– Decreased attention span– Memory impairment– Irritability– May caused by therapeutic medicines as well as
circulating mediators• In children– No clear excess pathology– No specific behavioral pattern implicating
histamine overproduction was identified

Pathology

Pathology
Dermatologic pathology
Bone marrow pathology
Radiologic pathology
Liver pathology
Spleen pathology
Lymph nodes pathologyDD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Urticaria pigmentosa
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Increased mast cells (>/= 10x of normal) within the papillary dermis
• With variable extension throughout reticular dermis and into the subcutaneous fat
• Absence of other pathology• Gross skin examination must be correlated
with the number of mast cells in the skin

Urticaria pigmentosa
http://www.skinpathology.org/wp-content/uploads/Urticaria-Pigmentosa-Histopathology-1024x768.jpg

Urticaria pigmentosa
http://www.skinpathology.org/wp-content/uploads/Urticaria-Pigmentosa-Histology-1024x768.jpg

Diffuse cutaneous mastocytosis
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

TMEP
Ahmet Altiner MD, Julia Tzu MD, Rishi Patel MD, Shane Meehan MD, Miguel Sanchez, et al., Dermatology Online Journal 17 (10): 7

Bone marrow pathology
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Most common site of pathologic mast cell infiltrates in mastocytosis
• Most useful Bx site for pathologic diagnosis
• Majority of infiltrates are focal (may be diffuse in some cases)

Bone marrow pathology
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Often situated paratrabecularly
• Consist of nodular aggregates of spindle-shaped mast cells, which may be accompanied by lymphocytes and eosinophils

Bone marrow pathology
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Hypercellular marrow, as a prognostic factor– With ↓percentage of fat cells = Significant predictor
of poor prognosis– 1/3 of patients had associated hematologic disorders
• Dysmyelopoietic syndromes• Myeloproliferative disorders• Acute leukemia• Malignant lymphoma• Chronic neutropenia• Had significantly reduced 5-year survival rates• In most patients, hematologic disorder is detected after
mastocytosis is diagnosed

Bone marrow pathology
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• In mast cell leukemia– Diffuse infiltration by atypical, immature mast cells– Mast cells account >/= 10% of the peripheral WBC
• In aggressive mastocytosis with a terminal leukemic phase– Circulating mast cells appear late in the disease
course– Percentage of circulating mast cells is relatively
low

Bone marrow pathology
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• BM Mast cell hyperplasia in non-mast cell diseases– Uremia– Osteoporosis– Hematologic conditions (lymphomas,
preleukemias, leukemias)

Radiologic pathology
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.
• Radiographically detectable BM infiltration are up to 70% of patients– Proximal long bones = Most often affected– Followed by the pelvis, ribs, and skull
• Skeletal scintigraphy– More sensitive than radiographic surveys in
detecting and locating active lesions– May aid in evaluating the extent of disease and
disease progression

Liver pathology• Mast cell infiltration in liver– More severe in patients with SM-AHNMD or ASM– Correlates with hepatomegaly, splenomegaly, ALP
levels, and GGT levels• Portal fibrosis correlates with mast cell
infiltration and portal inflammation• Nodular regenerative hyperplasia, portal
venopathy, and venoocclusive disease may contribute to portal hypertension
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Spleen pathology• Most common finding = Trabecular fibrotic
thickening• Splenic mast cell lesions have been found in– Paratrabecular– Parafollicular– Follicular– Diffuse red pulp
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Spleen pathology
http://www.webpathology.com/image.asp?case=385&n=2

LN pathology• Most common location of infiltration =
Paracortical region• Less frequent– Parafollicular and follicular replacement– Medullary cord– Sinus infiltration
• May resemble follicular and T cell lymphomas, monocytoid B cell hyperplasia and lymphoma, Kaposi sarcoma, hairy cell leukemia, and histiocytosis X
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

LN pathology
John Lazarchick, http://imagebank.hematology.org/Content/740/3803/3803_full.JPG

LN pathology
John Lazarchick, http://imagebank.hematology.org/AssetDetail.aspx?AssetID=3804

Approach for diagnosis

Proposed algorithm
P. Valent, et al., Int Arch Allergy Immunol 2012;157:215–225.

Proposed algorithm
P. Valent, et al., Int Arch Allergy Immunol 2012;157:215–225.

Proposed algorithm
P. Valent, et al., Int Arch Allergy Immunol 2012;157:215–225.

Proposed algorithm
P. Valent, et al., Int Arch Allergy Immunol 2012;157:215–225.

Proposed algorithm
P. Valent, et al., Int Arch Allergy Immunol 2012;157:215–225.
= WHO’s criteria

Classification of MCAS
P. Valent, et al., Int Arch Allergy Immunol 2012;157:215–225.

Classification of MC disorders
P. Valent, et al., Int Arch Allergy Immunol 2012;157:215–225.

Diagnosis(WHO’s criteria for Dx)

Cutaneous mastocytosis• Typical clinical findings of:– Urticaria pigmentosa/maculopapular cutaneous
mastocytosis (UP/MPCM)– Diffuse cutaneous mastocytosis (DCM)– Or solitary mastocytoma
• With typical infiltrates of mast cells in a multifocal or diffuse pattern on skin biopsy
Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Systemic mastocytosis• 1 major+1 minor, or 3 minor criteria are
required
– Major Criterion • ≥15 foci of mast cells infiltrates in sections of bone
marrow and/or another extracutaneous organ• (Confirmed by tryptase immunohistochemistry or
other special stains)
Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Systemic mastocytosis• 1 major+1 minor, or 3 minor criteria are
required– Minor Criteria• >25% of mast cells are abnormal:
– Spindle shape or atypical morphology (in Bx of BM/other extracutaneous organs)
– Immature or atypical morphology (in BMA specimens)
• Detection of activating point mutation at codon 816 of KIT in BM, blood, or another extracutaneous organ• Mast cells in BM, blood, or another extracutaneous
organ express CD117 with CD2 and/or CD25• Serum total tryptase persistently >20 ng/mL (without
associated clonal myeloid disorder)Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Varients of mastocytosis• “B” findings – >30% infiltration by mast cells (focal, dense
aggregates) in BMBx and/or serum total tryptase >200 ng/mL
– Signs of dysplasia or myeloproliferation in non–mast cell lineages (but insufficient for Dx of a hematopoietic
neoplasm) + normal/slightly abnormal blood counts– Hepatomegaly without impairment of LFT, and/or
palpable splenomegaly without hypersplenism, and/or lymphadenopathy.
Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Varients of mastocytosis• “C” findings :– BM dysfunction: >/= 1 of
• ANC <1.0 x109/L• Hb <10 g/dL• Platelets <100 × 109/L)• And no obvious non–mast cell hematopoietic malignancy
– Palpable hepatomegaly + impaired LFT, ascites, and/or portal hypertension
– Skeletal involvement + large osteolytic lesions and/or pathologic fractures
– Palpable splenomegaly + hypersplenism– Malabsorption + Wt loss (from GI mast cell infiltrates)Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Varients of mastocytosis• Indolent Systemic Mastocytosis (ISM) – Meets criteria for systemic mastocytosis– No “C” findings– No evidence of an associated clonal, hematologic
non–mast cell lineage disease (AHNMD) – In this variant the mast cell burden is low, and skin
lesions are usually present • BM mastocytosis – ISM + BM involvement, but no skin lesions
• Smoldering systemic mastocytosis – ISM, with >/=2 “B” findings and no “C” findings Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Varients of mastocytosis• Systemic Mastocytosis with Associated Clonal,
Hematologic Non–Mast Cell Lineage Disease (SM-AHNMD) – Meets criteria for SM– And criteria for AHNMD• (MDS, MPN, AML, lymphoma, or other hematologic
neoplasm that meets criteria for distinct entity in WHO classification)
Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Varients of mastocytosis• Aggressive Systemic Mastocytosis (ASM) – Meets criteria for SM with one or more “C” findings– No evidence of mast cell leukemia.– Usually without skin lesions– Lymphadenopathic mastocytosis with eosinophilia– Progressive lymphadenopathy
• With peripheral blood eosinophilia• Often with extensive bone involvement, and
hepatosplenomegaly• Usually without skin lesions
– Cases with rearrangement of PDGFRA are excluded Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Varients of mastocytosis• Mast Cell Leukemia (MCL) – Meets criteria for SM– BMBx: Diffuse infiltration by atypical, immature
mast cells– BMA smears: >/= 20% mast cells + mast cells >/=
10% peripheral WBC• Variant:– Leukemic mast cell leukemia as above– <10% of WBC are mast cells– Usually without skin lesions
Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Varients of mastocytosis• Mast Cell Sarcoma (MCS) – Unifocal mast cell tumor– No evidence of SM– Destructive growth pattern; high-grade cytology
• Extracutaneous Mastocytoma – Unifocal mast cell tumor– No evidence of SM. – No skin lesions; nondestructive growth pattern;
low-grade cytology
Horny H-P, et al. Mastocytosis. In: Swerdlow SH, et al, editors. WHO classification of tumors of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Varients of mastocytosis• Proposed additional criteria – Monoclonal mast cell activation syndrome (MMAS)• BM examination to have met 1-2 minor diagnostic criteria
for mastocytosis• But lack the full diagnostic criteria for systemic
mastocytosis
– Mast cell activation syndrome (MCAS)• Episodic allergy-like signs and symptoms (e.g., flushing,
urticaria, diarrhea, wheezing) involving >/=2 organ systems• Without identifiable etiology
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Other surrogate markers• Serum histamine and 24-hr urinary histamine
metabolites (N-methylhistamine, and methylimidazoleacetic acid)
– Less often used– Disadvantages• Variability among healthy individuals and patients• Difficulty in assay standardization• False-positive• Easily altered result• Nonspecific
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Other surrogate markers• Metabolites of arachidonic acid– Urinary PGD-M or 9α,11β- dihydroxy-15-oxo-
2,2,18,19-tetranorprost-5-ene-1,20-dioxic acid– Plasma thromboxane B2 and its metabolites– Limitations• Source is not exclusively limited to mast cells ->
insufficient specificity for diagnostic purposes
• 24-hr urinary 5-hydroxyindoleacetic acid and urinary metanephrines– For R/O carcinoid tumor/pheochromocytoma
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Other W/U• Other tissue Bx• Bone scans or skeletal surveys• Abdominal U/S or CT scan• Upper GI series• Small bowel radiography• Endoscopy (to R/O PU or GERD)
• Dual-energy x-ray absorptiometry (DEXA) scan (to monitor osteoporosis)
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Treatments

Treatments
MC-mediated symptoms
GI symptoms
Hematologic abnormality
Osteoporosis
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

MC-mediated symptoms• Epinephrine– Rx episodes of systemic hypotension– Patients should be taught to administer this
medication themselves– Intensive therapy as for anaphylaxis might be needed
• H1 & H2 receptor antagonist– Mainly reduce flushing– Anti-H1 first, if inadequate response, then use anti-
H2• LTRA– Add on to antihistamines to help flushing
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

MC-mediated symptoms• Disodium cromoglycate (cromolyn sodium) – Inhibits degranulation of mast cells– Relief of GI complaints– Not reduce plasma or urinary histamine levels
• 8-methoxypsoralen with PUVA (or even natural sunlight in some cases)– Relieve pruritus&whealing in adult after 1-2 mo of Rx– Associated with transient decrease dermal mast cells– Pruritus relapsed in 3-6 months after discontinuation– Used only in patients with extensive cutaneous
disease unresponsive to other therapyDD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

MC-mediated symptoms• Topical steroids with plastic wrap occlusion
for 8 hr/day x 8-12 wks– Used to treat UP or DCM– Number of mast cells decreases as lesions resolve– Lesions recur after Rx discontinuation but may be
last for up to 1 year
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

GI symptoms• Gastric acid hypersecretion symptoms (peptic
symptoms and PU)– H2 RA and PPI
• Diarrhea– Anticholinergics -> partial relief
• Severe malabsorption– Oral steroids
• Ascites– Portacaval shunt
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Osteoporosis• Calcium supplementation• Estrogen replacement (postmenopausal women)• Bisphosphonates• Narcotic analgesics– May potentiate mast cell degranulation
• Radiotherapy– Palliative role in decreasing bone pain in patients with
aggressive forms of disease• IFN-α2b– Relieve musculoskeletal pain– Improve bone mineralization
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Hematologic abnormality• Managed as dictated by associated specific
hematologic abnormality• IFN-α2b and 2-chloro-2-deoxyadenosine
(cladribine, 2-CdA)– Potential first-line therapy for patients with
aggressive forms • BMT– Good for associated hematologic disorders– Poor effect on mast cell hyperplasia
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Hematologic abnormality• Imatinib mesylate – Approved for Rx of aggressive forms of mastocytosis in
patient without D816V mutation– May be useful in unusual presentations of mastocytosis,
which are associated with novel mutations in c-kit– Patients with increased mast cells + peripheral
eosinophilia + FIP1L1-PDGFRA fusion oncogene also respond
– Mutational analysis of lesions are essential before Rx• Other tyrosine kinase inhibitors eg. midostaurin
(PKC412)– Able to inhibit KIT with the D816V mutation in vitro– Now in clinical study
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Hematologic abnormality• Chemotherapy– Unable to produce remission– Unable to prolong survival in MCL– Has no place in the treatment of indolent
mastocytosis– But may be considered for advanced disease
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Hematologic abnormality• Splenectomy– May improve survival times in mastocytotic
patients with with poor prognosis• Radiotherapy– Used in the management of refractory bone pain
in patients with aggressive disease• BMT– May be considered for extremely ill patients, – May yield a better prognosis if mast cell
suppression is attempted before BM
DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Prognosis

Prognosis• Patients with CM only = Best prognosis, followed by
those with ISM• >50% of children with isolated UP resolve by
adulthood• UP in adulthood may evolve into systemic disease• Occasionally, ISM converts to SM-AHNMD• Course depends largely on prognosis of specific
hematologic disorder and response to Rx• Mean survival of MCL pt: <12 months• Survival time ASM pt: 2-4 years (with aggressive
symptomatic management)DD Metcalfe., Middleton’s Allergy 8th edition, 2013, 1224-1236.

Take Home Message• Mast cell disorders vary greatly in clinical
presentations • Primary pathomechanism is the activating
mutation in KIT • Signs and symptoms are caused by:– Mast cell mediators– Increased mast cell burden– Associated hematologic disorder
• Treatments– Symptomatic Rx for mastocytosis– Specific Rx for associated hematologic disorders

Thank you