Mariano Provencio Servicio de Oncología Médica Hospital ... · QUIMIOTERAPIA ADYUVANTE ALPI CDDP...
43
LA QUIMIOTERAPIA COMO VERTEBRADORA DEL TRATAMIENTO DEL CÁNCER DE PULMÓN NO MICROCÍTICO Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro
Transcript of Mariano Provencio Servicio de Oncología Médica Hospital ... · QUIMIOTERAPIA ADYUVANTE ALPI CDDP...

LA QUIMIOTERAPIA COMO VERTEBRADORA DEL TRATAMIENTO DEL CÁNCER DE PULMÓN NO MICROCÍTICO
Mariano Provencio
Servicio de Oncología Médica
Hospital Universitario Puerta de Hierro

Agenda
• En adyuvancia
• En estadios intermedios
• En estadios avanzados
• En segundas líneas

QUIMIOTERAPIA ADYUVANTE
ALPI CDDP + MMC + VDS x 3 n=1209
BLT CDDP + VP16 o alc. vinca x 3-4 n=381
KATO UFT vs observación n=999
IALT CDDP + VP16 o alc. vinca x 3-4 n=1867
CALGB CBDCA + PCT n=344
NCI-C CDDP + VINORELBINA n=482
ANITA CISPLATINO + VINORELBINA n= 840
Ensayos Aleatorios Posteriores a 1995 con > 300 pacientes

ESTUDIO ALPI
Scagliotti, JNCI 2003
• Combinación en estudio: MVP, estándar cuando se diseñó. • Estadios: I - IIIA- 1209 pacientes
• Resultados: el TTP y la SG fueron favorables en la rama
de tratamiento, sin significación estadística.
• Sólo el 39% de los pacientes recibió los 3 ciclos previstos.
• Conclusión de los autores: « dado el bajo cumplimiento del régimen MVP utilizado en este estudio, estudios futuros deberán explorar tratamientos más efectivos »

ESTUDIO: Big Lung Trial
Waller, Eur J Cardiothorac, 2004
• Analiza el papel de la QT en adyuvancia o neoadyuvancia en pacientes tratados con cirugía, RT. Se aleatoriza tratamiento o control. (n=381 en la rama de adyuvancia)
• Combinaciónes en estudio: MIC, MVbC, VC, VdC
• No se observan diferencias en la supervivencia entre los
grupos de tratamiento entre los pacientes que reciben la adyuvancia tras cirugía.
• Estudio de bajo poder • 29 meses seguimiento…

The IALT; NEJM 04
ESTUDIO IALT
• Diferentes esquemas a elegir, por no haber consenso en:
• La dosis de cisplatino • El doblete de referencia basado en cisplatino • Los estadios elegibles para la quimioterapia adyuvante • La radioterapia postoperativa
• CISPLATINO: 80 mg/m2 cada 3 sem. x 4 ciclos o 100 mg/m2 cada 4 sem. x 3 ó 4 c. o 120 mg/m2 cada 4 sem. x 3 ciclos
+ • NAVELBINE: 30 mg/m2 semanal • ETOPÓSIDO: 100 mg/m2 x 3 días por ciclo • VINBLASTINA: 4 mg/m2 semanal
• VINDESINA: 3 mg/m2 semanal
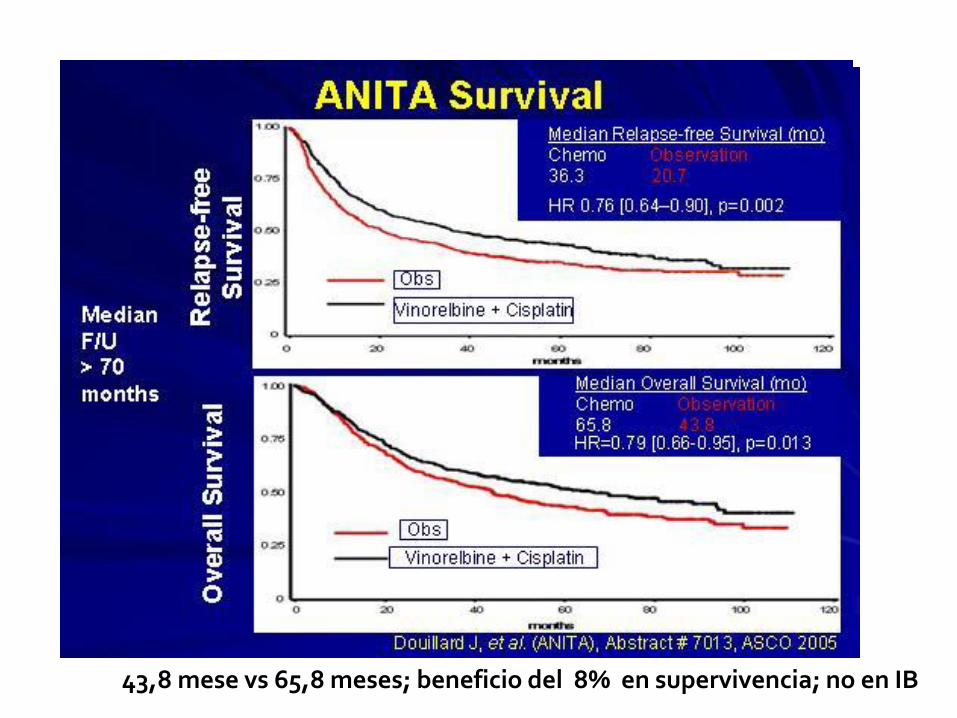
43,8 mese vs 65,8 meses; beneficio del 8% en supervivencia; no en IB

Visión crítica estudios adyuvancia
SOBRE EL ENSAYO SOBRE LA CIRUGÍA
– IALT: se paró el reclutamiento con 60% • 65% seguimiento del previsto
– Cumplimiento: • IALT: 31% reciben menos de 3
ciclos, 9% nada
• ALPI: 26%, 8% ninguno
– Radioterapia: • ALPI: 43%
• IALT: 27%
• NCIC-BR10: 0%
• ANITA: 28%
– Tipo de cirugía: neumonectomía
• IALT: 35%
• BR10: 25%
– Disección ganglionar completa o muestreo:
• Desconocida en todos, salvo ALPI: 57% vs 43%

JCO 2008; 26: 3552-3559.
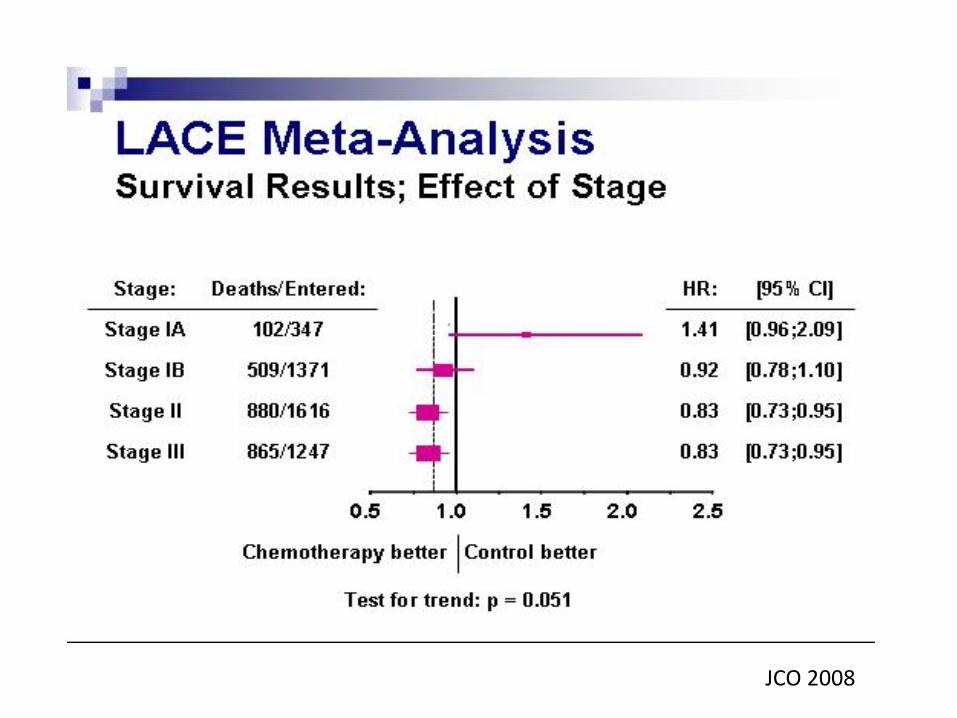
JCO 2008

Author Year Type Data Nº trials N HR
Hotta 2004 Published data 11* 5716 0.87
Sedrakyan 2004 Published data 19 7200 0.87
Berghmans 2005 Published data 17 7644 0.85
Bria 2005 Published data 11 + 1 MA 6494 0.93
Hamada 2005 Individual patient data 6** 2003 0.74
Pignon (LACE) 2006 Individual patient
data
5 4584 0.89
NSCLC MA 2010 Individual patient
data
34 8447 0.86
4% at 5y
*Recent trials only ; **UFT trials only
Meta-analysis in ADJ setting
Hotta – JCO 2004 * Sedraykan – J Thorax Cardiov S 2004 * Berghmans – Lung Cancer 2005 Bria – JCO 2005 * Hamada – JCO 2005 * Pignon – JCO 2008 * NSCLC MA – Lancet 2010

IMPACTO DE LA QUIMIOTERAPIA ADYUVANTE EN CÁNCER DE MAMA Y PULMÓN

Evaluación cuantitativa de los resultados de un ensayo clínico
Riesgo Relativo 0,43 (IC 95%; 0,36-
0,68)
Reducción
Relativa Riesgo 53% (IC 95%,38-44)
R Absoluta del
Riesgo 40% (IC 95%, 28,6-
50)
Número
Necesario a tratar 3 (IC 95%, 2-4)
ANITA N1 S GLOBAL
Riesgo Relativo 0,89 (IC 95%, 0,81-
0,98)
Reducción
Relativa Riesgo 11% (IC 95%,1.6%-
14,2%)
R Absoluta del
Riesgo 7,9% (IC 95%, 1,6%-
14,2%)
Número NT 13 (IC 95%, 6-62)
ANITA QT vs Observación Sv. Global
Riesgo Relativo 0,81 (IC 95%, 0,70-
0,94)
Reducción
Relativa Riesgo 19% (IC 95%,6-30)
R Absoluta del
Riesgo 5,9% (IC 95%, 1,5-
8,5)
Número
Necesario a tratar 21 (IC 95%, 12-68)
NEJM- MOSAIC-SLE
Riesgo Relativo 0,87 (IC 95%, 0,81-
0,95)
Reducción
Relativa Riesgo 13% (IC 95%,0-19)
R Absoluta del
Riesgo 10% (IC 95%; 4-16)
Número NT 10 (IC 95%,7-25)
ANITA QT vs Observación SLE (60m)
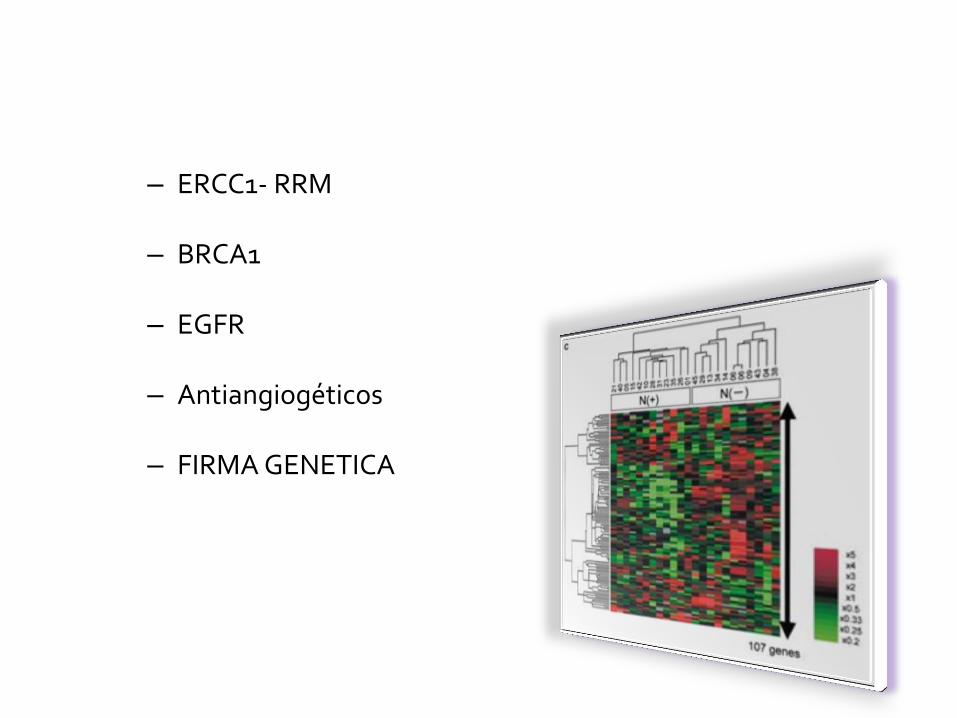
– ERCC1- RRM
– BRCA1
– EGFR
– Antiangiogéticos
– FIRMA GENETICA

Quimioterapia adyuvante: expresión de ERCC1. Olaussen K et al. NEJM 2006
14-month benefit in overall survival 6.2-month benefit in overall survival for chemotherapy vs control (n= 1867) (IALT
Group. NEJM 2004)
Chemotherapy
n=389
5-year survival rate,
Median survival
Control group
n=372
5-year survival rate,
Median survival
Hazard ratio for death
CT vs. no CT
ERCC1 negative tumors
n=426
47% [40%-55%]
56 months
39% [32%-47%]
42 months
0.65 [0.50-0.86]
p = 0.002
ERCC1 positive tumors
n=335
40% [32%-49%]
50 months
46% [37%-55%]
55 months
1.14 [0.84-1.55]
p = 0.40

Chen HY. N Engl J Med 2007; 356: 11-20
DUSP6 MMD STAT1 ERBB3 LCK
FIRMA GENETICA DE LA “FAMILIA CHEN”
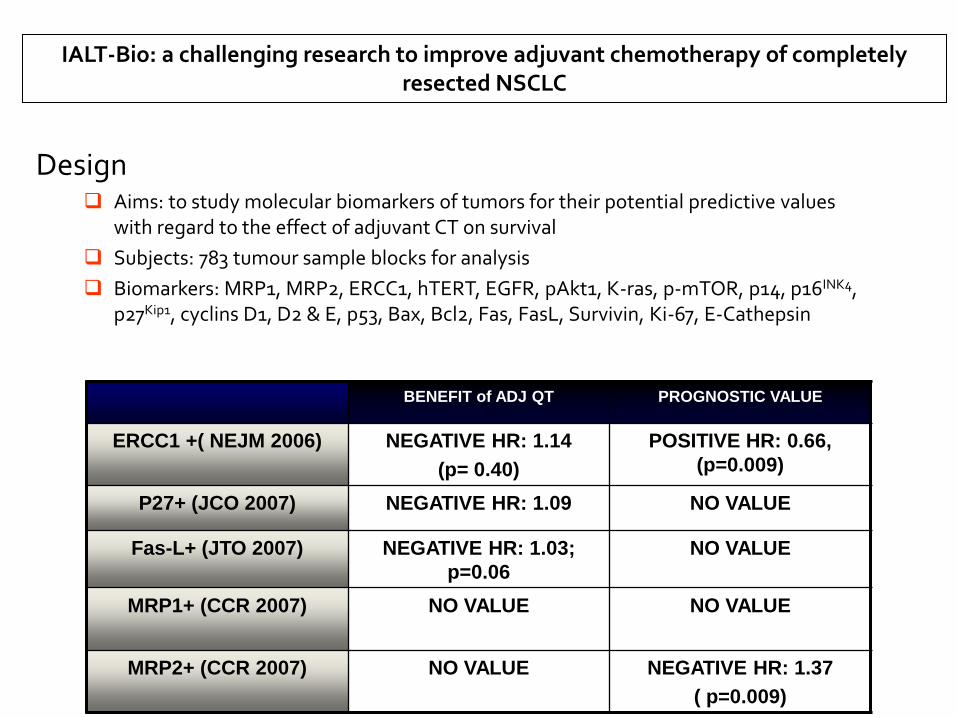
Design Aims: to study molecular biomarkers of tumors for their potential predictive values
with regard to the effect of adjuvant CT on survival
Subjects: 783 tumour sample blocks for analysis
Biomarkers: MRP1, MRP2, ERCC1, hTERT, EGFR, pAkt1, K-ras, p-mTOR, p14, p16INK4, p27Kip1, cyclins D1, D2 & E, p53, Bax, Bcl2, Fas, FasL, Survivin, Ki-67, E-Cathepsin
IALT-Bio: a challenging research to improve adjuvant chemotherapy of completely resected NSCLC
BENEFIT of ADJ QT PROGNOSTIC VALUE
ERCC1 +( NEJM 2006) NEGATIVE HR: 1.14
(p= 0.40)
POSITIVE HR: 0.66,
(p=0.009)
P27+ (JCO 2007) NEGATIVE HR: 1.09 NO VALUE
Fas-L+ (JTO 2007) NEGATIVE HR: 1.03;
p=0.06
NO VALUE
MRP1+ (CCR 2007) NO VALUE NO VALUE
MRP2+ (CCR 2007) NO VALUE NEGATIVE HR: 1.37
( p=0.009)
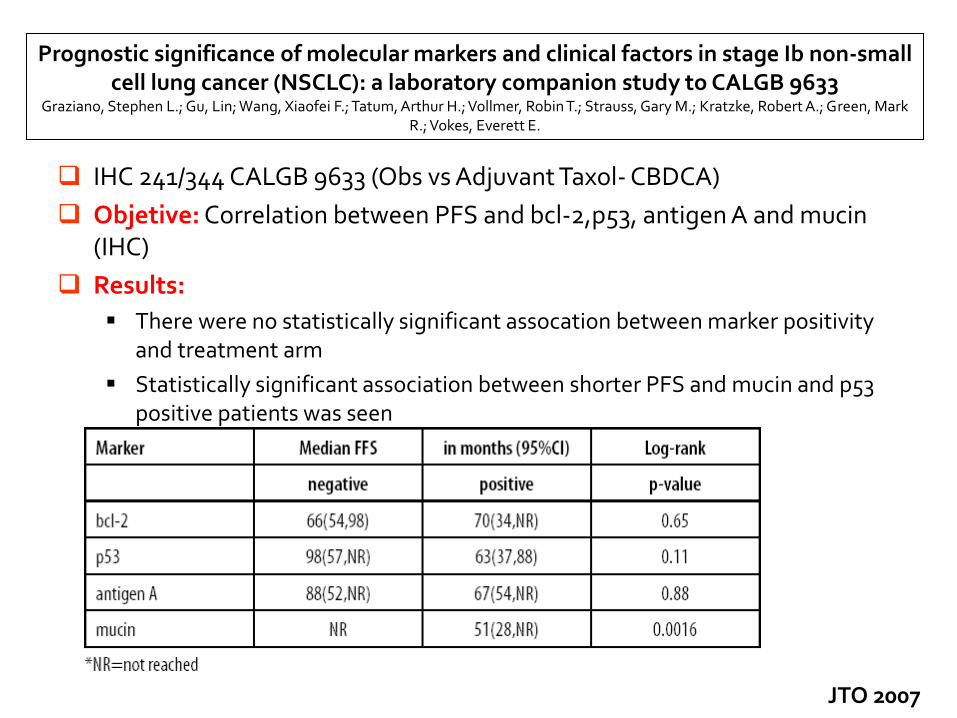
Prognostic significance of molecular markers and clinical factors in stage Ib non-small cell lung cancer (NSCLC): a laboratory companion study to CALGB 9633
Graziano, Stephen L.; Gu, Lin; Wang, Xiaofei F.; Tatum, Arthur H.; Vollmer, Robin T.; Strauss, Gary M.; Kratzke, Robert A.; Green, Mark R.; Vokes, Everett E.
IHC 241/344 CALGB 9633 (Obs vs Adjuvant Taxol- CBDCA)
Objetive: Correlation between PFS and bcl-2,p53, antigen A and mucin (IHC)
Results:
There were no statistically significant assocation between marker positivity and treatment arm
Statistically significant association between shorter PFS and mucin and p53 positive patients was seen
JTO 2007

Molecular biomarkers in JBR10
BENEFIT of ADJ QT Prognostic value
P53 IHC+ Positive HR: 0.54
(p=0.02)
Negative HR: 1.89
p=0.03
High Class III Beta
tubulin
Positive HR: 0.45
(p=0.0002)
Negative HR:1.92
(p=0.01)
kRas mutations No value No value
p53 mutations No value No value
Tsao et al. JCO 2007
Séve et al. CCR 2007

MAGRIT, a double-blind, randomized, placebo-controlled phase III study to assess the efficacy of the recMAGE-A3 + AS15 cancer immunotherapeutic as adjuvant therapy in patients with resected MAGE-A3-positive non-small cell lung cancer (NSCLC)
• Study objective
– To determine if recMAGE-A3 + AS15 cancer immunotherapeutic (MAGE-A3 CI) as adjuvant therapy over 27
months improves DFS in patients with resected NSCLC
Primary endpoint
• DFS
R 2:1
PD
PD Key patient inclusion criteria
• Stages IB, II, IIIA NSCLC
• Completely resected
tumour
• MAGE-A3-positive
• PS 0–2
(n=2,272) 13 IM injections of placebo
(n=757)
13 IM injections of MAGE-A3 CI
(n=1,515)
Stratification
• Chemotherapy
Secondary endpoints
• OS, lung cancer specific survival,
immunogenicity
• Safety, health-related QoL
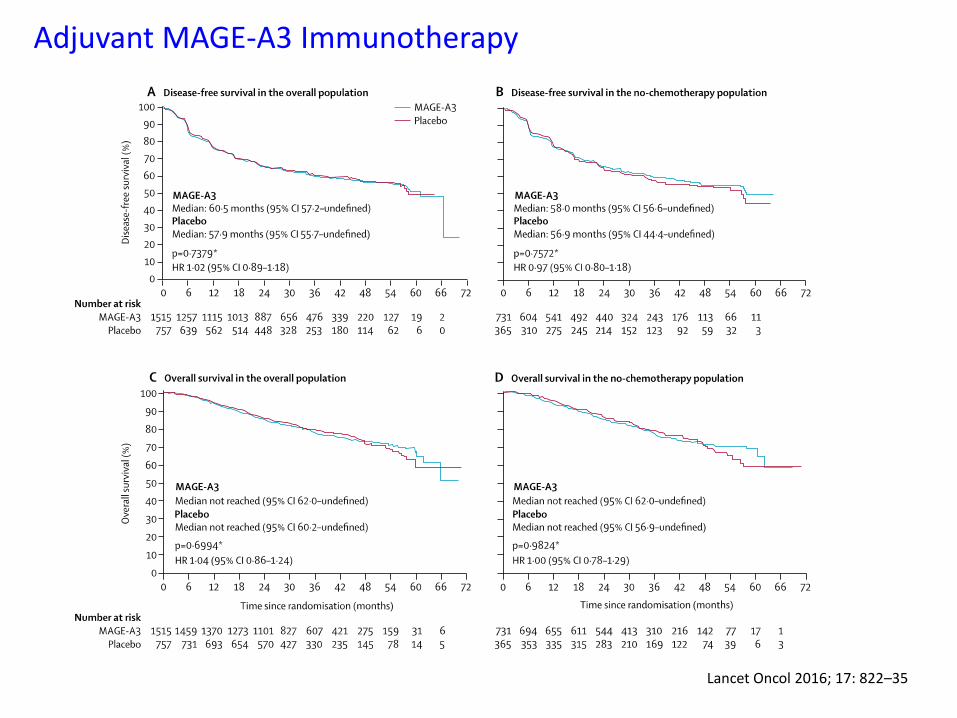
Adjuvant MAGE-A3 Immunotherapy
Lancet Oncol 2016; 17: 822–35

Postop Erlotinib: RADIANT Trial
http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2015.61.8918

RADIANT: Outcomes
http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2015.61.8918

Gefitinib: adjuvant trial in EGFR mut+: CTONG1104
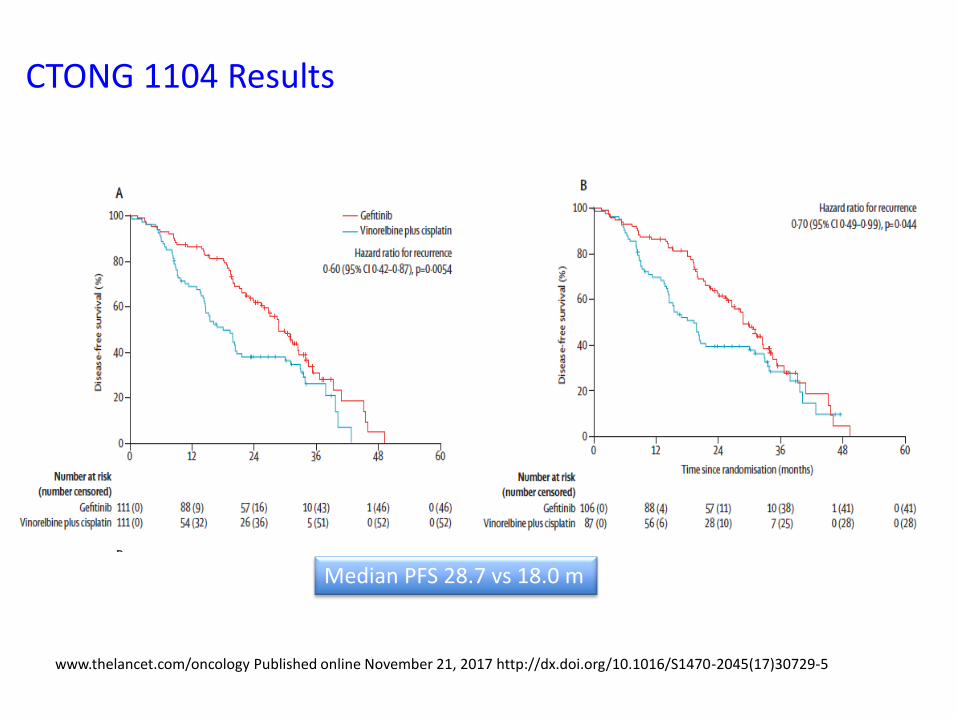
CTONG 1104 Results
www.thelancet.com/oncology Published online November 21, 2017 http://dx.doi.org/10.1016/S1470-2045(17)30729-5
Median PFS 28.7 vs 18.0 m

Adding Bevacizumab to postoperative chemotherapy: E1505 Trial
Study objective
• To evaluate the addition of bevacizumab to adjuvant chemotherapy in early stage resected NSCLC
Key patient inclusion
criteria
• Resected
• Stage IB (≥4 cm)–IIIA
• 6–12 weeks post-op
• No prior
chemotherapy
• ECOG PS 0–1
(n=1,501)
R
1:1
Arm A: Chemotherapy* x 4 cycles
(n=749)
Arm B: Chemotherapy* x 4 cycles +
bevacizumab 15 mg/kg q3w x 1 yr
(n=752)
Stratification
• Cisplatin doublet, stage, histology, gender
*Chemotherapy regimens q3w
Cisplatin 75 mg/m2 D1 combined with any of the following:
♦ vinorelbine 30 mg/m2 D1, 8
♦ docetaxel 75 mg/m2 D1
♦ gemcitabine 1200 mg/m2 D1, 8
♦ pemetrexed 500 mg/m2 D1
Primary endpoint: OS
Secondary endpoints: DFS, safety

E 1505 Results
www.thelancet.com/oncology Published online November 7, 2017 http://dx.doi.org/10.1016/S1470-2045(17)30691-5 1

Customized BRCA1 Adjuvant Treatment in Stage II-II NSCLC (SCAT)
T2 BRCA1
T3 BRCA1
Gem/Cis
Docetaxel
Docetaxel/Cis
T 1 BRCA1
Planned number of patients: 432 (amended)
CT should be started within 8 weeks after surgery
PORT in N2 patients
CONTROL
EXPERIMENTAL
Docetaxel/Cis
Statification factors:
- Stage: N1 vs. N2 - Age <65 vs > 65 y - Histology: Non-SCC vs. SCC - Type of resection: Lobectomy vs Pneumonectomy
Eudract: 2007-000067-15 NCTgov: 00478699
1
:
3

Low BRCA1 levels High BRCA1 levels
Median Survival: Cis-Gem: 74 m (59-89) Cis-Doc: 40.1 m (25-78)
HR: 0.622 (p = 0.005)
Median Survival: Doc: 80.2 m (68-145) Cis-Doc: NA
HR: 1.289 (p = 0.436)
Overall Survival: treatment effect in BRCA subgroups
ESMO Guidelines
Adjuvant ChT should be offered to patients with resected stage II and III NSCLC [I, A] and can be considered in patients with resected stage IB disease and a primary tumour >4 cm [II, B].
Pre-existing comorbidity, time from surgery and postoperative recovery need to be taken into account in this decision taken in a multidisciplinary tumour board [V, A].
For adjuvant ChT, a two-drug combination with cisplatin is preferable [I, A]. In randomised studies, the attempted cumulative cisplatin dose was up to 300 mg/m2, delivered in three to four cycles.
The most frequently studied regimen is cisplatin–vinorelbine.
At the present time, the choice of adjuvant therapy should not be guided by molecular analyses, e.g. ERCC1 mutation testing [IV, B].
In the current state of knowledge, targeted agents should not be used in the adjuvant setting [II, A].
In view of the equivalence of neoadjuvant and adjuvant ChT for OS, the consistent results and broad evidence base support adjuvant ChT as the timing of choice [II, C].
Annals of Oncology 28 (Supplement 4): iv1–iv21, 2017 doi:10.1093/annonc/mdx222

“We need: - ambitious pioneers - couple optimism and
audacity
- access to new technology or other innovations and - launch themselves into a daring, dizzying adventure”

Incorporating TKi in the treatment of early stages
Goss G. J Clin Oncol 2013
From 2002-2005
503 p, planned 1242
gefitinib 2 y

Incorporating Bevacizumab and Erlotib in the combined-modality
treatment of stage III NSCLC: Results of a phase I/II trial
Trial LCCC 9603
LCCC 2001
LCCC 0215
CALGB 30105
RTOG 0324
CALGB 30407
Socinski 2012
Nº p 62 29 23 43 87 101 45
Induction QT
CbP CbP CbPI CbP - - CbP Beva
Concurrent CbP CbP CbP+ gefitinib
CbP CbP + Cetuxi
CbPem +/- Cetuxi
CbP Beva + Erlotinib
TCRT, Gy 60-74 78-90 74 74 63 70 74
PFS rate 1 year, %
47 45 40 55 50 50 44
Median S, m 26 24 16 24,3 22,7 21-25 18,4
Esophagitis,G 3 /4 %
8 16 19,5 16 8 13-16 29
J Clin Oncol Nov 2012 J Clin Oncol Nov 2008

“The use of bevacizumab and erlotinib is not
recommened in the setting of combined-modality
therapy in stage III NSCLC.
This recomendation is based on the lack of
efficacy
and the risk of high toxicity, particulary
esophageal”.


Evaluated the addition of gefitinib to
sequential or concurrent Ch-RT in
unresectable stage III NSCLC
63 p
Poor risk 1: RT (66Gy) + Gefitinb 250
mg
PFS: 13.4 m, median OS: 19 m
Good risk 2: RT + Gefitinib + CbP
PFS: 9.2 m; median OS: 13 m
“Sequential CRT with Gefitinib with wild type or mutated EGFR was promising
Concurrent CRT plus gefitinib was disappointing even for tumor with activating
EGFR mutations” J Thorac Oncol 2010; 5 (9): 1382-90

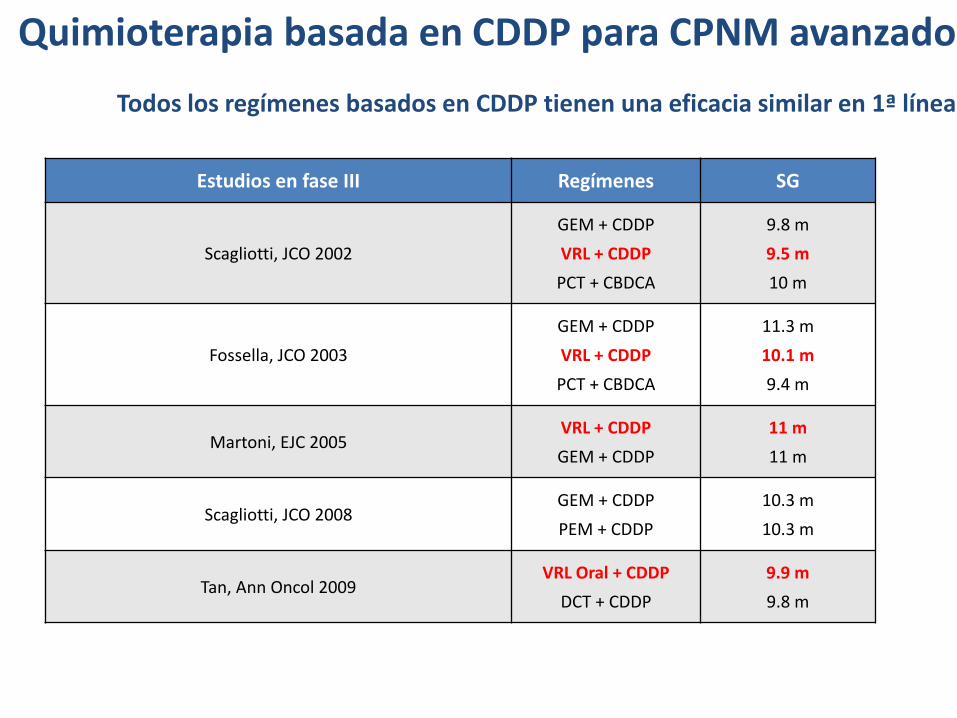
Quimioterapia basada en CDDP para CPNM avanzado
Todos los regímenes basados en CDDP tienen una eficacia similar en 1ª línea
Estudios en fase III Regímenes SG
Scagliotti, JCO 2002
GEM + CDDP
VRL + CDDP
PCT + CBDCA
9.8 m
9.5 m
10 m
Fossella, JCO 2003
GEM + CDDP
VRL + CDDP
PCT + CBDCA
11.3 m
10.1 m
9.4 m
Martoni, EJC 2005 VRL + CDDP
GEM + CDDP
11 m
11 m
Scagliotti, JCO 2008 GEM + CDDP
PEM + CDDP
10.3 m
10.3 m
Tan, Ann Oncol 2009 VRL Oral + CDDP
DCT + CDDP
9.9 m
9.8 m

Reck M et al, NEJM 2016

Brahmer J et al, ,WCLC 2017

Borghaei H J et al, WCLC 2017

Borghaei H J et al, WCLC 2017

Carefull … right target…
BIOLOGICAL BASES BIOMARKER
IDENTIFICATION
RIGHT DRUG RIGHT PATIENT