
Mantle Cell Lymphoma: The Inevitable Relapse Peter Martin, MD Assistant Professor of Medicine...
23
Mantle Cell Lymphoma: The Inevitable Relapse Peter Martin, MD Assistant Professor of Medicine Division of Hematology/Oncology Weill Cornell Medical College New York, New York
-
Upload
corey-bradford -
Category
Documents
-
view
214 -
download
0
Transcript of Mantle Cell Lymphoma: The Inevitable Relapse Peter Martin, MD Assistant Professor of Medicine...

Mantle Cell Lymphoma:The Inevitable Relapse
Peter Martin, MDAssistant Professor of Medicine
Division of Hematology/OncologyWeill Cornell Medical College
New York, New York

Johnson PWM et al. J Clin Oncol. 1995;13(1):140-147.
Patterns of survival in FL
T = 20 years
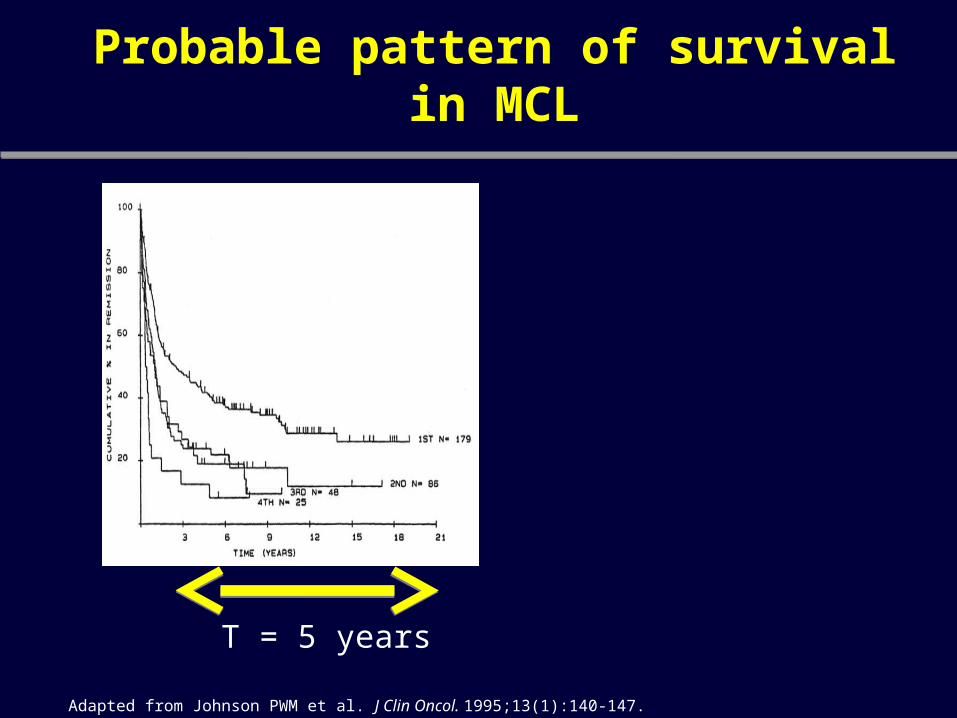
Adapted from Johnson PWM et al. J Clin Oncol. 1995;13(1):140-147.
Probable pattern of survival in MCL
T = 5 years

Goy A et al. Ann Oncol 2008;20:520-525
Bortezomib in Relapsed or Refractory MCL (Phase II PINNACLE Study):
Progression-free survival

Haberman TM, et al. Br H Haematol. 2009; Zinzani PL, ASH 2008. Reeder CB, et al. ASH 2008. Wang et al. ICML 2011
STUDY Design Results/Comments
NHL-002
N=15Median of 4 prior rx
Prior ASCTPrior Bort
ORR: 53% (CR-20%)Median DOR: 13.7 mosMedian PFS : 5.6 mon
Dose reductions in 53%
NHL-003N= 39
Median age 66, 3 prior Rx Bort-23%
ORR: 41% (CR or CRu-13%)Median DOR: 13.7 mos
Grade 3-4 : Neutropenia (51%), thrombocytopenia (25%), anemia (13%), fatugue (10%) and Febrile
Neutropenia (10%)
Prior BORT- POOLED NHL-002 and 003
N=14, median prior Rx-4, 50% Bort refractory
ORR-57%, CR or CRu-21%.Similar AEs
Rev+ RituxN=46
Phase IIOORR 57%, CR 33%
RD 19 mo.
Lenalidomide
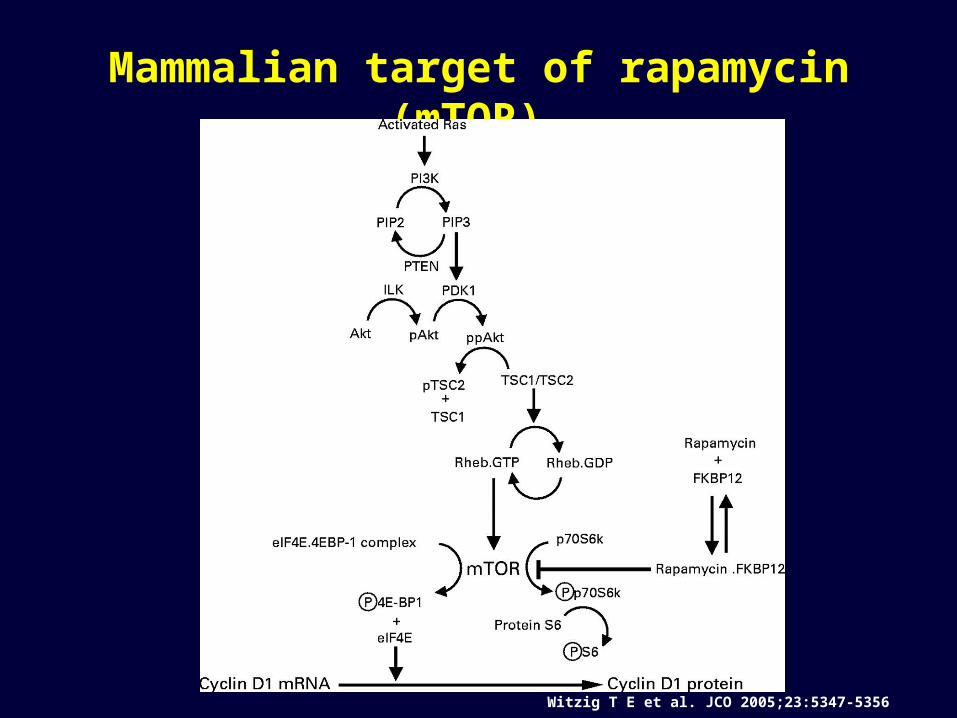
Mammalian target of rapamycin (mTOR)
Witzig T E et al. JCO 2005;23:5347-5356

Dose N RR TTP Grade 3-4 heme tox.
Witzig 250 mg 35 38% 6.5 mo. 84%
Ansell 25 mg 29 41% 6 mo. 54%
Phase 2 studies of temsirolimus in relapsed MCL
Witzig et al. JCO 2005;23:5347Ansell et al. Cancer 2008;113:508
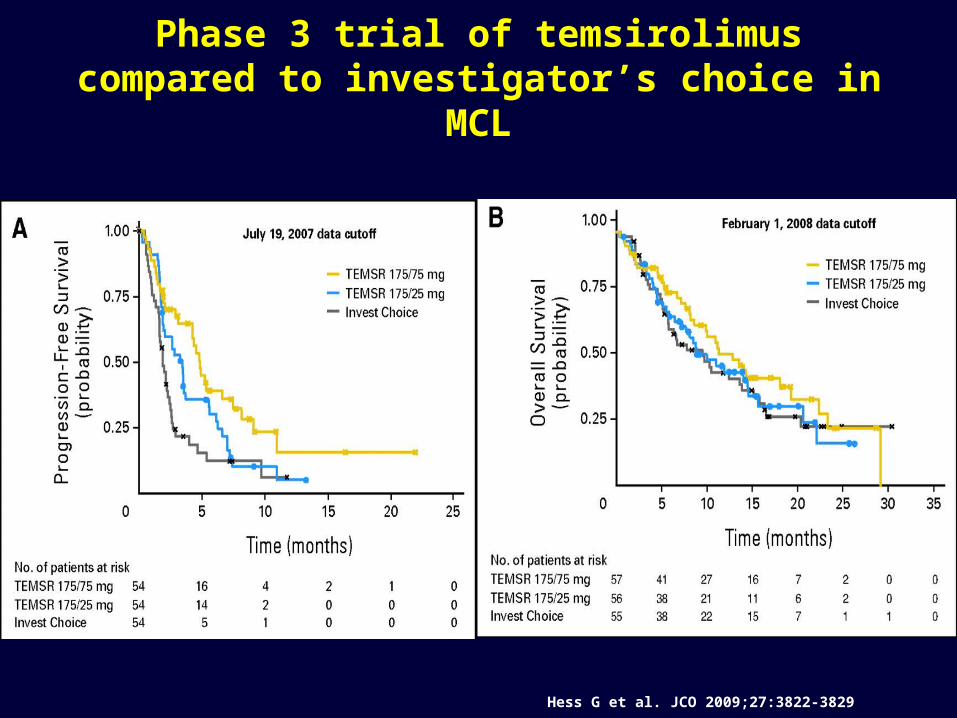
Hess G et al. JCO 2009;27:3822-3829
Phase 3 trial of temsirolimus compared to investigator’s choice in MCL
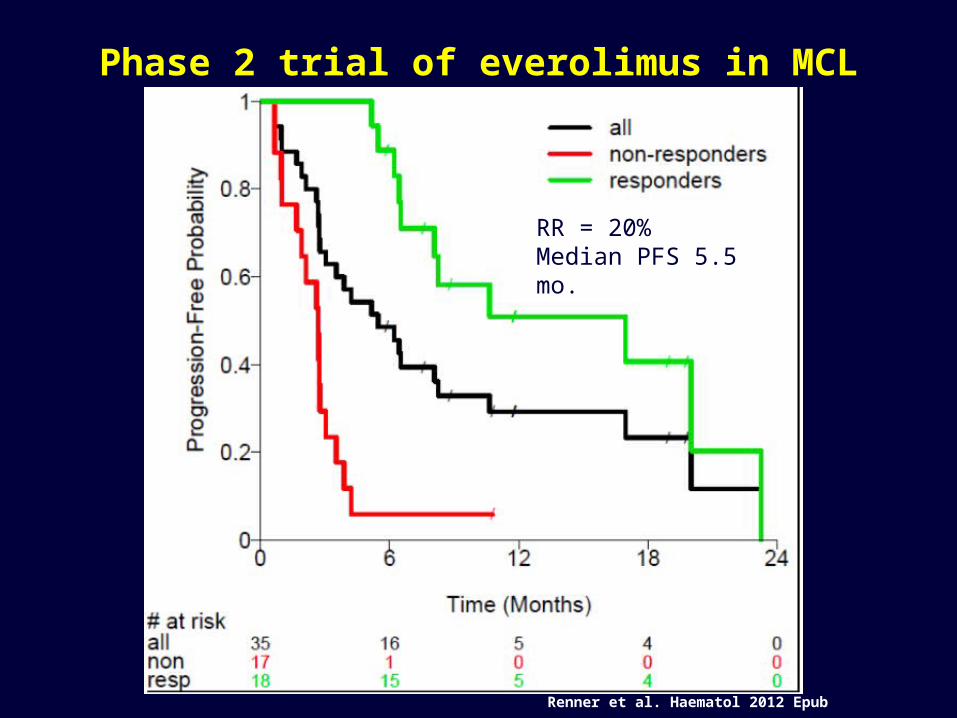
Renner et al. Haematol 2012 Epub
Phase 2 trial of everolimus in MCL
RR = 20%Median PFS 5.5 mo.

BCR, NF-κB, and PI3K/AKT/mTOR deregulation in MCL
Pérez-Galán P et al. Blood 2011;117:26-38

Phase 2 trial of fostamatinib (oral Syk inhibitor) in relapsed NHL
Friedberg J W et al. Blood 2010;115:2578-2585
MCL patients N=91 PR4 SD4 PD
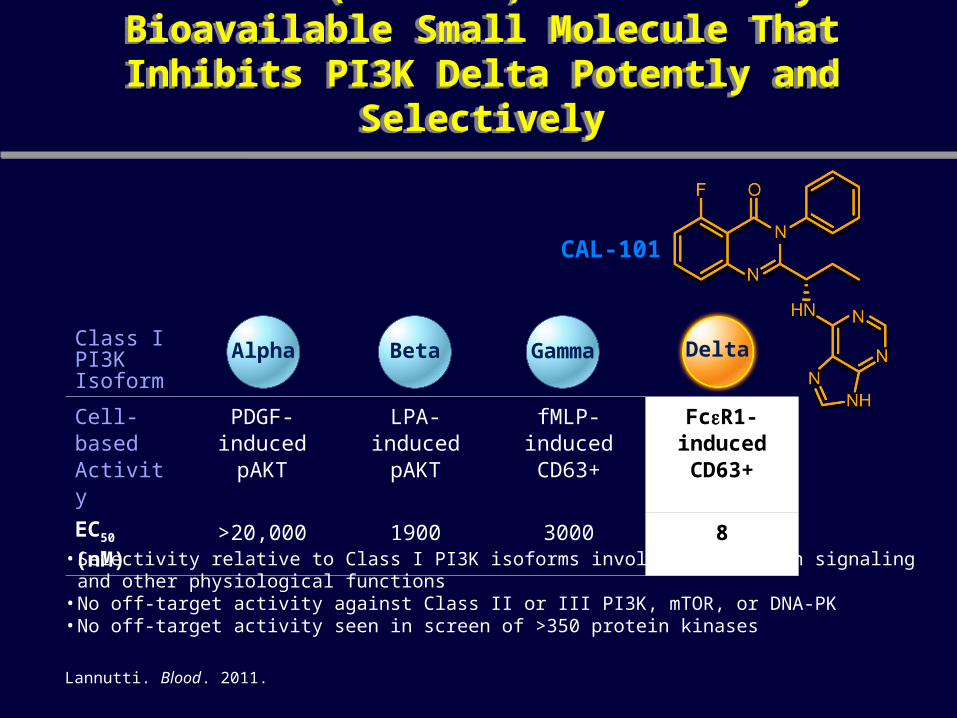
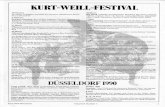
CAL-101 (GS-1101) Is an Orally Bioavailable Small Molecule That Inhibits PI3K Delta
Potently and Selectively
CAL-101 (GS-1101) Is an Orally Bioavailable Small Molecule That Inhibits PI3K Delta
Potently and Selectively
Class IPI3K Isoform
Cell-based Activity
PDGF-induced pAKT
LPA-induced pAKT
fMLP-induced CD63+
FcR1-induced CD63+
EC50 (nM) >20,000 1900 3000 8
Alpha Beta Gamma Delta
• Selectivity relative to Class I PI3K isoforms involved in insulin signaling and other physiological functions• No off-target activity against Class II or III PI3K, mTOR, or DNA-PK• No off-target activity seen in screen of >350 protein kinases
Lannutti. Blood. 2011.
CAL-101

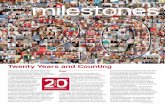
Cal-101 in B-cell Lymphoma Best Response
-50*
-75% C
hang
e in
Lym
ph N
ode
Area
-25
-100
+25
+50
+75
+100
0
MCL(n = 21)
iNHL(n = 30)
Best on-treatment change in tumor size(ITT analysis)
Inevaluable (patients without a follow-up tumour assessment; includes two patients with LPL with no adenopathy)
* Criterion for response [Cheson 2007, Hallek 2008]
Kahl B et al. Blood (ASH Annual Meeting Abstracts). 2010;116:1777.
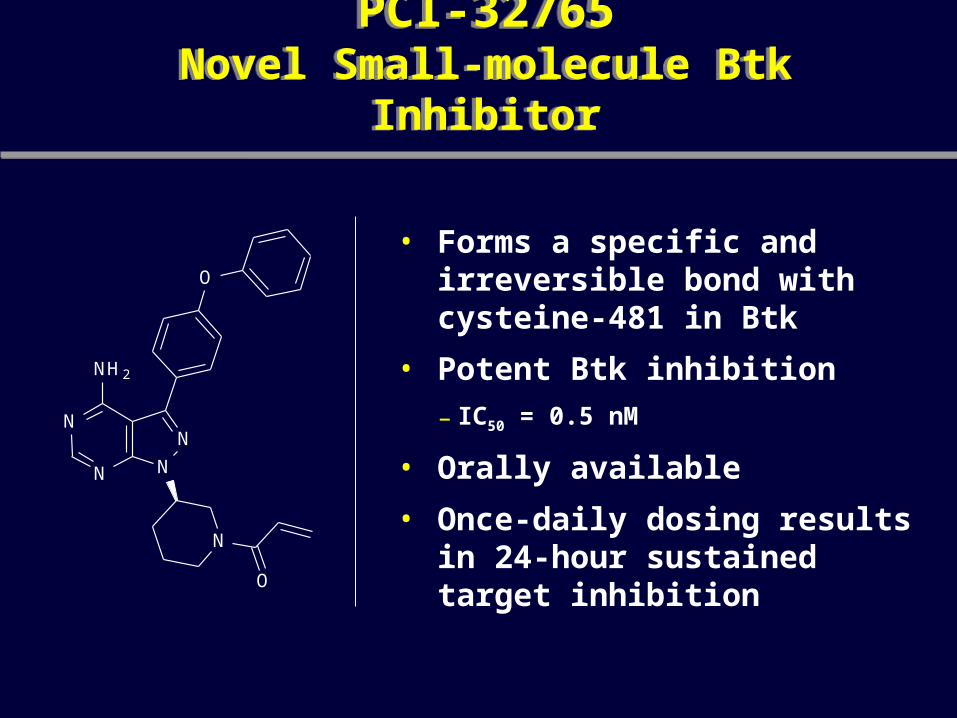
PCI-32765Novel Small-molecule Btk Inhibitor
PCI-32765Novel Small-molecule Btk Inhibitor
• Forms a specific and irreversible bond with cysteine-481 in Btk
• Potent Btk inhibition – IC50 = 0.5 nM
• Orally available
• Once-daily dosing results in 24-hour sustained target inhibition
N
N
NN
N H 2
O
N
O

Best Response Best Response
BTZ-naïve(n = 31)
BTZ-exposed(n = 20)
Total(n = 51)
CR
PR
SD
PD
71%
16%13%
65%69%
20%15% 18%
15%
50%
16%
55%
16%
53%
BTZ= Bortezomib
*Wang et al. ASH 2011; Abstract 442

n/N ORR %All Patients 35/51 69Bulky Disease 4/7 57RefractoryYesNo
14/2121/30
6770
Prior cancer treatments < 3 regimens ≥ 3 regimens
23/3012/21
7757
Prior high intensity therapyYesNo
22/3113/20
7165
MIPI Score: Low RiskIntermediate RiskHigh Risk
6/813/2015/20
756575
Best Response by Patient Characteristics
16

The Cell Cycle
G1
S
G2
M
p21p27p57
Negative
Go
Positive
Cyclin D + CDK4/6
pS-Rb-E2F
Cyclin E + CDK2
pST-Rb E2F release
p16p15p18p19
CDK: Cyclin-Dependent Kinasep18INK4c (CDKN2C)
mid-G1 checkpoint
Slide courtesy of Dr Selina Chen-Kiang
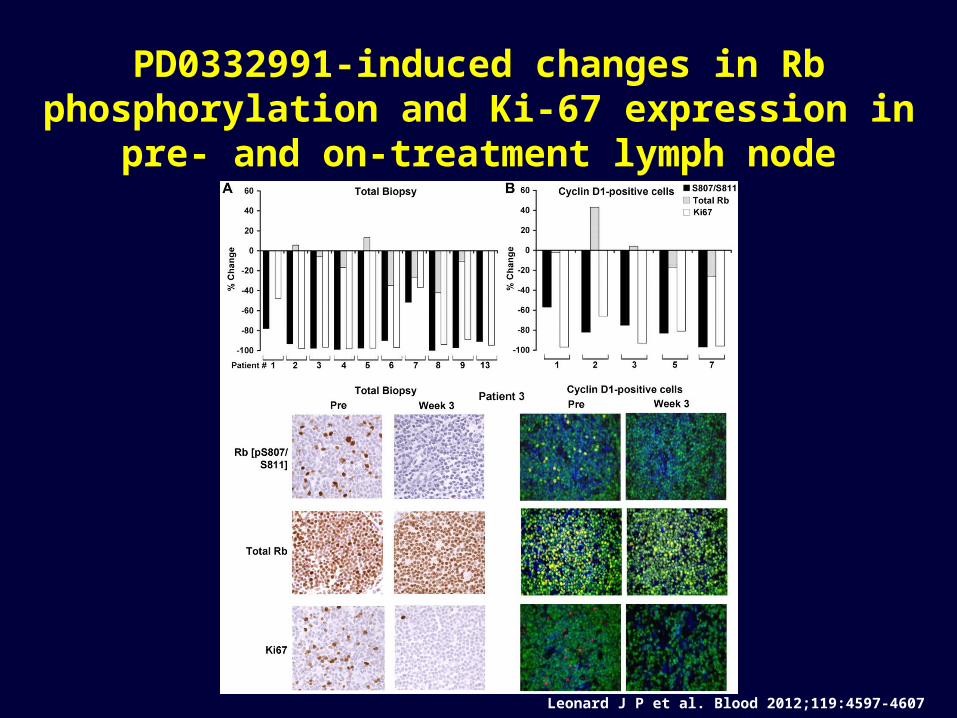
PD0332991-induced changes in Rb phosphorylation and Ki-67 expression in pre- and
on-treatment lymph node biopsies.
Leonard J P et al. Blood 2012;119:4597-4607

Quantification of FDG- and FLT-PET changes on PD0332991 and correlation with each other and
time to progression.
Leonard J P et al. Blood 2012;119:4597-4607

The anti-apoptotic phenotype and alterations in BCL-2 family members in MCL
Pérez-Galán P et al. Blood 2011;117:26-38

Low-dose metronomic oral chemotherapy
• Prednisone 20 mg at breakfast• Etoposide 50 mg at lunch• Cyclophosphamide 50 mg at supper• Procarbazine 50 mg at bedtime• Start daily, then titrate frequency based
on ANC
Regimen Design N RR Outcome
PEPC retrospective 22 82% TTP 17 mo.
RT-PEPC prospective 25 73% PFS 10 mo.
Coleman et al. Leuk Lymphoma 2008;49:447-450Ruan et al. Cancer 2010;116:2655-2664

Conclusion
• All MCL patients eventually acquire resistance to intermittent chemotherapy
• Treatment with novel agents/continuous therapy is required to maintain remissions
Future challenges
• Is there a role for early detection/treatment of subclinical relapse?
• Should novel treatments be used as single agents in relapse or combined with upfront induction/consolidation/maintenance regimens?
• Mechanisms of response/resistance of novel agents need to be clarified to justify rational combinations.










![Relapse of drug addictors; A review€¦ · 2.Relapse rate: Relapse is very common after treatment for drug addiction [3], it was stated that 25-50% of substance abusers will relapse](https://static.fdocuments.in/doc/165x107/5f2c786cf88b454211793241/relapse-of-drug-addictors-a-review-2relapse-rate-relapse-is-very-common-after.jpg)



