Manual small incision cataract surgery for subluxated cataract with lens coloboma
3
Contact Lens & Anterior Eye 35 (2012) 89–91 Contents lists available at SciVerse ScienceDirect Contact Lens & Anterior Eye jou rn al h om epa ge: www.elsevier.com/locate/clae Case report Manual small incision cataract surgery for subluxated cataract with lens coloboma Ruchi Goel, Saurabh Kamal ∗,1 , Bhawna Khurana, Sushil Kumar, K.P.S. Malik, Sonam Angmo Bodh, Malvika Singh Guru Nanak Eye Centre, New Delhi, India a r t i c l e i n f o Keywords: Subluxated cataract Lens coloboma Manual small incision cataract surgery a b s t r a c t Introduction: The lens coloboma results from a segmental defective or absent development of the zonules. It is usually unilateral and bilateral cases are rare. These eyes are at greater risk of complications during cataract surgery due to ocular malformations. In addition the capsular bag requires stabilization using modified capsule tension ring, capsular tension segment or capsular anchor. Methods: Lens extraction is indicated for cataract or subluxation if visual function is sufficiently compro- mised. We report our surgical experience in a patient with bilateral isolated lens coloboma by performing manual small incision cataract surgery (MSICS) in left eye and phacoemulsification in right eye. Results: The nuclear rotation was hampered because of the lack of zonules and presence of lens coloboma. MSICS was converted to the intracapsular technique in left eye, though breaking the nucleus into pieces during phacoemulsification in right eye enabled its mobilization and successful completion with implan- tation of modified capsule tension ring. Conclusions: A patient with lens subluxation and lens coloboma is better managed by phacoemulsification as compared to the MSICS. © 2011 British Contact Lens Association. Published by Elsevier Ltd. All rights reserved. 1. Introduction Lens coloboma represents incomplete formation of the lens due to failure of fetal fissure to close completely. Segmentally defective development or absence of zonules results in a coloboma of the lens secondary to flattening of the equator in the region of the zonular defect [1]. Coloboma of the lens is typically unilateral and located inferiorly; and if bilateral it is seen to be symmetrical [2]. Cataract is said to occur at an earlier age than normal in such cases and it maybe a posterior subcapsular variant or a dense nuclear cataract. Lax- ity of capsule and zonules makes the cataract surgery challenging. Placement of intraocular implant poses problems of stabilization and centration. The manual small incision cataract surgery (MSICS) has become popular in India although phacoemulsification gives better unaided visual acuity [3], but has been found to be effective and economical [4,5] requiring less capital investment. We describe our surgical experience in the management of a case with bilateral subluxated cataract with symmetrical lens coloboma using MSICS in one eye and phacoemulsification in the other eye. ∗ Corresponding author at: Guru Nanak Eye Centre, Maulana Azad Medical Col- lege, New Delhi, India. Tel.: +91 9953715616. E-mail address: [email protected] (S. Kamal). 1 361, Sector – 30, Faridabad, Haryana 121008, India. 2. Case report 37 year old male presented to the out-patient department with complain of gradual deterioration of vision in both eyes. Best cor- rected visual acuity (BCVA) was 20/400 OD and 20/200 OS, with a manifest refraction of −12.00 DS both eyes. Intraocular pressure was 12 and 14 mm Hg in OD and OS respectively. On examination, the patient had bilateral visually significant cataract with kidney shaped lens coloboma and absent zonules on the temporal side extending from 8 o’clock to 11 o’clock and 2 o’clock to 5 o’clock in OD and OS respectively. There was bilateral temporal 180 ◦ sub- luxation (Fig. 1A and B). Gonioscopy revealed bilateral open angles. There was no uveal or retinochoroidal coloboma. Posterior segment showed tessellated fundus and posterior vitreous detachment. The patient was posted for left eye MSICS under peribulbar anes- thesia. Sclerocorneal tunnel was dissected superiorly and scleral flap was dissected at 4 o’clock for fixation of modified capsular ten- sion ring (M-CTR). Following continuous curvilinear capsulorrhexis (CCC) of size 5 mm and complete hydro procedures, nucleus failed to rotate (Fig. 2A). Finally the entire nucleus was removed using irrigating vectis due to inability to prolapse it out of the bag. After anterior vitrectomy, another scleral flap was dissected at 10 o’clock. A posterior chamber intraocular lens (PCIOL) of +13.00 D was then fixed transscleral using ab externo technique (Fig. 2B). BCVA at 5th month of follow up was 20/60 with a well positioned IOL and no secondary problems. 1367-0484/$ – see front matter © 2011 British Contact Lens Association. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.clae.2011.12.001
-
Upload
ruchi-goel -
Category
Documents
-
view
217 -
download
2
Transcript of Manual small incision cataract surgery for subluxated cataract with lens coloboma
C
Mc
RMG
a
KSLM
1
tdsdisaiPahbaosi
l
1d
Contact Lens & Anterior Eye 35 (2012) 89– 91
Contents lists available at SciVerse ScienceDirect
Contact Lens & Anterior Eye
jou rn al h om epa ge: www.elsev ier .com/ locate /c lae
ase report
anual small incision cataract surgery for subluxated cataract with lensoloboma
uchi Goel, Saurabh Kamal ∗,1, Bhawna Khurana, Sushil Kumar, K.P.S. Malik, Sonam Angmo Bodh,alvika Singh
uru Nanak Eye Centre, New Delhi, India
r t i c l e i n f o
eywords:ubluxated cataractens colobomaanual small incision cataract surgery
a b s t r a c t
Introduction: The lens coloboma results from a segmental defective or absent development of the zonules.It is usually unilateral and bilateral cases are rare. These eyes are at greater risk of complications duringcataract surgery due to ocular malformations. In addition the capsular bag requires stabilization usingmodified capsule tension ring, capsular tension segment or capsular anchor.Methods: Lens extraction is indicated for cataract or subluxation if visual function is sufficiently compro-mised. We report our surgical experience in a patient with bilateral isolated lens coloboma by performingmanual small incision cataract surgery (MSICS) in left eye and phacoemulsification in right eye.
Results: The nuclear rotation was hampered because of the lack of zonules and presence of lens coloboma.MSICS was converted to the intracapsular technique in left eye, though breaking the nucleus into piecesduring phacoemulsification in right eye enabled its mobilization and successful completion with implan-tation of modified capsule tension ring.Conclusions: A patient with lens subluxation and lens coloboma is better managed by phacoemulsificationS. Britis
as compared to the MSIC© 2011
. Introduction
Lens coloboma represents incomplete formation of the lens dueo failure of fetal fissure to close completely. Segmentally defectiveevelopment or absence of zonules results in a coloboma of the lensecondary to flattening of the equator in the region of the zonularefect [1]. Coloboma of the lens is typically unilateral and located
nferiorly; and if bilateral it is seen to be symmetrical [2]. Cataract isaid to occur at an earlier age than normal in such cases and it maybe
posterior subcapsular variant or a dense nuclear cataract. Lax-ty of capsule and zonules makes the cataract surgery challenging.lacement of intraocular implant poses problems of stabilizationnd centration. The manual small incision cataract surgery (MSICS)as become popular in India although phacoemulsification givesetter unaided visual acuity [3], but has been found to be effectivend economical [4,5] requiring less capital investment. We describeur surgical experience in the management of a case with bilateral
ubluxated cataract with symmetrical lens coloboma using MSICSn one eye and phacoemulsification in the other eye.∗ Corresponding author at: Guru Nanak Eye Centre, Maulana Azad Medical Col-ege, New Delhi, India. Tel.: +91 9953715616.
E-mail address: [email protected] (S. Kamal).1 361, Sector – 30, Faridabad, Haryana 121008, India.
367-0484/$ – see front matter © 2011 British Contact Lens Association. Published by Elsoi:10.1016/j.clae.2011.12.001
h Contact Lens Association. Published by Elsevier Ltd. All rights reserved.
2. Case report
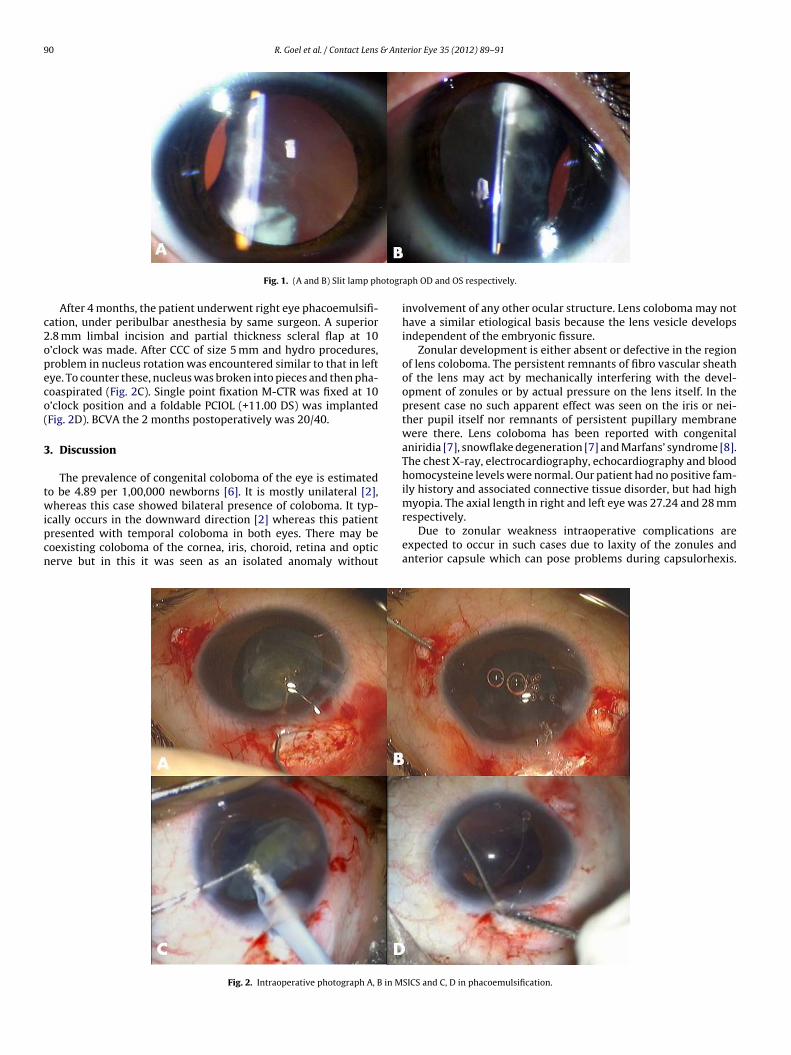
37 year old male presented to the out-patient department withcomplain of gradual deterioration of vision in both eyes. Best cor-rected visual acuity (BCVA) was 20/400 OD and 20/200 OS, witha manifest refraction of −12.00 DS both eyes. Intraocular pressurewas 12 and 14 mm Hg in OD and OS respectively. On examination,the patient had bilateral visually significant cataract with kidneyshaped lens coloboma and absent zonules on the temporal sideextending from 8 o’clock to 11 o’clock and 2 o’clock to 5 o’clockin OD and OS respectively. There was bilateral temporal 180◦ sub-luxation (Fig. 1A and B). Gonioscopy revealed bilateral open angles.There was no uveal or retinochoroidal coloboma. Posterior segmentshowed tessellated fundus and posterior vitreous detachment.
The patient was posted for left eye MSICS under peribulbar anes-thesia. Sclerocorneal tunnel was dissected superiorly and scleralflap was dissected at 4 o’clock for fixation of modified capsular ten-sion ring (M-CTR). Following continuous curvilinear capsulorrhexis(CCC) of size 5 mm and complete hydro procedures, nucleus failedto rotate (Fig. 2A). Finally the entire nucleus was removed usingirrigating vectis due to inability to prolapse it out of the bag. Afteranterior vitrectomy, another scleral flap was dissected at 10 o’clock.
A posterior chamber intraocular lens (PCIOL) of +13.00 D was thenfixed transscleral using ab externo technique (Fig. 2B). BCVA at 5thmonth of follow up was 20/60 with a well positioned IOL and nosecondary problems.evier Ltd. All rights reserved.
90 R. Goel et al. / Contact Lens & Anterior Eye 35 (2012) 89– 91
otogr
c2opeco(
3
twipcn
Fig. 1. (A and B) Slit lamp ph
After 4 months, the patient underwent right eye phacoemulsifi-ation, under peribulbar anesthesia by same surgeon. A superior.8 mm limbal incision and partial thickness scleral flap at 10’clock was made. After CCC of size 5 mm and hydro procedures,roblem in nucleus rotation was encountered similar to that in leftye. To counter these, nucleus was broken into pieces and then pha-oaspirated (Fig. 2C). Single point fixation M-CTR was fixed at 10’clock position and a foldable PCIOL (+11.00 DS) was implantedFig. 2D). BCVA the 2 months postoperatively was 20/40.
. Discussion
The prevalence of congenital coloboma of the eye is estimatedo be 4.89 per 1,00,000 newborns [6]. It is mostly unilateral [2],hereas this case showed bilateral presence of coloboma. It typ-
cally occurs in the downward direction [2] whereas this patientresented with temporal coloboma in both eyes. There may beoexisting coloboma of the cornea, iris, choroid, retina and opticerve but in this it was seen as an isolated anomaly without
Fig. 2. Intraoperative photograph A, B in M
aph OD and OS respectively.
involvement of any other ocular structure. Lens coloboma may nothave a similar etiological basis because the lens vesicle developsindependent of the embryonic fissure.
Zonular development is either absent or defective in the regionof lens coloboma. The persistent remnants of fibro vascular sheathof the lens may act by mechanically interfering with the devel-opment of zonules or by actual pressure on the lens itself. In thepresent case no such apparent effect was seen on the iris or nei-ther pupil itself nor remnants of persistent pupillary membranewere there. Lens coloboma has been reported with congenitalaniridia [7], snowflake degeneration [7] and Marfans’ syndrome [8].The chest X-ray, electrocardiography, echocardiography and bloodhomocysteine levels were normal. Our patient had no positive fam-ily history and associated connective tissue disorder, but had highmyopia. The axial length in right and left eye was 27.24 and 28 mm
respectively.Due to zonular weakness intraoperative complications areexpected to occur in such cases due to laxity of the zonules andanterior capsule which can pose problems during capsulorhexis.
SICS and C, D in phacoemulsification.

& Ant
VclBm
iaaloptodfpi
lotM
R. Goel et al. / Contact Lens
itreous loss may occur secondary to prolapse through theoloboma in the presence of an intact capsule. There may be prob-ems associated with IOL stability and centration. PostoperativelyCVA might be reduced due to amblyogenic affect of irregular astig-atism caused by the asymmetrical lens.Surgical management of severe subluxation is challenging in
tself. MSICS is commonly practiced in developing world. It requires large size CCC, preferably 6 mm or more, which is difficult tochieve in subluxated cases. Once the CCC is complete, the capsu-ar bag can be stabilized using a M-CTR, capsular tension segmentr capsular anchor [9]. The nuclear rotation within the bag is arerequisite for both phacoemulsification and MSICS. The rota-ion was hampered because of the lack of zonules and presencef lens coloboma [10]. Though breaking the nucleus into piecesuring phacoemulsification enabled its mobilization and success-ul completion, it was not possible to rotate a complete nucleus androlapse it out of the bag in MSICS, which had to be converted to
ntracapsular cataract extraction.In our experience, due to the difficulty in achieving a large capsu-
orrhexis size, rotation of an intact nucleus and thereby its prolapseut of the bag, a patient with lens coloboma and severe subluxa-ion is better managed by phacoemulsification in comparison to
SICS.
[
erior Eye 35 (2012) 89– 91 91
References
[1] Amari F, Segawa K, Ando F. Lens coloboma and Alport like glomerulonephritis.Eur J Ophthalmol 1994;4:181–3.
[2] Aggarwal A, El-Bash AR, Inker S, Musarella MA. Symmetrical bilateral lenscolobomas in two brothers. J Paediatr Ophthalmol Strabismus 2004;41:302–4.
[3] Gogate PM, Kulkarni SR, Krishnaiah S, Deshpande RD, Joshi SA, PalimkarA, et al. Safety and efficacy of phacoemulsification compared with manualsmall-incision cataract surgery by a randomized controlled clinical trial. Oph-thalmology 2005;112:869–74.
[4] Gogate PM, Deshpande M, Wormald RP, Deshpande R, Kulkarni SR. Extracap-sular cataract surgery compared with manual small incision cataract surgeryin community eye care setting in Western India: a randomised controlled trial.Br J Ophthalmol 2003;87:667–72.
[5] Gogate PM, Deshpande M, Wormald RP. Is manual small incision cataractsurgery affordable in the developing countries? A cost comparison with extra-capsular cataract extraction. Br J Ophthalmol 2003;87:843–6.
[6] Bermejo F, Martinez-Frias ML. Congenital eye malformations:clinical–epidemiological analysis of 1,124,654 consecutive births in Spain. AmJ Med Genet 1998;75:497–504.
[7] Doganay S, Emre S, Firat P. Bilateral aniridia lenticular coloboma and snowflakedegeneration. Ophthalmic Surg Lasers Imaging 2009;40:54–6.
[8] Mehrotra AS, Solanki N, Sabharwal KK. Bilateral coloboma of lens in Marfan’ssyndrome. Indian J Ophthalmol 1985;33:201–2.
[9] Assia EI, Ton Y, Michaeli A. Capsule anchor to manage subluxated lenses: initialclinical experience. J Cataract Refract Surg 2009;35:1372–9.
10] Mizuno H, Yamada J, Nishiura M, Takahashi H, Hino Y, Miyatani H. Capsulartension ring use in a patient with congenital coloboma of the lens. J CataractRefract Surg 2004;30:503–6.