Martin R. Cowie Professor of Cardiology Imperial College ...
37
Martin R. Cowie Professor of Cardiology Imperial College London (Royal Brompton Hospital) [email protected] @ProfMartinCowie
Transcript of Martin R. Cowie Professor of Cardiology Imperial College ...
Martin R. Cowie
Professor of Cardiology
Imperial College London
(Royal Brompton Hospital)
@ProfMartinCowie
Declaration of interests
• Research grants from ResMed, Boston Scientific, St Jude Medical, Bayer
• Consultancy advice and speaker’s fees from Medtronic, ResMed, Boston Scientific, St Jude Medical, Respicardia, Servier, Pfizer, Novartis, Roche Diagnostics, Sorin, Boehringer-Ingelheim, Vifor, Fire1Foundry, Neurotronik
• Non-Executive Director of National Institute for Health and Care Excellence (NICE): but opinions expressed are my own
Today’s talk
Advanced heart failure
– “Requiring assessment for transplant, MCS or palliative care”,
typically: • Inotrope dependent, and/or
• symptoms at rest, or with minimal exertion, and cannot perform many activities of daily living
• peak MVO2 < 14 mls/kg/min
• 6MWT < 300m
• Failing or intolerant of conventional HF therapy
• Requiring repeated hospitalization for more intensive management
• Estimated 1-year survival by the SHFM of <80%
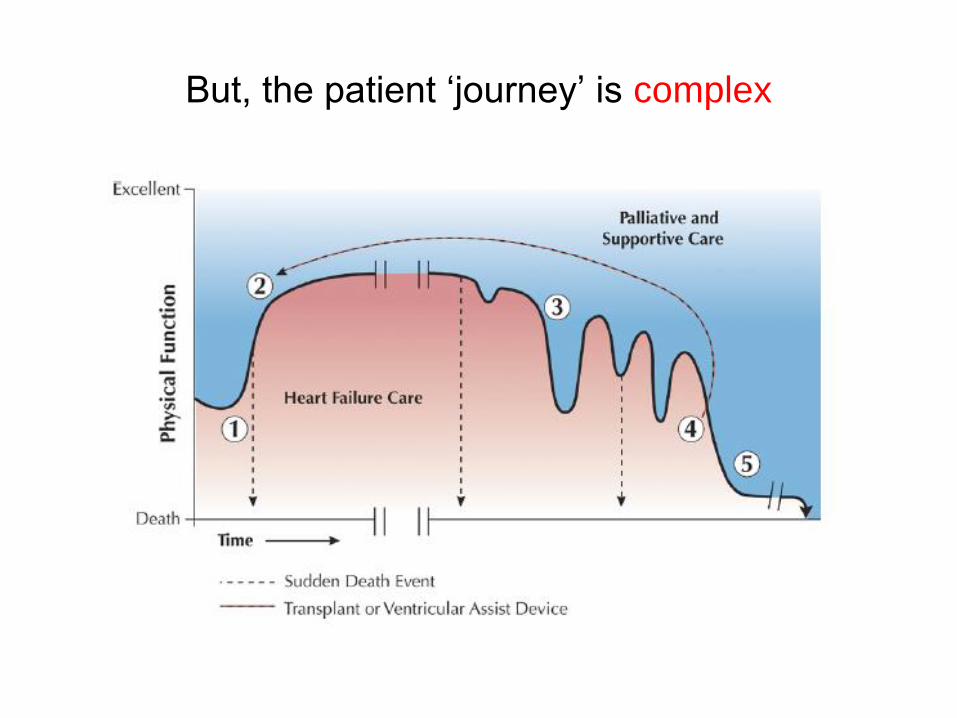
But, the patient ‘journey’ is complex
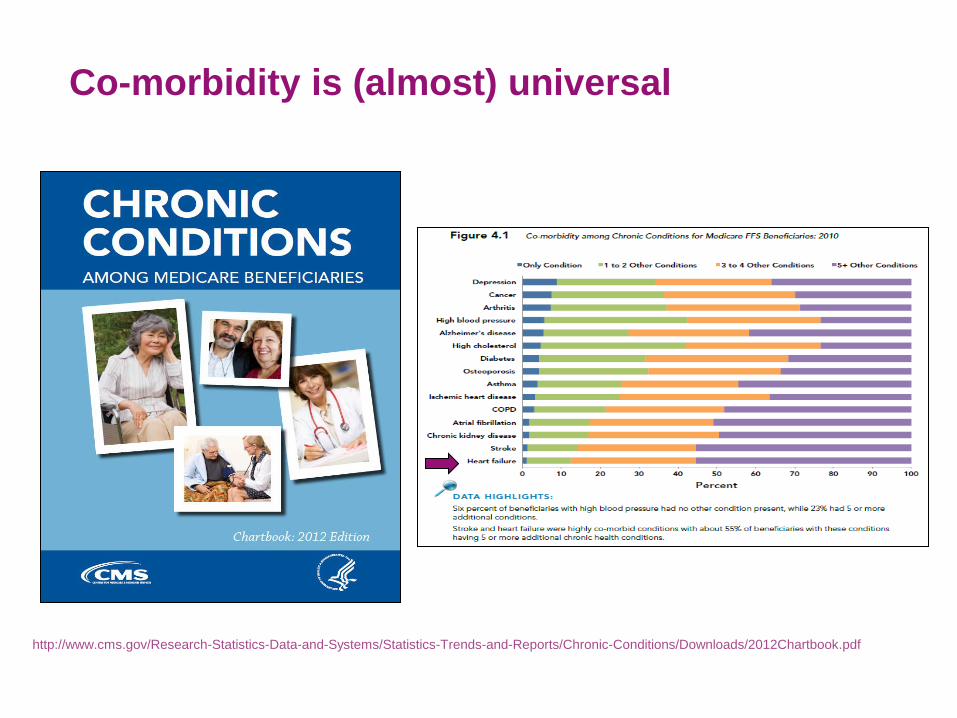
Co-morbidity is (almost) universal
http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Chronic-Conditions/Downloads/2012Chartbook.pdf
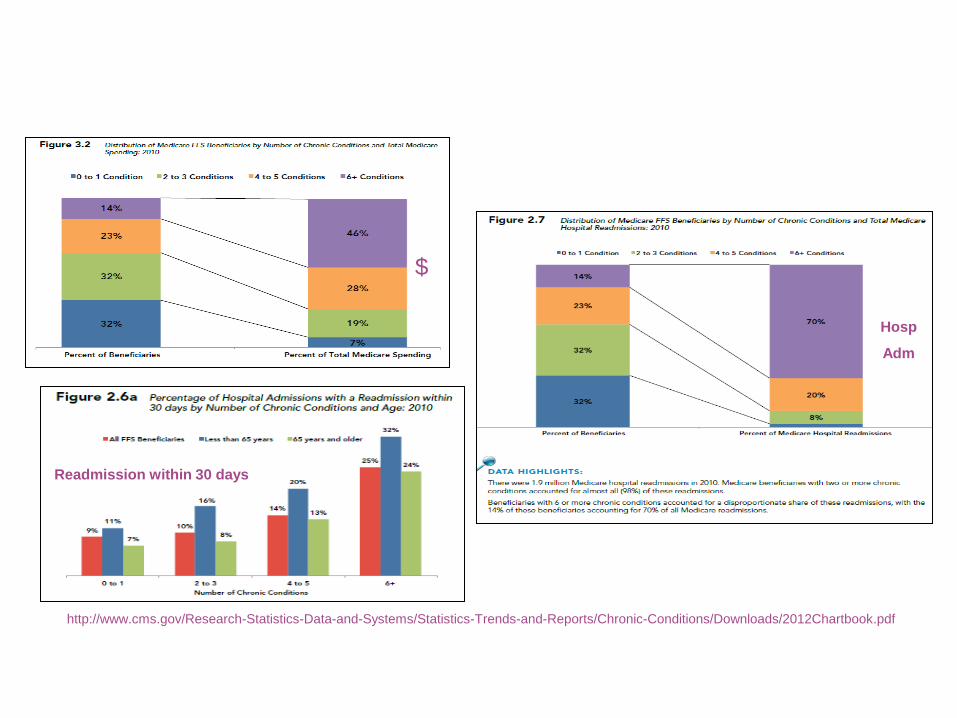
http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Chronic-Conditions/Downloads/2012Chartbook.pdf
$
Hosp
Adm
Readmission within 30 days
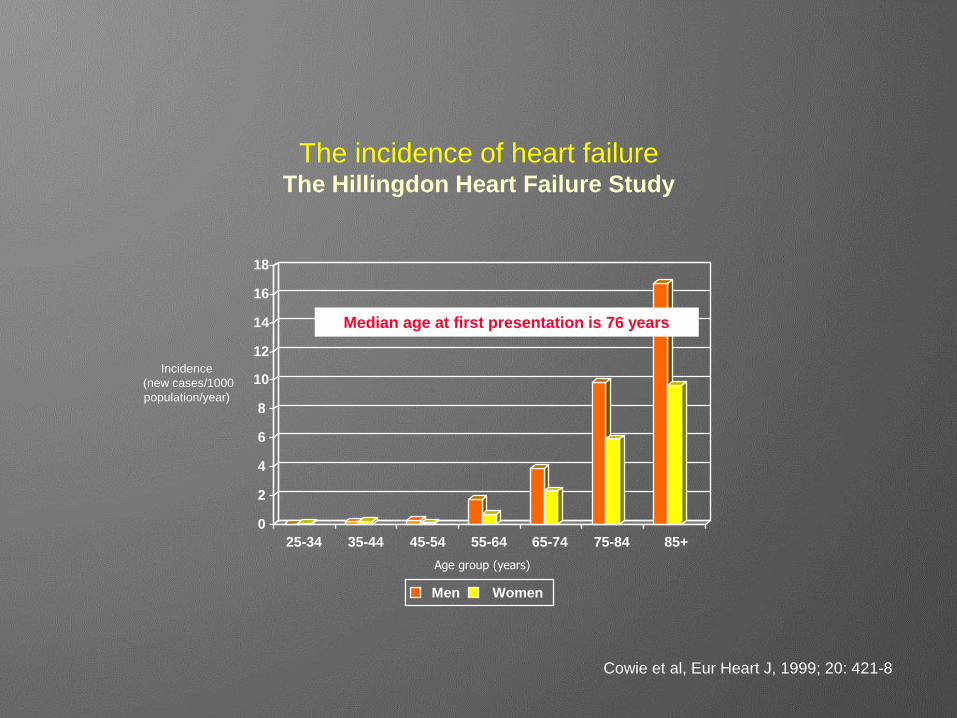
The incidence of heart failure The Hillingdon Heart Failure Study
0
2
4
6
8
10
12
14
16
18
25-34 35-44 45-54 55-64 65-74 75-84 85+
Men Women
Incidence
(new cases/1000
population/year)
Age group (years)
Cowie et al, Eur Heart J, 1999; 20: 421-8
Median age at first presentation is 76 years
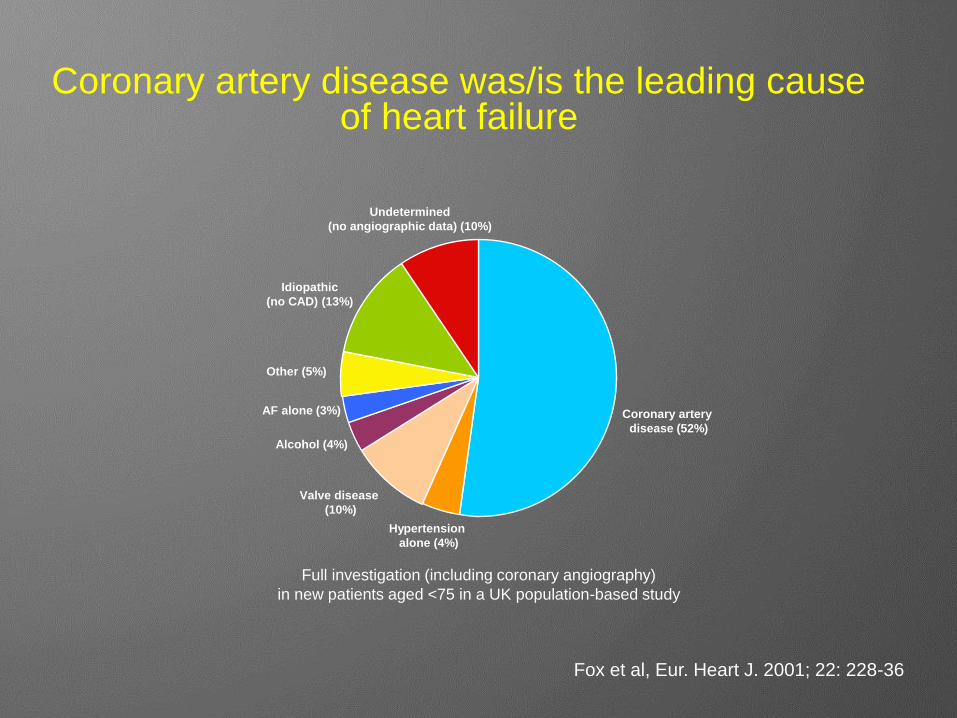
Coronary artery disease was/is the leading cause of heart failure
Fox et al, Eur. Heart J. 2001; 22: 228-36
Full investigation (including coronary angiography)
in new patients aged <75 in a UK population-based study
Coronary artery
disease (52%)
Hypertension
alone (4%)
Valve disease
(10%)
Alcohol (4%)
AF alone (3%)
Other (5%)
Idiopathic
(no CAD) (13%)
Undetermined
(no angiographic data) (10%)
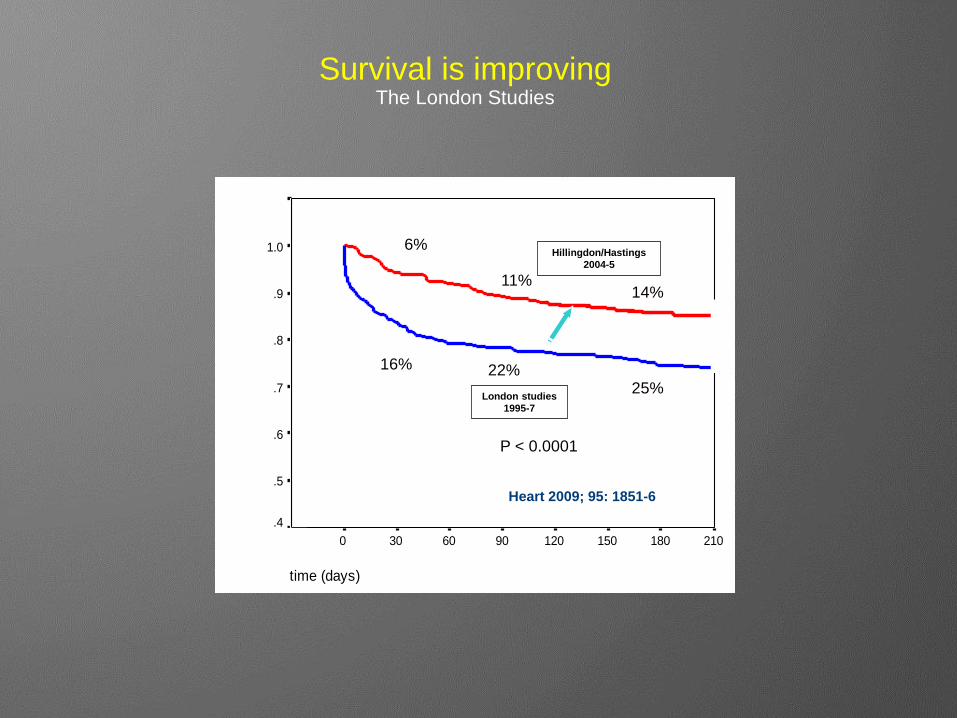
time (days)
2101801501209060300-30
Cum
ula
tive s
urv
ival
1.1
1.0
.9
.8
.7
.6
.5
.4
Hillingdon/Hastings
2004-5
London studies
1995-7
6%
11% 14%
16% 22% 25%
P < 0.0001
Survival is improving The London Studies
Heart 2009; 95: 1851-6
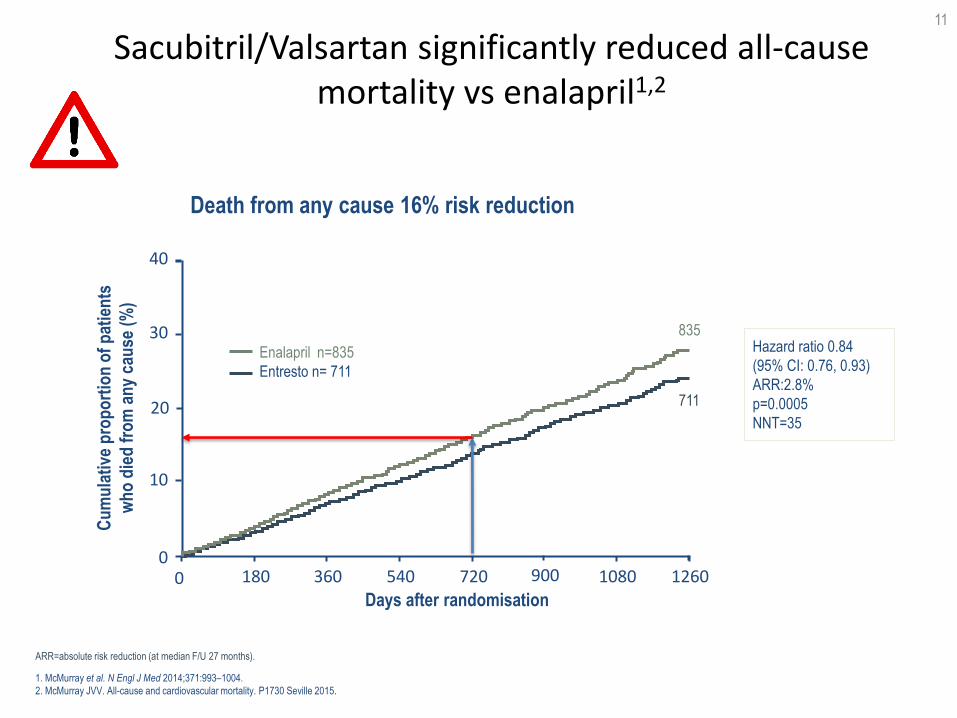
Sacubitril/Valsartan significantly reduced all-cause mortality vs enalapril1,2
11
1. McMurray et al. N Engl J Med 2014;371:993–1004.
2. McMurray JVV. All-cause and cardiovascular mortality. P1730 Seville 2015.
Hazard ratio 0.84
(95% CI: 0.76, 0.93)
ARR:2.8%
p=0.0005
NNT=35
ARR=absolute risk reduction (at median F/U 27 months).
30
10
0 0 1080 900
Cu
mu
lati
ve p
rop
ort
ion
of
pat
ien
ts
wh
o d
ied
fro
m a
ny
cau
se (
%)
Enalapril n=835
Entresto n= 711
Days after randomisation
20
40
180 360 540 720 1260
835
711
Death from any cause 16% risk reduction
What about the hospital perspective?
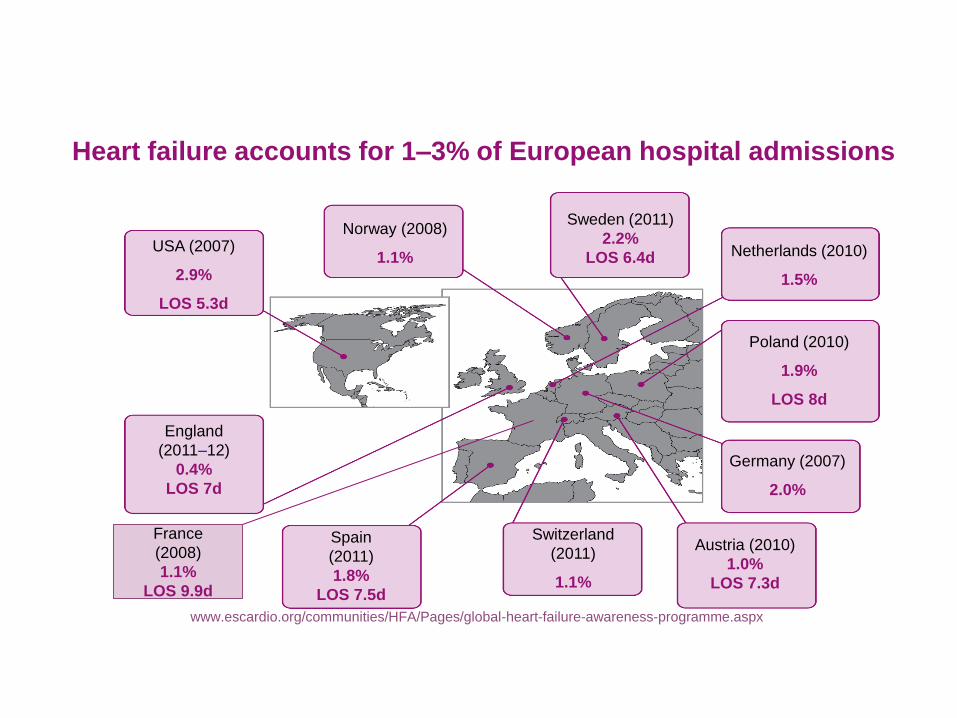
Heart failure accounts for 1–3% of European hospital admissions
USA (2007)
2.9%
LOS 5.3d
Sweden (2011)
2.2%
LOS 6.4d
Norway (2008)
1.1% Netherlands (2010)
1.5%
Poland (2010)
1.9%
LOS 8d
Austria (2010)
1.0%
LOS 7.3d
Germany (2007)
2.0%
Switzerland
(2011)
1.1%
Spain
(2011)
1.8%
LOS 7.5d
England
(2011–12)
0.4%
LOS 7d
France
(2008)
1.1%
LOS 9.9d
www.escardio.org/communities/HFA/Pages/global-heart-failure-awareness-programme.aspx
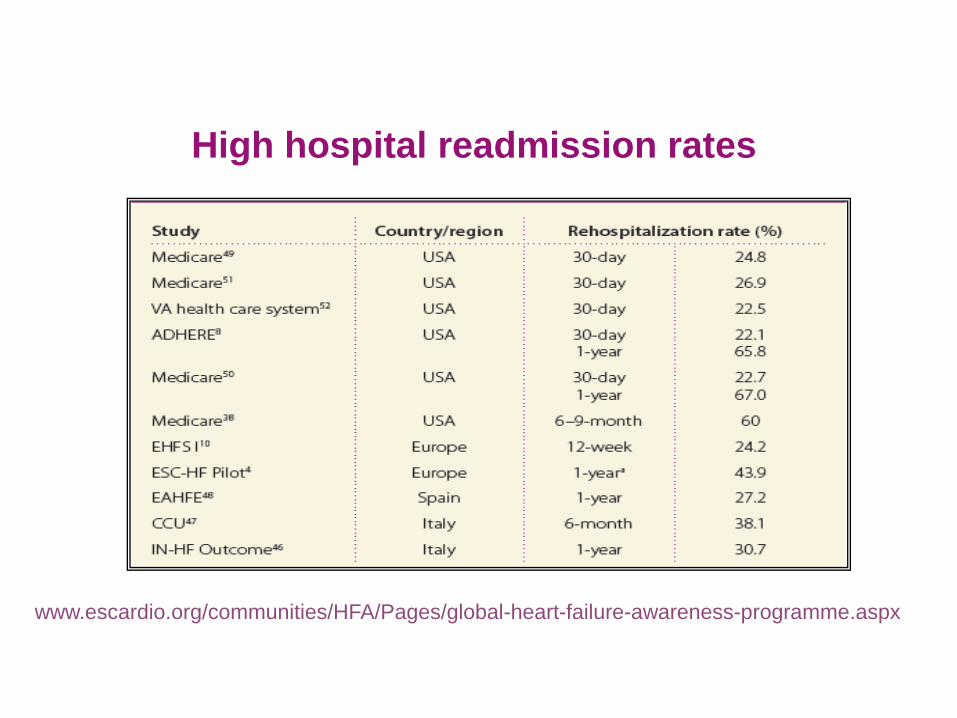
High hospital readmission rates
www.escardio.org/communities/HFA/Pages/global-heart-failure-awareness-programme.aspx
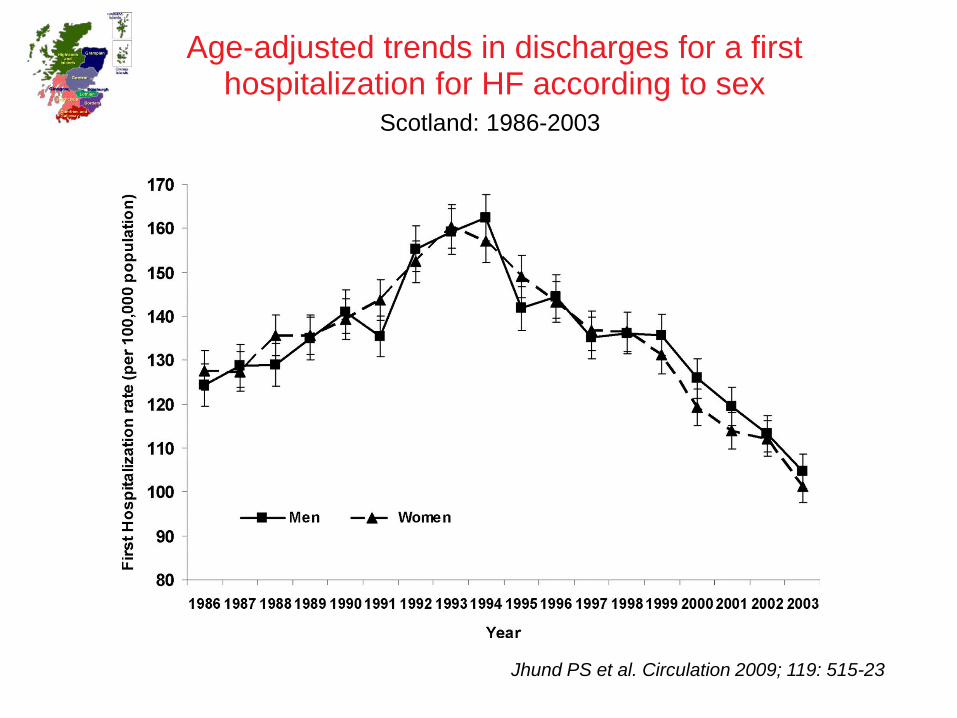
Age-adjusted trends in discharges for a first hospitalization for HF according to sex
Scotland: 1986-2003
Jhund PS et al. Circulation 2009; 119: 515-23
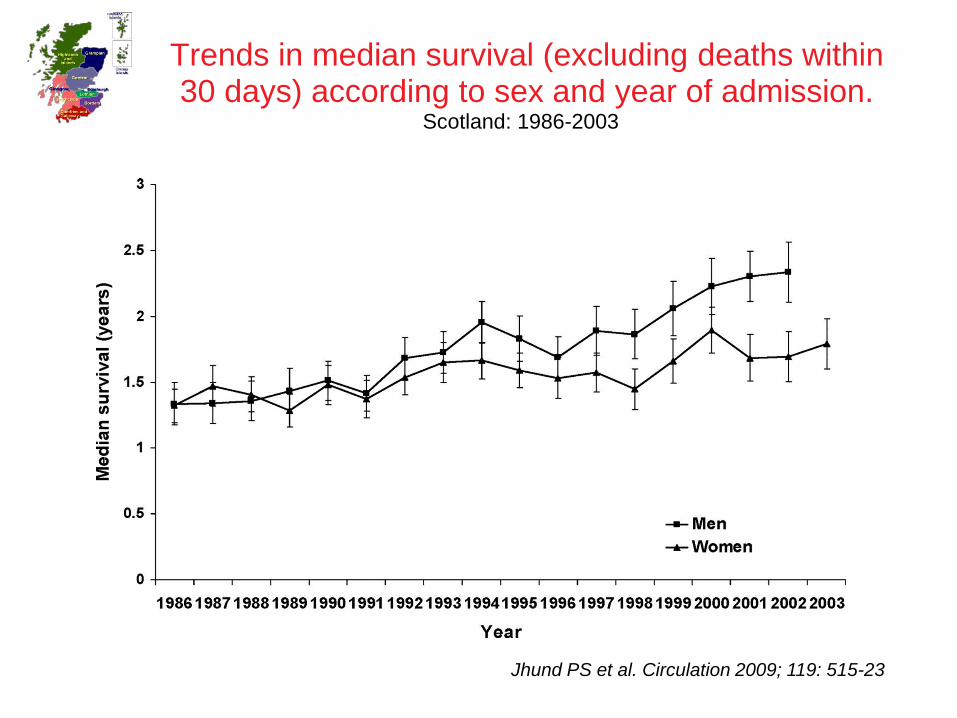
Trends in median survival (excluding deaths within 30 days) according to sex and year of admission.
Scotland: 1986-2003
Jhund PS et al. Circulation 2009; 119: 515-23
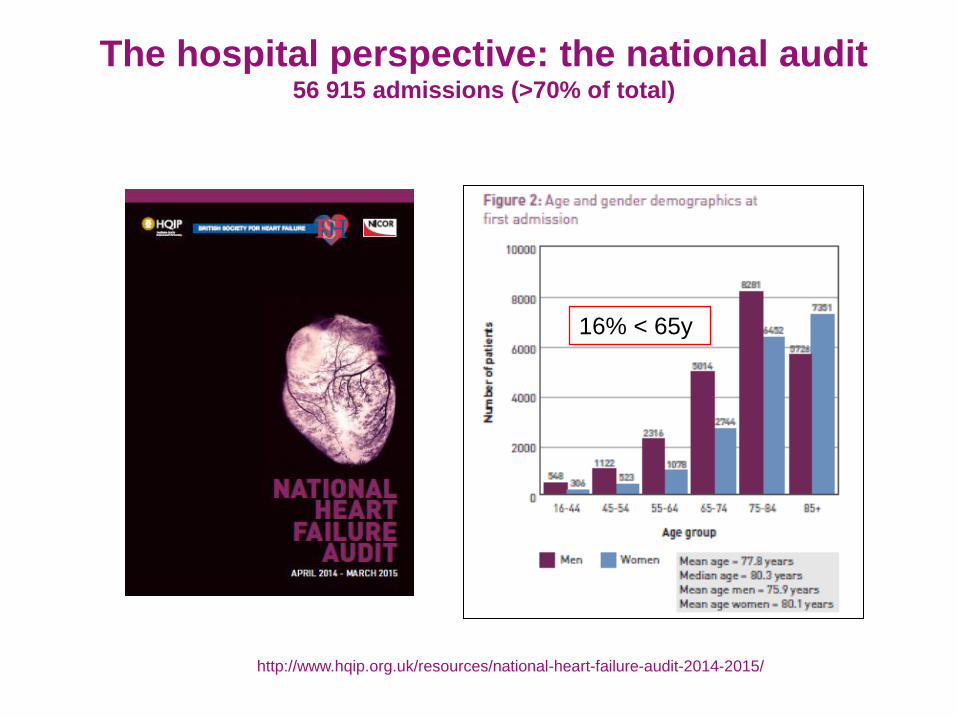
The hospital perspective: the national audit 56 915 admissions (>70% of total)
http://www.hqip.org.uk/resources/national-heart-failure-audit-2014-2015/
16% < 65y
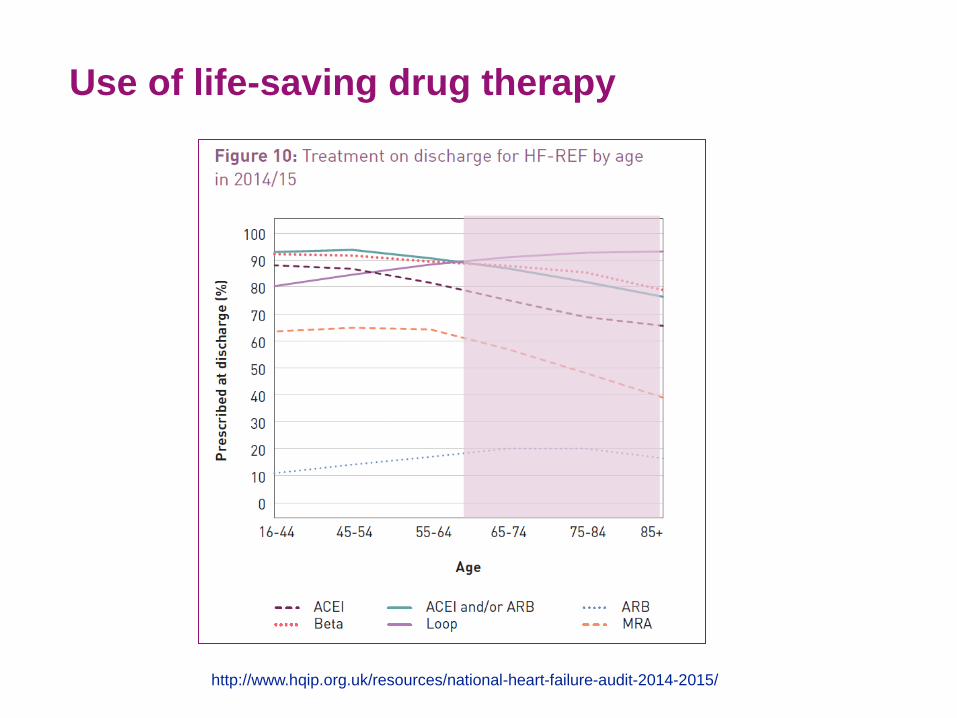
Use of life-saving drug therapy
http://www.hqip.org.uk/resources/national-heart-failure-audit-2014-2015/
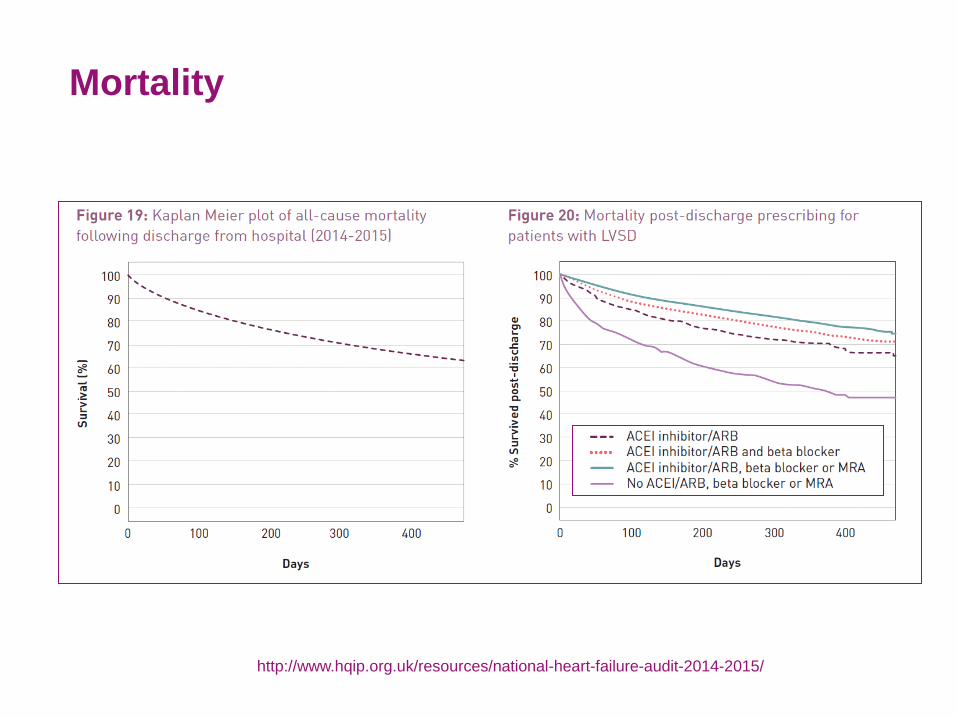
Mortality
http://www.hqip.org.uk/resources/national-heart-failure-audit-2014-2015/
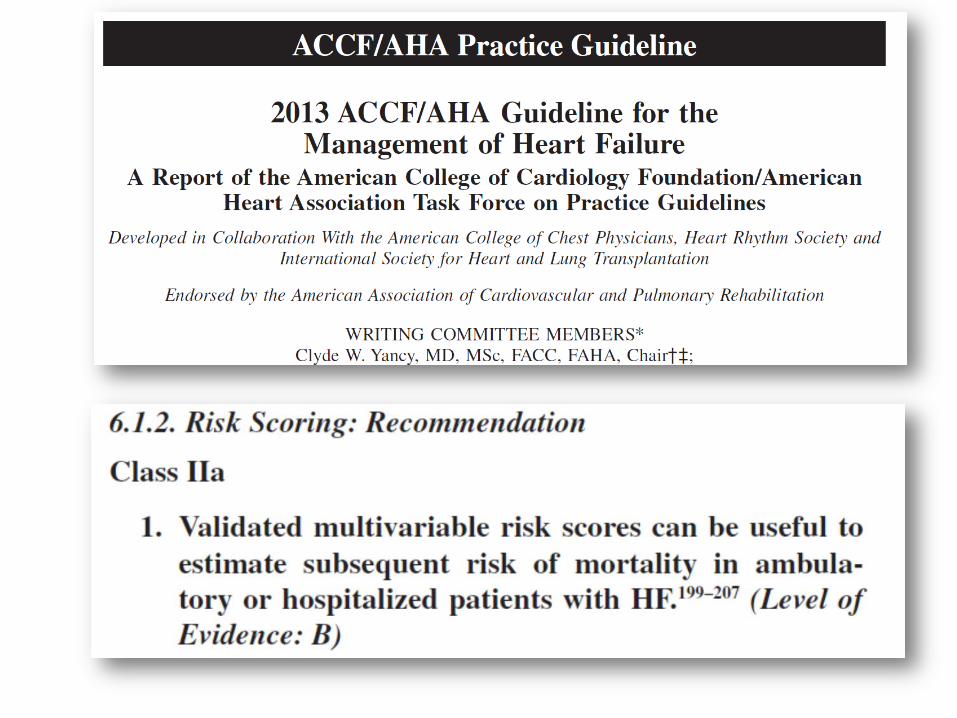
Estimating prognosis
When to refer for tx or MCS?
• Not too soon – patient takes unnecessary risk of operation and is exposed to the long-term complications of transplantation (or MCS) therapy
• Not too late e.g. renal failure, liver failure, respiratory failure – risk of an operation increases markedly
Why risk stratify?
Identify risk more accurately
Identify appropriate
interventions (to reduce risk)
Aid decision re appropriate
place of care
Aid shared decision making
Aid advance planning
WHAT? WHERE? WHEN? WHY?
Something we all do subconsciously
BADLY!
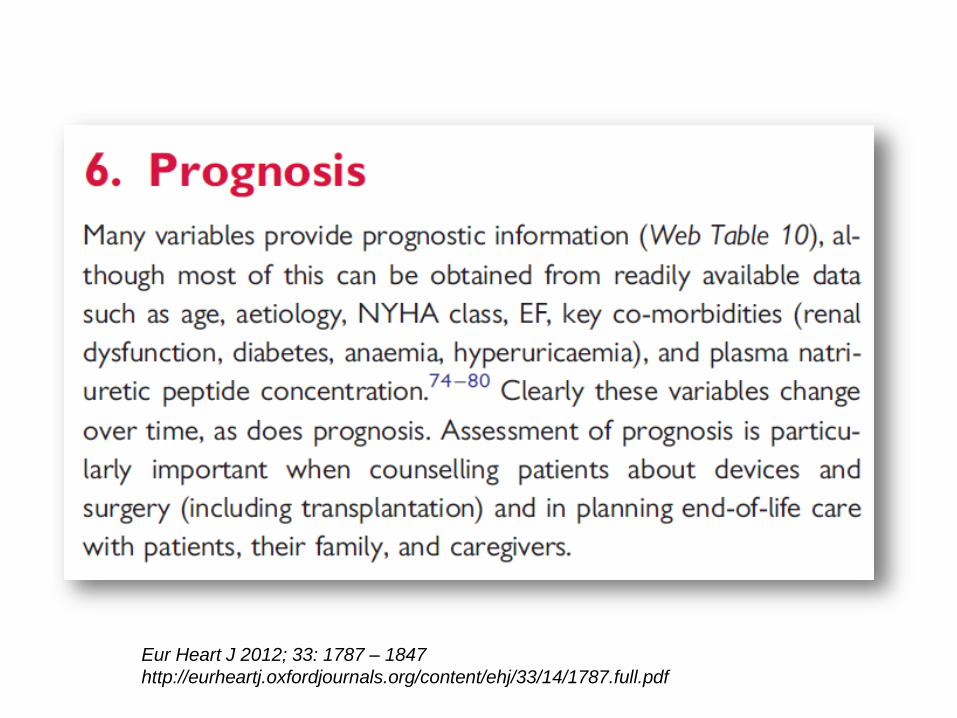
Eur Heart J 2012; 33: 1787 – 1847
http://eurheartj.oxfordjournals.org/content/ehj/33/14/1787.full.pdf
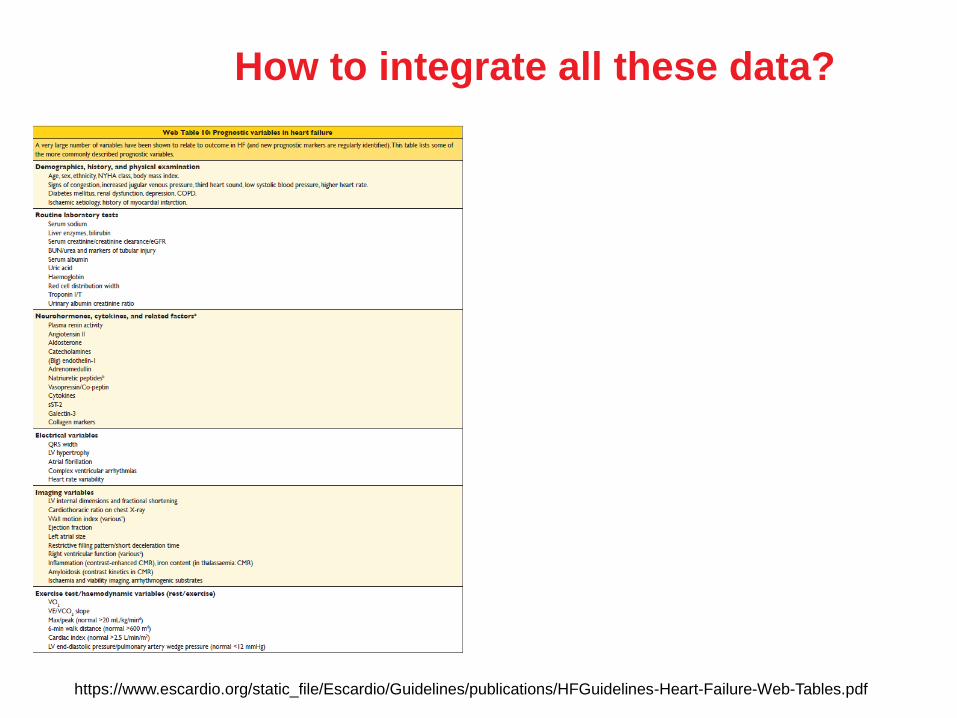
How to integrate all these data?
https://www.escardio.org/static_file/Escardio/Guidelines/publications/HFGuidelines-Heart-Failure-Web-Tables.pdf
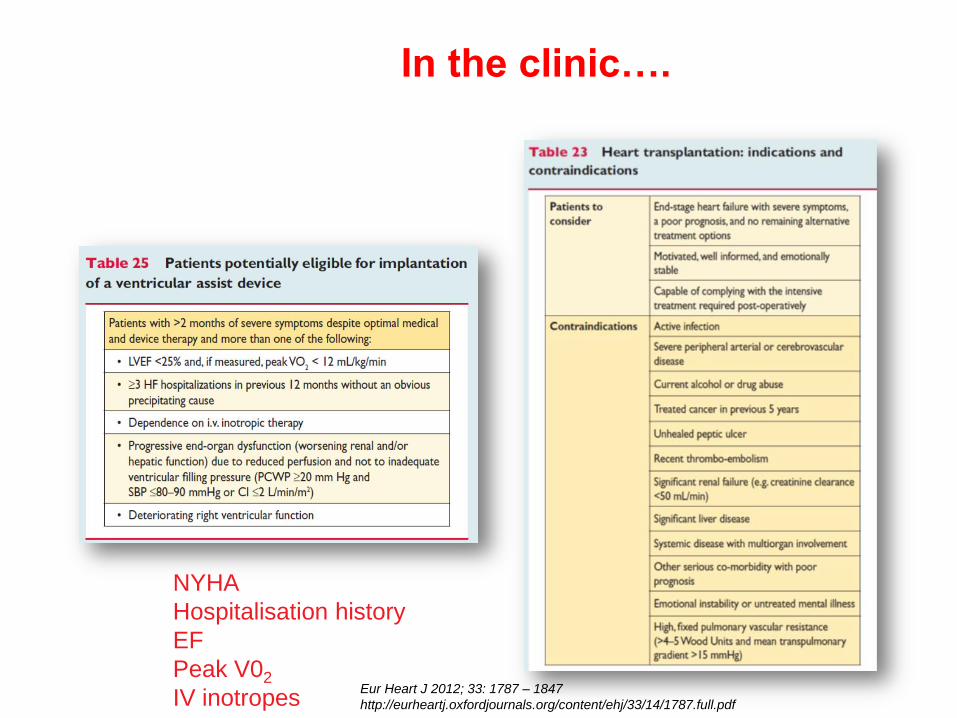
In the clinic….
NYHA
Hospitalisation history
EF
Peak V02
IV inotropes Eur Heart J 2012; 33: 1787 – 1847
http://eurheartj.oxfordjournals.org/content/ehj/33/14/1787.full.pdf
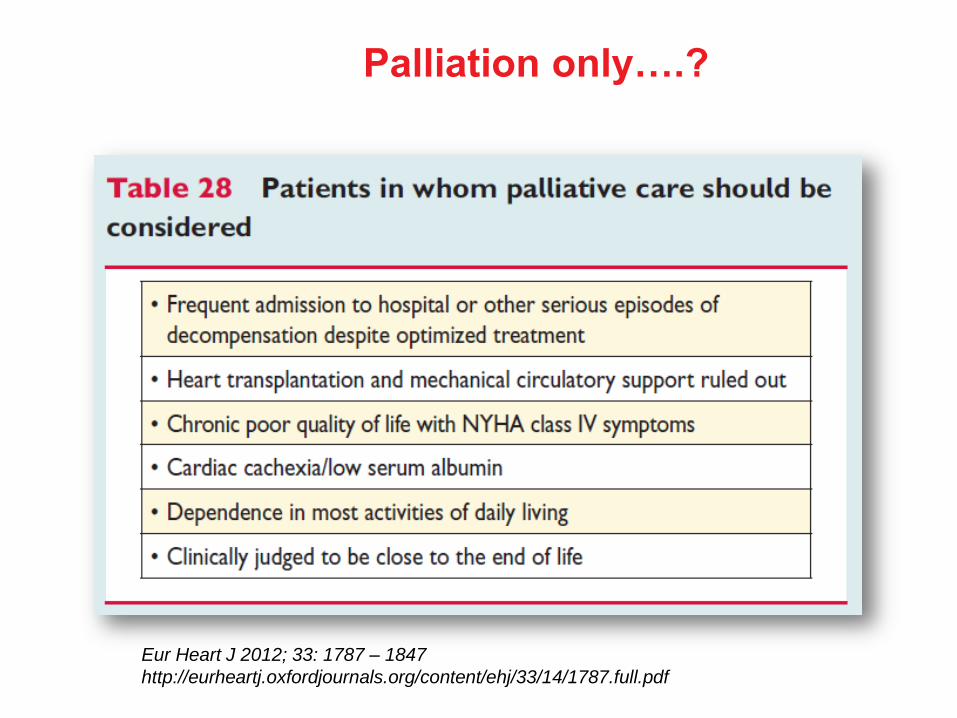
Palliation only….?
Eur Heart J 2012; 33: 1787 – 1847
http://eurheartj.oxfordjournals.org/content/ehj/33/14/1787.full.pdf
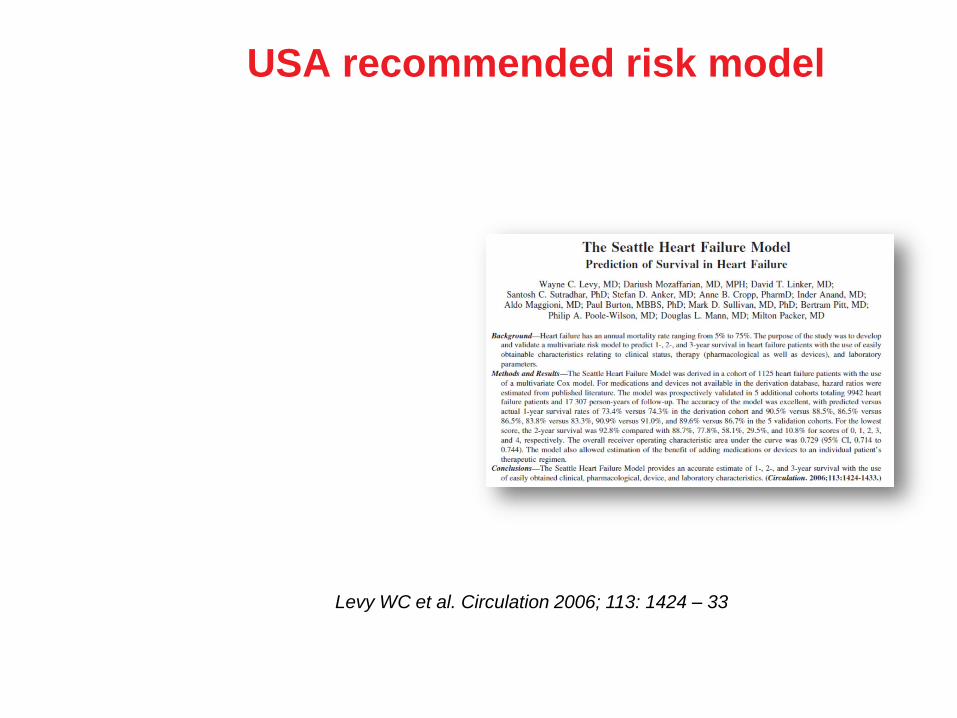
USA recommended risk model
Levy WC et al. Circulation 2006; 113: 1424 – 33
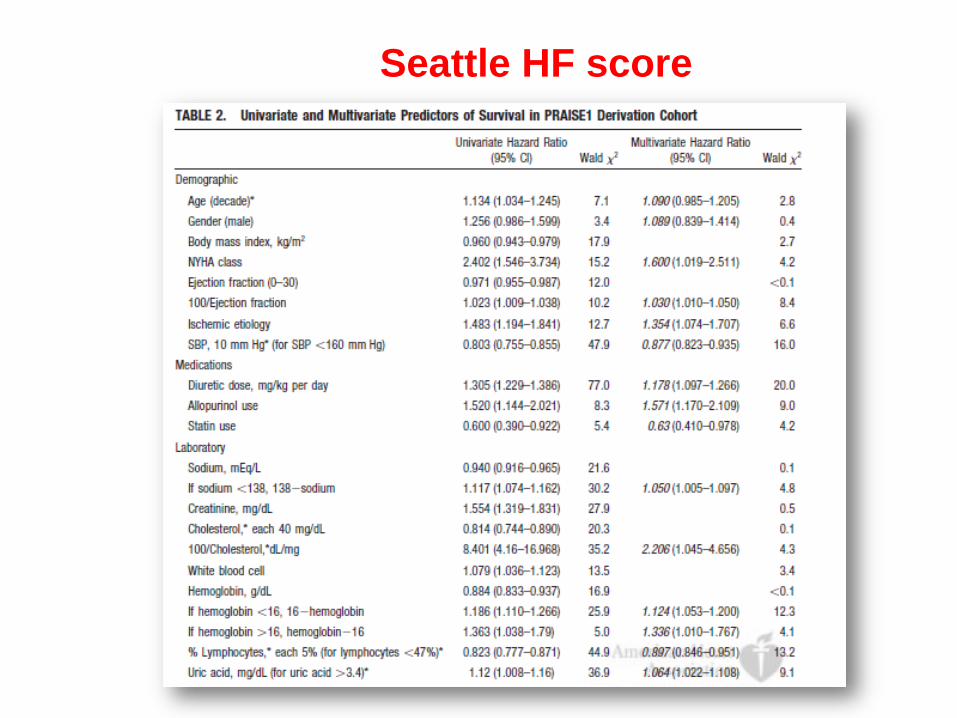
Seattle HF score

Seattle HF Score For ambulatory patients
Also: HF Survival Score; CHARM score; CORONA score; I-PRESERVE score
Available at:
http://SeattleHeartFailureModel.org
Beware!
AUC for ROC curve for mortality prediction in Seattle HF Score = 0.73 (“moderately good”)
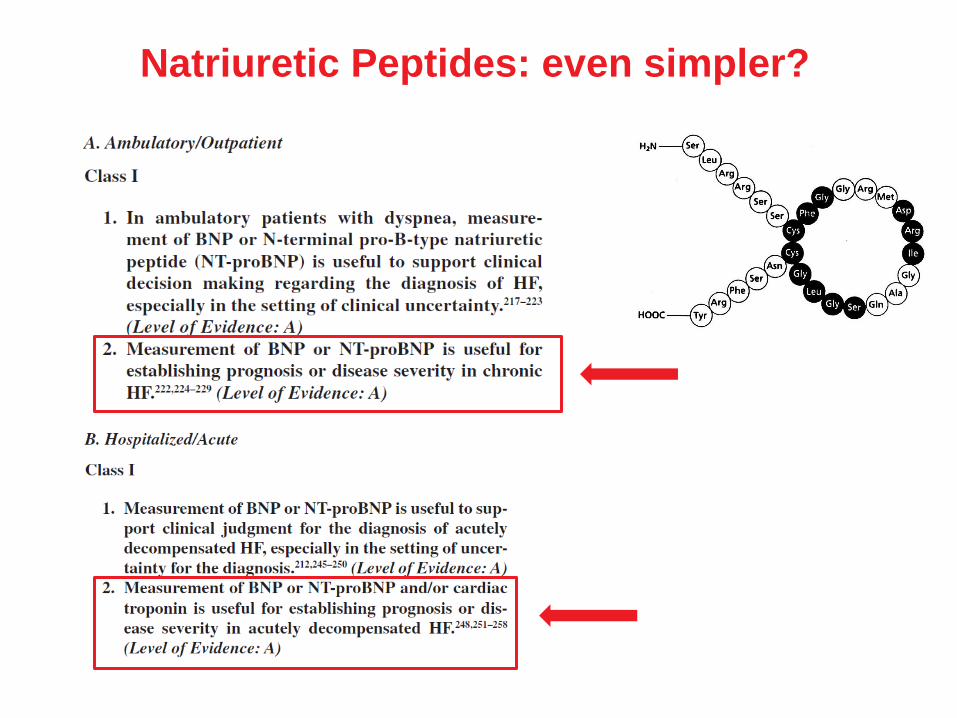
Natriuretic Peptides: even simpler?
Years of thought….
Heart 2003; 89: 587 – 88
Risk stratification relies on communication
Doctors should be more open about
possible courses of action, and
likely results of these actions
No communication = denial of patient
opportunity to make fully informed
choices
Inaccurate estimates of prognosis may
distort a patient’s choice
Predictions do not need to be very
precise: treatment preferences may
change substantially if patient knows
he/she has ≥ 10% chance of dying in 1
year*
Cowie MR. Heart 2003; 89: 587 – 8. *Weeks JC et al. JAMA 1998; 279: 1709 – 14
What would you do differently if you knew you had a 20% chance of being
dead in January 2018?