Mantle technique
38
MANTLE FIELD RADIATION TECHNIQUE FOR HODGKIN’S LYMPHOMA Dr Mayur Mayank 19.05.2011
-
Upload
mayur-mayank -
Category
Health & Medicine
-
view
4.674 -
download
5
Transcript of Mantle technique

MANTLE FIELD RADIATION TECHNIQUE FOR HODGKIN’S LYMPHOMA
Dr Mayur Mayank19.05.2011

WHAT IS MANTLE TECHNIQUE ?
The name Mantle technique comes from the word ‘mantle’ which is a type of cloak.
It has been named so because the areas included in this radiation field technique resembles a person wearing a cloak.
It has been used traditionally for the treatment of Hodgkin's lymphoma.

• It is a type of Extended field radiation technique and includes multiple involved and uninvolved lymph node groups.
• When the multiple sites are involved above the diaphragm then the field used is known as Mantle Field.

• Mantle field is used for Supradiaphragmatic field.
• It includes the following group of lymph nodes:
• Bilateral Cervical• Bilateral Supraclavicular• Bilateral Infraclavicular• Bilateral Axillary• Bilateral Hilar• Bilateral Mediastinal


TREATMENT OF HODGKIN’S LYMPHOMA In the earlier days, before the advent of
effective chemotherapy, radiation alone was used for the treatment of HL.
This meant use of large radiation fields as well as raising the radiation dose to normal tissue limits.
It was associated with late development of many complications and increased mortality of cured patients beyond what was expected of normal population.


With the advent of effective and less toxic chemotherapy drugs, the use of RT alone in HL has now got a limited role.
In several types of HL now, chemotherapy alone has become the primary modality of treatment with RT used for consolidation and reduction of risk of relapse.

CLASSIFICATION OF RISK GROUPS FOR HL
EARLY ADVANCED
FAVOURABLE UNFAVOURABLE FAVOURABLE UNFAVOURABLE
STAGE I/II STAGE III/IV

Early Favorable :Clinical stage I/II without any risk factors
Early Unfavorable :Clinical stage I/II with one or more of the following risk factors :
1. Large mediastinal mass2. Extra nodal involvement3. Involvement of >=3 LN areas4. High ESR (>30mm/hr for B stage; >50mm/hr
for A stage)5. B symptoms

Advanced Favorable :Clinical stage III/IV with 0-3 risk factors
Advanced Unfavorable :Clinical stage III/IV with >=4 risk factors
Risk factors1. Male sex2. Age 45 yrs or more3. Hb < 10.5 gm%4. Albumin < 4.0 gm/dL5. Stage IV disease6. WBC count >= 15,000/mm37. Absolute lymphocyte count <600/mm3 or
lymphocyte count <8% of total WBC count

USES OF RADIATION THERAPY IN HODGKIN’S LYMPHOMA
RT ALONE (Potentially Curative)1. Lymphocyte predominant HL (Stage I/II)2. Classical HL (Stage IA/IIA)
RT - COMBINED MODALITY (Potentially Curative)
3. Classical HL (Stage I/II-favorable and unfavorable)
4. Advanced HL

CHEMOTHERAPY DRUGS USED FOR HL
1. MOPP regimen : Mechlorethamine, vincristine (oncovin), procarbazine, prednisolone.
Had high risks of sterility and secondary malignancies (leukemia, lung cancer).
2. ABVD regimen : Adriamycin, bleomycin, vinblastine, dacarbazine.
This regimen is much better tolerated by patients and the risks that were associated with the MOPP regimen are very less in this regimen.

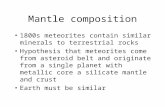
FIELD SIMULATION IN MANTLE FIELD• The patient is placed supine with maximum extension of the neck and arms above the head, or at 90* angle towards the side, or in ‘akimbo’ position, i.e., hands on the waist.

• In the arms above the head position, the axillary nodes were brought further away from the chest. This helped in a more generous lung shielding.
• In the ‘akimbo’ position, the humeral heads can be shielded and also it minimized the effect of tissue folds in supraclavicular/low neck regions.

• Neck should be in maximum extension to exclude the oral cavity and teeth from the RT field and to decrease the dose to the mandible.
CORRECT
• All palpable lymph nodes should be marked with wires.

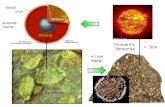
BORDERS
Superior : Through the chin, bisecting the mandible, to the mastoid process.
Lateral : Flashing the axillae
Inferior : Inferior axillary at the inferior tip of scapula. Inferior mediastinal at the initial mediastinal extent of the disease with a ~ 5 cms margin ( T10-T11 interspace ).

SHIELDING
Lung blocks : Made separate for anterior and posterior.
Upper border in anterior : 2 cms below medial clavicle, and a thin lung band is left at the lateral clavicles.
Upper border in posterior : a thin band is left under the clavicles as the infraclavicular LN’s are located anteriorly.
Lateral Borders : a 1 cm band is left in costal curves which extends until the 5th or 6th costa and finishes horizontally in chest wall.
Medial Border : bilateral mediastinal and hilar lymphatics are included (mediastinal enlargement should be included).

• Head of Humerus is shielded both anteriorly and posteriorly.
• Larynx is shielded anteriorly.
• Heart is shielded below the hilar level without including the mediastinal LN’s both anteriorly and posteriorly.
• Spinal cord shielding is done in midline for dosages >40 Gy.
• A small block is put at the inferior border of spinal cord posteriorly.
• Oral cavity is shielded if the superior border includes the oral cavity.


• The central axis of the field is usually at the sternal notch or close to it.
• The central axis, points 10 cms left and right of it, and the inferior border, should be marked with a tattoo to check during the daily setup and to allow the possibility of infradiaphragmatic RT at later stages.

ANTERIOR POSTERIOR


DOSE PRESCRIPTION
Beams : Parallel opposed
SSD : at 100-120 cms (Extended SSD)
Field Size : 40 x 40 cm2
Dosage : 36 - 40 Gy (Standard dose at Stanford was 44 Gy)

MODIFICATIONS OF MANTLE FIELD
MINI MANTLE : Hilar and Mediastinal lymph nodes are not included.
MODIFIED MANTLE : Axillary lymph nodes are not included.


COMPLICATIONS
ACUTE :
Fatigue Radiation dermatitis in the areas of
irradiated skin. Mouth dryness Pharyngitis

EARLY :
Lhermitte’s Sign : Electric-shock like sensation radiating down the back of both legs when the head is flexed.
Seen in ~<5% patients within 6 weeks to 3 months after Mantle field RT.
Resolves spontaneously within few months with no late/permanent spinal cord damage.
Pneumonitis
Pericarditis

LATE :
Hypothyriodism
Secondary Malignancies : High incidents of patients treated by mantle field RT to develop secondary solid tumors – most commonly lung and breast.
Coronary Artery disease

PROBLEMS FACED IN MANTLE FIELD
LARGE FIELD
EXTENDED SSD
IRREGULAR BLOCKS AND SHIELDS
SLANTING BODY CONTOURS
INHOMOGENOUS DOSE
DISTRIBUTION

LARGE FIELD(40 X 40 cm2)
EXTENDED SSD(100 – 120 cms)
• A change in the SSD leads to a change in the Percentage Dose Depth (PDD) and the beam output.
• Mayneord Factor is used to determine the PDD for the extended SSD.

IRREGULAR BLOCKS AND SHIELDS
SLANTING BODY CONTOURS
IRREGULAR FIELD
• The irregular fields which are produced are corrected by using Clarkson’s Method for irregular field dose calculation.

• Due to the inhomogeneous dose distribution, the minimum dosimetry should include an irregular field point calculation for each important nodal region in the field.
• The dose variations determined by these calculations must be compensated by individually designed compensators or selective area blocking.

NEWER TECHNIQUES
IFRT (Involved Field Radiation Therapy)
This is limited to the site of the clinically involved lymph node group.For extra nodal sites, the field includes the organ alone (if there is no evidence of lymph node involvement).The “grouping” of lymph nodes is not clearly defined.

ILRT (Involved Lymph node field RT)
This is the latest radiation field which has been introduced for the treatment of HL.The clinical target volume (CTV) includes only the originally involved lymph node(s) volume (pre-chemotherapy) with the addition of 1cm margin to create a planning target volume (PTV).

CONCLUSION The Mantle Field used earlier for irradiating
supradiaphragmatic HL had many drawbacks : the field size involved was too large with an
extended SSD. the demarcation of the proper target field with
the proper sheidings was a very difficult and time consuming task to perform
the dose calculation for the involved field was also a very troublesome task with lots of calculations involved.
the late complications, especially that of secondary solid tumors, was a major cause of morbidity and mortality after the primary HL had been treated.

The newer modalities of Radiation therapy like IFRT and ILRT (used in combination with chemotherapy) use smaller fields and the treatment planning and simulation, dose calculation and complications associated with them are much less than what was seen with Extended field techniques like Mantle Field.
Also, as they are used in conjugation with chemotherapy, so the dose can be reduced from 40 Gy to 30 Gy.
The use of chemotherapy drugs has helped in limiting the use of RT in cases of Hodgkin’s Lymphoma, and combined modality of treatment is more effective and less toxic than radical radiation alone.

THANK YOU