MAR 2009/2014 Report
44
1 MOTHERS AT RISK Safe Mothers, Healthy Babies, Literate Girls 2009-2014
-
Upload
alexandra-birladianu -
Category
Government & Nonprofit
-
view
299 -
download
0
Transcript of MAR 2009/2014 Report

1
MOTHERS AT RISKSafe Mothers, Healthy Babies, Literate Girls
2009-2014

2
Mothers At Risk 2009-2014 Report
The Mothers At Risk 2009-2014 Report
is distributed to members, beneficiaries
and partners of Mothers At Risk. It is
edited at the Mothers At Risk office in
Brussels, Belgium
Mothers at Risk, a.s.b.l.
23 Rue Darwin
1050 Brussels, Belgium
http://www.mothersatrisk.org
Copyright © 2014 by Mothers At Risk
Design: Alexandra Birladianu
Ajay Singh - www.chilifactor.com
All rights reserved.
No part of this publication may be
reproduced, stored in a retrieval system,
or transmitted, in any form, or by any
means, electronic, mechanical,
photocopying, recording, or otherwise,
without the prior consent of the
publisher.

3
TABLE OF CONTENTS
Message From Prof. Dr. Alain Vokaer 4
Message From Diana Perez-Buck 5
Overview 2009-2014 6
The Issues 7
Invest in Maternal and New Born Health 8
Invest in Girls Education 9
Milestones 2009-2014 10 Our Work: - Kenya 12 - Egypt 14 - Haiti 16 - Nicaragua 18 - Morocco 20 - Tanzania 22 - Belgium 24 - Peru 26
Financial Snapshots 28
Our Partners 29 Our Team - Mothers At Risk Board 30 - Executive Team 31 - Management Committee, MAR Fund, King Baudouin Foundation 32 - MAR Advisors 33
MAR Fundraising Recitals 34
Events 36
MAR In The News 37
Volunteers 38
Working Together 40

4
MESSAGE FROM PROF. DR. ALAIN VOKAERPRESIDENT, MANAGEMENT COMMITTEE, MOTHERS AT RISK FUND, KING BAUDOUIN FOUNDATION
In my more than 40 years practicing as an obstetrician together with my wife, a certified midwife, we have had the fortune of assisting thousands of women to safely deliver healthy babies. Over the course of these decades we have also witnessed the serious complications that can and do arise, and we know all too well that adequate prenatal prevention and timely skilled interventions at the moment of birth can make the difference between life and death. Today, inexcusably, almost 300,000 women continue to die every year from pregnancy and childbirth-related complications - most of them in developing countries. And motherless children are ten times more likely to die within two years of their mother’s death. What is more, for every maternal death, approximately 20 more women suffer severe illness or injury.
The vast majority of these tragic deaths and disabilities could be prevented if women had better access to family planning and to quality care during pregnancy and childbirth. More generally, if girls and women have more access to education, their health and that of their children improves dramatically. It is these challenges that inspired the creation of Mothers at Risk (MAR) by a small but very dynamic group of volunteers, whose evolution I have had the pleasure of following and contributing to over the years. MAR has consistently grown to encompass more projects, reach more beneficiaries, establish new partnerships and become increasingly professionalized while retaining a flexible and responsive organizational structure that are its trademark. I am convinced that we urgently need initiatives like MAR to accelerate progress towards a day when all women reach motherhood healthy and literate and have access to adequate standards of care. I commend MAR and its community of friends and supporters, and I look forward to accompanying them further in this journey to help enable women to become healthy, literate and empowered so they may in turn build stronger families, communities and societies.

5
MESSAGE FROM DIANA PEREZ-BUCKFOUNDER, MOTHERS AT RISK
Never underestimate the power of a small group of committed people
to change the world. Indeed, it is the only thing that ever has.
– Margaret Mead This exciting idea, that ordinary citizens can help solve intractable problems, was very much at the core of my motivation to launch Mothers at Risk (MAR) five years ago. I wondered: with the unspeakable tragedy of maternal mortality unfolding across the globe, could a handful of individuals make a difference? Five years later, surprised and humbled by the many committed people I have encountered, my answer is a resounding ‘yes’! I am thinking first and foremost of the outstanding individuals who lead our local partner organizations and with whom we have had the privilege of working these years - Eleni, Claire, Anastasia, Iman, Nadene, Francisca, Luis… They are tireless and charismatic problem-solvers, activists and leaders working to help transform the situation for women in their communities in the Middle East, Sub-Saharan Africa and Central America. Their unwavering belief in the possibility of change gives us great optimism. Mothers at Risk, across all its activities and endeavors, is entirely volunteer-run thanks to thousands of hours dedicated by scores of truly outstanding people from all walks of life, backgrounds and nationalities. Each and every one of our volunteers brings added value to our joint effort, and it is a real privilege to be surrounded by talented, high-caliber professionals who have chosen to contribute their expertise and skills to MAR. Thanks to these collective contributions, we have been able to help bring prenatal care and safe delivery closer to rural women in Tanzania, Haiti, Kenya and Nicaragua. We have invested in the education of vulnerable girls in Egypt. And we have supported women who face motherhood alone, in extreme conditions of social, economic and emotional exclusion in Morocco and in Belgium. We have been touched by the stories of mothers, girls and babies whose lives have been impacted for
the better by these efforts. Like baby Emmanuel in nomadic Turkana, Kenya, born safe and sound thanks only to the overnight efforts of the medical team of the Nariokotome dispensary. Or Magdala, who after barely surviving the birth of her second son, became a midwife in her native Haiti to help other women avoid the same fate. And Fatima, a poor and single mother in Tangier, who can now better support herself and her daughter Jamila thanks to the job she secured after vocational training. Or Yasmeen, a girl from the slums of Cairo, who is now literate. We could not have supported any of this without the institutions and individuals who have supported us financially, starting with the startup capital provided by our founding donors, followed by other generous private donors and by organizations like Rotary, as well as private sector companies such as Alcatel-Lucent, the bpost and the Belgian National Lottery. We are indebted to them all for their vote of confidence in us. Looking back at these first five years I am immensely proud of what we have accomplished but I am equally aware of how much there is still to do. In Khmer, the language of Cambodia, childbirth is known as “crossing the river. May MAR’s work continue to serve so that more women may ‘cross the river’ safely.

6
OVERVIEW 2009-2014
2009-2014 AT A GLANCE
o 37 projects, 8 Countries, 3 continents
o Over 5000 beneficiaries
o Total grants awarded: 323,688 Euros
o Total funds raised: 433,246 Euros
OUR MISSION
Mothers at Risk (MAR) is an independent, international non-profit organization devoted to reducing the vulnerability of mothers, women
and girls living in poverty, so they may have safer pregnancies and deliveries and reach motherhood healthier and better educated.
HaitiNicaragua
Peru
Belgium
MoroccoEgypt
Kenya
Tanzania

7
THE ISSUESMothers at Risk came into being by a group of people who were moved by the unacceptable risks women around the world still face in childbirth. In these next pages, we illustrate some of the sobering facts that have moved us into action.
MATERNAL AND NEWBORN MORTALITY • Over 289,000 women die from pregnancy and childbirth-
related complications each year. That is 800 women a day• 99% of these deaths happen in developing countries• For every maternal death, approximately 20 women
suffer severe illness, injury, or disability• Maternal deaths leave one million orphan children
behind, and these children are 10 times more likely to die within two years of their mother’s death
• Nearly 3 million newborn babies die every year unnecessarily
• 90% of these maternal and newborn deaths are preventable when women have access to three types of interventions: quality care during pregnancy and birth; access to emergency obstetric care when problems arise during pregnancy and delivery; and adequate reproductive health services.
MOTHERHOOD AND THE GIRL-CHILD• Worldwide 31 million girls of primary school age are not
enrolled in school• Many of them become mothers while still girls• Research shows that the consequences of adolescent
childbearing include higher risk of complications during pregnancy and maternal mortality. Teenage pregnancies are also correlated with increased rates of infant mortality and malnutrition, lower levels of education for the mother and their children, and increased risk of poverty
• If girls stay in school beyond grade 7 they are: o More likely to have healthier children o More likely to have an average of 2.2 fewer children o More likely to send their children to school o More likely to marry 4 years later o Less likely to die in pregnancy/ childbirth
MOTHERHOOD ALONE AND EXCLUDED Beyond pregnancy and delivery, raising children in poverty can be an insurmountable challenge for those women facing the experience alone, impoverished and excluded. Some may be far from their homes, seeking refuge or asylum from conflict, violence or persecution. Some women may have lost their partners and may become sole breadwinners. Others may have become pregnant out of wedlock and be shunned by their families and communities. Some, out of desperation, may revert to dangerous back-street abortions or feel no choice but to abandon their newborn babies. We support vulnerable women experiencing pregnancy, delivery and the early years of their children alone so they and their babies may be as safe, healthy and independent as possible.

8
THE CONNECTION
WOMEN DIE FROM PREGNANCY AND CHILDBIRTH-RELATED COMPLICATIONS EACH YEAR.
289,000+289,000+
Motherless children are up to 10 TIMES more likely to die within 2 years of their mother’s death.
NEARLY
INVESTING IN MATERNAL AND NEWBORN HEALTH:
THREE MILLION THREE MILLION NEWBORN BABIES DIE EVERY YEAR.
That’s 800 women a day.
99% of these deaths occur in developing countries.
Nearly 90% are preventable.
For every maternal death, approximately 20 women suffer severe illness, injury, or disability.
{{
INVEST IN MATERNAL AND NEWBORN HEALTH
STRATEGIES TO IMPROVE MATERNAL & NEWBORN HEALTH
THE 3 DELAYS
Increase access to
family planning
Increase access to quality care for pregnancy and childbirth
Saves women’s & children’s lives
Strengthens health systems
Increase access to safe
abortion services
When a woman seeks care, she faces:
Delay in seeking help
Delay in reaching a health care facility
Delay in receiving appropriate care upon arrival
1.
2.
3.
Improves economies
WHO WINS? EVERYBODY.

9
THE PICTURE IS DIFFERENT FOR GIRLS AND BOYS
WHY DO GIRLSDROP OUT?
BUT… IF WE COULD KEEP GIRLS IN SCHOOL BEYOND GRADE 7, THEY WOULD BE:
More likely to have an average of 2.2
fewer children
More likely to have healthier
children
More likely to send their
children to school
Less likely to die in pregnancy/
childbirth
More likely to marry
4 years later
INVEST IN GIRLS’ EDUCATION
WHO WINS? EVERYBODY.
Entering School
100 girls per 100 boys
Secondary Education
84 girls per 100 boys
Primary School
92 girls per 100 boys
Enrollment rates in sub-Saharan Africa{
{
OF PRIMARY SCHOOL AGE ARE NOT ENROLLED IN SCHOOL.31 MILLION GIRLS 31 MILLION GIRLS
Tertiary Education
61 girls per 100 boys
CHILDMARRIAGE
SCHOOLFEES
SEXUAL VIOLENCE
LACK OF SANITARY FACILITIES

10
MILESTONES 2009-2014
2009
August MAR is registered in Belgium as a non-profit organizationSeptember First field visits to Egypt and NicaraguaOctober MAR partners with the Yantalo Foundation in Peru to survey over 450 mothers and pregnant
women, as well as health care providers in the upper Amazon jungle area, to assess the local communities’ use of maternal health services
November MAR Fund is established at the King Baudouin Foundation, where a group of private donors provide seed funding for MAR projects
December MAR Website goes live
2010
April MAR joins the White Ribbon Alliance for Safe Motherhood (WRA)May First project launched with Moroccan partner ‘100% Mamans’, an exchange program between
Moroccan and Belgian shelters for mothersJune First field visit to MoroccoJuly MAR inaugurates partnership with the Egyptian Association for the Development and
Enhancement of Women (ADEW) for a survey on delivery care of close to 400 mothers and 25 traditional birth attendants in the slums of Cairo
2011
January MAR starts supporting the annual salaries of midwives in a prenatal mobile clinic in the isolated Central Plateau Region of Haiti in partnership with Midwives for Haiti.
February In Nicaragua, MAR and the maternal waiting home ‘Casa Materna Cihuatlampa’ partner to address the higher maternal mortality risk and school attrition associated with adolescent pregnancies, through a reproductive and sexual health education program in the province of Jinotega
March MAR’s first fundraising recitalApril The Rotary Club Hamburg-Bergedorf sponsors a pilot project of combined life skills and
literacy for 40 girls in the Cairo slumsMay MAR admitted to membership in the World Health Organization’s (WHO) Partnership for
Maternal Neonatal and Child Health (PMNCH)August Grant awarded by the Belgian postal service bpost for a literacy program for mothers
developed by MAR in collaboration with the shelter Chevrefeuille and the Belgian literacy federation Lire et Ecrire
September MAR office inaugurated

11
2012
June MAR begins supporting the Casa Materna Ocotal in NicaraguaSeptember MAR sponsors the first in a series of trainings of midwives with the health department of the
Diocese of Musoma in TanzaniaOctober MARs funding surpasses $100,000November The Alcatel-Lucent Foundation awards MAR a grant to scale up from 40 to 200 girls the life-
skills and literacy program in the Cairo slums with local partner ADEW
2013 May MAR enters into a new partnership with the Missionary Community Saint Paul Apostle in
northern Kenya to support the maternal health of nomadic womenJune MAR launches the Friends of MAR initiative July First field visit to HaitiMarch MAR receives its largest donation from a private philanthropist: $100,000; Colgate matches it
with a $100,000-contributionDecember MAR develops a project-based partnership with the International Center for Reproductive
Health (ICRH) at Ghent University to support maternal homes in Kenya
2014 March MAR becomes a partner of Vesalius College and establishes an internship program offered to
Vesalius studentsMay The 15th MAR fundraising recital is held.June The MAR-ICRH project to support maternal homes in Kenya is selected for a grant by the
Millennium Development Fund of the Loterie Nationale July MAR is awarded a grant from the Fonds Elisabeth et Amelie to promote food security and
water access in Turkana, KenyaSeptember MAR marks its five-year anniversary

12
KENYA
Location: Turkana, Kenya
MAR Thematic Area: · Maternal health · Education and livelihoods · Infrastructure
Total Grant: 126,439 Euros
Local Partner: The Missionary Community Saint Paul Apostle (MCSPA)
Turkana is a remote, arid, semi-desert region in North-East Kenya. It is very isolated and lacks basic infrastructure and services. Its 800,000 inhabitants belong to the Turkana tribe and are semi-nomadic shepherds who live in endemic poverty. In recent years the entire region has been suffering from drought, leading to loss of livelihood assets and widespread food insecurity. With droughts becoming longer and more unpredictable due to climate change, Turkana is in a situation of ‘chronic crisis’, with families struggling to recover from one drought to the next and pastoralists unable to rebuild their herds.
Eighty percent of the population lacks acceptable access to clean water, and water-borne diseases are widespread. Education and literacy levels are low and there is limited knowledge on health and nutrition issues. Women and children are particularly vulnerable. Nationally, the maternal mortality rate is among the highest in the world, with 400 deaths for ever 100,000 live births, and the rate of mortality for children under five is 73 for every 100,000 live births.

13
OUR WORK IN KENYAOur Local PartnerThe Missionary Community of Saint Paul Apostle (MCSPA) has worked in Turkana for 27 years carrying out community-based development programs with the goal of improving the lives of the Turkana. It serves 150,000 people in a 10,000 km2 area, providing access to water, sanitation, health care, basic agriculture training, nutritional units and food aid when necessary. MCSPA works closely with the government and other non-governmental organizations, and in the area where MCSPA is active, child malnutrition is 15 percentage points lower than elsewhere in the region.
Our ContributionMAR’s goal is to support MCSPA’s comprehensive efforts to improve the living conditions and coping mechanisms of the people of Turkana. We do this through the following initiatives:
o A project to increase access to basic health services and mother and child-care for pregnant and lactating women of Kokuselei by establishing mobile clinics and training village health promoters in seven villages in Turkana. This project also focuses on improving overall health and nutrition through training on food preparation and the introduction of greater diversity in the local diet.
o MAR has facilitated a partnership between MCSPA and the ‘Elisabeth et Amelie Fund’ to improve access to water for domestic and agricultural use in the Nakwasuro area of Turkana, that was also drought affected. The project involves the drilling of a borehole and the installation of a solar pumping system as well as promoting the establishment of small-scale, women-led agriculture to complement nomadic pastoralism.
o MAR has also supported the construction of a community room at the dispensary that is now used for holding workshops with the women and trainings.
o Due to the extreme drought in the region in 2013 and 2014, MAR also assisted with the provision of emergency food aid to vulnerable families for a three- month period targeting in particular children under five, pregnant and lactating women and the elderly.
Thank you very much for working together with us in so many aspects, you are really contributing to a deep change in Turkana. We hope we can continue to work together for many years.
You are our angels in Brussels! – Eleni, representative of MAR local partner MCSPA in Kenya, 2014

14
EGYPT
Location: Cairo, Egypt
MAR Thematic Area: · Education and livelihoods · Maternal Health
Total Grant: 117,942 Euros
Local Partner: The Association for the Development and Enhancement of Women (ADEW)
Urban PovertyAs is true in many parts of the world, urbanization and urban poverty in Egypt are rising, as populations of urban slums grow both in absolute numbers and relative to the rest of the urban population. Cairo has one of the largest slum populations in the country and the world, known as aashwa’iat, or ‘random’ areas. They house hundreds of thousands of people in crowded conditions, have inadequate or insufficient basic amenities like running water, electricity, and sanitation, and are exposed to environmental hazards and to decaying or weak infrastructure. The millions living in these urban slums, are largely unaccounted for and are therefore ‘invisible’ and, to a great extent, forgotten. Life in these urban slums is particularly harsh for women and girls, who additionally face societal and cultural prejudices.
Opportunities for girlsGirls in these slums grow up in an environment of drastic inequality compared to boys. They usually leave school before their brothers and remain mostly confined to their homes where their potential to escape poverty is slim. They join the ranks of the over 90 million young girls thought to be out-of-school worldwide, of which more than a quarter become mothers before the age of 18. In Egypt, the government and civil society organizations have made considerable strides towards the goal of achieving universal primary education, but in many rural areas and urban slums, some 50 percent of school-age children either do not attend school, or eventually drop out around the age of 11. Gender disparity remains a challenge.
Deliveries in poor urban settingsEgypt has made remarkable progress in efforts to curb maternal mortality, having reduced the maternal mortality ratio between 1990 and 2010 by over 71% and considered on track to achieve the maternal health Millennium Development Goal (MDG 5) by the 2015 deadline. However urban population growth is outstripping the capacity of many urban health centers to provide quality maternal services, resulting in lower standards of care and evidence of discrimination of poor urban women. This marginalization is resulting in many poor urban women choosing to deliver at home with unskilled attendants despite the proximity of health centers.

15
OUR WORK IN EGYPTOur Local PartnerEstablished in 1987, the Association for the Development and Enhancement of Women (ADEW) advocates for women’s rights in Egypt and supports women living in the poorest urban and peri-urban slums, in particular female–headed households. ADEW’s initiatives include micro-credit lending, legal services, literacy promotion for women and girls and health services.
Our ContributionGirls Dreams and Literacy (GDL) is a combined program developed by ADEW and MAR to empower girls in poor urban communities to gain life-skills and literacy and to create opportunities for staying in, and/or returning to school. The program’s objectives are to:i) Promote literacy and life skills for girls through the ‘Girls’
Dreams and Literacy’ curriculumii) Document obstacles and challenges preventing girls from
completing formal education in targeted communities,iii) Strengthen community-wide learning and access to formal
educational opportunities for girls through the participatory approach of ‘Facilitated Learning’.
A first pilot project for 40 young women was funded by the Rotary Club Hamburg-Bergedorf, and following its success a scaled-up program for 200 girls is being implemented over a period of three years (2012-2015) funded by the Alcatel-Lucent Foundation, whose employees have also volunteered their time.
Survey of ‘dayas’ and mothers: To better understand the enduring preference of poor urban mothers for deliveries with traditional birth attendants (“dayas’), MAR and ADEW surveyed almost 400 mothers and 26 dayas in two of Cairo’s largest slums. The survey showed these women face unique challenges to accessing quality facility-based deliveries and that targeted interventions will be necessary to improve the quality and patient care at facility-based deliveries and to promote the uptake of these services by poor urban women are needed. MAR and ADEW will be working on developing programs along two mutually reinforcing lines of action:a) to promote new, officially-sanctioned roles for the dayas in
community health promotion and in advocacy for institutional deliveries.
b) to promote an increase in institutional deliveries in the slums by ensuring better access to skilled care for deliveries, including through enhanced quality care at hospital deliveries.
Again, thank you for your interest, your passion, and your belief in our work; this kind of partnership is what keeps us going & managing our way through the challenges we face. You’re not just partners in this program, but an inspiring developmental institution that we’re so fortunate to be
working with on equal grounds– Sarah Hani, representative of MAR local partner in
Egypt, ADEW, 2014

16
HAITI
Location: Hinche, Haiti
MAR Thematic Area: Maternal health
Total grant: 19,534 Euros
Local Partner: Midwives for Haiti
Haiti is the poorest country in the Western Hemisphere and has the highest maternal mortality rate in the region, at 300 deaths for every 100,000 live births. Due to a lack of resources, and workforce attrition, Haiti has a severe shortage of skilled healthcare providers. Only 26 percent of births are attended by skilled healthcare professionals. To make matter worse, the devastating 2010 earthquake damaged many healthcare facilities. Most births take place at home assisted by non-qualified persons unable to help in the event of complications. Haiti also has the highest rates of infant and under-five mortality (89 for every 1,000 live births) in the Western Hemisphere. A quarter of all newborns have low birth weight and hundreds of thousands of children suffer from chronic malnutrition. Better access to skilled care during pregnancy and delivery is desperately needed in order to ensure healthy pregnancies and healthy babies.

17
OUR WORK IN HAITIOur Local PartnerMidwives for Haiti is a small US-based organization founded in 2005. Its core mission is to enable access to maternal and infant care in remote areas in Haiti. The organization works with the Ministry of Health to provide obstetrics training to Haitian auxiliary nurses so they can attend births and provide prenatal care to rural women that otherwise have limited access to medical care during pregnancy. Our ContributionOne way to expand access to prenatal care in hard-to-reach or underserved areas is through mobile health clinics. Mothers at Risk sponsors midwives who travel with Midwives for Haiti’s prenatal mobile clinic in the remote Central Plateau Region in Haiti. The mobile clinic reaches 16 villages monthly and provides prenatal care to hundreds of women. Prenatal care ensures that any problems are detected and addressed in time, and helps the mother take care of her health and that of her unborn baby.
We’re so glad that you’re supporting Magdala and Marie Denise! You are making an impact on more than just these
two midwives. You are helping their families and the hundreds of women in Haiti’s central plateau who benefit from their experience and compassion. Thanks again for
your amazing support!– Emily Davis Midwives for Haiti 2014

18
NICARAGUA
Location: Jinotega and Ocotal, Nicaragua
MAR Thematic Area: Maternal health
Total Grant: 14,924 Euros
Local Partners: Casas Maternas Mery Barreda and Cihuatlampa
Nicaragua is, after Haiti, the poorest country in the region and has one of the highest rates of maternal mortality in Latin America, at over 90 per 100,000 live births. Although the number of women dying in childbirth has decreased over the past 25 years, maternal mortality remains especially high among women in rural areas due to lower prenatal care coverage and lower rates of deliveries attended by skilled personnel. While nationally 74 percent of births are attended by skilled health professionals, this figure drops to just over 50 % in rural areas. Nicaragua also has one of the highest adolescent fertility rates in the world with over a quarter of girls aged 15-19 already having had a baby. Research shows that the consequences of adolescent childbearing include higher risk of complications during pregnancy and maternal mortality. Teenage pregnancies are also correlated with increased rates of infant mortality and malnutrition, lower levels of education for the mother and their children, and increased risk of poverty.

19
OUR WORK IN NICARAGUAOur PartnersCasas Maternas (maternal waiting homes) form an integral part of the national strategy to curb pre-natal, maternal and neonatal mortality by sheltering expectant mothers from isolated rural communities with high obstetric risk during the weeks before delivery. At the Casas Maternas they are monitored by health professionals, and deliver in nearby hospitals or medical centers with skilled care rather than at home. MAR has supported the Casa Materna Cihuatlampa in the region of Jinotega, and the Casa Materna Mary Barreda in Ocotal, Nueva Segovia, which each shelter an average of 300 mothers yearly, a quarter of which are adolescents.
Our ContributionMAR has supported a year-long community outreach program to promote maternal, sexual and reproductive health awareness in Jinotega and surrounding villages. This program aimed to ensure that adolescents who are already pregnant receive proper prenatal care and are attended in delivery by skilled personnel; and to help reduce the number of unwanted adolescent pregnancies through information and awareness-raising. Under the project, fifty health community promoters and youth leaders were trained in maternal, sexual and reproductive health issues and in community outreach techniques, including peer-to-peer education. Once trained, they went into the communities to raise awareness through workshops, focus groups, visits to schools and presentations in communities and in the Casa Materna.
MAR also designed and funded an organizational and needs assessment of the Casa Materna Ocotal to identify urgent and long-term needs of the maternal home. This resulted in a plan to strengthen the Casa Materna across different areas including:o Infrastructure repairs and basic equipmento Running costs (including food, staff, utilities, etc)o Promoting community and institutional partnerships to support the Casao Improving administrative and financial management processeso Strengthening the program of educational activities for sheltered mothers o Supporting training for the Casa’s staffo Identifying funding sources
According to the local school professor Mrs. Afrania, with the implementation of the Mothers at Risk program, teenage
pregnancies have been decreasing at the high school at a noticeable rate compared to previous years.
– Report by local project manager Rina, Jinotega Nicaragua, 2013

20
MOROCCO
Location: Tangier, Morocco
MAR Thematic Area: Education and livelihoods
Total Grant: 27,152 Euros
Local Partner: 100% Oumahat
Pregnancy out of wedlock carries a heavy social stigma in Morocco. Despite an important reform to Morocco’s family code, the Moudawana, in 2004 the unwed mother and her baby have few rights under current law. It is considered a great dishonor to the family, and the pregnant woman is often shunned or pressured to abandon her baby. Most of these abandoned babies are institutionalized and face life-long discrimination.
21
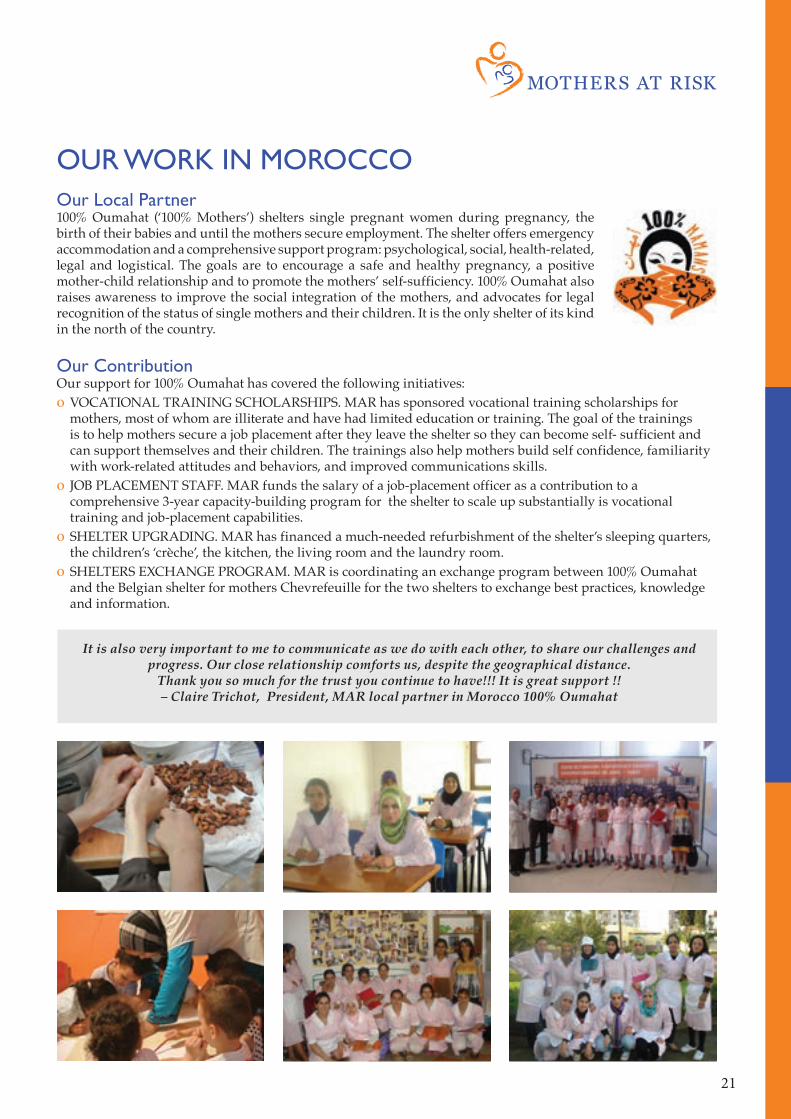
OUR WORK IN MOROCCOOur Local Partner100% Oumahat (‘100% Mothers’) shelters single pregnant women during pregnancy, the birth of their babies and until the mothers secure employment. The shelter offers emergency accommodation and a comprehensive support program: psychological, social, health-related, legal and logistical. The goals are to encourage a safe and healthy pregnancy, a positive mother-child relationship and to promote the mothers’ self-sufficiency. 100% Oumahat also raises awareness to improve the social integration of the mothers, and advocates for legal recognition of the status of single mothers and their children. It is the only shelter of its kind in the north of the country. Our ContributionOur support for 100% Oumahat has covered the following initiatives:o VOCATIONAL TRAINING SCHOLARSHIPS. MAR has sponsored vocational training scholarships for
mothers, most of whom are illiterate and have had limited education or training. The goal of the trainings is to help mothers secure a job placement after they leave the shelter so they can become self- sufficient and can support themselves and their children. The trainings also help mothers build self confidence, familiarity with work-related attitudes and behaviors, and improved communications skills.
o JOB PLACEMENT STAFF. MAR funds the salary of a job-placement officer as a contribution to a comprehensive 3-year capacity-building program for the shelter to scale up substantially is vocational training and job-placement capabilities.
o SHELTER UPGRADING. MAR has financed a much-needed refurbishment of the shelter’s sleeping quarters, the children’s ‘crèche’, the kitchen, the living room and the laundry room.
o SHELTERS EXCHANGE PROGRAM. MAR is coordinating an exchange program between 100% Oumahat and the Belgian shelter for mothers Chevrefeuille for the two shelters to exchange best practices, knowledge and information.
It is also very important to me to communicate as we do with each other, to share our challenges and progress. Our close relationship comforts us, despite the geographical distance.
Thank you so much for the trust you continue to have!!! It is great support !!– Claire Trichot, President, MAR local partner in Morocco 100% Oumahat

22
TANZANIA
Tanzania continues to have one of the highest maternal mortality rates in Africa and the world at 454 deaths for every 100,000 live births. And Tanzania is one of the ten countries in the world where two-thirds of all babies’ deaths globally occur. The scarcity of trained health professionals and the difficulties for women in reaching hospital for pre-natal check-ups and delivery, due to dispersed health centers and hospitals in rural areas, are key challenges. In addition, there is a critical lack of health service professionals who are skilled in providing comprehensive emergency obstetric and newborn care, and few health facilities equipped for this standard of care. Disease (including but not limited to malaria and HIV/AIDS), early pregnancies and a paucity of family planning services all contribute as well towards the present situation, particularly in rural areas. The Mara region is among the three worse performing regions in the country for skilled birth attendance during delivery, with only one in three births taking place in a health facility (compared to the national average, which is 50%).
Location: Mara Region, Tanzania
MAR Thematic Area: Maternal health
Total Grant: 12,697 Euros
Local Partners: Diocese of Musoma

23
OUR WORK IN TANZANIAOur Local PartnerEstablished in May 1975, the Roman Catholic Diocese of Musoma undertakes pastoral and development activities in the Mara Region. The Diocese is particularly concerned with health care and it focuses on reducing infant and maternal mortality and morbidity in the area. Annually, over 17,000 patients benefit from prenatal care and 732 deliver in the Diocese’s twelve health facilities. Eight of the health facilities owned by the Diocese are equipped to provide comprehensive emergency obstetric and new born care. Our ContributionMAR sponsors training workshops on basic emergency obstetric care (EOC) and antenatal care (ANC) for scores of service providers (nurse midwives, nursing officers, public health nurses, clinical officers) working within the health care facilities managed by the Diocese of Musoma. This training is based on the national curriculum and is lead by expert facilitators from the Ministry of Health and Social Welfare. Maintaining these health care workers’ skills and knowledge up-to-date is essential to saving the lives of the mothers and babies they attend to. MAR also sponsors ongoing oversight and supervision of this staff to ensure consistent quality and standards and to identify gaps in performance. MAR and the Diocese’s efforts are fully aligned with the priorities of the recently-adopted Mara Region Strategic Plan for the Accelerated Reduction of Maternal and Newborn Deaths 2013-2016.
We present our sincere thanks for the good support we receive from Mothers at Risk. This workshop enlightens our mind and capabilities to provide quality care to reduce maternal and child mortality
rates. May almighty God bless you all, guide you all and protect you all.– Anastasia, Diocesan Health Secretary, Musoma, Tanzania

24
BELGIUM
Across European cities, urban poverty and inequality persist. Poor urban women, and particularly new immigrants, deal with a complex range of challenges including unemployment and low income, low levels of education and skills, dysfunctional family situations, domestic violence and a lack of social and family support networks. Motherhood in this context is particularly difficult and has the potential to increase their vulnerability.
Location: Brussels, Belgium
MAR Thematic Area: Education and livelihoods
Total grant: 5000 Euros
Local Partner: Chevrefeuille

25
OUR WORK IN BELGIUMOur Partner“Chevrefeuille” is a shelter for vulnerable mothers with over 40 years of experience. Since it opened its doors, it has sheltered over 2000 pregnant women and new mothers of both Belgian and immigrant origin. It enjoys an outstanding reputation for its multi-dimensional support of mothers covering their social, administrative, educational, emotional and practical needs. Chevrefeuille’s goal is to help women become self sufficient, develop strong bonds with their baby and access housing and employment in order to be able to sustain themselves and their children independently.
Our ContributionIn partnership with the Belgian literacy federation ‘Lire et Ecrire’, MAR and Chevrefeuille have developed a literacy program for illiterate immigrant mothers, which was selected by the Literacy Fund of the Belgian Post (bPost) for a start-up grant. In this program Chevrefeuille provides scholarships to immigrant mothers and supports them over several years as they progress through various stages of literacy, become more self-sufficient and contribute to their children’s own literacy and schooling. MAR has also developed and exchange program between Chevrefeuille and the shelter for mothers ‘100% Oumahat’ in Tangier, Morocco to promote and facilitate the exchange of best practices, knowledge and information between these two shelters.
This year was the first time I have taken literacy lessons. I feel like I have made a lot of progress and I have much more confidence now. I relied on others before, but now I feel like I can do a lot more on my own. When I look for a job I can express myself and ask questions. I understand the
signs on the street, I can now get around on my own. I feel very motived and ready to continue learning.
– JN, immigrant mother, participant in literacy program
After 3 intense and fascinating days, thanks to all of you, we return to Tangier with the spirit ‘oxygenated’ and a full heart…completely energized! We have
had some marvelous exchanges and we leave feeling like we have accomplished so much more than our original objectives. You cannot imagine just much we are now full of hope and certainty about our choices and our daily struggles”.
– Claire Trichot, President 100% Oumahat

26
PERU
Despite economic growth in Peru over the last years, more than half of the rural population continues to live in poverty. The maternal mortality rate at 90 deaths per 100,000 live births, although a considerable improvement from 2000 levels, is still unacceptably high. Most women who die in childbirth are poor, indigenous rural women. Much remains to be done to ensure access to adequate pre-natal, natal and post-natal care for all Peruvian women, in particular those in hard-to-reach areas.
Location: Yantalo, Peru
MAR Thematic Area: Maternal health
Total Grant: in-kind
Local Partner: The Yantalo Foundation

27
OUR WORK IN PERUOur Local PartnerThe Yantalo Foundation is a local organization working in the village of Yantalo and surrounding rural areas, in the province of San Martin, in the upper Amazon jungle. The mission of the Yantalo Foundation is to improve health and education standards in the area. The Foundation is building a 16-bed International Clinic to serve all the people of the San Martin region, regardless of their ability to pay, while also serving as a training center for Peruvian medical students and physicians.
Our ContributionMothers at Risk partnered with the Yantalo Foundation, the Tarapoto Nursing School and the Yantalo local administration to develop and implement a maternal health assessment in Yantalo. 465 mothers and pregnant women, as well as traditional birth attendants and the local health staff were interviewed to better assess the uptake of maternal health services in the area. The survey showed evidence of several challenges, including inconsistent, incomplete prenatal care; a low rate of postnatal check-ups; low awareness of sexual and reproductive health issues; high incidence of domestic violence; and high incidence of teenage pregnancies. As a result of this assessment, the Yantalo Foundation was able to develop targeted strategies to increase prenatal coverage, encourage postnatal check-ups and enhance overall reproductive health in the area.

28
FINANCIAL SNAPSHOTS
MAR Sources of Funding
Private46%
MAR mobilized more than 430,000 Euros
Funds Raised (000’ of Euros)
(in Euros)
* Estimate
More than 300,000 grantsawarded for 37 projects
Grants awarded (000’ of Euros)
Summary of funds raised, grants awarded and available funding
* preliminary figures as of September 30th 2014
Events12%
Institutional13%
Corporate29%
Total 2009-2014: 433,246 Euros
17.3
48.4
96.8
139.9
122.7
7.3
26.915.4
119.3
154.6
Summary 2009 2010 2011 2012 2013 2014 (*) TotalMAR Fund 15,000 7,813 31,195 7,736 122,935 110,480 295,159 MAR ASBL 2,373 - 12,290 89,126 16,999 12,300 133,087 Other 5,000 5,000 Funds Raised 17,373 7,813 48,486 96,862 139,934 122,780 433,246 MAR Fund - 7,345 21,978 9,965 44,386 137,084 220,758 MAR ASBL - - - 5,440 74,930 17,560 97,930 Other - - 5,000 - - - 5,000 Grants Awarded - 7,345 26,978 15,405 119,316 154,644 323,688 MAR Fund 15,000 15,167 23,444 21,029 97,336 65,974 65,974 MAR ASBL - - 9,086 89,199 30,136 16,961 16,961 Available Funds 15,000 15,167 32,530 1,10,228 127,471 82,936 82,936

29
OUR PARTNERSProject Partners:Kenya: Missionary Community Saint Paul Apostle (MCSPA)Haiti: Midwives for HaitiEgypt: The Association for the Development and Enhancement of WomenNicaragua: Casa Materna Mery Barreda, Casa Materna ChihuatlampaTanzania: The Diocese of MusomaBelgium: ChevrefeuillePeru: The Yantalo FoundationMorocco: 100% Mamans
Special ThanksWe want to thank the following people and organizations for their pro bono support to MAR in key areas:o The web solutions company Crystal Digit for developing and managing our website and communicationso The employee gift-matching programs of Google and Colgate.o The design of our 2009-2014 Report by Ajay Singh of Chilly Factor and by Alexandra Birladianu of the
Alcatel-Lucent Foundationo The law firm KS4V (Keuleneer, Storme, Vanneste, Van Varenbergh, Verhelst) for legal advice.o Katharina von Wendt of designwerkstatt ([email protected]) for her design and layout of MAR
printed materials. o Level 13 Europe Ltd, for donating proceeds of art and musical eventso Vinos Alfonso Escubos for recurrent contributions to MAR’s fundraising events
simple web solutions for your company
Institutional Partners: King Baudouin FoundationThe International Center for Reproductive HealthThe White Ribbon AllianceThe Partnership for Maternal Newborn and Child Health
Funders:The Alcatel-Lucent Foundation bpostLoterie Nationale, Rotary Club Hamburg-BergedorfElisabeth and Amelie Fund

30
OUR TEAM: MOTHERS AT RISK BOARDDIANA PEREZ BUCK (Board, Executive Team) A former Fulbright scholar, and a graduate of the Fletcher School of Law and Diplomacy, in Boston, Diana worked for the UN Volunteers Program (UNDP) for seven years and helped the US non-profit Vital Voices Global Partnership develop a capacity-building program for Afghan women parliamentarians. She currently serves on the Board of the shelter for disadvantaged mothers ‘Chevrefeuille’ in Brussels.
OLIVIA LOEWE (Board, Executive Team) earned degrees in law and business administration at the Universidad Pontificia de Comillas (ICADE) in Madrid and, as a Deutscher Akademischer Austausch Dienst Scholar, a Master of Law at the Ruprecht- Karls- University in Heidelberg. She has practiced business law in Madrid, and has worked as Director in the banking sector in Frankfurt, Madrid and Milan. Before joining Mothers at Risk she was active with an anti-poverty nonprofit in Bogotá, Colombia.
BECCA NASRALLAH (Board, Executive Team) is a dental surgeon by training. She obtained a degree at the United Medical and Dental School of Guys and St Thomas, London University, and had a private practice in Lebanon.
KATHLEEN BECKMANN is an expert at the German Ministry for Development Cooperation (BMZ) and was most recently the BMZ’s Nicaragua Country Director
DANA STRUPOVA is a lawyer by training, she has practiced law in the U.S., Germany and the Czech Republic, has been a Director at the professional services firm PricewaterhouseCoopers and is now General Counsel for the award-wining Dialogue Social Enterprise.
RACHEL HAMMONDS currently works as legal adviser for a research project on global health and human rights at the Institute of Tropical Medicine in Antwerp, Belgium. She was previously a consultant with Medecins Sans Frontieres and researcher at Harvard University’s François-Xavier Bagnoud (FXB) Center for Health and Human Rights.
DR. MARIE DIANE BUCK’s field is Education and Organizational Leadership. Diane has taught extensively at the university level, and has served for most of her career as Director of intercultural programs as well as government programs to enhance opportunities for the elderly and for physically and intellectually-challenged persons.

31
CRISTINA SAMITIERDirector (Operations). Cristina has degrees in Business and Accounting from Argentina and an MBA from the INSEAD Business School in Fontainebleau / Singapore. She worked in Mergers and Acquisitions in Argentina for 8 years and was most recently a Management Consultant at Bain & Company Belgium.
TERESA POPPELWELLDirector (Programs). Teresa is a planning consultant with more than fourteen years of policy, program and management experience with the United Nations and international NGOs. Teresa has a MA in Planning from the University of British Columbia (1997) and an MSt in Forced Migration and Refugee Studies from the University of Oxford (2002). Teresa has used her professional training and experience to conduct sector assessments, develop poverty reduction strategies, and design programs and projects in a number of countries including Afghanistan, Iran, Burma, Maldives, Pakistan, Philippines, and Indonesia.
MIRIAM CACERESFundraising Coordinator. Miriam obtained a degree in Business Administration in Peru and an MBA in International Marketing in Germany and has sales and marketing experience in the medical and pharmaceutical industries.
LETICIA DE ALVEARVolunteer Coordinator. Leticia is a lawyer by training and a sworn translator
PAULINE CAMACHO FIELDINGEvents Coordinator. Pauline is Director of Level 13 Europe, a boutique EU policy consultancy. Pauline is a conference interpreter at the European Union institutions (from English, French, Portuguese and Spanish into German), and is a trained psychotherapist
MOTHERS AT RISK EXECUTIVE TEAM

32
MANAGEMENT COMMITTEE,MAR FUND, KING BAUDOUIN FOUNDATIONTo manage our funds with the utmost rigor we have created the Mothers at Risk Fund at the King Baudouin Foundation in Brussels, a public institution involved in social and economic development in Belgium and abroad. The Mothers at Risk Fund is lead by a Management Committee chaired by an expert in the field of maternal health, and composed of donors and philanthropy advisers.
PROF. DR. ALAIN VOKAERProfessor Emeritus of Obstetrics and Director Emeritus of the Mother and Child Clinic at the Brugmann University Hospital in Brussels.
DR. GEORG FROWEINPartner, Hengeler Mueller, Frankfurt, Germany.
DR. EDURNE NAVARRO VARONAPartner, Uría Menéndez, Brussels, Belgium.
MR. GEORGE A. NAZISenior Advisor, Network Services Strategy Lead, Accenture, Brussels, Belgium
DR. FRANCOISE PISSARTFrancoise Pissart, Director, Fondation Roi Baudouin
DR. SVEN VÖLCKERPartner, Latham & Watkins, Brussels, Belgium.

33
MAR ADVISORSDr. Ramiz Alakbarov (Azerbaijan) is United Nations Population Fund (UNFPA) Representative in Haiti. He has been Head of Office for UNFPA in South Sudan and the UNFPA Regional Desk Adviser for Arab States in New York. Dr. Alakbarov has worked for over 15 years for the United Nations, including in Central Asia, Eastern Europe, Turkey, Iraq, Sudan and the Democratic Republic of Congo. His published research covers, among other topics, reproductive health matters and humanitarian response.
Dr. Sarah Sabry (Egypt), Guest Lecturer/Research Associate, University of Zurich, Switzerland. Dr. Sabry’s research is focused on urban poverty, informal areas, civil society and social policy in Egypt. She has extensive fieldwork experience in Egypt’s informal areas. She has been a consultant for various organizations including the Ford Foundation, the International Institute for Environment and Development (IIED), the International Development Research Centre (IDRC) and the Arab Human Rights Fund. Past positions include chairing the board of a local Egyptian NGO working on poverty reduction, supporting the establishment of the Community Service program at the American University in Cairo and teaching Political Economy of Development at SOAS.
Dr. Eleanor O’Gorman (Ireland) is Senior Associate with the Centre for Gender Studies and Research Associate with POLIS at the University of Cambridge in the UK. Eleanor runs a private consulting practice on international conflict and development including issues of gender, peacebuilding and aid strategy. Her clients include the United Nations, the European Union, the UK Government and GIZ (Germany). Her field experience includes Nepal, Sri Lanka, Pakistan, Democratic Republic of Congo, Liberia, and Zimbabwe. Eleanor previously served as a Senior Adviser with the United Nations in New York and Brussels. She is the author of 2011 book titled Conflict and Development with Zed Books, London.
Dr. Jean Evrard (Belgium) is Head of Neonatology and Pediatrics at the Namur Regional Hospital in Namur, Belgium. A neonatologist by specialization, he has served as the Head of the neonatal intensive care unit for over 20 years. Dr. Evrard has volunteered in Senegal for several development projects, including the construction of a maternity, and has led pediatric projects in the Ghoussous slums north of Cairo for the Belgian organization FACE Charity.
Stefanie von Westarp (Canada) just completed three years in Haiti as Deputy Head of Aid, for Canada’s Department of Foreign Affairs, Trade and Development (formerly CIDA). Prior to this Stefanie has worked in South Sudan, Honduras and Madagascar in various aspects of development, including public health.
Dr. Angelika Wolfrum (Germany) is Assistant Medical Director at the Department of Obstetrics and Gynecology, Marienkrankenhaus Schwerte, Germany.
Prof. Dr. Alain Vokaer (Belgium) recently retired as Head of the Mother and Child Clinic at Brugmann University Hospital in Brussels, and as Professor of Obstetrics at the Université Libre de Bruxelles. He is a long-time practitioner specializing in pregnancies with complications.
Edmund Bengtsson (Denmark) is the former Head of the Evaluation Unit and currently Knowledge Manager at the United Nations Volunteers Program (UNV), part of the United Nations Development Program (UNDP) at UNV Headquarters in Bonn, Germany. He has worked for UNDP for over 25 years, both in African country offices and in Europe serving most recently as Head of Evaluation and Policy.
Dr. Renee Herfs (Germany) is a Gynecologist-Obstetrician in private practice in Grünwald-Munich, Germany
Catherine Adams (US) is Supervising Attorney specializing in gender and domestic violence at Legal Aid, West Virginia

34
MAR FUNDRAISING RECITALSWe wish to thank the following musicians who have generously performed pro bono in the course of 15 recitals to raise funds for Mothers at Risk projects:
1. Martine Reyners (Soprano)2. Louisa Petais (Mezzo Soprano)3. Patrick Heidsieck (Pianist)4. Dmytro Sukhovienko (Pianist)5. Rie Yamamoto (Pianist)6. Tatiana Longuinova (Pianist)7. Elodie Vignon (Pianist)8. Laure Stehling (Flute)9. Matthew Zadow (Baritone)
10. Eve Stehling (Author)11. Peter Tomek (Pianist)12. Hanna Selivanava (Soprano)13. Maria Palatine (Harp and Voice)14. Sophie de Tillese (Mezzo-Soprano)15. Marayana Butko (Pianist)16. Anne Sophie Maier (Backup Voice)17. Max de beer (Pianist)18. Estelle Goldfarb (Violinist)
19. Jasminka Derveaux (Lecturer)20. Dimitri Sesmis (Violinist)21. Caroline Stinson (Cellist)22. Fabian Fiorini (Pianist)23. Dimitra Mantzouratou (Pianist)24. Anait Karpova (Pianist)25. Caroline Stinson (Cellist)

35
36
EVENTS
A delegation from the International Studies Abroad
program visits MAR
MAR invited by US Ambassador to Belgium
MAR stand at St. Anthony’s Chrismas market
Speaking about MAR
Speaking about MAR
MAR launches the ‘CineMAR’ series
MAR speaks on International Women’s Day at St. John’s
International School
MAR at Procter & Gamble
Employee Day
MAR Art Vernissage
MAR featured at‘Easy Sundays’ Fundraiser
MAR at National Literacy Conference

37
MAR IN THE NEWS
MAR mentioned in Harper’s Bazaar
MAR mentioned in Procter & Gamble magazine
Interview of MAR Vicepresident in Paulus Rundbrief
MAR quoted in Egypt Community Times
Interview of MAR President in BCT Magazine
MAR mentioned in Seattle Times
Interview of MAR volunteer in European Parliament

38
VOLUNTEERS
Eva Elmet Georgina Ferrer
Danielle Van de Putte Diane Mazzitelli
Jola Montgelas
Isabel Yglesias
Engy Fahmy
Gordana Popovic
Eloisa de la Pena
Julia Borneman
Brigitte Straathof
Adrian Fielding Alexandra Birladianu Antonella Vittore
Catherine Chevallier Caroline BorggreveCarine Henoque
Ajay Singh
Louise CoganKelsey Lefebvre
39
Rocio Uriarte
Patricia Wallis
Sabine Elsayegh
Nima Shahsavari
Maya Bensalem Mikaela Nordenfelt
Patricia D’Amico
Nicole Pacheco
Stephanie Castro
Salome Cisnal
Yulia Andreeva
Samora Basil
Manuela Van Voorst Margaret DennisLucila Rivera
Maria Palatine Maria Roldan Marta Diez
Maria Barea
Maria Escubos
Penelope Wyatt
Mariela Nino Pineda

40
WORKING TOGETHER
As an intern at MAR I was able to see that a small team is able to accomplish very large things with the right amount of hard work and passion.
– Stephanie Castro, MAR intern

41
Working with you has been a real pleasure: your professionalism, the commitment of your members, the generosity of your donors, your mission to improve the conditions of each of the women and children who
have benefitted from your help...– Marguerite Beaudoin, Project Manager, King Baudouin Foundation
It has been a please to lend support to the great cause and work of MAR and work with such a dynamic and diverse group of talented and committed women. The professionalism and calibre of the volunteerism of
MAR is unique and inspiring.– Dr. Eleanor O’Gorman, MAR adviser
42
FIELD VISITS
43

44
Mothers at Risk, a.s.b.l.23 Rue Darwin1050 Brussels, [email protected]
Mothers at Risk FundKing Baudoin FoundationRue Brederodestraat 21, 1000 Brussels, [email protected]