



Mary Ann Ferguson,Pharmacist St Josephs Health Care ... · PDF fileIdentify and address...
56
Mary Ann Ferguson,Pharmacist St Josephs Health Care Concurrent Disorders Inpatient Unit [email protected]
Transcript of Mary Ann Ferguson,Pharmacist St Josephs Health Care ... · PDF fileIdentify and address...

Mary Ann Ferguson,Pharmacist
St Josephs Health Care
Concurrent Disorders Inpatient Unit

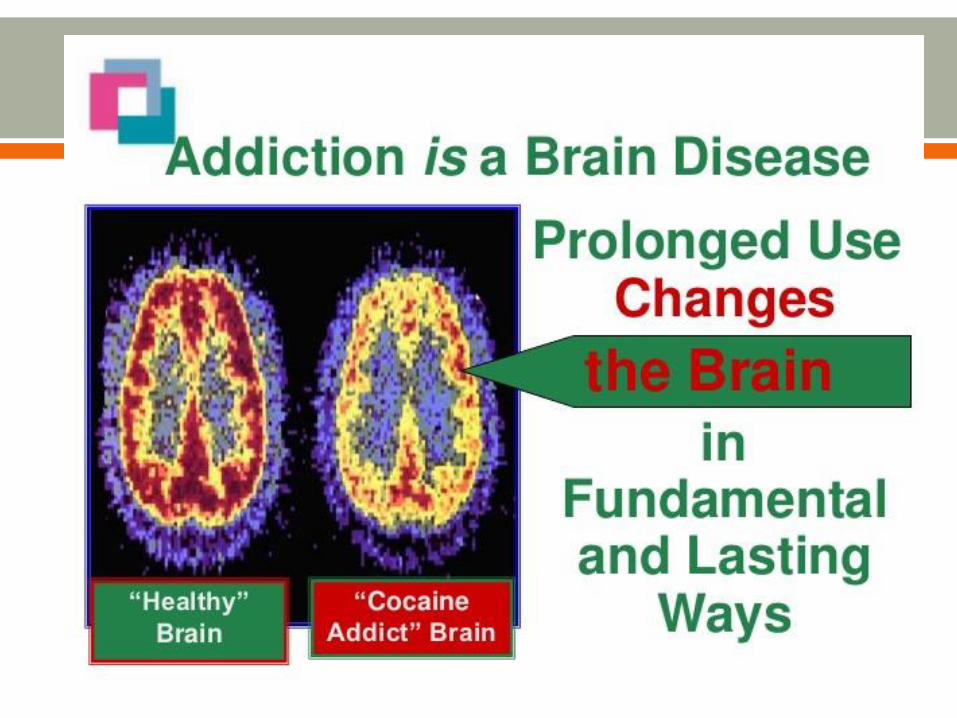
Medication should be considered as part of the treatment
plan for addictions/substance use disorders:
A- Never
B-Rarely
C-Sometimes
D-Always

Identify and address barriers to pharmacotherapy use in
addiction
Provide general overview of most commonly utilized
pharmacotherapies for opioid and alcohol use disorders

“Because of the difficulties that many
alcoholics have with drugs, some members
have taken the position that no one in A.A.
should take any medication. While this
position has undoubtedly prevented relapses
for some, it has meant disaster
for others.”
“No A.A. member should “play doctor”; all
medical advice and treatment should come
from a qualified physician”

The 4 Cs: o Loss of Control of use of the substance
o Compulsive use or Craving
o Continued use despite adverse Consequences
CSAM Definition: o A primary, chronic disease characterized by impaired control over the
use of a psychoactive substance or behaviour.
o Clinically the manifestations occur along biological, psychological, social & spiritual dimensions.
o Like other chronic diseases, it can be progressive, relapsing & fatal. o Common features are change in mood, relief from negative
emotions, provision of pleasure, preoccupation with the use of substances or ritualistic behaviour; & continued use of substances &/or engagement in behaviour despite adverse physical, psychological &/or social consequences.
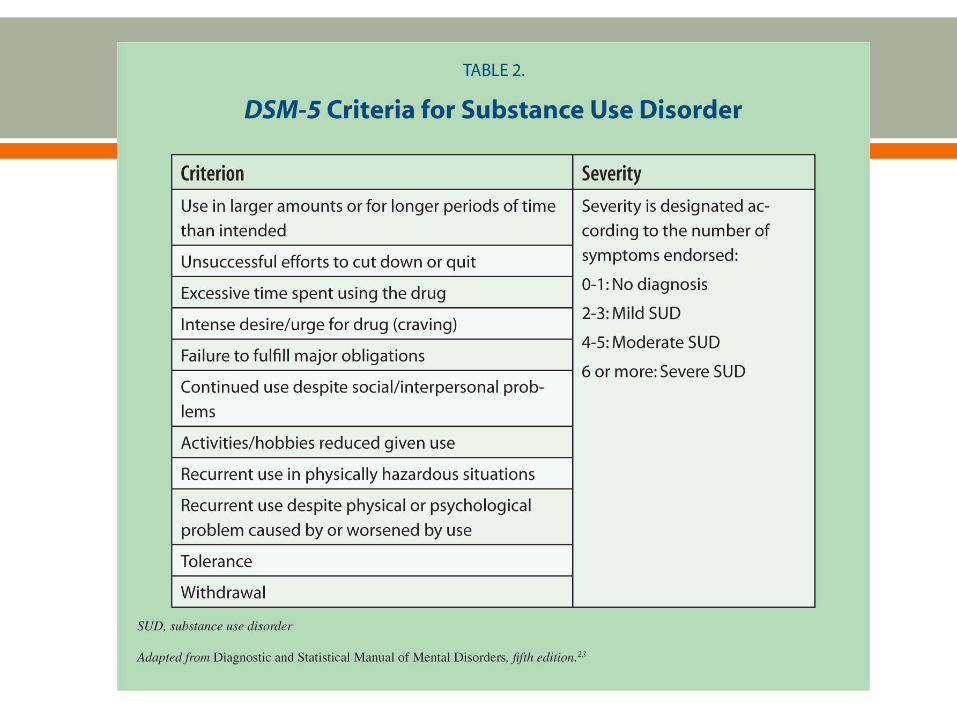
DSM-IV used the diagnoses substance abuse and substance dependence. This is NOT the same thing as physical dependence
Long term use of many drugs can result in tolerance and/or dependence
o This can happen with drugs that do not have the potential for addiction
o For some drugs, tolerance and dependence will develop in all who use it, but not everyone who becomes tolerant or dependent will become addicted
Addiction is characterized by craving for the drug and using it even when it causes harm.

Defined by what happens when you STOP taking a drug
o Withdrawal signs and symptoms!
Core symptom of addiction, but can occur in the absence of
addiction
What tends to fuel addiction, as once tolerance develops,
the euphoria from drugs tends to subside, and use fuelled
by avoidance of withdrawal symptoms.

Tolerance:
o The brain adapts to the constant presence of the drug
o It takes more drug to get the euphoria/desired effect
o Tolerance to some side effects (ie- respiratory
depression with opioids) doesn’t develop so quickly--
always risk of death from overdose
o Tolerance can be lost if a person stops using (ie- they
have been in prison or jail). Returning to previous doses
can result in fatal overdoses*

Risk of addiction affected by the speed with which the drug
enters the brain, the degree of fluctuation vs constancy in
drug concentration
Route of administration:
-Injection and smoking are greatest
risk of addiction due to rapid
increases of drug, followed by rapid
decreases

Half Life
-Time it take for drug to be eliminated from body
-Drugs with shorter half lives tend to be more liable to addiction
The more often a drug needs to be taken, the more a behaviour is
practiced, and the greater tendency to become habitual

Reward Pathways:
o Not a ‘smart’ part of the brain
• or the part of the brain that has to do with you wallet, or the number of
times you go to church
o Have less control over it than we think we do (area responsible for
holding breath, holding bladder)
o Fueled primarily by DOPAMINE!

The symptoms of which mental health
diagnosis can be explained partly by over
activity of dopamine?

Which of the following is NOT a treatment for substance use
disorders?
A- Opioid replacement therapy
B- Substance detox
C- 12 Step Programs
D- Individual Counselling

Which of the following are dangerous in withdrawal?
A- Benzodiazepines
B- Alcohol
C- Crystal Meth
D- Opioids
E- A and B
F- All of the above
G- None of the above

Withdrawal o Physical symptoms; “flu-like”, myalgias, abdominal cramps, diarrhea,
nausea, chills
o Psychological symptoms; anxiety, cravings, insomnia, fatigue, depression
o Objective signs; lacrimation, rhinitis, yawning, sweating, piloerection, restlessness, uncomfortable, mild tachycardia/hypertension
o Risks; relapse, overdose, suicide, miscarriage/premature labour
Physical symptoms peak at 2-3 days after last use and resolve by 5-10 days---psychological symptoms can last for weeks and months.
Symptomatic treatment: clonidine, loperaminde (IMODIUM), antiemetic (GRAVOL), acetaminophen/NSAID’s, benzodiazepines

1-Opioid Replacement Therapy
2- Safe injection sites
3- Access to Naloxone (NARCAN)
http://www.theglobeandmail.com/opinion/albertas-fentanyl-
response-is-tragic-the-solution-is-simple/article27231062/

1- Methadone Maintenance
Therapy (MMT)
2- Buprenorphine Maintenace
Therapy (BMT)
Unfortunately,
detoxification
followed by
abstinence has
shown little
success in
reducing illicit
opioid use

Evidence clearly shows that MMT has a positive impact on:
• Retention in treatment
• Illicit opioid use
Evidence is less clear but suggestive that MMT has a positive impact on:
• Mortality
• Illicit drug use (nonopioid)
• Drug-related HIV risk behaviors
• Criminal activity
Evidence suggests that MMT has little impact on:
• Sex-related HIV risk behaviors
Fullerton et al., 2014

Evidence clearly shows that BMT has a positive impact
compared with placebo on:
• Retention in treatment
• Illicit opioid use
Evidence is mixed for its impact on:
• Nonopioid illicit drug use

Medications are only part of the puzzle!
o Pharmacotherapy assists with physiological
symptoms psychosocial therapy helps patients
maintain pharmacotherapy pharmacotherapy
helps patients maintain psychosocial therapy
NIH 1997: “The safety and efficacy of narcotic
agonist maintenance treatment have been
unequivocally established”
2008 WHO: “Substitution therapies such as
methadone remain the most promising method of
reducing drug dependence.”

President Barack Obama tackled the opioid epidemic on Wednesday by telling health care providers across the country that access to medication-assisted treatment must be expanded.
For decades, those treating opioid addiction ignored the scientific consensus that the best approach involved medications approved by the Food and Drug Administration, coupled with counseling. Instead, the treatment industry insisted on a model known as "abstinence," in which any prescription medication aimed at addressing a patient's opioid use disorder was forbidden.
He released an order giving federal agencies with health care responsibilities 90 days to identify barriers to MAT and to come up with ways to remove them.
Full mu opioid agonist with long half-life
Does not induce euphoria in dependent patients—and
reduced euphoric effects of exogenous opioids.
Goal is to reach a stable dose where withdrawal and
cravings are supressed for 24 hours
Will not treat acute pain
Also an NMDA antagonist—may help prevent or reverse
opioid tolerance and hyperalgesia so patient can be
maintained on stable dose.
Only needs to be taken once daily.
Slow peak (at 2.5- 4 hours)
o No quick rush, or sudden crash leading to withdrawal.
o Long time to get to ‘steady-state’ dose
• Patients are at very high risk of overdose during induction phase (can
take 2-8 weeks to stabilize patients)
Mixed with Tang (to prevent injection)
Can only be prescribed by authorized methadone
prescriber.
Stable dose for most patients between 50-120mg
Any carries must be safely stored
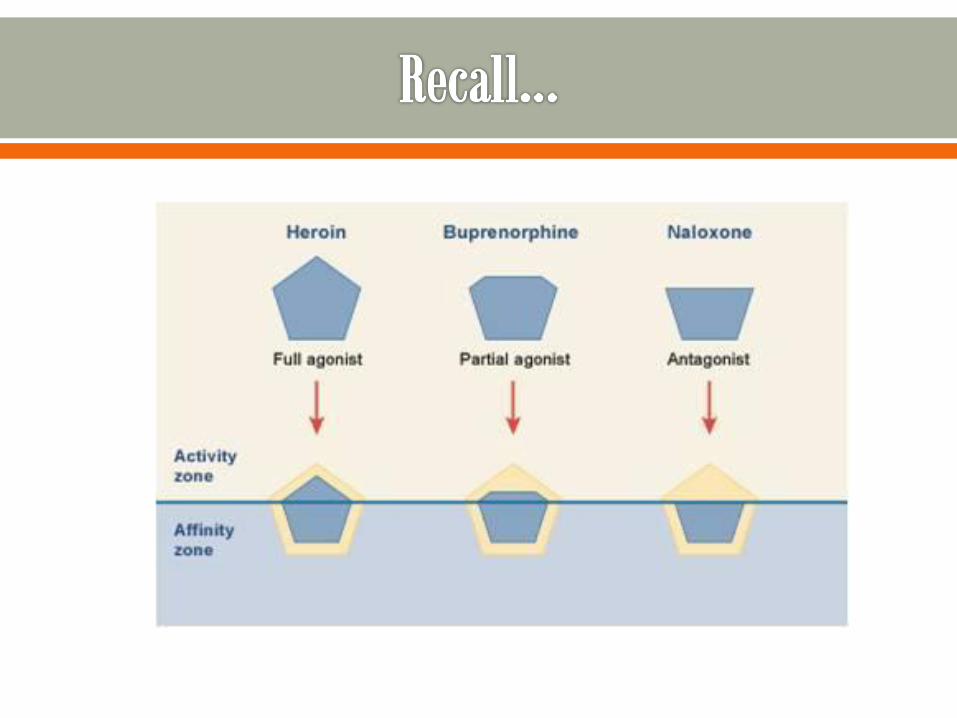
Partial Agonist at mu opioid receptor and antagonist at kappa* opioid receptor
High affinity for mu receptor
o Can displace full agonist opioids such as heroin
o Dissociates slowly from the receptors
No formal certificate required to prescribe (unlike methadone)
Preferred for:
o Pts who are at higher risk of methadone toxicity (elderly, BZD pt)
o Adolescents/young adults
o Short history of use
o Patients in communities where methadone treatment is unavailable
o Patients where pharmacy not open weekends.
o Patient preferences

Impacts:
1- Safety
2- Induction
3- Efficacy?

Ceiling effect makes respiratory depression less likely
o CAN occur with excessive use of EtOH , benzodiazepines or other
CNS depressants.

Because is partial agonist, will blunt response of any full
agonist opioids present, and induce a sudden withdrawal.
For this reason, started after patient has started entered
moderate withdrawal (and will then be experienced as
relieving, not causing, withdrawal.)



Advantages of buprenorphine over methadone:
Less side effects , including QTc prolongation
Less risk of overdose
Can be prescribed by primary care physicians.
Faster titration/stabilization period
Longer duration of action can mean more flexible dosing
In theory, less withdrawal when tapering (?in practice)
Disadvantages of buprenorphine over methadone:
COST $$$ (only covered by ODB by LU Code)
Have to be in withdrawal to initiate
Ceiling effect
**It is far easier to transition from buprenorphine to methadone, than from methadone to buprenorphine
PROGRAM CHARACTERISTICS MORE IMPORTANT THAN DRUG USED

Naloxone is an opioid antagonist
Not well absorbed under the tongue, so does not interfere
with the actions of the buprenorphine
However, if tablets crushed and injected, naloxone will block
effects of opioids and cause withdrawal for those with
opioids in the system.

Free Naloxone Kits for persons using or who have used opioids
Call 905 546 2424 x 7475 to arrange for in-home overdose training and
naloxone kits
Also available at Street Health Clinic (Wesley Centre and Urban Core) and
the AIDS Network.

The VAN (905) 317 9966
Elizabeth Fry Society
Wesley Health Clinic
The AIDS Network
Hamilton Urban Core Community Health Centre
East End Sdexual Health Clinic
Mountain Sexual Health Clinic
Dundas Sexual Health Clinic
Waterdown Sexual Health Clinic
ADGS

Block opioid receptor (antagonist) and reduces euphoric effect from drinking
Reduces heavy drinking and helps patients achieve and maintain abstinence
Do not need to abstain from alcohol prior to starting
Only covered by EAP—criteria: in psychosocial treatment
Side effects- nausea, elevated liver enzymes
Contra-indications
o On opioids
o Liver dysfunction
o Elevated liver enzymes- AST ALT (>3x normal)
o Pregnancy

Antagonizes glutamate receptors (excitatory neurotransmitter)
Does not reduce heavy drinking
Helps patients maintain abstinence Only effective if patients have been abstinent for at least several days
Covered by EAP—Criteria: in psychosocial treatment/program, abstinent for at least 4 days, contraindication or side effect from naltrexone.
Side effects: nausea, agitation
Contraindications:
o Significant kidney disease
o Pregnancy

Blocks conversion of acetaldehyde to acetate and causes build-up of acetaldehyde, leading to a very unpleasant reaction if alcohol ingested.
? Effective when taken under supervision
o No longer first line recommendation!
Side effects:- Hepatitis, neuropathy, depression, psychosis
Contra indications: elderly, cardiac disease, liver dysfunction, psychosis, cognitive dysfunction, pregnancy
MUST be abstinent for at least 2 days prior to initiation
Reaction can happen up to 7 days after stopping medication
NOT available commmercially. Must be compounded at specialty pharmacies.

Topiramate (TOPAMAX)
Ondansetron (ZOFRAN)
Baclofen
Gabapentin