
Preventive Controls for Human Foods & Preventive Controls ...
Naval Medical Command
DC 20372-5120
NAVMED P-5010-3(1988)0510-LP-2O2-87OO
Manual Of Naval Preventive Medicine
Chapter 3
VENTILATION ANDTHERMAL STRESS
ASHORE AND AFLOAT
DISTRIBUTION STATEMENT “A”

CONTENTS
Section I.
Section II.
Section III.
Section IV.
Page
Definitions and Instrumentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-1
Article 3-1. Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-13-2. Definitions and Instrumentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3- I
Design Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-4
Article 3-3. Objectives of Heating, Ventilation and Cooling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-53-4. Heating . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-53-5. Ventilation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-53-6. Mechanical Cooling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-63-7. Additional Considerations Aboard Ship . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-63-8. General Considerations Ashore . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-9
Physiological Principles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-9Article 3-9. Effects of Heat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-9
3-10. Effects of Cold . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-17
Thermal Standards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-20Article 3-11.
3-12.3-13.3-14.
IllustrationsTable 3-1.
3-2.
3-3.
3-4.3-5.3-6.3-7.3-8.
3-9.
3-10.3-11.
3-12.
3-13.
Figure 3-1.3-2.3-3.3-4.3-5.3-6.
General Requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-20Assessment of Heat Stress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-22Practical Heat Stress Standards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-28Practical Cold Stress Standards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-33
Summary of Thermal Physiology Heat Stress Design Conditions forSurface Vessels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-8
Recommended Threshold WBGT Values For Instituting SoundHot Weather Practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-9
Percent Optimum Heat Acclimatization on Consecutive Days ofHeat-Work Exposures for Physically Trained Personnel . . . . . . . . . . . . . . . . . . . . . . . . . 3-10
General Physiologic Impact of Fuel Combustion Gases and Fuel Vapors . . . . . 3-21Approximation of Metabolic Rates for Various General Physical Activities . . . 3-24Physiologic and Hygienic Implications of the Belding-Hatch HSI . . . . . . . . . . . . . . 3-25Time-Weighted-Mean Metabolic Rates for PHEL Curves I - IV . . . . . . . . . . . . . . . . 3-27Relationship of PHEL Curves I - VI to Intermittent Physical Work
and Rest Pauses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-27WBGT as a Guide in Regulating Intensity of Physical Exertion
During First 12 Training Weeks in Hot Weather . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-29PHEL Curve General Applicability Aboard Ships . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-30PHEL Times for PHEL Curves I -VI versus WBGT Without Presence
of FuelCombustion Gases and/or Fuel Vapors [80- 125 F] . . . . . . . . . . . . . . . . . . 3-31PHEL Times for PHEL Curves I - VI versus WBGT Index With Presence
of CombustionGases and/or Fuel Vapors [80- l15 F] . . . . . . . . . . . . . . . . . . . . . . . . . 3-32Cooling Power of Wind unexposed Flesh Expressed as
an Equivalent Temperature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-33Psychrometric Chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-3Percent Optimum Cooling vs. Air Velocity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-7Heat Acclimatization [Comparison of Methods] . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-10aPathogenesis of Complications of Excessive Physical Exercise . . . . . . . . . . . . . . . . . . . 3-12Water Requirements For Heat, Work & 15.0 Gms NaCl . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-16Water Requirements For Heat, Work & 25.5 Gms NaCl . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-16
i

Page3-7. Estimation of Mean Radiant Temperature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-223-8. Body Temperatures vs. Mean Radiant Temperature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-233-9. Physiological Heat Exposure Limits Chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-263-10. Mental Impairment Onset Vs. WBGT Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-283-11. Lethal Hypothermia Exposures in Water . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-34

VENTILATION AND THERMALSTRESS ASHORE AND AFLOAT
Chapter 3
Section I. DEFINITIONS AND INSTRUMENTATION
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ..Purpose 3-1Definitions and Instrumentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3-2
3-1. Purpose(1) The purpose of this chapter is to provide informa-
tion on the fundamentals of heating, ventilating andcooling, and to describe the physical and physiologicalmeasurements which must be made ashore and afloat inorder to assess the effects of hot and cold atmosphericconditions on personnel.
(2) Engineering aspects which relate to heating, ven-tilation and cooling design in shipboard situations comeunder the cognizance of the Naval Sea Systems Com-mand; those applying to shore establishments are han-dled by the Naval Facilities Engineering Command.Health standards governing these installations are pro-mulgated by the Naval Medical Command. In order toprotect the health and well-being of all personnel, it isimportant to be familiar with the fundamental principlesinvolved in heating, ventilation and air-conditioning asthey apply to the human.
3-2. Definitions and Instrumentation(1) Stress and Strain
(a) The thermal (heat or cold) stress of any givenworking situation is the combination of all of thosefactors which result in heat gains or losses relative to thebody or which prevent the body’s regulatory mecha-nisms from working efficiently. Thus, it is necessary toconsider the combined impact of climatic and non-climatic factors and to evaluate independent and inte-grated influences associated with the human.
(b) In accordance with engineering practices, envi-ronmental physiologists employ the term “stress” todesignate the force or load acting upon the biologicalsystem and the term “strain” to designate the resultingdistortion of the biological system. Thermal stress fac-tors are conventionally given as heat, cold, humidity,radiation, air movement and surface temperatures; ther-mal strain manifests itself in specific cardiovascular,thermoregulatory, respiratory, renal, endocrine, etc.,responses which differ from accepted human norms.
(c) It must be understood that not all thermal stressand strain are adverse to humans. Within the range ofhuman adaptability, factors that do not impair perfor-mance or increase susceptibility to other risks may beconsidered “acceptable” until proven otherwise. Due to
the fine line between acceptable and unacceptable levelsof heat stress and strain, extreme caution must beexercised to avoid cumulative harm to individuals.
(d) Thermal stress has been categorized as:(1) “Acceptable” when the human is able to
compensate without undue strain; or,(2) “Unacceptable” when the human is able to
compensate but incurs severe strain, or is unable tocompensate and incurs excessive strain.
(e) Thermal strains have been categorized as:(1) Those interfering with work performance and
safety; and,(2) Those with more overt manifestations of
physiologic decomposition such as heat rash, heatcramps, heat exhaustion, heat stroke, non-freezing orfreezing injuries.
(2) Climatic Measurements of Thermal Stress:(a) Dry-Bulb Temperature (DB) of air is that tem-
perature measured with an ordinary alcohol-in-glass, ormercury-in-glass, thermometer whose bulb is kept dryand shielded from radiation. When laypersons speak ofthe prevailing air temperature, determined from a con-ventional thermometer, they are speaking of the dry-bulb temperature. A variety of electronic sensors can beused in place of conventional thermometers; if properlyconstructed some of these (e.g., thermocouples andthermistors) may require comparatively little shieldingfrom radiant heat transfer. For routine monitoring ofdry-bulb temperatures in shipboard spaces, the NavalSea Systems Command approved alcohol-in-glassdry-bulb thermometer has the stock number9G-6685-00-243-9964.
(b) Wet-Bulb Temperature (WB) is measured with athermometer, similar to that used for dry-bulb temper-ature, except that a wet wick is fitted closely over thebulb (or sensor). A “natural” wet-bulb temperature isdefined as that obtained with no additional movementof air over the wick than that which occurs naturally inthe environment. An “aspirated” wet-bulb temperatureis obtained by increasing air movement over the wickwith a fan, motorized psychrometer, or sling psychrom-eter. The “true” wet-bulb environmental temperature isapproximated with an air flow of at least 250 feet perminute (fpm) over the wick and the bulb is shielded from
3-1

3-2 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-2
radiant heat. Excessive air velocity (e. g., greater than1500 fpm) may result in a significant degree of kineticheating. Although the natural wet-bulb temperaturedepends on the dry-bulb temperature and the moisturecontent of the air, it does not provide a direct indicationof the amount of water vapor in the air. The aspiratedwet-bulb temperature is therefore of greater value inplanning corrective engineering actions than the “nat-ural” wet-bulb temperature, and the term wet-bulb willhereafter refer to that which is aspirated unless otherwisespecified.
When the wet- and dry-bulb temperatures areidentical the air is said to be “saturated;" and the relativehumidity may be considered to be 100 percent. Anydecrease in the moisture content of the air will result inevaporation from the wetted wick of the wet-bulb ther-mometer, and in turn, the bulb of the thermometer willbe cooled to a temperature which reflects the reducedmoisture content of the air.
(c) Measurements of Humidity. Humidity is anexpression of the quantity of water vapor mixed with theother atmospheric gases. The Absolute Humidity (AH)is the mass of water vapor present per unit volume of air(kg/m’); the gas pressure (Torr) exerted by this watervapor is referred to as the Vapor Pressure (e or VP). Theratio of the actual amount of water in the air (absolutehumidity) to the maximum quantity of water that the aircan hold at a given temperature is the Relative Humidity(RH). The temperature at which the absolute humidityreaches a maximum and the air become saturated withwater vapor is called the Dew Point (Td).
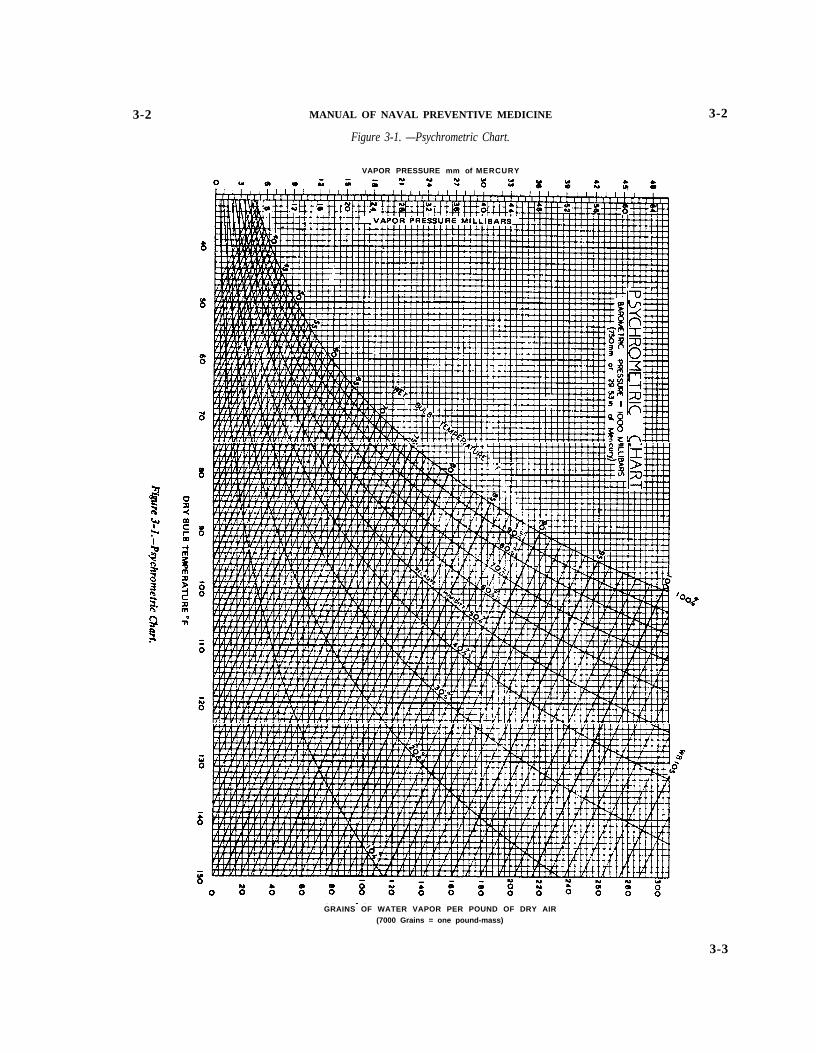
Vapor pressure is a measure of water content inthe atmosphere under given conditions. Relative humid-ity is primarily a ratio of partial and saturated vaporpressures, not a measure of water content. For example,one may find a 50 percent relative humidity at 50 F DBand 100 F DB, but the actual water content at 100 F DBwill be nearly six-fold greater than that at 50 F DB (SeeFigure 3-1). Therefore, the proper evaluation of thermalconditions requires specifying both dry- and wet-bulbtemperatures.
(d) Psychrometer—an instrument for measuringatmospheric humidity utilizing a dry- and wet-bulbthermometer and whirled manually or by motorized unitto provide the moderate air flow necessary to obtain anaspirated wet-bulb temperature reading. Psychometriccharts (Figure 3-1) help translate this information intorelative humidity and other thermodynamic characteris-tics of moist air. It is strongly recommended thatmotorized psychrometer be used for reproducibility ofmeasurements; in turn, the stock number for the ap-proved unit is 1H-6685-00-935-1389, calibration is notrequired. Electronic, motorized psychrometer are avail-able to provide direct readout of DB, WB, RH and Td.
(e) Air Movement or Velocity (V) is usually ex-pressed in feet per minute (fpm) or cubic feet per minute(cfm). It is measured by various instruments dependingupon the velocities of air movement. Low velocities(down to 10 fpm) require a heated Kata thermometer orthermo-anemometer (“hot-wire” anemometer or equiv-
3-2
alent); high unidirectional air velocities may be mea-sured with a velometer or vane anemometer.
(f) Radiant Heat is the transfer of thermal energy bywave motion from one object to another without warm-ing of the intervening space. The wave lengths involvedrange from the visible portion of the electromagneticspectrum (0.3-0.7 microns) to the longer radio waves. Inindustrial situations any part of the heat radiationspectrum may be present. Natural environments, how-ever, generally include two bands: solar radiation fromultra-violet to near infrared, and heat radiation in the farinfrared portion of the spectrum. For recall it is easier toremember that solar radiation is a shorter wavelengthand heat radiation (e.g., indoors) is a longer wavelength.Both forms of radiation liberate thermal energy whenabsorbed.
Not all of the radiant heat that strikes a surface isabsorbed. Any surface which has a high reflectance willminimize absorption of radiant heat; conversely, a sur-face with low reflectance will increase absorption ofradiant heat. The portion that is absorbed is termed“absorptance of the surface” while that which is notabsorbed is reflected by the “reflectance of a surface”.An exception exists for humans in that dark-pigmentedskin and light-colored skin are essentially alike in ab-sorbing the longer wavelength radiant heat (e. g.,indoors); however, in the sunlight darker skin has ahigher absorptance than lighter skin. The intensity ofradiant heat can be measured by use of a radiometer orpyrheliometer, or a globe thermometer.
(g) Globe Thermometer (G). The Vernon GlobeThermometer consists of a 6-inch hollow copper sphere,with a 0.022 inch thick wall, painted matte (flat) blackon the outside, and contains a temperature sensor likethat of an unshielded dry-bulb thermometer with itsbulb, or an equivalent, at the center of the sphere. AVernon globe requires about 20 minutes to achieveequilibrium. Smaller globes, from 1.64-4.0 inch outsidediameter, have been developed which have shorted equi-librium times; however, few have been demonstrated tobe equivalent with a Vernon Globe. Globe thermometersare required in the assessment of thermal stress becausethey integrate radiant heat exchange and convective heatloss into a single value.
(h) Wet-Bulb GIobe Temperature (WBGT) Meter,also known as the Heat Stress Meter, is a compactelectronic instrument that independently measures thedry-bulb, wet-bulb and globe temperatures. The instru-ment displays each of these values as well as computesand displays the WBGT Index value (described in Sec-tion IV). The approved Navy Heat Stress Meter(7G-6685-01-055-5298) is lightweight, self-contained,and equipped with a rechargeable power supply. A ven-tilating fan is included, in the shielded dry- and wet-bulbsensor assembly, to obtain aspirated wet-bulb tempera-tures. The entire unit can be adapted for remote moni-toring and recording. Use and maintenance of theNavy’s Heat Stress Meter is described and portrayed inthe Navy educational film “Care and Use of the HeatStress Meter” (35335-DN). Use of other electronic and
3-2 MANUAL OF NAVAL PREVENTIVE MEDICINE
Figure 3-1. —Psychrometric Chart.
VAPOR PRESSURE mm of MERCURY
3-2
GRAINS OF WATER VAPOR PER POUND OF DRY AIR(7000 Grains = one pound-mass)
3-3

3-2 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-3
manual heat stress monitoring devices, other than amotorized psychrometer, are not approved for shipboardpurposes unless the proposed devices meet the accuracyand response time test accuracy tolerances given in TableIII and Figure 3 of Navy Procurement Specification0513487126-SGA of 20 May 1987. No manual “heatstress monitors," which supposedly provide dry- andwet-bulb and globe temperatures and/or a so-calledfacsimile of the WBGT Index, are approved for ship-board uses due to inherent measurement errors over thewide range of thermal environments that exist through-out Navy ships. Special heat stress survey teams, fromshore activities, should employ the most reliable, accu-rate equipments available. Inquiries regarding approvalfor shipboard use and for comparative purposes shouldbe brought to the attention of MED-22. Naval MedicalCommand approval for shipboard uses can only beconsidered after receiving and evaluating a diversity ofcomparative data for each type of proposed alternativeheat stress monitoring device.
Stock numbers for the Navy approved WBGTMeter, accessories kit, globe assemblies alone and re-chargeable batteries, as of May 1988, are:
(a) WBGT Meter 7G-6685-01-055-5298(Shipboard AEL 2-870003051)
(b) Accessories (spare sensor/wind tunnel as-sembly, globe, wicks, etc.) 9G-6685-01 -055-5299 (Shipboard APL 100110001)
(c) Globe Assemblies 9G-6665-01-149-8635(d) Standard Nickel-Cadmium Rechargeable
AA Batteries 9G-6140-00-449-6001(i) The Infrared Thermometer (self-contained elec-
tronic) is used to measure the temperature of infraredenergy emitted from various sources. The practicalaspects of an infrared thermometer are that no contactwith surfaces is required. In industrial settings, a light-
weight, hand-held infrared thermometer allows scanningof surfaces to detect the functional adequacy of insula-tion, as well as to check overheating of equipments.Analog and digital readout and imaging devices arecommercially available. In all applications, extremecaution should be exercised in using infrared thermom-eters. A number of such devices require the instrumentto be four feet or more from the infrared sources toavoid infrared “flare”. Electromagnetic radiation“flare” will result in erratic values, leading to misinter-pretations of the data.
(j) Effective Temperature (ET) is an empirical sen-sory index, combining into a single value the effects oftemperature, humidity, air velocity and thermal radia-tion. Combinations of conditions which produce thesame subjective feeling of warmth in reference to still airare assigned the same effective temperature.
(k) Equivalent Temperature is commonly known as“Wind Chill”. As noted by Burton in 1955, “WindChill” lacks a scientific basis. The product of calculat-ing “Wind Chill” is a heat transfer factor, and therelationship of temperature and air movement providethe derived heat transfer. The temperature—air move-ment relationship is known as the Equivalent Tempera-ture. (See Article 3-14)
(1) The Mean Radiant Temperature (mrt) of anonuniform environment (e.g., walls, overhead, deckand objects of different emissivities and at differenttemperatures) is defined as the temperature of a uniformblack enclosure in which a solid body or an occupantwould exchange the same amount of radiant heat as inthe given nonuniform environment. It is estimated fromdry-bulb and globe temperatures and air movement andis useful in determining radiative heat transfer (net gainor loss) relative to humans. Section IV provides furtherinformation on mean radiant temperature.
Section II. DESIGN OBJECTIVES
ArticleObjectives of Heating, Ventilation and Cooling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-3Heating . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-4Ventilation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...3-5Mechanical Cooling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-6Additional Considerations Aboard Ship . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-7General Considerations Ashore . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-8
3-3. Objectives of Heating, Ventilation andCooling
(1) Major objectives of heating, ventilation and cool-ing include maintaining physical fitness, mental alert-ness, fighting ability and the general well-being ofpersonnel in the performance of their duties ashore orafloat. This should include consideration for the stressesof watches, prolonged cruising and battle or generalquarters situations. The design and maintenance ofenvironmental control systems should assure useful pro-
ductivity and recovery from undue physical stress ratherthan thermal comfort alone.
(2) In addition to temperature considerations, envi-ronmental control systems must assure that the air inconfined spaces contains sufficient quantities of oxygenand no harmful components.
(3) Special use areas such as selected Medical Depart-ment spaces, and those containing equipment and ma-terials which require individually controlled surround-ings, must be designed to guarantee optimal missionperformance under variable environmental conditions.
3-4
3-2 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-3
manual heat stress monitoring devices, other than amotorized psychrometer, are not approved for shipboardpurposes unless the proposed devices meet the accuracyand response time test accuracy tolerances given in TableIII and Figure 3 of Navy Procurement Specification0513487126-SGA of 20 May 1987. No manual “heatstress monitors," which supposedly provide dry- andwet-bulb and globe temperatures and/or a so-calledfacsimile of the WBGT Index, are approved for ship-board uses due to inherent measurement errors over thewide range of thermal environments that exist through-out Navy ships. Special heat stress survey teams, fromshore activities, should employ the most reliable, accu-rate equipments available. Inquiries regarding approvalfor shipboard use and for comparative purposes shouldbe brought to the attention of MED-22. Naval MedicalCommand approval for shipboard uses can only beconsidered after receiving and evaluating a diversity ofcomparative data for each type of proposed alternativeheat stress monitoring device.
Stock numbers for the Navy approved WBGTMeter, accessories kit, globe assemblies alone and re-chargeable batteries, as of May 1988, are:
(a) WBGT Meter 7G-6685-01-055-5298(Shipboard AEL 2-870003051)
(b) Accessories (spare sensor/wind tunnel as-sembly, globe, wicks, etc.) 9G-6685-01 -055-5299 (Shipboard APL 100110001)
(c) Globe Assemblies 9G-6665-01-149-8635(d) Standard Nickel-Cadmium Rechargeable
AA Batteries 9G-6140-00-449-6001(i) The Infrared Thermometer (self-contained elec-
tronic) is used to measure the temperature of infraredenergy emitted from various sources. The practicalaspects of an infrared thermometer are that no contactwith surfaces is required. In industrial settings, a light-
weight, hand-held infrared thermometer allows scanningof surfaces to detect the functional adequacy of insula-tion, as well as to check overheating of equipments.Analog and digital readout and imaging devices arecommercially available. In all applications, extremecaution should be exercised in using infrared thermom-eters. A number of such devices require the instrumentto be four feet or more from the infrared sources toavoid infrared “flare”. Electromagnetic radiation“flare” will result in erratic values, leading to misinter-pretations of the data.
(j) Effective Temperature (ET) is an empirical sen-sory index, combining into a single value the effects oftemperature, humidity, air velocity and thermal radia-tion. Combinations of conditions which produce thesame subjective feeling of warmth in reference to still airare assigned the same effective temperature.
(k) Equivalent Temperature is commonly known as“Wind Chill”. As noted by Burton in 1955, “WindChill” lacks a scientific basis. The product of calculat-ing “Wind Chill” is a heat transfer factor, and therelationship of temperature and air movement providethe derived heat transfer. The temperature—air move-ment relationship is known as the Equivalent Tempera-ture. (See Article 3-14)
(1) The Mean Radiant Temperature (mrt) of anonuniform environment (e.g., walls, overhead, deckand objects of different emissivities and at differenttemperatures) is defined as the temperature of a uniformblack enclosure in which a solid body or an occupantwould exchange the same amount of radiant heat as inthe given nonuniform environment. It is estimated fromdry-bulb and globe temperatures and air movement andis useful in determining radiative heat transfer (net gainor loss) relative to humans. Section IV provides furtherinformation on mean radiant temperature.
Section II. DESIGN OBJECTIVES
ArticleObjectives of Heating, Ventilation and Cooling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-3Heating . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-4Ventilation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...3-5Mechanical Cooling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-6Additional Considerations Aboard Ship . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-7General Considerations Ashore . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-8
3-3. Objectives of Heating, Ventilation andCooling
(1) Major objectives of heating, ventilation and cool-ing include maintaining physical fitness, mental alert-ness, fighting ability and the general well-being ofpersonnel in the performance of their duties ashore orafloat. This should include consideration for the stressesof watches, prolonged cruising and battle or generalquarters situations. The design and maintenance ofenvironmental control systems should assure useful pro-
ductivity and recovery from undue physical stress ratherthan thermal comfort alone.
(2) In addition to temperature considerations, envi-ronmental control systems must assure that the air inconfined spaces contains sufficient quantities of oxygenand no harmful components.
(3) Special use areas such as selected Medical Depart-ment spaces, and those containing equipment and ma-terials which require individually controlled surround-ings, must be designed to guarantee optimal missionperformance under variable environmental conditions.
3-4

3-3 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-5
Designs must address exhaust of gases and vapors whichare heavier than air, therefore, in both shipboard andashore applications, exhaust ventilation is required nineinches from the deck. Furthermore, just because thedesign supply air volumes and exhaust volumes meetdesign specification, optimal distribution within thespace or the work site must be assured.
3-4. Heating(1) In designing a heating system ashore, the relatively
narrow range of climatic conditions in a given locale canusually be anticipated and the system designed accord-ingly. This sort of planning is obviously difficult fornaval vessels on which heating systems must be designedto provide for a wide range of climatic conditions fromarctic cold in winter to tropical heat in summer. Theneed for design flexibility is further extended by variablerequirements for space, weight and power sources. Inaddition, the distance of the heating (or cooling) unitfrom the point of delivery must be considered. Forgeneral purposes in cold weather, the amount of heatsupplied should be planned to balance heat loss whenthe outside air temperature is 10 F DB and the sea watertemperature is 28 F, the air temperature at normal workstations should be sustained at least to 65 F.
(2) Aboard ship the conventional approach for heat-ing is accomplished by drawing fresh outside air overheating coils and discharging the heated air into variouscompartments where it is required. In order to avoidcondensation of moisture on and inside the air ducts andto provide a flexible heating system, outside air isinitially preheated to 42-50 F DB. The air is then heatedto the desired delivery zone temperature and distributedto the various compartments and spaces within thatzone. A “heating zone” is defined as a group of adja-cent spaces with approximately the same heatingrequirements.
(3) A zone temperature of 70 F DB is required aboardsurface vessels for berthing, dressing, lounge, messing,medical, dental, office and control spaces. No effort ismade to maintain a controlled moisture level in thesespaces during cold weather; therefore, Medical Depart-ment personnel should anticipate increased symptomsassociated with the drying of respiratory membranesamong individuals working in these areas.
(4) Heating designs for submarines differ from thoseof surface vessels in that they provide a regulatedhumidity for the living and control spaces noted above.Symptoms associated with the drying of the respiratorymembranes may be less pronounced than those notedaboard surface vessels. The heating design for subma-rine berthing, dressing, lounge, messing, medical, den-tal, office and control spaces should adhere to thefollowing specifications: dry-bulb 79 F, wet-bulb 59 F,relative humidity 50% and WBGT Index 63 F.
(5) With the exception of the above noted living andcontrol spaces and areas containing engineering propul-sion components, inside working spaces should be main-tained at approximately the given temperatures for pur-poses of efficiency and comfort of personnel. In those
cases where atmospheric heating and cooling needs ofthe individual cannot be met there is the added problemof adding or removing protective clothing; all normallyworn clothing must be viewed as protective in naturewhen considering the potential hazards aboard ships andashore.
3-5. Ventilation(1) The purpose of ventilation is to remove toxic
substances, offensive odors and excessive heat and mois-ture, and to provide an adequate oxygen supply. Navalventilation should be designed not only to preventconditions aboard ship which could lead to acute over-heating, but also to maintain an atmosphere conduciveto the physical and mental efficiency of personnel.Ventilation of work spaces must be adequate to controltoxic substances such as; solvents (e.g., perchloroethy-lene in dry cleaning plants, PD-680 Type II as adegreaser, etc.), fuel combustion gases (e.g., “stack gas”in firerooms), fuel vapors (e.g., fuel pump rooms,firerooms, auxiliary machinery rooms), hydrogen sul-fide in CHT pump rooms, etc. Ships with conventionalventilation system shall have the capability to electri-cally secure ventilation to prevent ingestion or spread ofNBC contamination within the ships. In 1983 Navypolicy was established that the Circle William materialcondition must not be set for longer than 5 minutes inmachinery spaces during training evolutions. The venti-lation systems in ships with Collective Protection Sys-tems (CPS) shall provide clean, filtered air within theCPS zones.
Ventilation systems must be as flexible as thosedesigned for heating. Hot weather cooling of givenspaces by ventilation should be planned so that thetemperature within those spaces will remain below spec-ified limits. These limits are determined, using as a basethe highest anticipated hot weather (outside) tempera-tures. For general planning purposes the design weatherconditions are 90 F DB, 81 F WB and 85 F sea watertemperature. Special considerations must be made forexternal ambient environmental conditions in the Per-sian Gulf; these design weather conditions are: 105 FDB, 95 F WB and up to 90 F sea water temperature.
(2) Air circulation within manned compartments mustbe sufficient to eliminate “dead spaces”. An adequateair exchange will insure the removal of odors and willprevent the accumulation of moisture on surfaces of thespaces. Ventilation exhaust from sanitary spaces, foodpreparation and dining areas, sculleries and garbagedisposal areas must not be recirculated or introducedinto any other spaces. Ventilation of food preparation,laundry, dry cleaning and propulsion spaces must bebalanced to provide a negative pressure within thoseareas, i.e., allowing for a net flow of air into the spaces.Propulsion spaces should have exhaust at 115070 ofsupply air in 600 pound per square inch (psi), gasturbine and diesel propulsion plants and aircraft carriermachinery spaces; exhaust 125% of supply in all other1200 psi propulsion plants.
(3) Cooling by ventilation is a process of diluting
3-5

3-5 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-7
inside air with cooler outside air. It has proved to be ofvalue aboard ships in reducing excessive temperatures inmanned spaces. In those cases where steam and waterleaks are minimal, negative pressure ventilation maypartially offset the adverse impact of high temperaturesupon personnel. However, as the ventilation systems ofships deteriorate it is unlikely that ventilation alone willcompensate for the increased environmental heat uponpersonnel. To achieve optimal exhaust ventilation inmachinery spaces the size of the screens over the exhaustuptake ducts should be 1½ inch grid mesh, and theventilation systems must be maintained at optimal ca-pability. In other spaces within a ship the exhaust uptakeducts of nine inches or less across should have ½ inchgrid mesh; if the exhaust uptake ducts are greater thannine inches across the screening must be 1½ inch gridmesh. It should be evident that usually it will not bepossible to cool spaces to needed temperatures by ven-tilation alone; although this is the general practice inengineering machinery spaces.
3-6. Mechanical Cooling(1) Mechanical cooling and dehumidification of air is
accomplished by passing incoming air over coils and finscooled with a suitabIe refrigerant. As the warm humidair circulates over the coils, it loses heat and the moisturecondenses on the fins. The conditioned air is thencirculated through a ducting system to appropriatespaces and compartments. Cooling coils may be locatedin an air supply duct with the refrigerating unit and fanplaced remotely, or the entire apparatus may be assem-bled into a single unit.
(2) Air-conditioning is frequently required in spacescontaining precision instruments which are sensitive toextremes of temperature and humidity. Appropriatefiltering of air will assure air purity within tolerancelimits for equipments and personnel working in thespaces.
(3) Mechanical cooling is a current feature of theliving areas and office spaces of combatant ships andmost auxiliaries. Basic medical areas are air-conditioned; this is done to improve the recovery ofpatients, which takes precedence over the customaryspace and weight limitations aboard ships.
(4) “Cold shock” may be produced when personnelpass from heated areas into air-conditioned spaces.Individuals experience a rapid loss of body heat due toan increased evaporation of sweat from wet skin anddamp clothing. Chilly sensations and shivering arecommon manifestations. A corollary is seen in personswho move into outdoor heat from excessively cooledenvironments. Personnel in this situation experiencesudden dilation of superficial blood vessels and flush-ing. “Cold shock” and its thermal counterpart may beminimized by regulating air-conditioned spaces so thatthe differential temperature between those areas andheated or outdoor environments does not exceed 15 FDB. Medical personnel should be alert to the occurrenceof these phenomena in individuals who work in thedaytime heat of natural environments or the high tem-
peratures of engine rooms, firerooms, galleys, laundries,etc. Persons entering cold rooms (e.g., walk-in freezers,cold storage boxes, cold test chambers, etc.) need pro-tection from “cold shock”; protection can be achievedby the temporary use of suitable clothing or limiting thefrequency and duration of exposures. (Also seeNAVMED P-5052-29)
3-7. Additional Considerations Aboard Ship(1) Excessive moisture may be generated in multiple
shipboard conditions. In firerooms and engine roomssteam and water leaks are common sources of increasedwater vapor. Inadequate steam exhausting from dish-washers creates a high moisture content in sculleries andin the air of passageways adjacent to sculleries. Watervapor in the air is increased by the evaporation of sweatfrom the human body. Individuals performing heavywork in a warm to hot environment may lose as much as1.5 liter (1.6 quarts) per hour in evaporated sweat. Moresedentary personnel may lose 0.2 liters (200 ml., 0.2quarts) of sweat per hour in hot spaces. Air-conditioning and dehumidification are the only effectiveways to sufficiently adjust the ambient moisture contentof living and working spaces; cooling by ventilationalone results in humidity that is always above that ofoutside air.
(2) Mechanical air supply and exhaust systems areprovided for most working and living spaces; the quan-tity for each should be balanced respectively within themajor sections of a ship. Ventilation of spaces in whichexcessive heat or undesirable odors are produced (fire-rooms, engine rooms, galleys, laundries, heads, etc.)requires a special design in order to provide a greatervolume of mechanical exhaust than supply (negativepressure); this maintains an induced air flow into thecompartment and prevents the spread of heat and odorsto adjacent spaces. Compartments used for living, ber-thing, etc., should be provided with a greater volume ofmechanical supply than exhaust (positive pressure) inorder to maintain an induced air flow out of the spaceand thus prevent the entrance of possibly contaminatedair from adjacent spaces.
(3) Ventilation and air-conditioning designs for livingcompartments, recreation spaces, mess decks (excludingserving lines), sick bay and inpatient wards, operatingrooms and intensive care spaces, administrative areas,control, and all operating electronic spaces aboardsurface vessels encountering the hot-weather outsidetemperatures of 90 F DB and 81 F WB (design limits,Article 3-5) or higher should favor conditions thatoptimize recovery from heat stress and maximize perfor-mance in hot and subtropical climates. The upperthermal design limits within the above noted spacesshould be 80 F DB, 68 F WB, 55% RH (14.3 Torr VP),with 72 F WBGT (as ET). For comparable spacesaboard submarines the design limits should be slightlylower in terms of moisture content of the air; 80 F DB,67 F WB, 50% RH, with 71 F WBGT (as ET).
(4) A preferred WBGT temperature of 78 F applies toprescribed hot-weather operational conditions in: laun-
3-6

3-7 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-7
dries, galleys, sculleries, passageways not open directlyon weather decks, and food serving lines. However, theupper thermal physiology shipboard heat stress designenvironments should not exceed that given in Table 3-1.Aboard submarines the overall demands within thevessel should preclude the environmental conditionsreaching 78 F WBGT during normal operations.
(5) Fireroom and engine room spaces require a specialapplication of the method of cooling spaces with outsideair. Frequently so much “wild heat” is produced anduncontrolled that it is neither practical nor feasible toreduce the temperatures within the entire space to thepoint of maintaining high physiological efficiency with-out unique engineering techniques. Some ships havecontrol booths in the propulsion spaces, the recirculat-ing air-conditioning units for these booths need to bedesigned to permit ready access for frequent cleaning.Outside of the control booths, and aboard those shipswithout control booths, personnel must have immediateaccess to spot cooling. Spot cooling is effected bydelivering outside air at high velocity via ventilationducts to the respective watchstander’s stations. By thismethod a “cone” of air is provided to watchstanders,even though the Effective Temperature outside the“cone” of air is very high.
Misconceptions have evolved regarding spot cool-ing, it has been widely believed: (1) that air velocities of2,000 fpm or more at a supply terminal provides optimalspot cooling; (2) that increasing the volume of air flowthrough a fireroom or engine room will automaticallyreduce the level of heat stress at watch stations; and, (3)that in a very hot space the watch standers will be keptcool by putting their heads up to or just inside a supplyterminal. In reality, the key element in spot cooling is nothigh velocities of air flow at the supply terminal but anoptimal effective air velocity flowing over the worker.This can be best accomplished by positioning the supplyterminal so as to assure a direct, unobstructed air streamat an equitable distance from the individual.
Figure 3-2 illustrates the relationship of air flowover workers versus the Percent Optimum Coolingachieved by the air flow. It can be seen that approxi-mately 72% optimum cooling is achieved at 250 fpm airmovement, 82% at 500 fpm, 90% at 750 fpm and 100%at approximately 1500 fpm; air flows over the workerwhich exceed 1500 fpm result in a rapid decrease in thepercent optimum cooling of the worker in a hot-humidenvironment. The very high air velocities cause turbu-lence and friction at exposed skin surfaces, which inturn, leads to heating of the skin and drying of the eyesand respiratory membranes. Unless the increased airflow is needed for engineering purposes, it is unecono-mical to increase the air flow six-fold (from 250 to 1500fpm) to obtain the remaining 28% optimum cooling.Furthermore, when air velocities over workers are 2,000fpm or higher the percent optimum cooling will havedropped to 36% or less. The reason that percent opti-mum cooling is essentially O% at 47 fpm air flow is dueto the natural “chimney effect” associated with standing
(6) Radiant heat control is essential relative to theworker. In the design of shipboard spaces which haveradiant heat sources it is necessary to insulate theradiating surfaces wherever possible. In those situationswhere metal surfaces cannot be insulated, they should bepainted with a low emissivity paint (emissivity less than0.4). Thermal insulation should have the lowest possiblethermal conductivity (k) value. The insulating materialshould be well-fitted together, should be of properthickness for the source temperature, should be keptintact, and protected by metal sheathing where hightraffic and abuse may occur. A reflective aluminizedoutside surface of thermal insulation pads will reduceradiant heat transfer into the space. In all cases, thermalinsulation should be kept dry to remain effective; whichrequires that steam and water leaks must be eliminated.Merely reinsulating radiating surfaces without first cor-recting the steam and water leaks leads to frequentreplacement of insulation.
Commercial industry statistical data, from multiplesamplings, show that the lowest k values for givendensities of thermal insulation are achieved with ceramic(refractory) fiber insulation, as compared with fiber-glass. Commercially available ceramic fiber at 8 poundsper cubic foot density has a lower k value than fiberglassinsulation at 11 pounds per cubic foot density; whereboth insulating materials are of equal thickness. Thelower the k value results in lower surface temperatureand lower radiant heat transfer, furthermore, the ce-
man.

3-7 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-7
ramic fiber insulation is lighter by approximately 3pounds per cubic foot. Until recently, the use of ceramicfiber insulation aboard Navy ships was only permitted attemperatures above 850 F. Military StandardsMIL-I-23 128 and MIL-STD-769 were revised, 1982and 1983 respectively, to permit use of ceramic fiberinsulation on machinery and piping surfaces below 850F. At the present time, all airborne thermal insulationmaterials should be considered as potentially healthhazardous.
(7) For many years the design of firerooms and enginerooms was based on equipment failure due to overheat-ing and the potential of heat transfer of excessive heat toadjacent compartments. It was believed that workerscould adapt or become “acclimatized” to the high levelsof heat. These concepts have been proven erroneous; thelimiting factor is the worker not the equipment. Thephysiological capability of workers cannot be altered totolerate excessively hot-humid and hot-dry shipboardspaces, therefore, it is essential to design such spaces topermit personnel to perform their watch standing andequipment maintenance safely. Table 3-1 is the ThermalPhysiology Design Criteria based on advanced, inte-grated technology. Allowances must be made for suffi-cient thermal recovery periods in thermal conditionssimilar to that noted in Article 3-7(3). Even with theexposure and recovery thermal design criteria givenherein, mental impairment of workers maybe detectableafter the first third of the respective exposure times. Theenvironmental conditions for recovery must permit at
least 6 hours of uninterrupted sleep per 24 hours. Thethermal design limits given in Table 3-1 apply to acute(short term) exposures only. No definitive informationexists at this time relative to the physiological effects oflong term (repetitive exposures over a number of years)exposures in hot-humid shipboard spaces; however, onecan assume that repeatedly exceeding the physiologicallimits of man is not conducive to the long term physio-logical well-being of the worker. (See Article 3-12.(8)regarding exceeding the PHEL values)
(8) The need for keeping the ventilation systems cleancannot be overemphasized. It has been estimated that alarge naval vessel may take in as much as several tons ofdirt a day into its ventilation system. Most of this iscomposed of fine, particulate matter which passesthrough filters but accumulate within ducting in highmoisture environments. A significant amount accumu-lates on the filters, screens, heaters, fans and coolingcoils and thus reduces the system’s capacity for deliver-ing the rated quantity of air. In order to obtain themaximum ventilation from existing equipment, all ven-tilation equipment should be cleaned and maintained onan established schedule. Use of a single layer of “cheese-cloth” may be used such as in galleys and laundriesprovided the cloth is changed frequently and dirt is notallowed to buildup. Maintenance of sufficient supplyventilation to control heat stress within a space shouldbe given priority over the use of “cheese-cloth” oversupply terminals.
Table 3-1. Summary of Thermal Physiology Heat Stress Design Conditions for Surface Vessels*
Thermal Values At Actual Work Sites*
SPACE/LEVEL Dry-Bulb Wet-Bulb Globe EffectiveVelocity**
[F] [F] [F] [FPM]
PROPULSION SPACES: (NON-GAS TURBINE)Upper Level 4 Hrs 107 86 115 250
6 Hrs 102 83 106 2508 Hrs 98 79 105 250
Lower Level 4 Hrs 98 84 108 2506 Hrs 92 81 100 2508 Hrs 89 78 96 250
PROPULSION SPACES: (GAS TURBINE)Upper Level 6 Hrs 98 85 100 250
8 Hrs 93 82 97 250Lower Level 6 Hrs 97 83 100 250
8 Hrs 91 81 94 250CATAPULT LAUNCH CONTROL ROOMS:
8 Hrs 92 80 97 250LAUNDRIES: 4 Hrs 96 85 103 250SCULLERIES: 3½ Hrs 92 83 94 250GALLEYS:
Food Prep. Area 4 Hrs 86 72 92 150Food Serving Area 3 Hrs 86 77 94 150
—*During normal work, excluding emergency or casualty control work rates. Environmental design conditions apply in work areas
regardless of external ambient weather and sea water temperatures.
3-8
3-8 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-9
3-8. General Considerations Ashore(1) Although the Navy has promulgated sound work
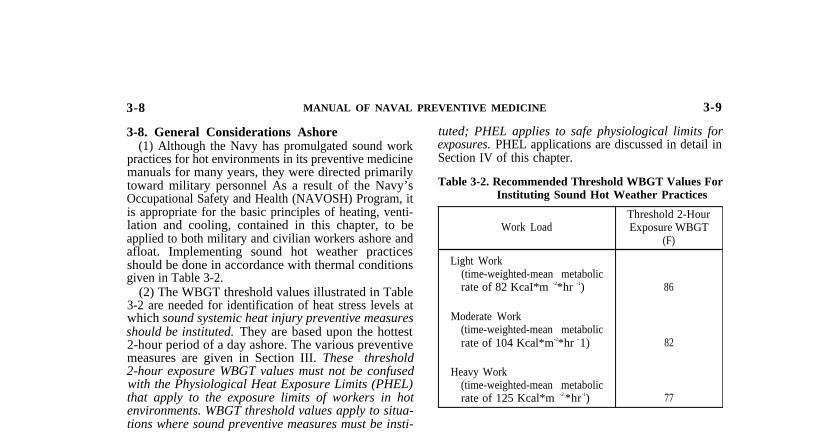
practices for hot environments in its preventive medicinemanuals for many years, they were directed primarilytoward military personnel As a result of the Navy’sOccupational Safety and Health (NAVOSH) Program, itis appropriate for the basic principles of heating, venti-lation and cooling, contained in this chapter, to beapplied to both military and civilian workers ashore andafloat. Implementing sound hot weather practicesshould be done in accordance with thermal conditionsgiven in Table 3-2.
(2) The WBGT threshold values illustrated in Table3-2 are needed for identification of heat stress levels atwhich sound systemic heat injury preventive measuresshould be instituted. They are based upon the hottest2-hour period of a day ashore. The various preventivemeasures are given in Section III. These threshold2-hour exposure WBGT values must not be confusedwith the Physiological Heat Exposure Limits (PHEL)that apply to the exposure limits of workers in hotenvironments. WBGT threshold values apply to situa-tions where sound preventive measures must be insti-
tuted; PHEL applies to safe physiological limits forexposures. PHEL applications are discussed in detail inSection IV of this chapter.
Table 3-2. Recommended Threshold WBGT Values ForInstituting Sound Hot Weather Practices
Threshold 2-HourWork Load Exposure WBGT
(F)
Light Work(time-weighted-mean metabolicrate of 82 KcaI*m -2*hr -1) 86
Moderate Work(time-weighted-mean metabolicrate of 104 Kcal*m-2*hr - 1) 82
Heavy Work(time-weighted-mean metabolicrate of 125 Kcal*m -2 *hr-1) 77
Section III. PHYSIOLOGICAL PRINCIPLES
ArticleEffects of Heat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-9Effects of Cold . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3-9. Effects of Heat(1) General Effects. Heat stress and heat strain have
both immediate and long-term effects on humans. Theimmediate effects are a significant loss of performance,efficiency and loss of duty time due to systemic heat injury.Generally, the long-term effects of heat stress and strain arcnot as apparent as the immediate effects. Prolonged expo-sure, however, is viewed as contributing to:
(a) Progressive loss of performance capability.(b) Increased susceptibility to other forms of stress.(c) Reduced heat tolerance.(d) Potentially increased physical disability com-
pensation.(2) Heat Balance Equation. In order to understand the
interaction between man and a heat stress environment,it is necessary to examine the concept of the empirical“Heat Balance Equation;” which is given as:
M ± R ± C – E =Swhere; M = metabolic rate or heat production of man
R = radiative heat gain to or loss from manC = convective and conductive heat gain to or
loss from manE = evaporative coolingS = heat storage in man
Man’s internal heat (M) is produced by basic metabolicfunction and heat of variable physical activity (work). Inthe “Heat Balance Equation” this factor (M) alwaysresults in a positive value; to be a living body the
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-10
function of metabolism must occur, therefore, heat willbe produced. Heat transfer by radiation (R), convectionand conduction (C) between man and its environmentmay result in a positive or negative heat balance. Forexample, if the environment is cooler than man anegative (toward the environment) heat balance willresult. Conversely, when the environment is warmerthan the subject, a positive heat balance (toward thesubject) results. If uncompensated, this latter stateresults in excessive heat storage and leads to the variousphysiological states we recognize as “heat strain”. Lossof body heat by evaporation (E) is the fourth means bywhich man is able to maintain thermal equilibrium.Evaporation by sensitive and insensitive perspirationresults in cooling of the body surface. Evaporation doesnot occur when the partial vapor pressure of water in theenvironment equals that of the body surface. Further, ifthe partial vapor pressure of water in the environmentexceeds that of the skin, environmental moisture con-denses on the skin with a resultant positive conductiveheat transfer by no evaporation. Evaporative heat lossfrom the respiratory mucosal surfaces is minimal, rep-resenting perhaps only 2070 of the matabolic heat (M).
(3) Thermoregulatory Mechanisms. Body heat is reg-ulated by a complex interactions of physical environ-mental factors (temperature, humidity, air movement,radiant heat, etc.) and the physiologic and behavioralresponse of the subject. The skin surface is the primary
3-9

3-8 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-9
3-8. General Considerations Ashore(1) Although the Navy has promulgated sound work
practices for hot environments in its preventive medicinemanuals for many years, they were directed primarilytoward military personnel As a result of the Navy’sOccupational Safety and Health (NAVOSH) Program, itis appropriate for the basic principles of heating, venti-lation and cooling, contained in this chapter, to beapplied to both military and civilian workers ashore andafloat. Implementing sound hot weather practicesshould be done in accordance with thermal conditionsgiven in Table 3-2.
(2) The WBGT threshold values illustrated in Table3-2 are needed for identification of heat stress levels atwhich sound systemic heat injury preventive measuresshould be instituted. They are based upon the hottest2-hour period of a day ashore. The various preventivemeasures are given in Section III. These threshold2-hour exposure WBGT values must not be confusedwith the Physiological Heat Exposure Limits (PHEL)that apply to the exposure limits of workers in hotenvironments. WBGT threshold values apply to situa-tions where sound preventive measures must be insti-
tuted; PHEL applies to safe physiological limits forexposures. PHEL applications are discussed in detail inSection IV of this chapter.
Table 3-2. Recommended Threshold WBGT Values ForInstituting Sound Hot Weather Practices
Threshold 2-HourWork Load Exposure WBGT
(F)
Light Work(time-weighted-mean metabolicrate of 82 KcaI*m -2*hr -1) 86
Moderate Work(time-weighted-mean metabolicrate of 104 Kcal*m-2*hr - 1) 82
Heavy Work(time-weighted-mean metabolicrate of 125 Kcal*m -2 *hr-1) 77
Section III. PHYSIOLOGICAL PRINCIPLES
ArticleEffects of Heat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-9Effects of Cold . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3-9. Effects of Heat(1) General Effects. Heat stress and heat strain have
both immediate and long-term effects on humans. Theimmediate effects are a significant loss of performance,efficiency and loss of duty time due to systemic heat injury.Generally, the long-term effects of heat stress and strain arcnot as apparent as the immediate effects. Prolonged expo-sure, however, is viewed as contributing to:
(a) Progressive loss of performance capability.(b) Increased susceptibility to other forms of stress.(c) Reduced heat tolerance.(d) Potentially increased physical disability com-
pensation.(2) Heat Balance Equation. In order to understand the
interaction between man and a heat stress environment,it is necessary to examine the concept of the empirical“Heat Balance Equation;” which is given as:
M ± R ± C – E =Swhere; M = metabolic rate or heat production of man
R = radiative heat gain to or loss from manC = convective and conductive heat gain to or
loss from manE = evaporative coolingS = heat storage in man
Man’s internal heat (M) is produced by basic metabolicfunction and heat of variable physical activity (work). Inthe “Heat Balance Equation” this factor (M) alwaysresults in a positive value; to be a living body the
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-10
function of metabolism must occur, therefore, heat willbe produced. Heat transfer by radiation (R), convectionand conduction (C) between man and its environmentmay result in a positive or negative heat balance. Forexample, if the environment is cooler than man anegative (toward the environment) heat balance willresult. Conversely, when the environment is warmerthan the subject, a positive heat balance (toward thesubject) results. If uncompensated, this latter stateresults in excessive heat storage and leads to the variousphysiological states we recognize as “heat strain”. Lossof body heat by evaporation (E) is the fourth means bywhich man is able to maintain thermal equilibrium.Evaporation by sensitive and insensitive perspirationresults in cooling of the body surface. Evaporation doesnot occur when the partial vapor pressure of water in theenvironment equals that of the body surface. Further, ifthe partial vapor pressure of water in the environmentexceeds that of the skin, environmental moisture con-denses on the skin with a resultant positive conductiveheat transfer by no evaporation. Evaporative heat lossfrom the respiratory mucosal surfaces is minimal, rep-resenting perhaps only 2070 of the matabolic heat (M).
(3) Thermoregulatory Mechanisms. Body heat is reg-ulated by a complex interactions of physical environ-mental factors (temperature, humidity, air movement,radiant heat, etc.) and the physiologic and behavioralresponse of the subject. The skin surface is the primary
3-9

3-9 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-9
site of heat exchange between the body anti the sur-rounding environment. Thermoregulation is mediatedby circulatory (e.g., central and capillary blood flow),neural (e.g., hypothalamic, autonomic pathways), andbiochemical (e.g., ionic and endocrine) functions involv-ing central or peripheral levels of response and byindividual behavioral variants. If man is to compensatefor environmental heat stress, this intricate physiologicnetwork must remain functionally intact. The degreeand reversibility of heat strain in any given case isdirectly related to the duration and severity of thedisturbance of mechanisms for heat regulation.
(4) Failure of Thermoregulation. When temperaturebalance mechanisms for the body fail, spiraling of bodytemperature is initiated. Heat storage increases; skin anddeep-tissue temperatures rise; cardiovascular, respiratoryand metabolic functions accelerate; and, renal functionis depressed. Increased metabolic heat pushes the cyclefaster to the point of cardiovascular and renal failureand irreversible damage to the nervous system andmuscular tissues. The cycle can be broken only by timelyand definitive therapy.
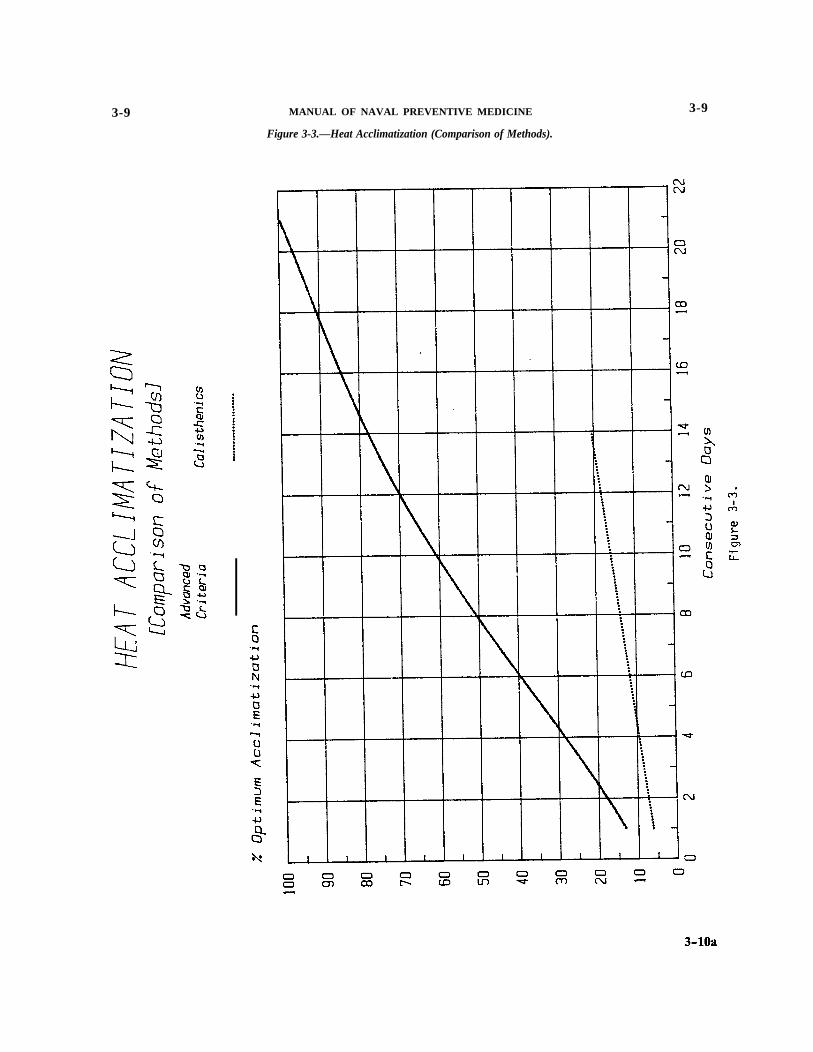
(5) Acclimatization. Physiologic response to heatstress has been treated thus far as a rapidly occurringprocess with decompensation resulting in relatively im-mediate damage or in cumulative injury over a moreprolonged time period. Under more favorable thermalconditions, the body can “acclimatize” or adapt toenvironmental heat stress. Until 1971 it was acceptedthat acclimatization to heat stress could be descriptivelycharacterized by near normalization of heart rate andskin and rectal temperatures during 4 to 6 days ofsuccessive heat exposure. In addition, sweat productionduring adaptation was expected to increase to levels of1.5 or more liters per hour. In 1971 Navy medicalresearchers indicated that these parameters were inade-quate to describe acclimatization accurately; the re-search indicated the earlier studies were premature in theassessment of heat acclimatization on consecutive days,as a number of other physiological parameters had notreached an adapted state. Using both untrained andtrained test subjects, the studies extended exposures outto 90 days. It was learned that heat acclimatization wasonly 78% complete after 14 consecutive days of work inhot-humid heat.
Application of advanced criteria for optimum heatacclimatization revealed, when personnel were previ-ously trained to perform moderate physical work with-out physiological strain in a thermally neutral environ-ment, that various body systems adapt at different rates.Table 3-3 illustrates the percent achievement of opti-mum heat acclimatization for 13 physiological parame-ters at 4 time intervals of consecutive days exposurewhile performing moderate physical work. Overall opti-mum heat acclimatization to hot-humid conditions of 95F DB, 88 F WB and air movement of 100 fpm wasachieved in 22 consecutive days of heat-work exposures.
As can be seen in Figure 3-3, the rationale prior to1971 overestimated how much heat acclimatization couldbe achieved in time periods as short as one week. In 1976
3-10
the findings of the Navy medical researchers were borneout by a research team in South Africa, who comprehen-sively studied energy exchanges, body temperatures, sweat-ing, cardiovascular adjustments, body fluid adjustments,body weight deficits and circulating protein changes.Clearly, there are 3 distinct stages of acclimatization, ofwhich the third stage begins after the seventh consecutiveday of inducing heat acclimatization.
Special consideration must be given to variousother factors. Heat acclimatization is not applicable tooverall heat stress levels indicated in Table 3–2; thus,personnel working in areas such as firerooms, enginerooms, laundries and steam catapult launch controlrooms should not be expected to adapt physiologicallyto their environment. In order to achieve maximumbenefits from acclimatization, it is extremely importantthat moderate (more than sedentary) work be performedduring the adaptation process. Even fully acclimatizedpersonnel are rendered more susceptible to heat injury inthe event of excessive fatigue; alcoholic intoxication;acute infectious disease; obesity; inadequate water, saltor caloric balance; and the use of medications contain-ing belladonna alkaloids. The rate of achievement ofheat acclimatization is retarded by the use of commer-cially prepared electrolyte-type beverages as well assupplementary sodium chloride (“salt”] in excess of 2
Table 3-3. Percent Optimum Heat Acclimatization onConsecutive Days of Heat-Work Exposuresfor Physically Trained Personnel
Physiologic Parameter
Rectal TemperatureTympanic Membrane
TemperatureDeep Esophageal
Temperature
Mean Skin Temperature
Heart RateSystolic Blood PressureDiastolic Blood PressurePulse PressureMean Arterial Blood
PressureEst. Total Vascular
ResistanceEst. Cardiovascular
Reserve
Sweat Rate
Urine Osmolality
Overall PercentAchievement
Percent Achievement On:
Day 1
6
6
51
80
81179
4
8
7
3
3
13
Day 7
38
37
82
93
37383636
35
37
36
37
39
45
Day 14
72
71
93
98
67567063
79
70
69
76
82
78
Day 21
100
100
100
100
100100100100
100
100
100
100
98
99.6
3-9 MANUAL OF NAVAL PREVENTIVE MEDICINE
Figure 3-3.—Heat Acclimatization (Comparison of Methods).
3-9

3-9 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-9
grams per day, this is discussed in more detail in thissection. Finally, a degree of stable acclimatization at anyone level of heat stress does not guarantee full acclima-tization to a higher level of heat stress.
(6) Heat Illnesses. There are various reasons whymilitary populations are more prone to heat disorders.The constant influx of unseasoned and unacclimatizedpersonnel into recruit training creates a potential for anincreased incidence of heat illnesses. Following recruittraining, exposure to a variety of environmental stressescan be expected, with little opportunity for prior adap-tation. In combat situations, with mass movements ofmilitary units to tropical and desert climates, welltrained personnel may be exposed to a higher level ofheat stress. A common-sense preventive measure pro-gram, emphasizing moderate physical activity and gen-eral health maintenance, will lead to the early adapta-tion of physically fit personnel to the more stressfulenvironment. Heat disorders have a world-wide distri-bution and may even occur in cold climates wheremetabolic heat production exceeds an individual’s adap-tive abilities. They may, in severe cases, be accompaniedby changes in serum electrolytes (hyponatremia, hypoch-loremia, acidosis, hyperkalemia), urinary electrolyteconcentrations (decreased sodium and chloride excre-tion, increased loss of potassium and hydrogen ions),proteinuria, increased consumption of protein, and coa-gulopathy (disseminated intravascular coagulationdefects). Acute overheating may thus lead to numerousheat related illnesses. In order to describe expeditiouslythese diseases and their management, they have beenconsolidated into 4 basic categories, excluding local heatinjury due to burns: (1) heat rash, (2) heat cramps, (3)heat exhaustion (including anhidrosis, salt-deficiency,water-deficiency, exercise-related heat exhaustion andheat syncope, and (4) heat stroke (includinghyperpyrexia).
(a) Heat Rash. The clinical picture of heat rash(miliaria rubra) is too well-known to require description.It is prevalent among military populations living in hotclimates or working in hot spaces ashore or aboard ship.It interferes with sleep, resulting in decreased efficiencyand cumulative fatigue, and thus, predisposes the indi-vidual to heat exhaustion. Heat rash impairs sweatingand decreases evaporative cooling on the skin surface; itmay, therefore, favor the evolution of heat stroke.
(b) Heat Cramps. Heat cramps may occur as anisolated syndrome with normal body temperature or inconjunction with heat exhaustion. They are precipitatedby the replacement of body water losses without concur-rent replacement of sodium chloride deficits. Heavilysweating individuals drinking large volumes of waterwith insufficient salt replacement are particularly atrisk. Heat cramps may be localized or generalized withrecently stressed muscle groups, particularly those of theextremities and abdominal wall are most frequentlyinvolved. Minimal serum and urinary electrolytechanges, as well as hemoconcentration, may be observedbut should not be expected. Clinically the patient usu-ally exhibits moist, cool skin and normal or slightly
elevated temperature. Muscular soreness (myalgia), anormal finding following heat cramps, must be differ-entiated from that occurring in association with rhab-domyolysis which is associated with necrosis of muscletissue. Whereas salt depletion appears to be instrumen-tal in the evolution of heat cramps, “salt loading” maybe contributory in the pathogenesis of rhabdomyolysis.Therefore, until definitive evidence is available, “saltloading” should be avoided in the prevention and ther-apy of heat cramps.
(c) Heat Exhaustion(1) Heat exhaustion occurs as the result of pe-
ripheral vascular collapse due to excessive dehydrationand salt depletion, however, the usual case involvesdehydration and over-exertion during physical work.The syndrome is characterized by profuse sweating,headache, tingling sensations in extremities, pallor,dyspnea, palpitations associated with gastrointestinalsymptoms of anorexia, and, occasionally nausea andvomiting. Neuromuscular disturbances with trembling,weakness, and incoordination coupled with cerebralsigns ranging from slight clouding of the sensorium toactual loss of consciousness complete the picture. Heatcramps may be present. Physical examination reveals amild to severe peripheral circulatory collapse with a pale,moist, cool skin and a rapid (120-200 beats per minuteat rest), thready pulse. Systolic blood pressure willgenerally have been quite elevated (180 mm Hg or higherduring work) prior to the onset of the illness, followedby a rapid drop while work continued, and withinnormal range by the time of examination; however, thewide pulse pressure during work will usually be de-creased at the time of physical examination. The oraltemperature may be subnormal (as in the case of hyper-ventilation being present) or slightly elevated. It is notuncommon to find rectal temperatures of heat exhaus-tion patients between 101-104 F, dependent upon thetype and duration of physical activity prior to the overtillness.
(2) Heat exhaustion is an accepted clinical diag-nosis and, as a classification of heat disorder, it consti-tutes the majority of reported cases of heat illnesses.However, from the standpoint of pathogenesis, heatexhaustion is not one but several entities. Exhaustion orcollapse in the heat can occur from physical work alone,even in the absence of dehydration or salt deficiency.Nevertheless, in some cases, more frequently in unaccli-matized personnel, water or salt deficiency is present tosome degree and may be primarily responsible for theclinical picture. Once again the problem of body saltcontent arises. Figure 3-4 illustrates numerous interact-ing factors predisposing heat cramps, heat exhaustion,heat stroke and rhabdomyolysis (noted under “HeatCramps”). Unless salt deficiency has been clearly dem-onstrated by laboratory analysis of serum or urine, oneshould be suspicious of salt loading if a reasonablynormal diet has been maintained and supplementary salthas been taken indiscriminately. Prior to 1972 there werenumerous reports indicating heat exhaustion patientshaving consumed between 6-24 salt tablets per 24 hours,
3-11

3-9 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-9
even when eating a well balanced diet. Since 1972 theNavy Medical Department placed use of salt tablets ona controlled basis, the high consumption of sodiumchloride has been primarily limited to eating fieldrations without sufficient water intake (See “Salt andWater Intake” in Article (8)(b)(2) of this Section). Allpatients suffering an episode of severe heat exhaustionshould be assigned light duty for 24-48 hours followingtheir initial recovery. Should a patient experience addi-tional bouts of heat exhaustion, a careful review of themedical history and working situation should be under-taken and corrective actions instituted. Strong considera-tion should be given to personnel being more suscep-tible to recurrence of heat exhaustion or possibly heatstroke. Recurrence of serious disorders are usually moresevere than the preceding bout. It is believed that thesusceptibility lasts, which requires affected personnel tobe reintroduced into the work situations in gradual stepsto determine their safe limitations. Documentation ofthe heat illness should be included in the individual’shealth record, details should be provided to guide fol-lowups or a clear history for future reviews.
(3) Heat Syncope is a familiar form of heatillness, not related to salt or water deficiency or toexcessive physical work. This type of heat illness istypically seen in troops standing in parade formation inhot outdoor climates. It is the result of pooling of bloodin dependent parts of the body and dilation of periph-
PATHOGENESIS OF COMPLICATIONS
OF EXCESSIVE PHYSICAL EXERCISE
Figure 3-4.
eral vessels. The disparity between vascular capacity andcirculating blood volume leads to cerebral ischemia.Vagotonia may be a contributing factor.
(4) Anhidrotic Heat Exhaustion maybe the resultof a preexisting dermatologic lesion (usually heat rash orsunburn) which interferes with sweat secretion. Person-nel may not be aware of progressive heat intoleranceassociated with impairment or absence of sweating. Saltand water deficiencies are not prominent in this form ofheat illness. Clinical examination reveals a warm, dryskin and an elevated deep body temperature, sometimesas high as 104–106 F. Exhaustion is present, but distur-bance of consciousness is uncommon in the early stagesof the disorder. Some individuals with the disorder maydevelop true heat stroke.
(5) When prompt first-aid is available, the mor-tality rate from heat exhaustion syndromes is extremelylow. As a rule, removal of the victim from a hotenvironment to a cool area, rest and fluid replacementwhen indicated will satisfy the needs of all but the mostsevere cases of this disorder.
(d) Heat Stroke — HEAT STROKE IS A MEDICALEMERGENCY and is associated with a potentially highmortality rate. Whereas heat exhaustion may be re-garded as the end result of overactive heat-balancemechanisms which are still functioning, heat strokeresults when thermoregulatory mechanisms are notfunctional, and the main avenue of heat loss (evapora-tion of sweat) is blocked. There may be prodromalsymptoms of headache, malaise and excessive warmth,or a general picture of heat exhaustion. The onset isusually abrupt with sudden loss of consciousness, con-vulsions, or delirium. Sweating may or may not beabsent in the typical case. Inquiry may reveal that thecessation of sweating was noted by the patient prior toonset of the other symptoms, however, with markedcentral nervous system (CNS) involvement (e. g., uncon-sciousness) this information usually comes too late.Since water intake may continue in the absence orreduction of sweating, overhydration rather than dehy-dration may occur. This is manifested by diuresis whichis an added signal of impending disaster. During theearly stages of this condition, after the body temperaturehas risen, the patient may exhibit euphoria. On physicalexamination the skin is hot, flushed and dry; in severecases petechiae may be present. Deep body temperatureis high, frequently in excess of 106 F. A rectal tempera-ture exceeding 108 F is not uncommon and indicates apoor prognosis. The pulse is full and rapid, while thesystolic blood pressure may be normal or elevated andthe diastolic pressure may be markedly depressed (60mm Hg or lower). Respirations are rapid and deep andsimulate Kussmaul breathing. As the patient’s conditionworsens, cyanosis is usually noted together with a pe-ripheral vascular collapse manifested by a rapid pulseand hypotension. The breathing becomes shallow andirregular. Pulmonary edema, incontinence, vomiting,hemorrhagic tendencies, disturbance of muscle tone,myocardial necrosis, menigismus, opisthotonos, jaun-dice, albuminuria, thrombocytopenia and prolongation
3-12

3-9 MANUAL OF NAVAL. PREVENTIVE MEDICINE 3-9
of the prothrombin time may occur. Renal failure withrapidly developing hyperkalemia and azotemia is notuncommon. Death may ensue very rapidly, but if thepatient survives until the second day, recovery chancesimprove. Rectal temperatures of 102-103 F may persistfor several days during which time mental disturbances,excitement and delirium may continue or recur. Head-ache may persist for several weeks after the attack. In thefirst few days after the temperature has been reducedfrom a critical level severe relapses may occur. Thepatient should, therefore, be observed carefully duringthis period and rectal temperatures should be recordedfrequently. Treatment, as outlined below, should bestarted again at the first indication of relapse. It is alsoimportant to emphasize that the heat regulating centersmay be extremely labile for many weeks after an attack.One attack of heat stroke predisposes to a second attack,and care should be taken by the individual to avoid asecond exposure to the precipitating condition. Analternative view is that the individual is a member of asusceptible population and remains susceptible. Carefuldocumentation of all factors associated with the occur-rence and treatment of this illness are essential.
(7) Treatment of Heat Casualties(a) Heat rash is best treated by keeping the skin dry
for part of the day at least. Cooled sleeping quarters willremedy the situation and permit personnel to work inhot-humid conditions without developing heat rash.Calamine lotion may be useful under appropriate envi-ronmental conditions. When the environment or physi-ological climate does not permit the skin to remain dryfor more than a few minutes a day, calamine linimentmay offer some relief.
(b) Heat cramps are initially treated by relieving thesevere pain and evaluating serum/urine chemistries forevidence of salt depletion. If such a deficiency exists, theadministration of O. 1% or physiologic saline solution bymouth or physiological saline intravenously may beindicated. Care should be taken not to give excessiveamounts.
(c) Heat exhaustion generally requires only rest in acool place and adequate water intake. As in the case ofheat cramps, saline solutions are indicated only whensalt depletion has been documented in the laboratory.When physical exertion preceded the onset of heatexhaustion, and a salt deficiency exists, the judiciousintravenous administration of physiologic saline or 5%glucose and saline may accelerate recovery. Recovery isusually prompt, but immediate return to duty is inad-visable except in the mildest cases.
(d) Anhidrotic heat exhaustion must be treated as ifit is heat stroke. Prompt intervention is essential. Untilthe normal skin function can be restored the patientshould not return to the environmental situation whichprecipitated the illness.
(e) Heat stroke is a MEDICAL EMERGENCY.Treatment principles are outlined below:
(1) Restore Normal Temperature. The body tem-perature must be lowered promptly to safe levels (rectaltemperature 100-101 F). The more prolonged the hy-
perpyrexia, the greater is the threat to life; the hyper-thermia accelerates metabolic heat production, causingthe body temperature to spiral upward at an ever-increasing rate. In the field, the patient’s clothing shouldbe removed, except for underwear. If there is a source ofcool water nearby, the patient should be immersed init—otherwise water should be sprinkled over the patientand its evaporation hastened by fanning. In addition tothese cooling measures, attendants should rub the vic-tim’s extremities and trunk briskly to increase the circu-lation to the skin. Arrangements should be made for theimmediate removal of the individual to a hospital orproperly equipped treatment facility; cooling measuresshould be continued during the transfer. Upon reachingthe medical facility, the patient should be placed in a tubof water and ice. W bile in the ice-water the extremitiesshould be massaged continuously as noted above. Whenthe rectal temperature drops to between 100-101 F, thevictim may be removed to a hospital bed. The rectaltemperature should be monitored every 10 minutes untilstable. Within the first few days of hospital treatmentthere should be careful observation for a relapse; thepatient may readily become hyperthermic or hypother-mic. It is desirable to maintain the rectal temperaturebetween 100-101 F. Rapidly increasing temperatures canusually be managed with ice water sponge baths andfanning; precipitous drops in temperature may requirethe judicious use of warm blankets. Shivering, involun-tary muscular activity, is undesirable because it accen-tuates tissue hypoxia and lactic acid acidosis. Again, thepatient’s rectal temperature should be monitored every10 minutes during a hyperthermic or hypothermiccondition.
(2) Drugs:(a) Sedative Drugs. Sedative drugs should be
avoided if possible since by their depressive effect theymay disturb central thermoregulatory centers. Restless-ness can usually be controlled with gentle restraint.Sedatives are indicated in the treatment of convulsions.If a longer acting drug is needed, pentobarbital shouldbe administered intramuscularly. Sodium amytal andmorphine are contraindicated.
(b) Other Drugs. Atropine or other drugswhich may interfere with sweating are contraindicated.Ephinephrine and other adrenergic drugs should not beused. However, when hypotension occurs accompaniedby low cardiac output (elevated central venous pressure,congestive heart failure) isoproterenol (or dopamine)can be effective in improving cardiovascular dynamics.Intravenous administration of mannitol to induce os-motic diuresis may be useful where renal tubular necro-sis is suspected. The use of aspirin, or like medications,is not indicated, since there is no evidence that it willlower body temperature in the noninfectious state. Smalldoses of diazepam (Valium— 10 mg) may be adminis-tered intravenously to control convulsions as needed.
(3) Intravenous Fluids. Parenteral administrationof physiological saline solution in moderate amounts(1,000-1,500 cc.) may be indicated. However, extremecaution must be exercised if a hyperthermic state exists;
3-13

3-9 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-9
in a hyperthermic state the patient may appear hypovo-lemic but would be normovolemic in a normothermicstate. Subsequent fluid administration must be deter-mined by hourly urinary output and serum electrolytedeterminations. Plasma volume expanders should beadministered with caution if there is evidence of shock,especially if the patient is reasonably normothermic; arapid pulse, of small volume, is an indication forconsidering their use. Care should be taken in theadministration of parenteral fluids if there are signs ofpulmonary congestion or rising central venous pressure.Close observation of the patient for renal failure isnecessary. Rapidly developing hyperkalemia and azote-mia necessitates hemodialysis or peritoneal dialysis.
(4) Venesection. Venesection is ineffective intreating the pulmonary edema which occurs with heatstroke.
(5) Oxygen. Oxygen may be desirable to combattissue anoxia. Oxygen should be administered by facemask or nasal catheter if cynosis or pulmonary conges-tion is present. The use of a nasal catheter rather than aface mask is recommended if the patient has beenvomiting, because of the danger of aspiration from theface mask.
(6) Other Complications. Spontaneous hemor-rhage may occur as the result of hypofibrinogenemia orconsumptive coagulopathy. Renal failure, pulmonarycongestion and cerebral edema may complicate theclinical course. Details of therapy are beyond the scopeof this manual. Readers are referred to current texts andtechnical papers on this subject.
(7) Disposition. All episodes of heat strokeshould be fully documented and made a part of thepatient’s permanent medical record. Evidence suggeststhat serious physiologic damage may persist long afterapparent recovery from heat stroke. Heat stroke victimsmay thus be more susceptible to recurrent episodes ofheat illness under less intense conditions. Heat strokevictims never be returned to heat stress similar to thatwhich precipitated the illness without the approval of anappropriate medical authority (Medical Board). A per-sonnel heat injury report (“Heat/Cold Injury Report”,NAVMED 6500/1) should be submitted to Commander,Naval Medical Command, Attention MED 22, Depart-ment of the Navy, Washington, D. C., 20372.
(8) Prevention of Heat Injuries(a) Engineering Control:
(1) Engineering measures begin with adequateisolation or insulation of the principal sources of heatand humidity. Sound engineering practice should bemaximum reduction of steam and water leaks, properventilation and maximum control of radiant heat. Insome situations the source should be completely en-closed and connected to an exhaust. Special industrialsettings may not permit the general atmosphere to becooled by ventilation or mechanical means, therefore,isolation of the workers from the sources of heat must bepracticed. When only a few workers are exposed in alarge space, control can be accomplished by spot coolingand use of clothing which is unstarched and has good
3-14
wicking characteristics, or by use of loose-fitting cover-alls through which cool air is circulated. The latter alsorequires an unrestrictive air supply which provides clean,filtered breathing air. The temperature of air striking aworker within the spot cooling cone should not be lessthan 80 F; for continuous exposure the velocity shouldbe approximately 250 fpm (See Article 3-7). Shortexposures to higher velocities, below those associatedwith skin friction (about 1500 fmp), are sometimesbeneficial in partially offsetting the presence of lowlevels of radiant heat. Workers can adjust their exposureby moving in and out of the spot cooling cone. Flexibleducts provide a means to regulate the location of spotcooling, thus avoiding excessive chilling of the head,shoulders and back. Engineering practice, however,should include proper positioning of supply terminals sothat maximal effective air velocities may be obtained.
(2) Control of radiant heat is essential, in termsof economy in operating the systems as well as thewell-being of personnel. As indicated in Article 3-7(6),thermal insulation should be well-fitted, no gaps, shouldbe of proper thickness for the source temperature,should be kept intact and protected by metal sheathingwhere high traffic of abuse may occur. Furthermore,multiple layers of paint reduce the effectiveness ofthermal insulation in controlling radiant heat. Snowwhite paint has an emissivity of approximately 0.9,whereas some highly buffed or polished stainless steels(e.g., Type 18-8, Allegheny metal No. 4 or No. 66) haveemissivities from 0.11-0.16. The lower the emissivity ofthe outer covering the better the control of radiant heat.However, it must be noted that applying thermal insu-lation over a low emissivity surface (e.g., pipes paintedwith low emissivity paint) does not effectively controlradiant heat transfer from the insulation surface. Theexposed surface emissivity is the important aspect ofradiant heat transfer. On bare, uninsulated metal theapplication of low emissivity paints (with emissivities of0.4 or less) will assist in controlling radiant heat transferto the space. Since the Navy undertook major replace-ment of asbestos thermal insulation with soft (fibrous)fiberglass there were many complaints that radiant heatincreased abroad ships. Part of the problem is associatedwith the quality of workmanship, but one cannot over-look the thermal conductivity (k) factors, densities andthicknesses of fiberglass replacement material. Thelower the k factor of thermal insulation the better thecontrol of radiant heat. Ceramic has a lower k factor at8 pounds per cubic foot density than the fiberglass at 11pounds per cubic foot density. Therefore, given equalthicknesses of ceramic (“refractory”) fiber insulationand fiberglass, the ceramic fiber insulation is superior incontrolling radiant heat. It is essential that the quality ofall thermal insulation materials must be checked toensure that specific characteristics of the materials areactually received to meet system design criteria. Whenextreme radiant heat is present, personnel should beprotected by use of reflective devices (e.g., clothing orscreens) and protection of hands, face and eyes. Alsowhenever personnel handle asbestos, fiberglass or ce-

3-9 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-9
ramic insulation materials, they should be protected; inparticular their respiratory systems should be protected.Asbestos and fiberglass have been proven to be delite-rious to the health of human, and recently ceramic fibershave been shown to be deleterious to the health ofanimals.
(3) In very special situations the use of vortexcooling garments may be used, but the objective liabil-ities may outweigh the subjective false sense of well-being which they impart; furthermore, as in the case ofcompressed air cooling, the air must be free of allpossible contaminants (e.g., same quality standard ofair used for diving). Other important preventive mea-sures include an adequate number of showers for theworkers, clean rooms for changing into dry clothes afterwork and a thermal environment with the design char-acteristics noted in Articles 3-7(3), 3-13(6) and 3-13(7).
(b) Medical Measures. Engineering methods are notalways effective and often must be supplemented orpreceded by medical measures. In physiologically com-pensable environments, performance in the heat can beimproved greatly by proper selection and acclimatizationof workers. In all hot environments, improved perfor-mance can be achieved by controlling fatigue, nutritionand alcoholic usage, and by periodic examination forunderlying illness and the early symptoms of heat strain.The reasons for different persons developing differentforms of heat illness are not clear. Until such informa-tion becomes available, every effort should be made torelieve excessive stress on each individual’s heat regulat-ing mechanism. The following measures will assist inreducing systemic heat injuries:
(1) Acclimatization. Heat acclimatization appliesto those environments which permit physiological com-pensation such as outdoors, or in those indoors situa-tions which are not excessively hot; for excessively hotindoors environments see Article 3-9(8)(b)(6). Heatacclimatization can only be acquired satisfactorily byworking in a compensable hot environment over aperiod of time (See Article 3-9(5)). Rapid acclimatiza-tion in raw recruits is impossible except under closemedical supervision; even then, it may be difficult toavoid some heat casualties. A “break-in” period ofabout two weeks, with progressive degrees of heatexposure and physical exertion will minimize the numberof systemic heat injuries and improve productivity overa longer time period.
(2) Salt and Water Intake. (Medical personnelwill find detailed information on salt and water require-ments in NAVMEDCOMINST 6260.6 series. )
(a) Indoctrination of supervisory personnel inrecognizing the need for liberal allowance of water willhelp abolish the false notion that men can be trained toresist dehydration. “Water discipline” must be replacedwith the doctrine of “water freedom” in which drinkingmoderate amounts of cooled water at frequent intervalsis encouraged.
(b) Maintenance of a proper salt content is ofgreatest importance, particularly to individuals in theearly stages of heat acclimatization. The rationale used
for many years was that large quantities of salt werebeing lost in the sweat and that the body was unable tomanage physiologic conservation of salt. Thus, it hadbeen widely assumed that large quantities of supplemen-tary salt were necessary, and that excessive amountswould be excreted without harmful effects. Unfortu-nately, many deleterious side effects were ignored foryears. The potential relationship of rhabdomyolysis andexcessive sale loading (Figure 3-4) lead to extensiveinvestigation of the relative value of supplementarysodium chloride intake by healthy young men (ages19-3 1) during training and heat acclimatization. It wasdetermined that:
(1) The current estimated “normal” dietaryintake of sodium chloride in the general United Statespopulation is approximately 15 gms daily. This estimateincludes the common practice of salt shaker supplemen-tation prior to tasting of served food.
(2) Field rations contain a variable amountof sodium chloride, dependent upon the Federal StockNumber and the manufacture dates. Individual CombatMeals (FSN 8970-577-4513) manufactured prior to 1975contain 22.1 gms of salt for those eating 3 meals per day,without using the salt packets. Individual Combat Mealsof the same stock number but manufactured as of 1975contain 9.0 gms of sodium chloride for three meals perday, without using the salt packets. Long Range PatrolFood Packets (FSN 8970-926-9222) contain 25.5 gms ofsodium chloride, without using the salt packets. Indi-vidual Ready-to-Eat Meals, replacing the IndividualCombat Meals noted above, contain 19.9 gms of sodiumchloride, without using salt packets. Each sodium chlo-ride (salt) packet contains 4 gms of salt, and up to 3packets are provided per day. Therefore, it is possible tohave an intake of 37.5 gms of NaCl per day. The highsalt content of field rations is basically to preserve thefood for a longer storage life.
(3) An individual’s greatest need would oc-cur during the combined stresses of initial physicaltraining and heat acclimatization in a hot-humid envi-ronment without water restriction. However, judicioususe of sodium chloride is recommended.
(4) The field grade salt tablets are 10 grain(0.648 gins; 0.255 gms of sodium and 0.393 gms ofchloride) each.
(c) The investigative results to date suggest thatthe free use of supplementary sodium chloride or salttablets is contraindicated under most conditions of heatstress. Proper sodium chloride level can be achieved byproviding adequate water a normal diet and a saltshaker on the table for conservative use, with no morethan the equivalent of 2.0 gms of supplementary salt(preferably not salt tablets) per day. Deviations fromthese recommendations must be governed by the pastand present medical histories of individual workers andadjusted according to individual need by the MedicalDepartment representative. There is clear evidence thatuse of commercially prepared electrolyte-type beveragesreduce physiologic performance. Furthermore, supple-mentary sodium chloride produces a 20% reduction of
3-15

3-9 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-9
the optimal work capacity of personnel in the heat,reduces the rate of achievement of optimal heat accli-matization and alters cardiac function. There are numer-ous deleterious physiologic changes which increase therisk of incurring heat illnesses when more than 2 gms ofsupplementary sodium chloride is ingested per day inhot environments. Use of supplementary sodium chlo-ride must be based upon the medical history and currentphysical status of each individual.
(d) Water intake requirements are a function ofwork performed, the level of heat stress and the amountof salt consumed. Figure 3-5 shows the relationship ofliters of water intake required as a function of heatstress, physical work and a “normal diet” sodiumchloride intake of 15.0 gms per day. Figure 3-6 showsthe same relationships but for 25.5 gms of sodiumchloride per day with the Long Range Patrol FoodPacket (FSN 8970-926-9222). In both Figures, no sup-plementary salt (salt packets) have been taken intoaccount. The water requirements in both Figures need tobe increased by 1 liter per day for every 6 gms of sodiumchloride (e.g., 2 liters per day for 3 salt packets (12 gmsof NaCl) per day in field rations).
(3) Special Programs. A program of special train-ing schedules for obese personnel and other groupssuspected of heat susceptibility will reduce systemic heatinjuries. Training supervisory and administrative per-sonnel should be taught to recognize the signs and
symptoms of excessive heat strain and impending heatstroke and heat exhaustion in these men.
(4) Clothing. Clothing should be worn loosely atthe neck, and at the cuffs of sleeves, and at the bottomof trousers to facilitate convective cooling. Some syn-thetic clothing materials interfere with evaporative cool-ing, although they may subjectively feel cooler. Poplinor other high natural fiber content clothes have good“wicking” characteristics and are superior materials forevaporative cooling. Navy dungarees are made from amixed fabric, 35% cotton and 65% synthetic fiber,which does not seriously interfere with evaporativecooling. Physiological heat transfer comparisons havebeen made between Navy 100 percent cotton fire retar-dant coveralls (e.g., those used outside of engineeringspaces) and mixed synthetic (5% Kevlar and 95% No-mex, known as “Aramid” and MIL-C–87093) fire retar-dant coveralls (e.g., engineering coveralls); no objectivedifferences were found although personnel thought themixed synthetic fiber coveralls were hotter. When thegiven mixed synthetic fiber coveralls were worn overunderwear, like that with dungarees, there was no sig-nificant thermal difference between wearing the cover-alls or dungarees. Physiological Heat Exposure Limit(PHEL) values do not need to be adjusted provided thecoveralls are worn only over underwear. However, wear-ing either of the Navy coveralls over dungarees andunderwear results in imposing a major heat load uponthe body due to added insulation and weight; obviously
Figure 3-5. Figure 3-6.
3-16

3-9 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-10
this is a serious problem in the case of personnel beingprotected in damage control situations, but one mustconsider the added protection from fires. It is stronglyrecommended that coveralls not be worn over dungareesduring damage or casualty control drills in hot and/orunventilated spaces, as this may readily induce heatexhaustion and heat stroke. Starch must not be utilizedwhere evaporative cooling from clothing is a majorfactor. Outdoors, helmet liners or headgear of similardesign provide more cooling and protection of the headthan caps.
(5) Field Training Exercises. Training exercisesrequiring sustained or severe physical effort, and thoseconducted in the prone position should be scheduled,when possible, in early morning or at night. Outdoorclasses should be conducted in the shade with adequateexposure to cooling wind. Even when training exercisesare performed in early morning or at night, high meta-bolic heat production by those performing physicalactivity can induce heat exhaustion or heat stroke. Onemust, therefore, continue to be aware of all factors thatmay precipitate systemic heat injuries.
(6) Excessive Heat Stress. When environmentalheat stress exceeds levels specified in Section IV, heatillness can be prevented by curtailing or suspendingnon-essential physical training and undue heat stressexposure. Obviously, operational mission requirements,excluding training programs, may preclude applicationof pertinent heat stress guides; in such cases the MedicalDepartment must be forewarned in order to adequatelyprepare facilities and staff for the anticipated increasednumber of heat illnesses. Mental and physical dysfunc-tion under thermal stress may be expected to amplify thefrequency of accidental injury.
(7) Other Medical Measures. Other medical mea-sures which will minimize the incidence of heat illnessesshould be considered. Adequate recovery from acute orcumulative fatigue (at least 6 hours of uninterruptedsleep per 24 hours in a comfortable thermal environ-ment), optimal physical fitness for the work to be done,absence of intercurrent illnesses, absence of febrilereactions (e. g., elevated body temperature due to immu-nizations), and absence of or minimal susceptibility toheat illnesses will aid in increased productivity of work-ers and help safe-guard their well being. Use of Navyeducational films is strongly recommended (See Article3-9(9) below).
(9) Educational Films. Navy educational films areavailable relative to the effects of heat stress, physicalwork, water requirements, sodium chloride intake andpredisposing factors relative to heat disorders. The “allhands” film, “Heat Stress Monster” (35025-DN), is ananimated film portrayal of multiple aspects of heatstress both ashore and afloat. On the other hand, “IfYou Can’t Stand The Heat . . .” (35026-DN) is acounterpart film for supervisory level personnel afloat.Many of the informational aspects of this Chapter arepresented in these films. Also see Article 3-2(2)(h)regarding the Navy educational film on “Care and Useof the Heat Stress Meter”.
3-10. Effects of Cold(1) The adverse effects of low environmental temper-
atures on the human body may be localized or general-ized, or a combination of both. They may occur attemperatures above or below freezing and under wet ordry conditions. The pathophysiologic features of coldinjury are dependent on the environmental temperature,exposure time and individual susceptibility or resistance.One form of adverse cold response has already beendiscussed under “cold shock” in Section 11, Article3-6(4).
(2) General Physiologic Effects of Acute Cold Expo-sure. The physiologic response to total body cooling ismanifested by the conservation of thermal energy and anincrease in heat production. With prolonged or severeexposure, the defense mechanisms fail, heat loss exceedsheat production, and the body temperature falls. Duringthe initial response to cold exposure, stimulation of thesympathetic nervous system causes a reflex superficialvasoconstriction with shunting of blood to the internalorgans. This is accompanied by reflex shivering whichincreases muscular activity, heat production and oxygenconsumption. Constriction of cutaneous capillary bedsis manifested by pallor, mottling or cyanosis of the skin;in hypersensitive individuals histamine release may causeurticaria. In responding to stress the body secretesepinephrine which accelerates the cardiac rate, increasesblood pressure and mobilizes liver glycogen stores.Blood coagulability is increased and pooling of water inthe extravascular spaces (skin, muscle, subcutaneoustissues) results in hemoconcentration. Sudden exposureto extreme cold causes reflex muscle spasm and respira-tory arrest. More gradual cooling eventually causesunconsciousness (88-89 F rectal) and is accompanied byslowing of respiration and heart rate, and falling of theblood pressure. Although some individuals have sur-vived rectal temperatures as low as 72 F, ventriculararrhythmias (fibrillation) and cardiac arrest may beexpected when rectal temperature falls below 80 F. Inpersons exposed to rain, snow, wind and cold, the onsetof hypothermia may be insidious. The first warning maycome with violent shivering, marked fatigue, stubbor-nest and hallucinations as the body temperature dropsbelow 91-95 F. Unconsciousness and cardiorespiratoryarrest may rapidly follow unless resuscitative efforts arebegun immediately.
(3) Chronic Effects of Cold Exposure. It has beensuggested that recurrent exposure to cold and to changesin environmental temperature may lower individual re-sistance to infectious disease. Research in this area isincomplete; therefore, definitive conclusions cannot bestated.
(4) Characteristics of Localized Cold Injury:(a) Nonfreezing Injury. Non-freezing injuries occur
at ambient temperatures above 32 F, but below 50 F, andare most frequently manifested as chilblain (pernio) andcold water immersion foot (trench foot). Exposure timeis variable but is usually measured in hours. A highenvironmental moisture favors non-freezing injuries byaccelerating heat loss. Peripheral vasoconstriction, ve-
3-17

3-10 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-10
nostasis and increased blood viscosity impair normaltissue oxygenation and the removal of cellular metabo-lites. This may be accompanied by increased capillarypermeability and intravascular agglutination or sludgingof red blood cells. Chilblain is characterized by initialblanching and pallor—followed on rewarming by flush-ing, itching and edema. Blistering may be present andcontinued cold exposure may lead to hemorrhagic orulcerative lesions. Cold water immersion foot may ini-tially be no more troublesome than chilblain; however,prolonged exposure leads to more severe anoxic impair-ment. During the hyperemic phase the pain is usuallysevere, tissue destruction is more pronounced and gan-grene may supervene with the resultant loss of the limb.Late complications of cold water immersion foot includedyshidrosis, Raynaud’s phenomenon and causalgia. Sec-ondary complications, including infection and throm-bophlebitis, are not uncommon.
(b) Freezing Injury (Frostbite). The pathophysiol-ogy of frostbite is presently uncertain. It occurs only atenvironmental temperatures below freezing and the ex-tent of tissue destruction depends primarily on thetemperature and length of exposure. The freezing ofintracellular and extracellular fluid results in the forma-tion of ice crystals which mechanically disrupt cellmembranes. There is a lack of agreement as to whetherthe injury is due to cellular injury and changes invascular permeability or to the vascular stasis and tissuehypoxia. First degree frostbite is similar to mild chilblainwith hyperemia, mild itching and edema; no blisteringor peeling of the skin occurs. Second degree frostbite ischaracterized by blistering and desquamation. In thirddegree frostbite there is necrosis of the skin and subcu-taneous tissues with ulceration. The most severe tissuedamage is seen in fourth degree frostbite with destruc-tion of connective tissues and bone accompanied bygangrene. Secondary infections and the sequelae notedfor non-freezing injuries are not infrequent.
(5) Factors Influencing Cold Injury(a) Weather The prevention of cold injury is facil-
itated by the availability of accurate meteorologicalinformation, including air temperature, humidity andwind velocity. For practical purposes, the cooling effectof air temperature and wind velocity have been com-bined in the Equivalent Temperature standard (WindChill Index Chart) which is presented in Section IV.
(b) Physical Work. Heavy physical activity mayaccentuate heat loss by perspiration; in addition, themoisture becomes trapped in-excess clothing and reducesits insulating capacity. Prolonged excessive activity leadsto mental and physical fatigue which may lead to fatalhypothermia in a cold environment. Total immobility,on the other hand, decreases the production of bodyheat with cooling of the extremities and circulatoryimpairment in dependent parts. It is advisable, there-fore, to tread the middle ground and recommend mod-erate activity with adequate rest. Increased exercise ofthe extremities should be encouraged when personnel arein confined positions in cold climates.
(c) Physical Well-Being and General Health. Per-
3-18
sons with previous cold injury, especially that of recentorigin, heavy smokers and those taking medicationswhich affect the vasomotor tone are at special risk incold environments. Seriously wounded individuals withsignificant blood loss and decreased activity are predis-posed to cold injury as are those on starvation ornear-starvation diets. Consumption of alcoholic bever-ages causes vasodilation and accelerates heat loss, thusfavoring the development of frostbite and hypothermia.
(d) Personal Characteristics. Although the epide-miologic reasons are unclear, younger lower rankingpersonnel, Caucasians from United States climates withminimum January temperatures above 20 F, and Amer-ican Blacks appear to share an increased hazard ofdeveloping cold injury. Persons with negativistic behav-ior patterns are also at risk. Therefore, line commandersand Medical Department personnel may find it particu-larly valuable to concentrate preventive educationamong these individuals.
(e) Clothing. Protective clothing, available whenneeded and properly worn, is essential to conservationof body heat. Garments should be clean, dry and allowfor adequate air circulation between and through layers.Apparel should be fitted so as to avoid peripheral limbconstriction with attending circulatory impairment. Thefeet and hands require special care in order to avoidmaceration of the skin and secondary infection. This isbest accomplished by adequate changes of socks andgloves and liberal use of soap and water cleansing. Whenpossible, footgear should be dried between periods ofuse.
(f) Preventive Education. All personnel should beoriented to their individual responsibility in the preven-tion of cold injuries. Predisposing and preventive factorsshould be widely promulgated, and negative attitudesdiscouraged.
(6) Treatment of Local Cold Injuries(a) First Aid. Frozen body parts should be re-
warmed until thawed. This can be accomplished byimmersion in a water bath of 104-106 F; temperaturesabove this level should be strictly avoided. In the fieldwhere water is not available, the part may be-warmed inthe axilla of a normothermic companion. In most casesthe frozen body part has already thawed by the time thevictim comes for initial treatment and further activewarming measures are not required. Wet clothing shouldbe removed and body parts dried and protected fromtrauma. Blisters should be left intact and sterile fluffdressings applied. Deep body temperature should bemaintained with blankets and warm liquids. All individ-uals with cold injury of the extremities should bemanaged as litter patients with the limb slightly elevated.All cold injury victims should be evaluated by qualifiedMedical Department personnel as soon as possible.
(b) AVOID: COLD-INJURED PARTS SHOULDNOT BE RUBBED WITH SNOW OR ICE WATER OROTHERWISE TRAUMATIZED. BECAUSE OFTHEIR EFFECTS ON CAPILLARY CIRCULATION,THE USE OF ALCOHOLIC BEVERAGES ANDTOBACCO IS STRICTLY CONTRAINDICATED.

3-10 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-10
OINTMENTS AND CREAMS SHOULD NOT BEAPPLIED.
(c) Symptomatic Care. Pain is sometimes severe inrewarmed limbs and may require administration ofnarcotics for relief. Itching and urtication may be re-lieved by antihistaminics and milder analgesics.
(d) Definitive Therapy:(1) Affected parts should be kept clean and either
treated “closed” with sterile dressings or “open” withsterile sheets and proper nursing precautions.
(2) Tetanus boosters should be given where indi-cated.
(3) Since frostbite victims are frequently dehy-drated, they may benefit from the administration ofLactated Ringer’s Solution. Low-molecular-weight dex-tran or Heparin may be indicated if vascular “sludging”or thrombophlebitis are suspected.
(4) In frostbite devitalized and gangrenous tissuesmay separate spontaneously after 60-90 days. Sympa-thectomy may be indicated in severe cases of frostbiteand immersion foot to relieve causalgic pain. Surgicaldebridement may become necessary as well as skingrafting. Amputation should be conservative.
(5) Physical therapy includes early active andpassive movement of affected parts and later rehabilita-tion of compromised function.
(6) Antibiotic therapy may be necessary if sec-ondary infection becomes a problem, and should ideallybe guided by bacterial culture and sensitivity testingevidence.
(e) Disposition. All episodes of cold injury shouldbe documented in the patient’s medical records. Recur-rent episodes may be cause for reassignment or medicalboard.
(7) Clinical Manifestations and Treatment of Gener-alized Hypothermia:
(a) Generalized hypothermia may be classified asinduced or accidental. Induced hypothermia is a valuedadjunct to general anesthesia for select surgical proce-dures. It is implemented under controlled conditions byqualified personnel. Vital functions (circulatory, respi-ratory, cardiovascular) are carefully monitored as thebody temperature is lowered and maintained for theduration of the surgery. Temperatures are generallymaintained above 82 F. Accidental hypothermia may beobserved in newborns, in the elderly and in associationwith certain lesions of the endocrine and central nervoussystems. In the military, it is most frequently seen inindividuals who have been exposed to cold for prolongedperiods of time. Fatigue, severe wounds, cold waterimmersion (aircraft, ship and submarine accidents), andinadequate cold weather gear contribute to the evolutionof accidental hypothermia. Case reports suggest thattolerance to deep hypothermia (77 F) may occasionallybe enchanced by the depressant effect of alcoholicintoxication and excessive doses of sedative drugs. Thisphenomenon, however, is unpredictable and shouldnever be considered in the context of therapy. Individualcold tolerance and the unreliability of the clinical signsof “death” during severe hypothermic episodes make it
imperative that resuscitative measures be instituted im-mediately in all cases of accidental hypothermia. Car-diovascular and respiratory support should ideally becontinued until it can be confirmed by more sophisti-cated means that all signs of life are absent.
(b) Clinical Manifestation of Hypothermia. Thepatient is pale, comatose, and may appear dead. Respi-rations are slow and shallow and may be difficult todetect. The pulse is faint or absent, the precordialimpulse may be inapparent and the blood pressure isfrequently unobtainable. The victim is hyporeflexic andunresponsive to painful stimuli. Pupils are unreactive tolight, but are usually not dilated. The body tissues aresemirigid and resist passive movement. Body tempera-tures are frequently below 82 F (rectally), and cannot bemeasured with the usual clinical thermometers (Seebelow for Subnormal Clinical Thermometer). Urineoutput is negligible. Death may occur in spite of appar-ently successful resuscitative measures.
For clinical monitoring of hypothermic patients,there is a special thermometer available. The followinginformation is provided:
Thermometer, Clinical Human, Oral/Rectal,Subnormal(Range 70-100 F) Stock number9L-6515-00-139-4593
(c) Therapy of Accidental Hypothermia:(1) Genera{ Measures. Initial resuscitative mea-
sures should concentrate on the restoration of vitalfunctions. If respirations are present and ventilation isadequate, the therapists attention may be diverted toother resuscitative measures. Otherwise mouth-to-mouth resuscitation and external cardiac massage (ifindicated) should be initiated in the field. The patientshould be kept warm during transportation to a medicalfacility and examined for concurrent injury and drug orethanol intoxication. Supplemental oxygen will usuallybe indicated. An oral airway should be inserted. Uponarrival at a medical facility, the apneic patient shouldhave an endotracheal airway inserted to aid mechanicalventilation and suction. Intravenous lines should beestablished for the administration of resuscitative fluidsand the measurement of central venous or pulmonarywedge pressures. A nasogastric tube will allow evacua-tion of stomach contents and prevent aspiration, and anindwelling urinary catheter will serve to monitor urineoutput. Blood gas, pH, and electrolyte determinationswill aid in effective management. Body temperature isbest monitored by rectal thermistor probe, otherwise usethe subnormal clinical thermometer noted above.
(2) Rewarming. Rewarming must be approachedwith caution in order to avoid serious consequences.Controversy still exists as to the most effective and safestmeans by which to restore normal body temperature.Rapid rewarming appears to be the most effective incases where cold exposure (most frequently cold waterimmersion) has been brief. It is accomplished by totalbody immersion in warm water (about 104 F). Hypo-thermic patients, however, may be inadvertently burnedby this approach and are subject to the poorly under-stood phenomenon of “rewarming shock”. Slow re-
3-19
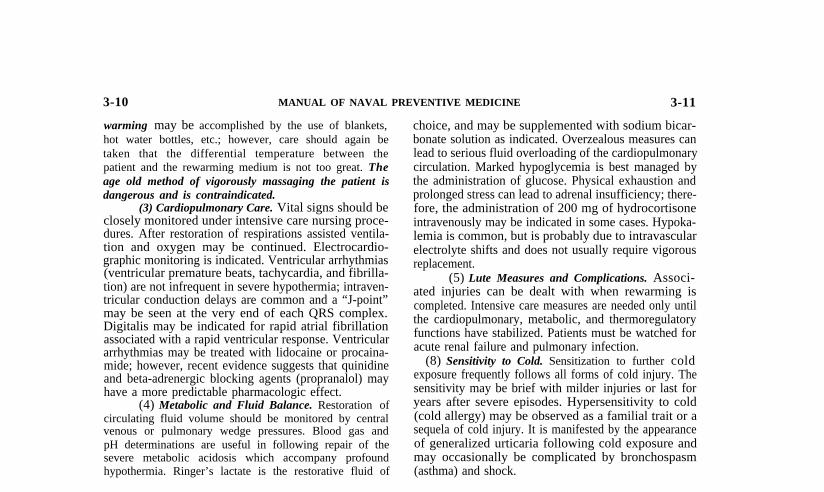
3-10 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-11
warming may be accomplished by the use of blankets,hot water bottles, etc.; however, care should again betaken that the differential temperature between thepatient and the rewarming medium is not too great. Theage old method of vigorously massaging the patient isdangerous and is contraindicated.
(3) Cardiopulmonary Care. Vital signs should beclosely monitored under intensive care nursing proce-dures. After restoration of respirations assisted ventila-tion and oxygen may be continued. Electrocardio-graphic monitoring is indicated. Ventricular arrhythmias(ventricular premature beats, tachycardia, and fibrilla-tion) are not infrequent in severe hypothermia; intraven-tricular conduction delays are common and a “J-point”may be seen at the very end of each QRS complex.Digitalis may be indicated for rapid atrial fibrillationassociated with a rapid ventricular response. Ventriculararrhythmias may be treated with lidocaine or procaina-mide; however, recent evidence suggests that quinidineand beta-adrenergic blocking agents (propranalol) mayhave a more predictable pharmacologic effect.
(4) Metabolic and Fluid Balance. Restoration ofcirculating fluid volume should be monitored by centralvenous or pulmonary wedge pressures. Blood gas andpH determinations are useful in following repair of thesevere metabolic acidosis which accompany profoundhypothermia. Ringer’s lactate is the restorative fluid of
choice, and may be supplemented with sodium bicar-bonate solution as indicated. Overzealous measures canlead to serious fluid overloading of the cardiopulmonarycirculation. Marked hypoglycemia is best managed bythe administration of glucose. Physical exhaustion andprolonged stress can lead to adrenal insufficiency; there-fore, the administration of 200 mg of hydrocortisoneintravenously may be indicated in some cases. Hypoka-lemia is common, but is probably due to intravascularelectrolyte shifts and does not usually require vigorousreplacement.
(5) Lute Measures and Complications. Associ-ated injuries can be dealt with when rewarming iscompleted. Intensive care measures are needed only untilthe cardiopulmonary, metabolic, and thermoregulatoryfunctions have stabilized. Patients must be watched foracute renal failure and pulmonary infection.
(8) Sensitivity to Cold. Sensitization to further coldexposure frequently follows all forms of cold injury. Thesensitivity may be brief with milder injuries or last foryears after severe episodes. Hypersensitivity to cold(cold allergy) may be observed as a familial trait or asequela of cold injury. It is manifested by the appearanceof generalized urticaria following cold exposure andmay occasionally be complicated by bronchospasm(asthma) and shock.
Section IV. THERMAL STANDARDS
ArticleGeneral Requirements. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-11Assessment of Heat Stress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...3-12Practical Heat Stress StandardsPractical Cold Stress Standards
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-13
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-14
3-11. General Requirements(1) The major objectives of the thermal standards are to
facilitate mission accomplishment by maximizing produc-tivity and maintaining the well-being of personnel.
(2) Elimination of Smoke and Noxious Odors. Smokeand noxious odors are readily detectable in closed spaces.Ventilation rates to eliminate odors from berthing areasand living quarters are considerably in excess of thoserequired to supply oxygen and remove carbon dioxide.Attempts to filter or mask unpleasant odors have notmet with significant success. Tobacco smoke is likewisedifficult to remove from confined spaces aboard ship,particularly in submarines where air is recirculated.Noxious odors are not physically harmful, but tend toexert an unfavorable effect on appetite and morale.Tobacco smoke, on the other hand, may have variedharmful effects on smokers as well as non-smokers.Personnel exhibit a variable tolerance for tobacco smokewith some individuals developing symptoms of hyper-sensitivity (allergy). Smoke acts as an irritant to the eyesand respiratory membranes. Smoking should be prohib-
3-20
ited in spaces where the carbon monoxide content of theair exceeds the following limits:
(a) 25 parts per million and continuous exposure for90 days.
(b) 50 parts per million and exposure for 8 hoursdaily.
(Other standards exist depending on the length ofexposure, physical activity performed and requirementsfor mental acuity.)
(3) Elimination of Fuel Combustion Gases and/orFuel Vapors. Fuel combustion gases and fuel vaporshave toxic effects upon personnel. In the area of thermalphysiology, these gases and vapors cause vasodilation ofthe peripheral blood vessels at times when cardiovascu-lar stability has already been compromised. Since hu-mans cannot increase their existing circulating bloodvolume to compensate for the marked increase of theircardiovascular system capacity, the resultant effect is toincur further impairment of the cardiovascular system tomeet the physiologic demands of the work and environ-ment. This produces a critical impact when the added

3-10 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-11
warming may be accomplished by the use of blankets,hot water bottles, etc.; however, care should again betaken that the differential temperature between thepatient and the rewarming medium is not too great. Theage old method of vigorously massaging the patient isdangerous and is contraindicated.
(3) Cardiopulmonary Care. Vital signs should beclosely monitored under intensive care nursing proce-dures. After restoration of respirations assisted ventila-tion and oxygen may be continued. Electrocardio-graphic monitoring is indicated. Ventricular arrhythmias(ventricular premature beats, tachycardia, and fibrilla-tion) are not infrequent in severe hypothermia; intraven-tricular conduction delays are common and a “J-point”may be seen at the very end of each QRS complex.Digitalis may be indicated for rapid atrial fibrillationassociated with a rapid ventricular response. Ventriculararrhythmias may be treated with lidocaine or procaina-mide; however, recent evidence suggests that quinidineand beta-adrenergic blocking agents (propranalol) mayhave a more predictable pharmacologic effect.
(4) Metabolic and Fluid Balance. Restoration ofcirculating fluid volume should be monitored by centralvenous or pulmonary wedge pressures. Blood gas andpH determinations are useful in following repair of thesevere metabolic acidosis which accompany profoundhypothermia. Ringer’s lactate is the restorative fluid of
choice, and may be supplemented with sodium bicar-bonate solution as indicated. Overzealous measures canlead to serious fluid overloading of the cardiopulmonarycirculation. Marked hypoglycemia is best managed bythe administration of glucose. Physical exhaustion andprolonged stress can lead to adrenal insufficiency; there-fore, the administration of 200 mg of hydrocortisoneintravenously may be indicated in some cases. Hypoka-lemia is common, but is probably due to intravascularelectrolyte shifts and does not usually require vigorousreplacement.
(5) Lute Measures and Complications. Associ-ated injuries can be dealt with when rewarming iscompleted. Intensive care measures are needed only untilthe cardiopulmonary, metabolic, and thermoregulatoryfunctions have stabilized. Patients must be watched foracute renal failure and pulmonary infection.
(8) Sensitivity to Cold. Sensitization to further coldexposure frequently follows all forms of cold injury. Thesensitivity may be brief with milder injuries or last foryears after severe episodes. Hypersensitivity to cold(cold allergy) may be observed as a familial trait or asequela of cold injury. It is manifested by the appearanceof generalized urticaria following cold exposure andmay occasionally be complicated by bronchospasm(asthma) and shock.
Section IV. THERMAL STANDARDS
ArticleGeneral Requirements. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-11Assessment of Heat Stress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...3-12Practical Heat Stress StandardsPractical Cold Stress Standards
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-13
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3-14
3-11. General Requirements(1) The major objectives of the thermal standards are to
facilitate mission accomplishment by maximizing produc-tivity and maintaining the well-being of personnel.
(2) Elimination of Smoke and Noxious Odors. Smokeand noxious odors are readily detectable in closed spaces.Ventilation rates to eliminate odors from berthing areasand living quarters are considerably in excess of thoserequired to supply oxygen and remove carbon dioxide.Attempts to filter or mask unpleasant odors have notmet with significant success. Tobacco smoke is likewisedifficult to remove from confined spaces aboard ship,particularly in submarines where air is recirculated.Noxious odors are not physically harmful, but tend toexert an unfavorable effect on appetite and morale.Tobacco smoke, on the other hand, may have variedharmful effects on smokers as well as non-smokers.Personnel exhibit a variable tolerance for tobacco smokewith some individuals developing symptoms of hyper-sensitivity (allergy). Smoke acts as an irritant to the eyesand respiratory membranes. Smoking should be prohib-
3-20
ited in spaces where the carbon monoxide content of theair exceeds the following limits:
(a) 25 parts per million and continuous exposure for90 days.
(b) 50 parts per million and exposure for 8 hoursdaily.
(Other standards exist depending on the length ofexposure, physical activity performed and requirementsfor mental acuity.)
(3) Elimination of Fuel Combustion Gases and/orFuel Vapors. Fuel combustion gases and fuel vaporshave toxic effects upon personnel. In the area of thermalphysiology, these gases and vapors cause vasodilation ofthe peripheral blood vessels at times when cardiovascu-lar stability has already been compromised. Since hu-mans cannot increase their existing circulating bloodvolume to compensate for the marked increase of theircardiovascular system capacity, the resultant effect is toincur further impairment of the cardiovascular system tomeet the physiologic demands of the work and environ-ment. This produces a critical impact when the added

3-11 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-11
load of heat stress is present. The ambient concentrationsof aromatic hydrocarbons, using hexane as the referencegas for quantitative analysis, which produce such re-sponses in humans is between 10-14 mg/m3 of air. Higherconcentrations of aromatic hydrocarbons have relativelylittle further effect on human short-term exposure; concen-trations as high as 690 mg/m3 have not resulted in signif-icant changes from that measured at the lower concentra-tions. One must be aware that the threshold concentrationsfor aromatic hydrocarbons and oxides of nitrogen andsulfur, in combined environmental stress situations, appearto be quite low. Cardiovascular “shock” occurs withoutsignificant hyperthermic responses. Table 3-4 generalizessome of the physiologic impact of fuel combustion gasesand fuel vapors where 135 personnel exhibited and sensedbody changes due to the presence of these gases and vaporsaboard Navy ships in mild heat stress situations. In allcases, the Physiological Heat Exposure Limits (PHEL)times alone were 4–6 hours, but the personnel exposureshad to be terminated quite prematurely when the overalleffects justified removal for physiological safety purposes.
Since the physiologic thresholds of the gases andvapors are low, the results from calorimetric detectortubes used aboard ships should be considered unreliable.Research has shown that ambient water vapor results infalse low values from a variety of calorimetric detectortubes, water molecules occupy sites in the chemical bedsand thereby reduce the number of available sites for
Table 3-4. General Physiologic Impact of Fuel Com-bustion Gases and Fuel Vapors
Parameters Change
Cardiovascular:Heart Rate Slight increaseSystolic Blood Pressure Marked reductionDiastolic Blood Pressure Marked reductionMean Arterial Blood Pressure Very marked
reductionEstimated Cardiac Output Marked increaseTotal Vascular Resistance Very marked
reductionOverall Cardiovascular Reserve Very marked
reduction
Sensory:Tip of Tongue Tingling/numbnessNose Tingling/numbnessFinger Tips Tingling/numbnessToes Tingling/numbness
Eyes Lacrimation
Respiratory Distress
Body Temperatures No apparent changeat time of exitingenvironment
reactions to occur in the detector tubes. Gas free engi-neering methods, generally available aboard ships, can-not reliably measure these low levels of likely toxiccomponents in fuel combustion gases and fuel vaporsthat are pertinent to this subject. Portable, direct read-ing instrumentation which is durable, accurate at lowconcentrations, has specificity for a variety of atmos-pheric components, has a high degree of reproducibility,maintains calibration and has an adequate response timeis extremely expensive. We are left with the difficulty ofestimating the presence of physiologically significantlevels of atmospheric contaminants and what to do tominimize the impact upon personnel, especially if thecontaminants are permitted to remain in work spaces.
Fortunately, the Physiological Heat Exposure Lim-its (PHEL) Chart and information available regardingthe sensory, eyes and respiratory responses of shipboardpersonnel in such environments exists. During whatwould normally be 4-6 hour heat stress exposure limits,it was repeatedly found that the physiologically safeexposure times could be determined by use of the PHELChart. Using the methods described in this Chapter andthe OPNAVINST 5100.20 series for determining theWBGT Index and PHEL times, reduction of the deter-mined PHEL exposure times by 66% would minimizethe reduced physiologic performance of personnel. Forexample, a PHEL stay time of 4 hours becomes 1.4hours (1 hr 24 reins) and 6 hours becomes 2.1 hours (2hrs 6 reins). Therefore, adjustment of the PHEL valuesfor heat stress exposures provides a simplified means ofestimating physiological exposure times to fuel combus-tion gas and fuel vapor pressures, with and without thepresence of limiting heat stress. Regardless, long-term,repetitive exposures to such atmospheric contaminantsmay have other far more serious consequences to thewell-being of personnel. Obviously, the elimination ofpersonnel exposures to fuel combustion gases and fuelvapors that adversely impact upon the health of person-nel should be an engineering and operational goal.Personnel exposures to fuel combustion gases and fuelvapors must be prohibited on a routine basis, emergencyexposure situations should be the only exception.
(4) Air Supply for Ventilation. One of the mostimportant factors in the design of a ventilating system isthe uniform distribution of air. Under favorable condi-tions the required air supply can be obtained by naturalventilation methods without creating objectionabledrafts. The maximal air supply should be governed bythermal requirements for maintaining the desired work-ing, living and messing space conditions indicated inSection II of this chapter. In cool or cold atmospheres,it is desirable to limit the velocity of air currents towithin the threshold of perceptibility so far as to imparta sense of freshness without producing unpleasantdrafts. The velocity at which room currents becomenoticeable varies with the dry- and wet-bulb tempera-tures, and ranges from a low of 10 fpm in cold environ-ments to about 80 fpm or higher in warm environments.In order to avoid drafty conditions, air movement incool atmospheres should be maintained at less than 50
3-21

3-11 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-12
fpm; in warm conditions it should be kept between100-200 fpm. Intermittent exposure to much highervelocities is indicated in the presence of radiant heat;however, reference should be made to the special con-siderations indicated in Section H, 3-7 (5) and (6). Fornatural ventilation it is good practice to select the pointof air entry in order to control the volume and distribu-tion. Selective entry of air through specific openings orby “infiltration” allows for thermal tempering before itreaches living or working spaces. When untempered airpasses over personnel, it can result in chilling andcomplaints of drafts. Some individuals may then de-mand increased heating of a space to the dissatisfactionof other occupants. “Foot drafts” may be due to faultyventilation or to variable vasomotor circulatory responsein the extremities. It is best managed by selective use ofsuitable clothing. In firerooms and engine rooms thepreferred minimal effective air velocity over personnel is250 fpm. Air blowing between 250-1500 fpm on thehead and shoulders will result in relatively little gains ineffective cooling, beyond 1500 fpm there will be reducedeffective cooling, while above 2080 fpm will result inheating of dry skin (See Figure 3-2).
(5) Air Supply Requirements for Respiration andElimination of Smoke and Odors. Outside air supply tospaces where light work is performed should not be lessthan 425 liters (15 cubic feet) per minute per person; or2 air changes per hour, whichever is greater. Where thework load is heavy, the outside air supply should beincreased to 566 liters (20 cubic feet) per minute perman, or 3 air changes per hour. In spaces where smokingis permitted, 850 liters (30 cubic feet) of air should beprovided per minute for each smoker. In living spaces850 liters (30 cubic feet) of air should be supplied perminute per designed occupancy; messing areas should beprovided with 566 (20 cubic feet) per minute per personeating during maximum occupancy. These are minimalair quantities for the removal of noxious odors andsmoke and are not intended as standards for the removalof potential industrial contaminants.
3-12. Assessment of Heat Stress(1) The empirical heat balance equation presented in
Section 111 summarizes the environmental and metabolicparameters which constitute an individual’s thermal loadin a given environment. Efforts to develop anall-encompassing heat stress index, that unconditionallydescribes all thermal variables in all situations, have metwith varying degrees of both success and failure. Theusefulness of a single thermometer in the measurement ofheat stress conditions is extremely limited. Engineeringsurveys of heat stress require separate readings (dry-bulb,wet-bulb, globe, and surface temperatures plus air veloci-ties) at the supply duct face (opening) and at the worklocation. Environmental physiology studies of heat stressrequire the foregoing measurements in addition to theassessment of human body temperatures and individualwork loads. The evacuation of heat strain requires all of theabove measurements as well as a worker’s heart rates,blood pressures and pre- and post-exposure body weights.
(2) Mean Radiant Temperature (mrt). In calculatingthe radiant heat balance between man and his environ-ment, one must first estimate the mean radiant temper-ature of the surroundings. This may be calculated invarious ways using the globe and dry-bulb temperatures,and the air velocity data noted above. The simplestmethod is by use of the nomogram illustrated in Figure3-7. The difference between the globe and dry-bulb
3-22
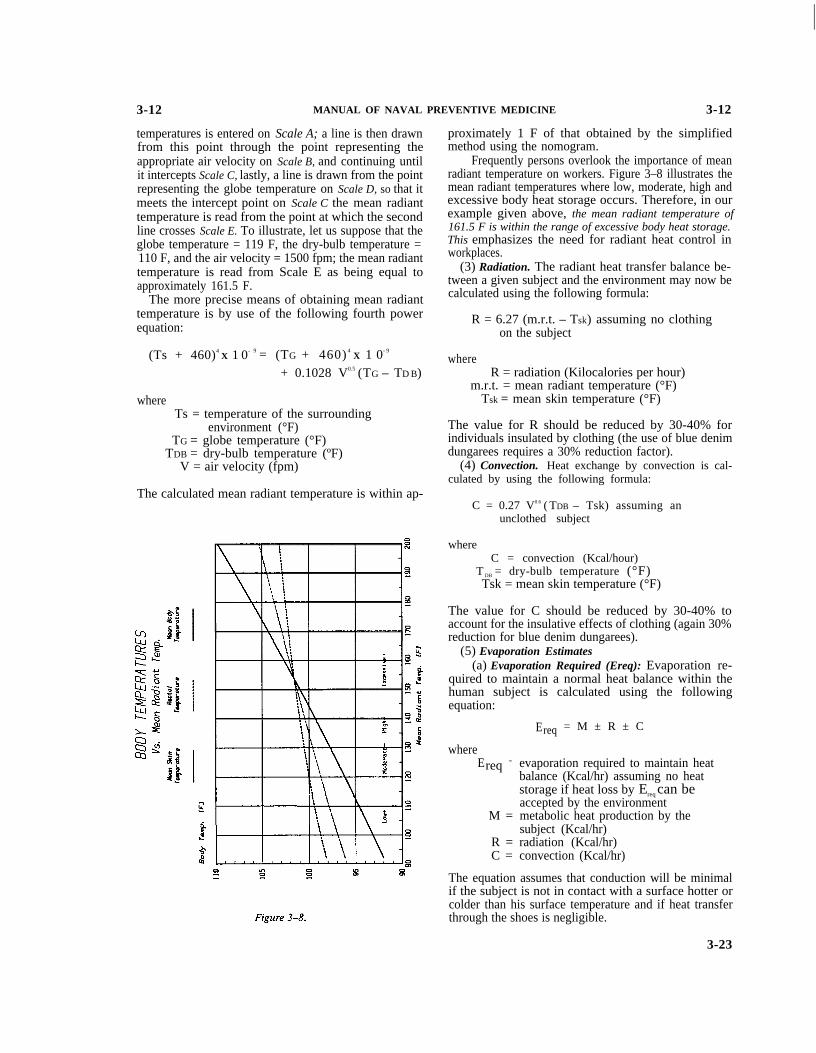
I
3-12 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-12
temperatures is entered on Scale A; a line is then drawnfrom this point through the point representing theappropriate air velocity on Scale B, and continuing untilit intercepts Scale C, lastly, a line is drawn from the pointrepresenting the globe temperature on Scale D, so that itmeets the intercept point on Scale C the mean radianttemperature is read from the point at which the secondline crosses Scale E. To illustrate, let us suppose that theglobe temperature = 119 F, the dry-bulb temperature =110 F, and the air velocity = 1500 fpm; the mean radianttemperature is read from Scale E as being equal toapproximately 161.5 F.
The more precise means of obtaining mean radianttemperature is by use of the following fourth powerequation:
(Ts + 460)4 X 1 0- 9 = (TG + 460) 4
X 1 0- 9
+ 0.1028 V0.5 (TG – TD B)
whereTs = temperature of the surrounding
environment (°F)TG = globe temperature (°F)
TDB = dry-bulb temperature (ºF)V = air velocity (fpm)
The calculated mean radiant temperature is within ap-
proximately 1 F of that obtained by the simplifiedmethod using the nomogram.
Frequently persons overlook the importance of meanradiant temperature on workers. Figure 3–8 illustrates themean radiant temperatures where low, moderate, high andexcessive body heat storage occurs. Therefore, in ourexample given above, the mean radiant temperature of161.5 F is within the range of excessive body heat storage.This emphasizes the need for radiant heat control inworkplaces.
(3) Radiation. The radiant heat transfer balance be-tween a given subject and the environment may now becalculated using the following formula:
R = 6.27 (m.r.t. – Tsk) assuming no clothingon the subject
whereR = radiation (Kilocalories per hour)
m.r.t. = mean radiant temperature (°F)Tsk = mean skin temperature (°F)
The value for R should be reduced by 30-40% forindividuals insulated by clothing (the use of blue denimdungarees requires a 30% reduction factor).
(4) Convection. Heat exchange by convection is cal-culated by using the following formula:
C = 0.27 V0.6 ( TDB – Tsk) assuming anunclothed subject
whereC = convection (Kcal/hour)
T DB = dry-bulb temperature (°F)Tsk = mean skin temperature (°F)
The value for C should be reduced by 30-40% toaccount for the insulative effects of clothing (again 30%reduction for blue denim dungarees).
(5) Evaporation Estimates(a) Evaporation Required (Ereq): Evaporation re-
quired to maintain a normal heat balance within thehuman subject is calculated using the followingequation:
whereEreq =
M =
R =C =
Ereq = M ± R ± C
evaporation required to maintain heatbalance (Kcal/hr) assuming no heatstorage if heat loss by Ereq can beaccepted by the environmentmetabolic heat production by thesubject (Kcal/hr)radiation (Kcal/hr)convection (Kcal/hr)
The equation assumes that conduction will be minimalif the subject is not in contact with a surface hotter orcolder than his surface temperature and if heat transferthrough the shoes is negligible.
3-23

3-12 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-12
(b) Maximum Evaporative Capacity (Emax): Themaximum amount of heat, lost by evaporation, whichcan be accepted by the environment (maximum evapo-rative capacity of the environment) is calculated fromthe following equation:
Emax = 1.01 V0.6 (42 – VPa)
whereEm a x
v =v Pa =
42 =
maximum evaporative capacity (Kcal/hr)air velocity (fpm)Partial vapor pressure of the environ-ment (mm Hg.) at the combined dry-bulb and wet-bulb temperatures.vapor pressure at the skin of thesubject assuming a mean skin tem-perature of 95° F; this figure willdiffer by approximately 1.3 mm Hgfor each 1°F change in the mean skintemperature from 95ºF.
The value for Emax should be reduced by 30-40% toaccount for the insulative effect of clothing (blue denimdungarees require a 30% reduction factor).
(6) Heat Stress Index (Belding-Hatch): The HeatStress Index (HSI) is calculated as the ratio of theEvaporation Required (Ereq) to the Maximum Evapora-tive Capacity (Emax):
HSI = Ereq X 100Emax
The HSI is an expression of heat load in terms of theamount of sweat which needs to be evaporated in orderto maintain heat balance. The index compares theamount of heat lost by evaporative cooling from com-pletely wetted skin to the maximum evaporative capacityof the environment. The HSI was considered useful insubjectively estimating metabolic heat production dur-ing different categories of physical activity. Estimates ofvarious types of metabolic rates during different physicalactivities are given in Table 3-5.
The Heat Stress Index was originally intended forapplication among men working 8-hour shifts in civilianindustry. Investigation, however, has shown that a neg-ative ( – ) index occurs when the vapor pressure of theskin is lower than the partial vapor pressure of theenvironment; this can happen even when the mean skintemperature is in the range of 101-110 F. Thus, althougha negative HSI theoretically indicates cold strain (SeeTable 3-6) it can, in fact, occur in the presence of severeheat strain. The limitations of the HSI required devel-opment of a more reliable means of assessing maximumsafe exposure time in the presence of heat stress. A morereliable exposure limit index has been developed and isdiscussed later in this section under the heading ofPhysiological Heat Exposure Limits (PHEL). Notwith-standing the contradictory nature of the HSI, the equa-tions given in the preceding text are of use in partitioningthe avenues of heat loss and gain between the subjectand the environment.
3-24
(7) Wet-Bulb Globe Temperature Index (WBGT). Asderived, the WBGT Index was unique in that it took intoaccount the four physical variables of the thermalenvironment (air temperature, humidity, radiant heatand air movement). The simplicity of the approach wasthat one need not perform direct measurement of airvelocity and that the globe thermometer integrates radi-ant heat and convective heating or cooling into onevalue. [Note: The globe temperature is neither radiantheat by itself nor what is known as the mean radiant
Table 3-5. Identification Of Approximate MetabolicRates
Physical Activity
a) Sitting
Moderate arm & trunk movement(e.g., typing, drafting, driving a carin light traffic)
Moderate arm & leg movement(e.g., general laboratory work, slowmovement about an office)
Heavy arm & leg movement (e.g.,driving a car in moderate traffic)
b) Standing
Light work at machine or bench,mostly arms
Light work at machine or bench,some moving about (e.g., using atable saw, driving a truck in lighttraffic)
Moderate work at machine orbench, some walking about (e.g.,replacing tires, driving a car inheavy traffic)
c) Walking About, with ModerateLifting or Pushing (e.g., driving atruck in moderate traffic, scrubbingin a standing position)
d) Intermittent Heavy Lifting, Pushingor Pulling (e.g., sawing wood byhand, calisthenic exercise, pick andshovel work)
e) Hardest Sustained Work
AverageMetabolic RateKCal*m -2*hr-1
68
82
99
82
99
119
164
238
300

3-12 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-12
temperature; the globe temperature value is a compositeof radiant and convective heat transfers. ]
Initial practical applications of the WBGT Index
Table 3-6. Physiological Implications Of The HSI
HSI
-20 to-10
0
+ 10 to+30
+40 to+60
+70 to+90
+ 100
Above+ 100
[Note:
(Belding-Hatch)
Physiologic and Behavioral Implications
Mild cold strain. (See implication of negative HSIabove) This condition frequently exists in areaswhere men recover from exposure to heat.
No thermal strain.
Mild to moderate heat strain. Where a job involve!higher intellectual function, dexterity, or alterness,subtle to substantial decrements in performancemay be expected. In performance of heavy physicswork, little decrement unless ability of individualsto perform such work under no thermal strain ismarginal.
Severe heat strain, involving a threat to healthunless personnel are physically fit. Break-in periodrequired for those not previously acclimatized.Some decrement in performance of physical workis to be expected. Medical selection of personneldesirable because these conditions are unsuitablefor those with cardiovascular or respiratoryimpairment or with chronic dermatitis. Theseworking conditions are also unsuitable foractivities requiring sustained mental effort.
Very severe heat strain. Only a small percentage ofthe population may be expected to qualify for thiswork. Personnel should be selected (a) by medicalexamination, and (b) by trial on the job (afteracclimatization). Special measures are warranted toassure adequate water and salt intake (See SectionIII). Amelioration of working conditions by anyfeasible means is highly desirable, and may beexpected to decrease the health hazard whileincreasing efficiency on the job. Slight“indisposition” which in most jobs would renderworkers unfit for this exposure.
The maximum strain tolerated by fit, acclimatizedyoung men for 8-hour exposures.
Overstrain, for 8-hour exposures. Tolerance ofbrief exposures will depend not on the amount bywhich the HSI exceeds + 100 but on the rate ofheat accumulation by the body.
In steam, diesel and nuclear shipboard situations thelevel of heat stress frequently exceed physiological limits for atleast 4-hour exposures. Therefore, one must consider a com-posite of heat stress and strain, behavioral, other physiologicaland time factors before application of the HSI to worksituations less than the 8-hour design criteria.]
equations were to estimate ranges of heat stress thatwarranted decreasing physical activity in order to mini-mize incidence of heat injuries outdoors. It has beenassumed by many persons over at least the last 20 yearsthat the two-variable combination of wet and dry bulbtemperatures applies indoors, while the three-variableequation applies only outdoors. In reality, there are noless than eight equations for obtaining the WBGTIndex; therefore, selection of the most appropriateWBGT Index equation became a serious matter in termsof the limitations of some of the equations.
From 1963-1968, volumes of data were reviewed andcompared with the Navy Bureau of Ship files. Literaturesearches and computer plotting of all available data indi-cated that maximum utility, for both engineering andenvironmental physiology purposes, would be obtained byuse of the below WBGT equation. This was a majorchange from the comfort assessment concept of EffectiveTemperature and use of the WBGT Index.
WBGT = [(0.7 * Shielded Psychometric Wet Bulb)+ (0.2 * Matte Black Globe Temp.)+ (O. 1 * Shielded Dry Bulb Temp.)]
Extremely complex heat-work physiology experi-ments were conducted between 1968– 1975 in a largenumber of heat stress and work situations ashore andafloat. Seventeen physiological factors were employed,along with environmental variables and a wide range ofwork loads, to develop comprehensive physiologicalheat exposure limits criteria. Therefore, combining thegiven WBGT equation with the physiological responsesled to development of the Physiological Heat ExposureLimits (PHEL). [Refer to: National Bureau of Stan-dards, Special Pub. 491, pp 65-92, September 1977.]
Application of WBGT equations other than thatgiven above for determining PHEL values is an ex-tremely dangerous practice. There is too great a chanceof being wrong in terms of physiologically safe butreversible limits of human heat stress exposures withother WBGT equations. Obviously one may find sometheoretical situations where it makes no difference whichequation is applied, however, for practical purposes,maximizing the utility of environmental data for manyconstructive and corrective engineering and environ-mental physiologic purposes, minimizing the risks tohumans yet obtaining the longest safe stay times, theremust be consistency in applying the above WBGTequation. The Navy heat stress meter is designed to beconsistent with use of the given WBGT equation.
Only by use of above given WBGT equation, provid-ing the raw data used for the calculations, including theair velocity over man, indicating what clothing is wornand providing sufficient information whereby humanmetabolic rates can be predicted will permit maximumanalyses of the environmental physiologic situation.Whenever possible all available information should beprovided ! Furthermore, extreme care should be taken tospecify the presence or absence of air contaminants thatmay combine to have either a positive or negative impactupon humans at even low levels of heat stress. One mustbe continually aware of the fact that it is impossible for
3-25

3-12 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-12
humans to be exposed to only one variable simulta-neously in a non-laboratory environment. It is essentialto think in terms of dynamic situations where multipleenvironmental stresses result in various physiologicchanges that occur in compensable or intolerable situa-tions. One must know as many possible individualvariables to constructively analyze the work situation interms of the physiological well-being of workers.
(8) Physiological Heat Exposure Limits (PHEL). U.S.Navy Physiologic Exposure Limits (PEL) were firstestablished in 1971, however, in 1973 the EnvironmentalProtection Agency circulated a series of Public ExposureLimits (PEL) covering a broad range of exposure limitswhich did not include heat stress. Furthermore, aware ofthe Navy’s PEL for heat stress, the National Institute ofOccupational Safety and Health (NIOSH) publishedtheir Permissible Exposure Limits (PEL) for heat stressin September 1973. In order to avoid confusion regard-ing the acronyms PEL the Navy, in December 1973,adopted the more descriptive title “Physiological HeatExposure Limits” (PHEL). These criteria consisted ofthe previously published Physiological Exposure Limitsof 1971 with an additional curve for heavy work as incasualty control. The Navy limits recognize that underconditions of maximum work and heat stress the heatstrain will be readily apparent, but that it will bereversible; NIOSH Permissible Exposure Limits, on theother hand, were designed to restrict deep body temper-ature rises to a maximum of 100.4 F. In numerous worksituations it is unrealistic to limit work at a rectaltemperature of 100.4 F.
Compliance with the Navy’s PHEL takes into ac-count the multiple physiological factors relative to thewelI-being of personnel. The PHEL applies to greaterthan 95070 of the population, as there will always besomeone who may occasionally exceed the limits beforeincurring heat exhaustion or heat stroke. For the pur-pose of comparison, exceeding the PHEL is the same asstretching a rubber band close to its break point; sooneror later the rubber band is going to break. Seriouspersonnel heat injuries can be expected whenever thePHEL are exceeded, therefore, stretching the rubberband close to its limits too many times is courtingdisaster.
(a) Criteria for PHEL Chart Development. Thedevelopment of the PHEL curves entailed considerableheat stress research among personnel whose ages rangedfrom 18-40 years. Physiologic measurements includednine cardiovascular and four respiratory functions andrelated them to the total cardiovascular reserves. Threeinternal body temperatures and 10 skin temperatureswere serially recorded. The criteria for determiningmaximum safe physiological exposures was based upona composite of the above parameters (Refer to NationalBureau of Standards, Special Publication 491, pp 65-92,September 1977). The absence of muscle damage undervariable conditions of heat stress was verified by enzymeassay. In addition, subjects were monitored for theoccurrence of hyperventilation and changes in mentalstatus, particularly for euphoria. The measurements
3-26
were made before, during and following sustained phys-ical work in controlled heat stress conditions. Thesefindings were compared with a wide range of environ-mental conditions aboard ships from 197 1-1976; thefield data, using over 200 healthy Navy personnel,compared equally with the involved laboratory studies.
Time-weighted-means were calculated for bothmetabolic heat production and WBGT exposures. Thisallowed for the subsequent development of maximumheat exposure limits which were described by a family ofsix curves that fit power regression equations. Figure 3-9illustrates the six major PHEL curves.
(b) Time Weighted Mean Metabolic Rates (twin).The “time-weighted-mean” (Twin) concept must be ap-plied in unique situations not addressed as part ofPhysiological Heat Exposure Limits (PHEL) for ship-board applications. PHEL Curve Selection Tables forshipboard applications have taken into account thevarious work rates of personnel during various types ofand lengths of time each activity is performed (normalwatch, casualty control exercise and repair involvingheavy work), therefore, do not apply the Twm concept tothose situations. In cases where new or additional Twmsituations occur it is essential to determine both the TwmMetabolic Rate, and may be necessary to determine the
Figure 3-9.
3-12 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-12
Twm WBGT value and calculate the Twm PHEL Spe-cific value.
(c) Procedure for Time-Weighted-Mean Applica-tions:
1. Identify the metabolic rates (MR) for each segmentof the total time under consideration, using Table3-5.
2. Calculation of Twm Metabolic Rate
Twm MR = [(MR1 * tl) + (MR2 * t2) + . . . + (MRn* tn)] / [tl + t2 + . . . + tn)]
where;Twm MR =
MR1 =
tl =MR2 =
t2 =MRn =
time-weighted-mean metabolic rate(KCal*m -2*hr-1)metabolic rate (Kcal*m -2*hr –1) work forexposure time #1length of time (in decimal hours) for MR1metabolic rate (Kcal*m –2*hr -1) work forexposure time #2length of time (in decimal hours) for MR2metabolic rate (Kcal*m –2*hr –1) work forexposure time #n
tn = length of time (in decimal hours) for MRn3. Relationship of Twm Metabolic Rates to PHEL
Curves4. Identification Of Appropriate WBGT Curves
If the Twm MR from #2 above is close to a TwmMR in #3 above, then proceed with Table 3-8below in selecting the appropriate PHEL Curve:
5. Determination of Twm WBGTDetermine WBGT values for each of the locations
were the Twm Metabolic Rates apply. Then apply theWBGT values and times for the respective Twm Meta-bolic Rates to the equation given in Step #6 below.
6. Calculation of Twm WBGT Values
Twm WBGT = [(WBGT1 * tl) + (WBGT2 * t2) + . . .+ (WBGTn * tn)] / [tl + t2 + . . . +tn)]
where;Twm
WBGT = time-weighted-mean WBGT Index degreesF
WBGT1 = WBGT at time #1tl = length of time (in decimal hours) for
WBGT1WBGT2 = WBGT at time #2
t2 = length of time (in decimal hours) forWBGT2
Table 3-7
PHEL Curve Twm Metabolic Rate
I 76II 86111 96Iv 106v 116VI 126
Table 3-8
Type of Physical Activity
Sitting
Moderate arm & trunkmovement
Moderate arm & legmovement
Heavy arm & legmovement
Standing
Light work at machine orbench, mostly arms
Light work at machine orbench, some walkingabout
Moderate work atmachine or bench, somewalking about
Walking About, withModerate Lifting orPushing
Intermittent Heavy Lifting,Pushing or Pulling
Hardest Sustained Work
Lowest Metabolic Rate
Average & HighMetabolic Rate
PHEL Curve Selection TablesFor No. Minutes Work vs.
No. Minutes Rest
NOTES:1. Do Not Attempt To Apply The PHEL Curves and/or Work
Rates In Those Situations Indicated As “NA” (Not Applicable)Above. If the amount of work is underestimated it is likely thatpersonnel systemic heat injuries will be incurred.
2. If the types of physical activity are more mixed than notedabove, then there is no alternative but to resort to calculationsusing the TWM concept.
3. TWM metabolic rate calculations require restarting with Step#l above and selecting the metabolic activity for the specifictype of work given above, as well as the length of time thatapplies to the selected metabolic rate situation. Then apply theselected metabolic rate and time values to the below calcula-tions. Do likewise for the WBGT and respective time values.
3-27

3-12 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-13
WBGTn = WBGT for exposure time #ntn = length of time (in decimal hours) for
WBGTn7. Calculation of Twm Approximated PHEL Values
Twm Approximated PHEL = Antilog [(1/0. 13) *(A-Log Twm WBGT)] = hours
A = Log [111.0461 + (0.2377 * Twm MR) –(0.0027 * Twm MR2)] WBGT = degrees FPHEL values greater than 8 hours should beread as “ >8 hours” for the upper limits.
8. Reduction of PHEL Times Due to Fuel Combus-tion Gases and/or Pre-Combustion Fuel Vapors
PHEL times (hours) must be reduced by 65.6070when there is the presence of fuel combustiongases and/or pre-combustion fuel vapors.
(d) Relationships of PHEL Curves to Rest/WorkRatios. The laboratory data which led to the generationof the PHEL curves allowed for the development of arelated series of rest/work ratios for different degrees ofphysical activity. These relationships are illustrated inTable 3-8 above.
(e) Precautions. It must be emphasized that thePhysiological Heat Exposure Limits are maximum al-lowable standards and that they should be applied onlyin cases of short-term work exposures of up to 8 hoursduration. The limits presume that no prior heat injury ispresent and that no cumulative heat fatigue exists priorto re-exposure.
(9) Other Indices. Other indices of heat stress andstrain are available but are of limited use. The value ofany index is dependent upon the nature and extent of theproblem, the availability of resources, and the experi-ence of local personnel in regard to heat stress analyses.Consultation will be provided to commands if inquiriesare directed to the Naval Medical Command throughofficial channels.
(10) Information Regarding the “Wet Globe Temper-ature” ( WGT) Index. The WGT Index (“Botsball”) hasbeen used in a number of situations, however, it is notappropriate to utilize the WGT to determine Physiolog-ical Heat Exposure Limits. Army meteorological studieshave shown that in identically the same environmentalconditions no two WGT thermometers indicated thesame value, there was a marked bleaching of the blackcloth coverings after one month in use, the cloth cover-ings had various degrees of bristle formations, thecoverings occasionally did not wet uniformly, the waterreservoirs frequently need refilling at one hour intervals,WGT units required at least 5 minutes of stabilizationafter replenishing water in the reservoir, and the WGTvalues do not permit availability of essential data (dry-and wet-bulb and globe temperatures) for thermal anal-yses. Since 1971 there have been 8 equations publishedthat claim to permit conversion of WGT values toWBGT values, there is a tremendous disparity betweenthe products from these equations. Application of avail-able data, with and without conversion to estimatedWBGT values, to the PHEL chart has yielded unrealisticsafe exposure times. There have been similar unaccept-able findings regarding the use of WGT values for
3-28
estimating the amount of water needed when personnelperform work. Use of the WGT units may be expedientbut application of the WGT values has extremely limitedvalue. NAVMEDCOM has not approved the use of theWGT (“Botsball”) units.
(11) Predicting Onset Of Mental Impairment Due ToHeat Stress. In 1972 the Department of Health, Educa-tion and Welfare (HSM 72-10269, 1972, pg 188) pub-lished a curve entitled “Upper Limits of Exposure forUnimpaired Mental Performance”. Figure 3-10 illus-trates the curves for detectable onset of mental impair-ment as a function of the same metabolic rates for thePHEL curves; the decrements of cardiovascular reservealso have been taken into account. It is readily apparent,by comparing Figure 3-9 (in Article 3-12) with Figure3-10, that mental impairment begins much earlier and atlower heat stress conditions than persons reaching theirphysiological exposure limits. In heat stress conditions itcan be expected that mental acuity will have beenimpaired long before workers reach their physiologicallimits, physical performance decays in a similar fashionas that shown for mental impairment but in a differenttime frame.
3-13. Practical Heat Stress Standards(1) General. Sound health, physical conditioning for
the specific task, and adequate rest and nutrition areessential in minimizing the effects of thermal stress.Drinking water should be unrestricted and readily avail-able. Threshold WBGT values for the hottest 2-hour
Figure 3-10.

3-13 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-13
period of industrial-type work shifts should be deter-mined using the work load of personnel as described inSection 3-8 and Table 3-5. The threshold WBGT valuesversus work levels are repeated below:
Work Level WBGT (F)
Light 86Moderate 82Heavy
(2) Limitations on Physical Exertion. During the first12 weeks of hot weather training the limits of physicalexertion should be determined by the degree of environ-mental heat stress, metabolic heat production, the statusof acclimatization, and the physical status of individualpersonnel. The availability of adequate drinking waterand the frequency of rest periods should also receiveconsideration. Individuals who are over 35 years of age,those who are obese or whose nutritional status is poor,and those with evidence of chronic or acute cardiopul-monary dysfunction should be medically screen prior tophysical exertion under thermal stress. Table 3-9 out-lines the recommendations for different physical activi-ties at five WBGT Index ranges. It applies especially topersonnel during training and recreational exercises inhot weather. The below table is not a substitute for thePHEL curves nor is it possible to comply with the tablein combat situations.
(3) Heating Standards.(a) Surface Vessels. The recommended standards
for heating aboard surface vessels imply an optimumdry-bulb temperature of 70 F for the following spaces:
(1) Living compartments, recreation and messingspaces.
(2) Medical and dental spaces.(3) Office and control spaces.
Humidity control is not usually provided. Special re-quirements should be reviewed by the Medical Depart-ment before any action is taken.
(b) Submarines. Aboard submarines environmentalconditions are more closely controlled. Heating stan-dards should fall within the optimal limits of 79 F DB,59 F WB, 50% RI-I with 63 F WBGT. These standardsapply to:
(1) Living compartments, recreation and messingspaces.
(2) Medical and dental spaces.(3) Office and control spaces.
(c) Other Compartments. Excluding the abovenoted spaces and those associated with engineeringpropulsion components, inside working spaces are usu-ally maintained at lower temperatures during the winter.In these spaces, the control of personal warmth isfacilitated by the proper use of available clothing.
(4) Ventilation and Air-Conditioning(a) Surface Vessels. Ventilation and air-conditioning
standards for surface vessels should include the follow-ing upper limits for physical comfort and functionalwell-being: 80 F DB, 68 F WB, 55070 RH (14.3 Torr VP),with 72 F WBGT Index. The recommendations appIy to
the same spaces noted for the heating standards above.In addition, air-conditioning and ventilation are re-quired for manned electronics spaces and compartmentswith equipment sensitive to changes in temperature andhumidity.
(b) Submarines. The standards for comparablespaces aboard submarines are as follows: 80 F DB, 67 FWB, 50% RH, with 71 F WBGT.
(c) Other Compartments. Laundries, galleys, scul-leries, passages not opening directly on weather decks,and areas above food serving lines present situations inwhich it is difficult to contain heat and humidity withinspecific narrow limits. Standards for these areas, how-ever, should allow for physical health and well-being; theWBGT Index should not exceed 78 F during normaloperations. In addition, ventilation and cooling of suchspaces should be consistent with the information givenin Articles 3-6 and 3-7 (Section H) and Article 3-11(Section IV) of this chapter. Design criteria presented inTable 3-1 (Article 3-7, Section 11) must be considered inplanning ventilation for firerooms, engine rooms, laun-dries, sculleries, galleys and steam catapult launch con-
Table 3-9. WBGT as a Guide in Regulating Intensity of
WBGT Index[F]
Less Than 82
82-84.9
85-87.9
88-88.9
90 andAbove
Physical Exertion During First 12 TrainingWeeks in Hot Weather*
Flagcolor
Blue
Green
Amber
Red
Black
Intensity of Physical Exercise
Extremely intense physical exertionmay precipitate heat exhaustion orheat stroke, therefore, caution shouldbe taken.
Discretion required in planning heavyexercise for unseasoned personnel.This is a marginal heat stress limitfor all personnel.
Strenuous exercise and activity (e.g.,close order drill) should be curtailedfor new and unseasoned personnelduring the first 3 weeks of heatexposure.
Strenuous exercise curtailed for allpersonnel with less than 12 weekstraining in hot weather.
Physical training and strenuousexercise suspended for all personnel(excludes operational commitmentnot for training purposes).
* This table must not be used in lieu of the PhysiologicalHeat Exposure Limits (PHEL). The time-weighted-mean met-abolic rates applicable to Table 3-8 are considerably higher thanthose for PHEL Curves. For an analogy, Table 3-8 would applyto Marine Corps personnel in the field, whereas the PHELconcept applies to industrial settings.
3-29

3-13 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-13
trol rooms. In situations where the heat stress is excessiveand ventilation or cooling cannot be improved, thePhysiological Heat Exposure Limits need to be em-ployed to minimize the incidence of personnel heatinjuries.
(5) Shipboard Heat Stress Situations(a) Physiological Heat Exposure Limits (PHEL)
Chart. The PHEL chart illustrated in Figure 3-9 (Article3-12) provides the relationships of various metabolicrates, heat stress and maximum safe exposure times.Applicability of PHEL curves to routine watches andcasualty control exercises are given in Table 3-10 below,and the PHEL times for Figure 3-9 and Table 3-10PHEL curves are given in Table 3-11; where there is noapparent presence of fuel combustion gases (or “stackgas”) and/or fuel vapors. In all given situations the Twmmetabolic rates have been utilized, whereby the variedactivities (including movements about the spaces) andlengths of time for the various activities have been takeninto account. For Remaining Safe Stay Time situations,where different heat stress conditions, actual exposuretimes and/or recovery times apply, see Section (5)(b)below. When it is apparent that fuel combustion gases(or “stack gas”) and/or fuel vapors are present, usePHEL times given in Table 3-12.
Table 3-10. Physiological Heat Exposure Limit CurveGeneral Applicability
* Casualty
Personnel RoutineWatch Control
Exercise
Section 1. Steam Propelled ShipsA. Fire Room:
1. Boiler Tech. of the Watch(BTOW) II II
2. ABC Console Operator I I3. Upper Levelman II III4. Lower Levelman III IV5. Burnerman II III6. Messenger III IV
B. Engine Room: [IncludingNuclear]I. Engineering Officer of the
Watch [EOOW] I I2. Machinist Mate of the
Watch [MMOW] II III3. Throttleman I I4. Electrician Mate of the
Watch [EMOWJ I I5. Upper Levelman II III6. Lower Levelman II III7. Evaporator Watch I Not
Applicable8. Messenger III IV
C. Auxiliary Spaces [CV’S andFF 1052’s]:
1. Upper Levelman II II
2. Lower Levelman II IID. Steam Catapult Launch
Control Room:1. All Watch Personnel II II
Section 11. Diesel Propelled ShipsA. Engineering Officer of the
Watch [EOOW] I IB. Petty Officer of the Watch
[POOW] II IIIC. Electrician Mate of the
Watch [EMOW] I ID. Throttleman I IE. Repair Electrician I IF. Ship’s Service Diesel
Generator Watch I IG. Boiler Watch I 1H. Evaporator Watch II I1. Oiler/Messenger III IV
Section III. Gas TurbinePropelled Ships
A. All Engineering WatchPersonnel I II
Section IV. All Ships andSubmarines
A. Engineering CasualtyControl Evaluation Team Not[ECCET] Applicable II
B. Roving Watch Personnel III IIIC. Laundry Personnel III Not
ApplicableD. Scullery Personnel V Not
ApplicableE. Galley and Food Serving Not
Line Personnel II ApplicableF. Fleet Training Group
Instructors and OtherOff-Ship EngineeringObservers I II
G. Personnel ConductingHeavy Repairs or OtherStrenuous Work VI VI
* The work rate during Casualty Control Exercise is muchless than that needed for repair involving heavy work. DifferentPHEL Curve selections are required for different work ratesduring the Exercise Phase, however, all heavy work situationsrequire use of PHEL Curve VI.
(b) Remaining Safe Stay Times. There are a numberof situations where it is necessary to estimate theremaining safe stay times relative to various heat stressconditions, different work levels and/or to account forrecovery periods. Generally this is a complex task,however, a simplified approach is given in the belowequation:
RSSt = [(1 – (Et – R/2)) / Atl] * At2
where:
3-30
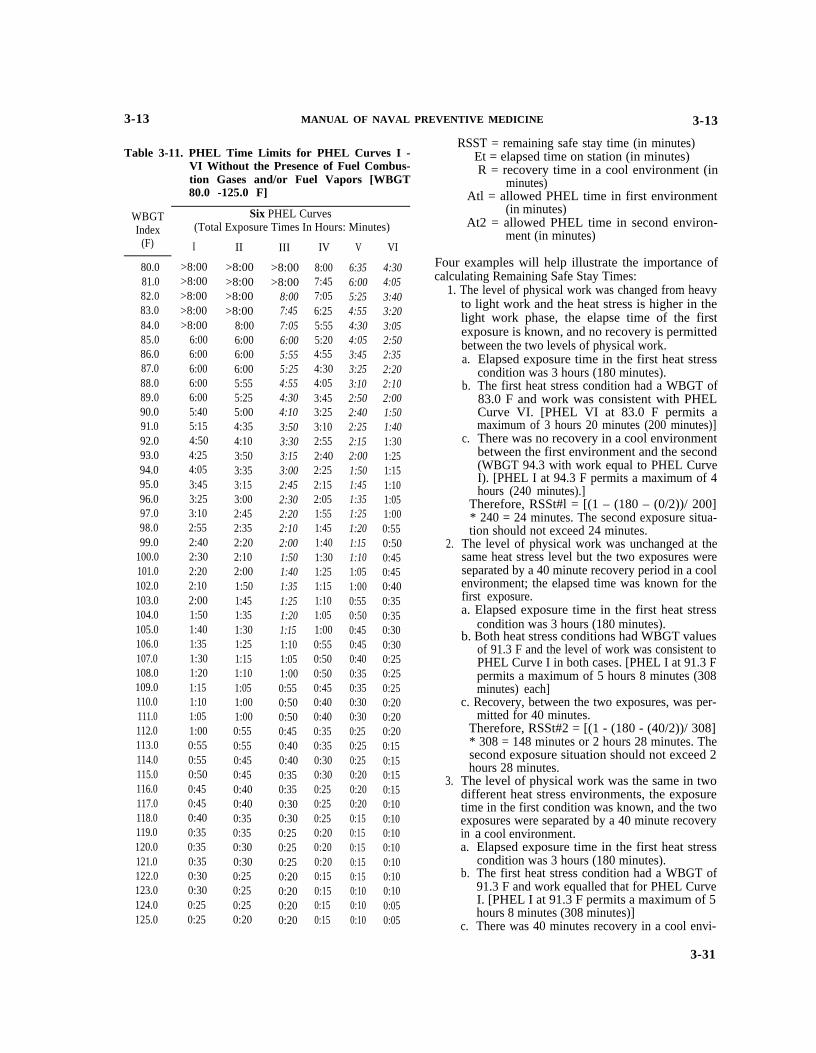
3-13 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-13
WBGTIndex
(F)
80.081.082.083.084.085.086.087.088.089.090.091.092.093.094.095.096.097.098.099.0
100.0101.0102.0103.0104.0105.0106.0107.0108.0109.0110.0111.0112.0113.0114.0115.0116.0117.0118.0119.0120.0121.0122.0123.0124.0125.0
Table 3-11. PHEL Time Limits for PHEL Curves I -VI Without the Presence of Fuel Combus-tion Gases and/or Fuel Vapors [WBGT80.0 -125.0 F]
Six PHEL Curves(Total Exposure Times In Hours: Minutes)
I
>8:00>8:00>8:00>8:00>8:00
6:006:006:006:006:005:405:154:504:254:053:453:253:102:552:402:302:202:102:001:501:401:351:301:201:151:101:051:000:550:550:500:450:450:400:350:350:350:300:300:250:25
II
>8:00>8:00>8:00>8:00
8:006:006:006:005:555:255:004:354:103:503:353:153:002:452:352:202:102:001:501:451:351:301:251:151:101:051:001:000:550:550:450:450:400:400:350:350:300:300:250:250:250:20
III
>8:00>8:00
8:007:457:056:005:555:254:554:304:103:503:303:153:002:452:302:202:102:001:501:401:351:251:201:151:101:051:000:550:500:500:450:400:400:350:350:300:300:250:250:250:200:200:200:20
IV
8:007:457:056:255:555:204:554:304:053:453:253:102:552:402:252:152:051:551:451:401:301:251:151:101:051:000:550:500:500:450:400:400:350:350:300:300:250:250:250:200:200:200:150:150:150:15
V
6:356:005:254:554:304:053:453:253:102:502:402:252:152:001:501:451:351:251:201:151:101:051:000:550:500:450:450:400:350:350:300:300:250:250:250:200:200:200:150:150:150:150:150:100:100:10
VI
4:304:053:403:203:052:502:352:202:102:001:501:401:301:251:151:101:051:000:550:500:450:450:400:350:350:300:300:250:250:250:200:200:200:150:150:150:150:100:100:100:100:100:100:100:050:05
RSST = remaining safe stay time (in minutes)Et = elapsed time on station (in minutes)R = recovery time in a cool environment (in
minutes)Atl = allowed PHEL time in first environment
(in minutes)At2 = allowed PHEL time in second environ-
ment (in minutes)
Four examples will help illustrate the importance ofcalculating Remaining Safe Stay Times:
1. The level of physical work was changed from heavyto light work and the heat stress is higher in thelight work phase, the elapse time of the firstexposure is known, and no recovery is permittedbetween the two levels of physical work.a.
b.
c.
Elapsed exposure time in the first heat stresscondition was 3 hours (180 minutes).The first heat stress condition had a WBGT of83.0 F and work was consistent with PHELCurve VI. [PHEL VI at 83.0 F permits amaximum of 3 hours 20 minutes (200 minutes)]There was no recovery in a cool environment
2.
3.
between the first environment and the second(WBGT 94.3 with work equal to PHEL CurveI). [PHEL I at 94.3 F permits a maximum of 4hours (240 minutes).]
Therefore, RSSt#l = [(1 – (180 – (0/2))/ 200]* 240 = 24 minutes. The second exposure situa-tion should not exceed 24 minutes.
The level of physical work was unchanged at thesame heat stress level but the two exposures wereseparated by a 40 minute recovery period in a coolenvironment; the elapsed time was known for thefirst exposure.a. Elapsed exposure time in the first heat stress
condition was 3 hours (180 minutes).b. Both heat stress conditions had WBGT values
of 91.3 F and the level of work was consistent toPHEL Curve I in both cases. [PHEL I at 91.3 Fpermits a maximum of 5 hours 8 minutes (308minutes) each]
c. Recovery, between the two exposures, was per-mitted for 40 minutes.
Therefore, RSSt#2 = [(1 - (180 - (40/2))/ 308]* 308 = 148 minutes or 2 hours 28 minutes. Thesecond exposure situation should not exceed 2hours 28 minutes.
The level of physical work was the same in twodifferent heat stress environments, the exposuretime in the first condition was known, and the twoexposures were separated by a 40 minute recoveryina.
b.
c.
a cool environment.Elapsed exposure time in the first heat stresscondition was 3 hours (180 minutes).The first heat stress condition had a WBGT of91.3 F and work equalled that for PHEL CurveI. [PHEL I at 91.3 F permits a maximum of 5hours 8 minutes (308 minutes)]There was 40 minutes recovery in a cool envi-
3-31

3-13 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-13
ronment between the first environmental expo-sure, and the second exposure at a WBGT of94.3 F with work equivalent to PHEL Curve I.[PHEL Curve I at WBGT of 94.3 F permits 4hours (240 minutes) stay time]
Therefore, RSSt#3 = [(1 – (180 – (40/2))/ 308]* 240 = 115 minutes or 1 hour 55 minutes. Thesecond exposure situation should not exceed 1hour 55 minutes.
4. The level of physical work changed from an inter-mediate level to lighter level and the heat stress wasconsiderably higher in during the second exposure.Both the elapsed time for the first exposure and therecovery time between exposures were known.a. Elapsed exposure time in the first heat stress
condition was 3 hours 15 minutes (195 minutes)b. The first heat stress condition had a WBGT of
87.7 F and work was consistent with PHELCurve IV. [PHEL IV at 87.7 F permits amaximum of 4 hours 15 minutes (255 minutes)]
c. There was 50 minutes recovery in a cool envi-ronment between the first exposure and thesecond, the work during the second exposurewas equivalent to PHEL Curve II, but theWBGT value was 100.9 F for the second expo-sure. [PHEL 11 at 100.9 F allows a maximum of2 hours 5 minutes (125 minutes)]
Therefore, RSSt#4 = [(1 – (195 – (50/2))/ 255]* 125 = 42 minutes. The second exposure situa-tion should not exceed 42 minutes.
NOTE: In application of the Remaining Safe Stay Timeequation it must be acknowledged that somecumulative fatigue will take place.
(c) Presence of Fuel Combustion Gases and/or FuelVapors. As indicated in Article 3-11(3), the apparentpresence of fuel combustion gases (or “stack gas”)and/or fuel vapors has a deleterious impact upon work-ers. To minimize excessive exposures it is possible toutilize the PHEL Curves provided the stay times arereduced 66%. Table 3-12 provides the reduced PHELvalues compared with those given in Table 3-11.
(d) Alternative Options for Regulating Heat Stress.It is sometimes impossible to control environmental heatwithin the specified limits in the face of increasedoperational demands. Alternative measures may there-fore be useful in limiting heat stress and reducingthe incidence of heat casualties. Several options arepossible:
(1) Insulate the source of heat.(2) Ventilation with cool air (Section II of this
chapter).(3) Reduce humidity (partial water vapor content)
by stopping steam leaks and venting steam to theoutside.
(4) Provide clothing which will maximize evapo-rative cooling.
(5) Limit exposure time (refer to PHEL Chart).(6) Avoid cumulative fatigue; maintain overall
physical health.
3-32
(7) Eliminate the presence of fuel combustiongases and fuel vapors.
(8) Automate and isolate operations which gen-erate excessive heat (not always feasible).
(6) Compressed Air and Vortex Cooling. Compressedair and vortex-type cooling methods present individual-ized assets and liabilities. Plans to utilize these tech-niques should be reviewed by the Naval Medical Com-mand prior to their operation/ use. The subjective senseof well-being afforded by these methods is not alwayssynonymous with the maintenance of object physiologic
Table 3-12. PHEL Time Limits for PHEL Curves I -VI With the Presence of Fuel CombustionGases and/or Fuel Vapors [WBGT 80.0-
WBGTIndex
(F)
80.081.082.083.084.085.086.087.088.089.090.091.092.093.094.095.096.097.098.099.0
100.0101.0102.0103.0104.0105.0106.0107.0108.0109.0110.0111.0112.0113.0114.0115.0
115.0 F]
Six PHEL Curves(Total Exposure Times In Hours: Minutes)
I
4:504:254:003:403:203:002:452:302:202:051:551:451:351:301:201:151:101:051:000:550:500:450:400:400:350:350:300:300:250:250:250:200:200:200:150:15
II
4:153:503:303:102:552:402:252:102:001:501:401:301:251:201:101:051:000:550:500:450:450:400:350:350:300:300:250:250:250:200:200:200:150:150:150:15
III
3:303:102:552:402:252:102:001:501:401:301:251:151:101:051:000:550:500:450:400:400:350:350:300:300:250:250:200:200:200:150:150:150:150:150:100:10
IV
2:552:402:252:102:001:501:401:301:251:151:101:051:000:550:500:450:400:400:350:300:300:250:250:250:200:200:200:150:150:150:150:100:100:100:100:10
V
2:152:001:501:401:301:251:151:101:051:000:550:500:450:400:350:350:300:300:250:250:200:200:200:150:150:150:150:100:100:100:100:100:100:050:050:05
VI
1:301:201:151:101:000:550:500:450:400:400:350:300:300:250:250:200:200:200:150:150:150:150:100:100:100:100:100:100:050:050:050:050:050:050:050:05
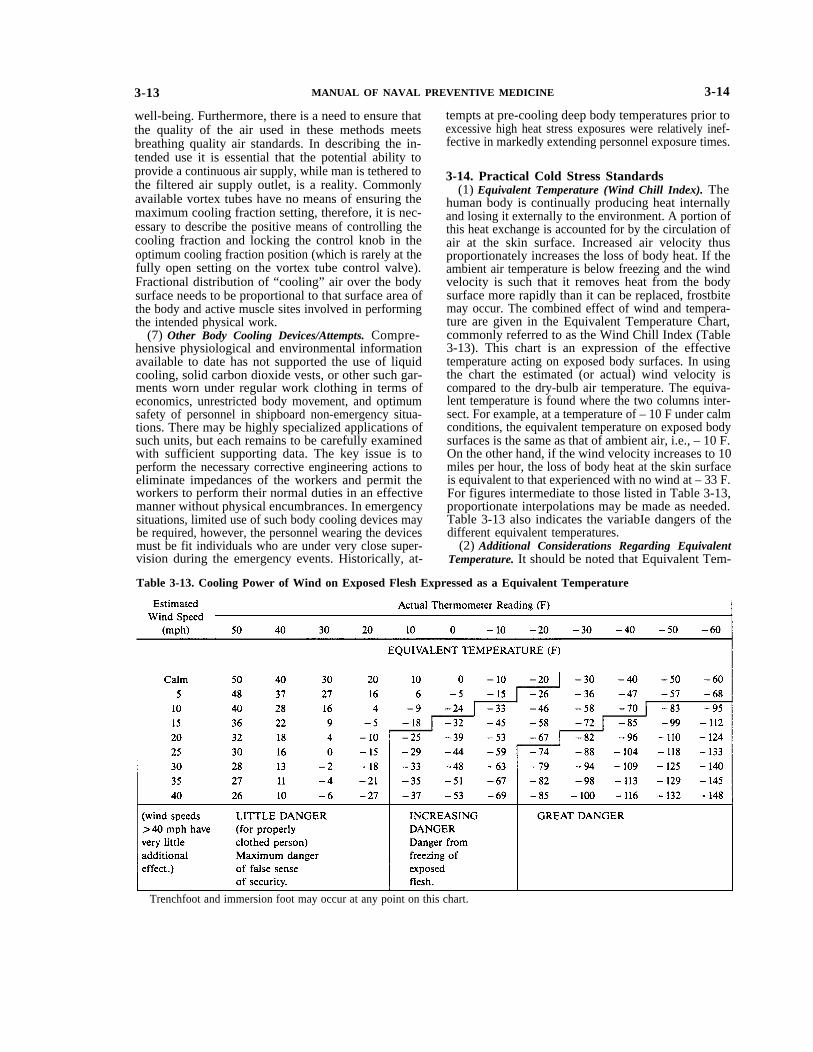
3-13 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-14
well-being. Furthermore, there is a need to ensure thatthe quality of the air used in these methods meetsbreathing quality air standards. In describing the in-tended use it is essential that the potential ability toprovide a continuous air supply, while man is tethered tothe filtered air supply outlet, is a reality. Commonlyavailable vortex tubes have no means of ensuring themaximum cooling fraction setting, therefore, it is nec-essary to describe the positive means of controlling thecooling fraction and locking the control knob in theoptimum cooling fraction position (which is rarely at thefully open setting on the vortex tube control valve).Fractional distribution of “cooling” air over the bodysurface needs to be proportional to that surface area ofthe body and active muscle sites involved in performingthe intended physical work.
(7) Other Body Cooling Devices/Attempts. Compre-hensive physiological and environmental informationavailable to date has not supported the use of liquidcooling, solid carbon dioxide vests, or other such gar-ments worn under regular work clothing in terms ofeconomics, unrestricted body movement, and optimumsafety of personnel in shipboard non-emergency situa-tions. There may be highly specialized applications ofsuch units, but each remains to be carefully examinedwith sufficient supporting data. The key issue is toperform the necessary corrective engineering actions toeliminate impedances of the workers and permit theworkers to perform their normal duties in an effectivemanner without physical encumbrances. In emergencysituations, limited use of such body cooling devices maybe required, however, the personnel wearing the devicesmust be fit individuals who are under very close super-vision during the emergency events. Historically, at-
tempts at pre-cooling deep body temperatures prior toexcessive high heat stress exposures were relatively inef-fective in markedly extending personnel exposure times.
3-14. Practical Cold Stress Standards(1) Equivalent Temperature (Wind Chill Index). The
human body is continually producing heat internallyand losing it externally to the environment. A portion ofthis heat exchange is accounted for by the circulation ofair at the skin surface. Increased air velocity thusproportionately increases the loss of body heat. If theambient air temperature is below freezing and the windvelocity is such that it removes heat from the bodysurface more rapidly than it can be replaced, frostbitemay occur. The combined effect of wind and tempera-ture are given in the Equivalent Temperature Chart,commonly referred to as the Wind Chill Index (Table3-13). This chart is an expression of the effectivetemperature acting on exposed body surfaces. In usingthe chart the estimated (or actual) wind velocity iscompared to the dry-bulb air temperature. The equiva-lent temperature is found where the two columns inter-sect. For example, at a temperature of – 10 F under calmconditions, the equivalent temperature on exposed bodysurfaces is the same as that of ambient air, i.e., – 10 F.On the other hand, if the wind velocity increases to 10miles per hour, the loss of body heat at the skin surfaceis equivalent to that experienced with no wind at – 33 F.For figures intermediate to those listed in Table 3-13,proportionate interpolations may be made as needed.Table 3-13 also indicates the variabIe dangers of thedifferent equivalent temperatures.
(2) Additional Considerations Regarding EquivalentTemperature. It should be noted that Equivalent Tem-
Table 3-13. Cooling Power of Wind on Exposed Flesh Expressed as a Equivalent Temperature
Trenchfoot and immersion foot may occur at any point on this chart.
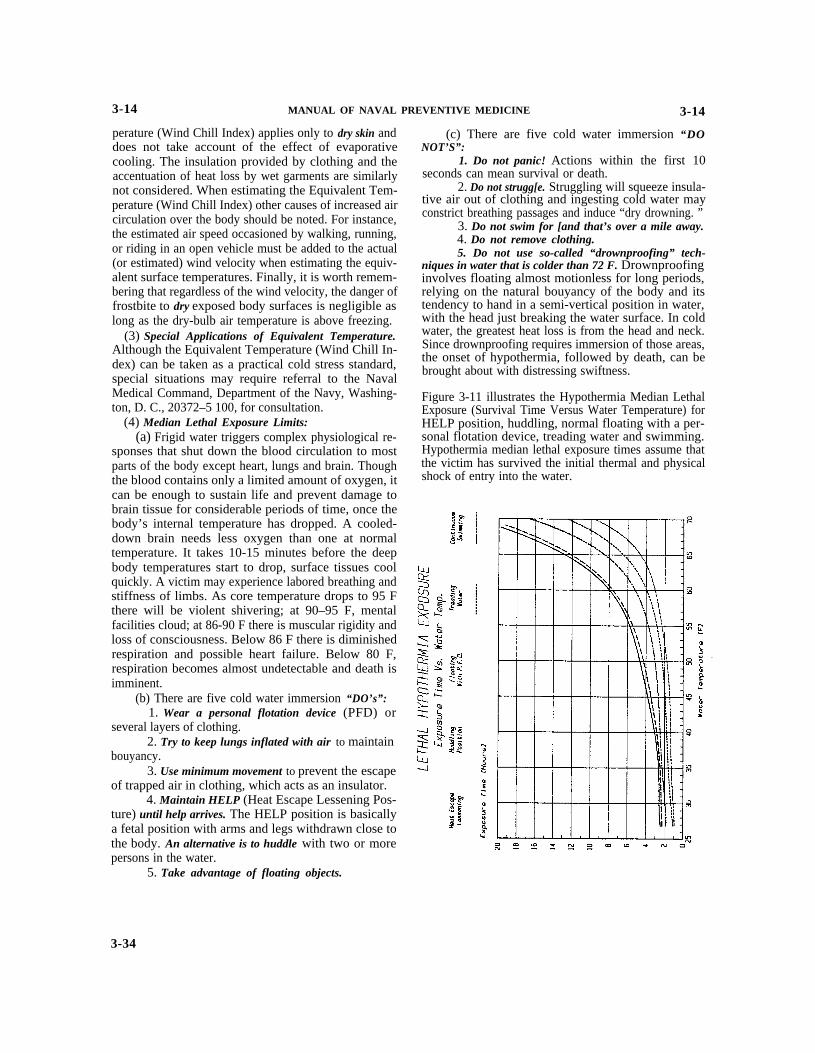
3-14 MANUAL OF NAVAL PREVENTIVE MEDICINE 3-14
perature (Wind Chill Index) applies only to dry skin anddoes not take account of the effect of evaporativecooling. The insulation provided by clothing and theaccentuation of heat loss by wet garments are similarlynot considered. When estimating the Equivalent Tem-perature (Wind Chill Index) other causes of increased aircirculation over the body should be noted. For instance,the estimated air speed occasioned by walking, running,or riding in an open vehicle must be added to the actual(or estimated) wind velocity when estimating the equiv-alent surface temperatures. Finally, it is worth remem-bering that regardless of the wind velocity, the danger offrostbite to dry exposed body surfaces is negligible aslong as the dry-bulb air temperature is above freezing.
(3) Special Applications of Equivalent Temperature.Although the Equivalent Temperature (Wind Chill In-dex) can be taken as a practical cold stress standard,special situations may require referral to the NavalMedical Command, Department of the Navy, Washing-ton, D. C., 20372–5 100, for consultation.
(4) Median Lethal Exposure Limits:(a) Frigid water triggers complex physiological re-
sponses that shut down the blood circulation to mostparts of the body except heart, lungs and brain. Thoughthe blood contains only a limited amount of oxygen, itcan be enough to sustain life and prevent damage tobrain tissue for considerable periods of time, once thebody’s internal temperature has dropped. A cooled-down brain needs less oxygen than one at normaltemperature. It takes 10-15 minutes before the deepbody temperatures start to drop, surface tissues coolquickly. A victim may experience labored breathing andstiffness of limbs. As core temperature drops to 95 Fthere will be violent shivering; at 90–95 F, mentalfacilities cloud; at 86-90 F there is muscular rigidity andloss of consciousness. Below 86 F there is diminishedrespiration and possible heart failure. Below 80 F,respiration becomes almost undetectable and death isimminent.
(b) There are five cold water immersion “DO’s”:1. Wear a personal flotation device (PFD) or
several layers of clothing.2. Try to keep lungs inflated with air to maintain
bouyancy.3. Use minimum movement to prevent the escape
of trapped air in clothing, which acts as an insulator.4. Maintain HELP (Heat Escape Lessening Pos-
ture) until help arrives. The HELP position is basicallya fetal position with arms and legs withdrawn close tothe body. An alternative is to huddle with two or morepersons in the water.
5. Take advantage of floating objects.
(c) There are five cold water immersion “DONOT’S”:
1. Do not panic! Actions within the first 10seconds can mean survival or death.
2. Do not strugg[e. Struggling will squeeze insula-tive air out of clothing and ingesting cold water mayconstrict breathing passages and induce “dry drowning. ”
3. Do not swim for [and that’s over a mile away.4. Do not remove clothing.5. Do not use so-called “drownproofing” tech-
niques in water that is colder than 72 F. Drownproofinginvolves floating almost motionless for long periods,relying on the natural bouyancy of the body and itstendency to hand in a semi-vertical position in water,with the head just breaking the water surface. In coldwater, the greatest heat loss is from the head and neck.Since drownproofing requires immersion of those areas,the onset of hypothermia, followed by death, can bebrought about with distressing swiftness.
Figure 3-11 illustrates the Hypothermia Median LethalExposure (Survival Time Versus Water Temperature) forHELP position, huddling, normal floating with a per-sonal flotation device, treading water and swimming.Hypothermia median lethal exposure times assume thatthe victim has survived the initial thermal and physicalshock of entry into the water.
3-34


















