Vaginal Massage, Vaginal Therapy, Vaginal Massage Therapy, Christchurch, Brisbane
Welcome to Mansion Street Women’s Health. This form contains questions about your medical, obstetrical, family, and social histories. This information is vital to us. Please answer the questions to the best of your knowledge. We realize that some of our patients have previously filled out this information; however, we need this to update our records. Leave blank any questions you do not know. Your answers are kept confidential. Thank you very much!
Name: ___________________ ___________________ _________ Date: _____________________ (last) (first) (MI)
Primary Care Physician: (Name & Phone #) _________________________________________________________
Age: ______________ Date of last menstrual period: ________________________
# of pregnancies: ____________ # of full term babies: __________ # of preterm babies: __________
# of abortions:__ ____________ # of miscarriages: ____________ # of living children: ___________
Age at onset of menses: ______ How often does your menses come: _______ Duration: ____________
Is flow heavy / mod / light? _____ Do you miss periods? Yes / No Cramps? Yes / No
Do you pass clots? Yes / No Do you ever miss work because of periods? Yes / No
Do you take any medications for your cramps? Yes / No If yes, what? _____________________________
SEXUAL HISTORY:
Are you sexually active? Yes / No Birth control method? Condoms / pills / tubal ligation / vasectomy? ______________
Do you have pain with intercourse? Yes / No Have you ever received the Gardisil vaccine? Yes / No
Have you ever been exposed to any sexually transmitted diseases? Yes / No If yes, please describe: __________________________
Sexual orientation (circle one) Men / Women / Both Number of partners in lifetime ________
Current partner since when? ___________
GYNECOLOGIC HISTORY
When was your last pap smear? _____________ Was it normal? Yes / No Have you ever had an abnormal pap? Yes / No
Did your abnormal pap require a Colposcopy / Cryo? Yes / No If yes, when? ___________________
Do you perform monthly self breast exams? Yes / No Do you know how? Yes / No
Ever have a mammogram? Yes / No If yes, list results, date & location ___________________________
Have you ever had a HALO Breast Pap Test? Yes / No If yes, list results, date & location ___________________________
Do you leak urine when you cough, sneeze, or laugh? Yes / No Is this a problem you want addressed? Yes / No
Have you ever had any gynecologic surgery? Yes / No If yes, please explain below and include dates:______________________________________________________________________________________________________________
In the chart below, please fill in the information requested for all pregnancies. Include abortions, miscarriages, and ectopics. If more room is needed, please use the back.Delivery / Birthdate
How long to conceive?
Infertility treatment?
Baby Weight Abortion / Miscarriage / Vaginal / Cesarean
Is current partner the father?
Complications
Mansion Street Women’s Health, P.L.L.C. HISTORY & PHYSICAL INFORMATION

Do you currently have a problem with any of the following? IF YES, PLEASE CIRCLE.
HEAD / EYES / EARS / NOSE / THROAT: CHEST:headaches chest painear aches shortness of breathhearing loss asthmavision loss racing heartnasal congestion / drainage irregular heart beatsore throatdifficulty swallowing GASTROINTESTINAL:stiff neck diarrhea constipationGENITAL URINARY: reflux disease / heartburndifficulty urinating irritable bowel diseaseloss of urine when cough / sneeze / or strain hemorrhoidsurgency (can’t hold it when you feel urge) hepatitis Type A, B, Cfrequency > 8-10 /day nocturia (get up at night to void) How often? ______ NEUROLOGIC: burning with urination any numbness or tinglingabnormal vaginal discharge loss of strength / weaknessvaginal odor dizzinessvaginal / vulvar itching pain with your period / menses MUSCULOSKELETAL:
Medication used _______________________ joint pain Where? ____________________Does it help? Yes / No back pain
Pain with intercourse / sex neck painVaginal pressure / pain
Other: __________________________________________________________________
PAST MEDICAL HISTORY: Please circle any of the following medical conditions that you have now or have had in the past:
Diabetes High blood pressure Heart disease or murmur....Are antibiotics needed? Y / NAsthma Seizures / Epilepsy Thyroid diseaseAnemia Migraine Headaches Reflux disease Cancer Stroke Irritable bowel syndromeBreast Disease Blood clots Kidney infections Fibromyalgia TB Kidney StonesDepression Anxiety Lung Disease OTHER _______________
Have you ever been hospitalized for anything non-obstetrical / gynecological in nature? Yes / No
If yes, please explain and include date(s) __________________________________________________________
Have you ever had any non gynecologic or obstetric surgery? (gall bladder, appendix, tonsils, etc.) If yes, please explain and include date(s) ___________________________________________________________________________________________
Are you ALLERGIC to any medication? If yes, provide name and reaction to drug______________________________________________________________________________________________________________________
Are you ALLERGIC to LATEX? Yes / No
What medications are you currently taking (include doses, please) _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
At what pharmacy do you have your prescriptions filled? ____________________________________________
Mansion Street Women’s Health, P.L.L.C. HISTORY & PHYSICAL INFORMATION

Has any blood relative ever had (past or present) any of the following? If yes, please describe who has had the problem:
Breast Cancer Ovarian CancerUterine Cancer DiabetesColon Cancer Heart DiseaseHypertension StrokeOther
Marital Status (please circle) Married Single Divorced Widowed Separated
Do you work outside of your home? Yes / No Occupation: _______________________________________
Do you smoke? Yes / No How much? ___________ How many years have you smoked? _________
Did you quit smoking? Yes / No If yes, when did you quit? ________ How many years did you smoke? _________
Do you drink alcohol? Yes / No How much / often _________ Have you ever used any recreational drugs? Yes / No
How many caffeinated beverages (coffee, tea, colas) do you drink daily? ___________
Have you ever been a victim of domestic violence? Yes / No Are you currently in an abusive situation? Yes / No
Do you wear your seat belt when driving? Yes / No Do you use a seat belt while a passenger? Yes / No
Do you exercise on a regular basis? Yes / No If yes, what type of exercise, how many days a week and for how long do you exercise? ______________________________________
Date of last Tetanus shot? ________________
Are you immunized against Rubella? Yes / No / Uncertain Have you had a flu shot this year? Yes / No
Have you ever had a pneumococcal (pneumonia) vaccine? Yes / No
If you are currently pregnant, please fill out the Pregnancy Questionnaire.
Thank you for completing this form. It will help us provide you with the best possible care possible!
Mansion Street Women’s Health, P.L.L.C. HISTORY & PHYSICAL INFORMATION

MANSION STREET WOMEN’S HEALTH ANNUAL INFORMATION SHEET
PATIENT INFORMATION Name:__________________________MI:______Maiden Name:_______________________
Address:___________________________________________________________________
City / State / Zip: __________________________________________________________
Phone-Cell _________________ Home_________________Work ____________________
Email address: ______________________________________________ (see next line)
Race (please circle one) White Black/African American Hispanic Asian American Indian or Alaska Native Native Hawaiian or Other Pacific Islander Multi-Racial Decline to answer Ethnicity (please circle one)
Hispanic / Latino NOT Hispanic / Latino Decline to answer
S.S.#:________________Date of Birth:__________Martial Status: M / S / D / W / SEP
Employer Name:_____________________________Employer Phone#:_______________
Employer Address:__________________________________________________________
City / State / Zip: __________________________________________________________
SPOUSE INFORMATION (or IF MINOR, legal parent / guardian):
Name:___________________________________________________________________
Spouse’s S.S.#:__________________________ Spouse’s Date of Birth:_____________
Employer Name:___________________________Employer Phone#:________________
Employer Address:_________________________________________________________
City / State / Zip: ________________________________________________________
INSURANCE
First Insurance Co. Name:________________________________________________
Subscriber Name (name on insurance card):__________________________________
Subscriber Date of Birth: _______________ Subscriber SS #: ____________________
Contract #: __________________________Group #:____________________________
Second Insurance Co. Name:______________________________________________
Subscriber Name (name on insurance card):___________________________________
Subscriber Date of Birth: _______________ Subscriber SS #: _____________________
Contract#:__________________________________Group #: ______________________
Person Responsible for Payment/Guardian if under 18: ________________________________
Current Physician:_________________________________________________________
Previous Physician:________________________________________________________
Referring Physician:______________________________________________________
Emergency Contact (DIFFERENT ADDRESS THAN ABOVE)
Name:__________________________Phone:________________ Relationship:_________________
Address: __________________________________________________________________________
City / State / Zip: __________________________________________________________________
Assignment and Release: I hereby authorize that my insurance benefits be paid directly to the undersigned physician. I authorize the release of any medical information, about me, to other treating providers for evaluation, administration of claims for benefits, and for developing cost-effective managed care. I acknowledge that I am financially responsible for any non-covered services. I authorize MSWH to contact and speak to my emergency contact if deemed necessary.
Financially Responsible Person :____________________________Date:__________________ Patient / Legal Guardian if under age 18.
Physician:_______________________________________________Date: __________________

! ! ! ! ! FINANCIAL POLICY !
Thank you for choosing Mansion Street Women’s Health, P.L.L.C. (MSWH) as your health care provider. We are committed to providing you with exceptional, quality healthcare. We would like you to understand your financial commitment for all services rendered in our office. The following is a statement of our Financial Policy that we ask that you read in its entirety and sign in that you agree.
For your convenience MSWH accepts the following methods of payment: Cash, Check, Money Order, Visa, Mastercard, Discover and American Express.
Insurance Claims (Participating): We have contracts with many insurance companies and will bill them as a courtesy service to you. As the patient of services rendered, you are responsible if your insurance company declines to make payment for any reason. All co-pays are due at the time of your appointment. Below is a partial list of insurance companies with which we are participating providers. If your insurance company is not listed here, please ask the front desk if we are currently a participating provider with your insurance.
Aetna ! ! ! ! ! ! Medicaid Blue Cross Traditional & PPO! ! ! Medicare Cofinity!! ! ! ! ! United Healthcare Community PlanMeridian Health Plan! ! ! ! Healthscope Benefits ! !Priority Health !! ! ! ! United Healthcare You should know that your insurance policy is a contract between you and your insurance company. Please be aware that it is your responsibility as a patient to know which services (for example: tests, labs, etc.) are covered benefits of your plan. Also please note that some of the services we provide may be non-covered services under your own insurance plan and are not payable by your insurance policy. You will be financially responsible for these services. Secondary insurances will be billed as a courtesy to our patients. Deductibles, co-insurances and non-covered services are due upon receipt of your first patient statement. Deductibles: If your insurance company has applied our charges for services rendered towards your deductible, then it is deemed your responsibility to make payment to our office. Insurance claims and deductibles are typically paid on a “first come first served/processed” basis by the insurance company and are not always paid in “Date of Service” order. Deductibles are due upon receipt of your first patient statement.
Non-Participating Insurance Claims: For patients with an insurance plan that we are non-participating with, we will bill your insurance as a courtesy with the understanding that whatever charges come back as not being paid for are your responsibility as the patient.
Minor Patients: Parents or legal guardians of patients who are minors (under the age of 18) are responsible for full payment as described herein.
Records Fee: Copies of your medical records are available to you and are subject to the per page guidelines set fourth by the State of Michigan Department of Community Health. Please inquire with the receptionist for further information.

FMLA Forms: A $10.00 fee will be assessed for each form needing to be filled out and payment in full is required before this paperwork will be released.
Obstetrical Care Patients: Those patients who will be receiving obstetrical care with our office will be presented with additional information regarding your charges and payment options.
No-Show Fees: A no-show / late cancellation fee of $25.00 will automatically be assessed to any patient who does not cancel their appointment at least 24 hours in advance or neglects to show up. Three no-shows are considered non-compliance with scheduled appointments and may result in your dismissal from the practice. In addition, please note that if you show up for an appointment 15 minutes or more LATE, it is office policy that you will be rescheduled. Since many appointments are scheduled and booked months in advance, please be on-time as it may be extremely difficult to be rescheduled timely. Thank you! ! *Please note that due to the nature of our practice, our doctors are sometimes called to surgery and/or labor & delivery. If you are here for an appointment and your provider is not in the office, we will advise you at that time. We thank you in advance for your patience in the event this situation arises!
Returned Checks: A fee of $40.00 will be charged to your account for all returned checks to this office for any reason (insufficient funds, stop payment, account closed, etc). This fee is assessed in addition to the amount of the original payment. We will not send the check thru the bank more than one (1) time. If subsequent checks are returned to us, we will no longer be able to accept a personal check from you or any immediate family members. Other methods of payment for your account must be utilized at that time.
Non-Compliance: If for any reason you choose not to comply with the MSWH Financial Policy as outlined herein, your account will be reviewed and could result in being forwarded to our collection agency. Should collection proceedings or other legal action become necessary to collect an overdue account, the patient or patient’s responsible party fully understands that MSWH will disclose all relevant personal and account information necessary to collect payment for services rendered. A collection fee of $50 shall be charged to your account if it is forwarded to our collection agency. Additional costs, such as court costs, attorney fees, and any interest charged will be the responsibility of said patient or signed representative acting on their behalf. Any patient sent to collections may also result in being dismissed from the practice. By signing below, I acknowledge that I have fully read, understand and completely agree to the above financial policy as set forth by Mansion Street Women’s Health, P.L.L.C. This document may be scanned into an electronic format and such printed copy of the electronic record shall be deemed an original.
_______________________________ ! ! ____________________________Printed Name !! ! ! ! MSWH Staff Signature
_______________________________ ! ! ____/_____/________ Signature of Patient or Responsible Party of Minor ! Date
Thank you for understanding our Financial Policy. Please let us know if you have any questions or concerns. We look forward to providing you with exceptional care throughout your visits with MSWH!
Automated Appointment Reminders Dear Patient,
We would like to inform you that we have instituted a new automated reminder system, named AutoRemindTM, which is already in effect. This system, being one of the more advanced on the market, allows us to remind you of your appointments in the manner that is best suited to your needs and habits!
AutoRemind can send you appointment confirmation requests via email, text messages, and voice calls to your mobile / home telephone numbers. PLEASE NOTE: The automated system will ask you to confirm your appointment at the end of the message, as well as inform you of our late cancellation / no-show fee policy. IT IS HIGHLY IMPORTANT THAT YOU LISTEN TO THE MESSAGE / READ THE
EMAIL IN ITS ENTIRETY AND CONFIRM YOUR APPOINTMENT ACCORDINGLY. PLEASE ADD
THIS ADDRESS TO YOUR CONTACTS/ADDRESS BOOK: [email protected]
We would also like to ask, on this occasion, that you update your contact information in our system for us to be able to deliver those reminders to you. Please fill out this registration form for MSWH & AutoRemind and we will implement your request right away.
From now on, there is no more reason to forget your appointments –
just request an AutoReminder that’ll fit your needs!
Name
Address
City: State: ZIP:Preferred telephone # ( ) Cell or home?Preferred secondary telephone #
( ) Cell or home?
Email address
Preferred reminder method – Please answer by CIRCLING 1 option only in all three preference questions below.
3 days in advance of your appointment: (CONFIRMATION)
email cell home text
If not confirmed, 2 days in advance of your appointment: (CONFIRMATION) email cell text home (AFTER 6 p.m.)
OPTIONAL- Would you also like a REMINDER the day before your appointment? * THE ONLY METHOD AVAILABLE HERE IS VIA EMAIL. YES or NO
PLEASE ADD THIS ADDRESS TO YOUR CONTACTS/ADDRESS BOOK: [email protected]
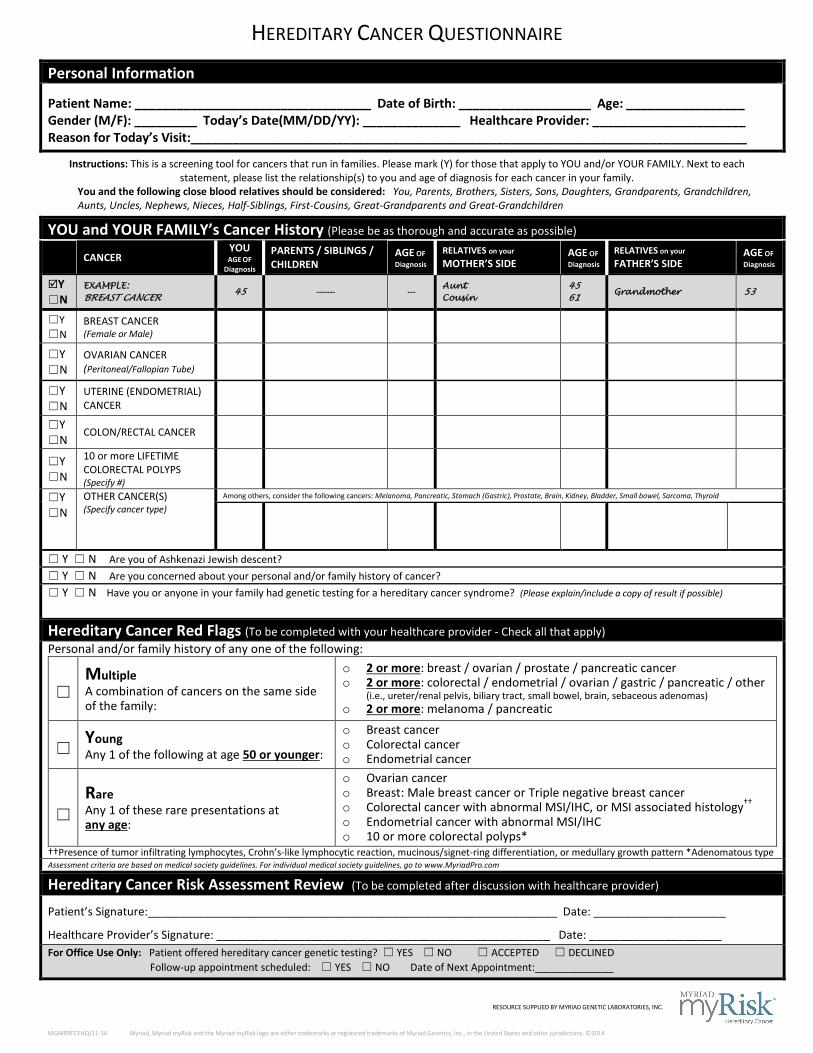
HEREDITARY CANCER QUESTIONNAIRE
Personal Information
Patient Name: __________________________________ Date of Birth: ___________________ Age: _________________ Gender (M/F): _________ Today’s Date(MM/DD/YY): ______________ Healthcare Provider: ______________________ Reason for Today’s Visit:________________________________________________________________________________
Instructions: This is a screening tool for cancers that run in families. Please mark (Y) for those that apply to YOU and/or YOUR FAMILY. Next to each statement, please list the relationship(s) to you and age of diagnosis for each cancer in your family.
You and the following close blood relatives should be considered: You, Parents, Brothers, Sisters, Sons, Daughters, Grandparents, Grandchildren, Aunts, Uncles, Nephews, Nieces, Half-Siblings, First-Cousins, Great-Grandparents and Great-Grandchildren
YOU and YOUR FAMILY’s Cancer History (Please be as thorough and accurate as possible)
CANCER YOU AGE OF
Diagnosis PARENTS / SIBLINGS / CHILDREN
AGE OF Diagnosis
RELATIVES on your MOTHER’S SIDE
AGE OF Diagnosis
RELATIVES on your FATHER’S SIDE
AGE OF Diagnosis
Y ☐N
EXAMPLE: BREAST CANCER
45 ------- --- Aunt Cousin
45 61
Grandmother 53
☐Y ☐N
BREAST CANCER (Female or Male)
☐Y ☐N
OVARIAN CANCER (Peritoneal/Fallopian Tube)
☐Y ☐N
UTERINE (ENDOMETRIAL) CANCER
☐Y ☐N
COLON/RECTAL CANCER
☐Y ☐N
10 or more LIFETIME COLORECTAL POLYPS (Specify #)
☐Y ☐N
OTHER CANCER(S) (Specify cancer type)
Among others, consider the following cancers: Melanoma, Pancreatic, Stomach (Gastric), Prostate, Brain, Kidney, Bladder, Small bowel, Sarcoma, Thyroid
☐ Y ☐ N Are you of Ashkenazi Jewish descent? ☐ Y ☐ N Are you concerned about your personal and/or family history of cancer? ☐ Y ☐ N Have you or anyone in your family had genetic testing for a hereditary cancer syndrome? (Please explain/include a copy of result if possible)
Hereditary Cancer Red Flags (To be completed with your healthcare provider - Check all that apply) Personal and/or family history of any one of the following:
☐
Multiple A combination of cancers on the same side of the family:
o 2 or more: breast / ovarian / prostate / pancreatic cancer o 2 or more: colorectal / endometrial / ovarian / gastric / pancreatic / other
(i.e., ureter/renal pelvis, biliary tract, small bowel, brain, sebaceous adenomas) o 2 or more: melanoma / pancreatic
☐ Young
Any 1 of the following at age 50 or younger:
o Breast cancer o Colorectal cancer o Endometrial cancer
☐
Rare Any 1 of these rare presentations at any age:
o Ovarian cancer o Breast: Male breast cancer or Triple negative breast cancer o Colorectal cancer with abnormal MSI/IHC, or MSI associated histology†† o Endometrial cancer with abnormal MSI/IHC o 10 or more colorectal polyps*
††Presence of tumor infiltrating lymphocytes, Crohn’s-like lymphocytic reaction, mucinous/signet-ring differentiation, or medullary growth pattern *Adenomatous type Assessment criteria are based on medical society guidelines. For individual medical society guidelines, go to www.MyriadPro.com
Hereditary Cancer Risk Assessment Review (To be completed after discussion with healthcare provider) Patient’s Signature:_________________________________________________________________ Date: _____________________
Healthcare Provider’s Signature: _____________________________________________________ Date: _____________________ For Office Use Only: Patient offered hereditary cancer genetic testing? ☐ YES ☐ NO ☐ ACCEPTED ☐ DECLINED Follow-up appointment scheduled: ☐ YES ☐ NO Date of Next Appointment:______________
RESOURCE SUPPLIED BY MYRIAD GENETIC LABORATORIES, INC.
MGMRRFCFHQ/11-14 Myriad, Myriad myRisk and the Myriad myRisk logo are either trademarks or registered trademarks of Myriad Genetics, Inc., in the United States and other jurisdictions. ©2014

Mansion St Women’s Health, P.L.L.C, 215 E. Mansion Street, Suite 3D, Marshall, MI 49068 (FAX 269-781-9248)
3600 Capital Ave. SW, Suite 205, Battle Creek, MI 49015 (FAX 269-719-8046)
Authorization for Disclosure of Health Information
Patient Name: _____________________Maiden Name: _____________ SSN: _____________ Date of Birth: ___________Home Phone: _______________ Cell/Work:__________________ Address: _____________________________ City/State/ZIP:___________________________ Email Address:________________________________________________________________ I hereby authorize the following people the designated information as marked below: Name: ___________________________________ Relationship:_______________________ ___ Billing/ Insurance ___Appointments/Scheduling ___Physician Office Notes ___Pathology/Lab Results ___Radiology Reports ___Operative/Procedure Reports Name:___________________________________Relationship:________________________ ___ Billing/ Insurance ___Appointments/Scheduling ___Physician Office Notes ___Pathology/Lab Results ___Radiology Reports ___Operative/Procedure Reports
I do not wish to have any information disclosed to anyone but myself. ___ I understand that authorizing the disclosure of this health information is voluntary. ___I understand I may refuse to sign this authorization and that my refusal to sign will not affect my ability to obtain treatment or payment or my eligibility for benefits. ___ I understand I may revoke this authorization in writing at any time by giving written notice to the Mansion Street Women’s Health, P.L.L.C, Office Manager, except to the extent that action has been taken in reliance on this authorization. I have read the information provided on this release and do hereby acknowledge that I fully understand the terms and conditions of this authorization. This document may be scanned into an electronic format and such printed copy of the electronic record shall be deemed an original. ______________________________________ ____________________________ ____________ Printed Name of Patient or Responsible Party (if minor) Signature of Patient or Responsible Party Date __________________________________________ _________ MSWH Employee Witness Signature Date

WHAT EVERY PATIENT SHOULD KNOW.
MANSION STREET WOMEN’S HEALTH, PLLC
NOTICE OF PRIVACY PRACTICES
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. If you have any questions about this Notice, please contact our Privacy Officer, Dr. Mark Walker at (269) 781-1183.
PROVIDERS COVERED BY THIS NOTICE
Mansion Street Women’s Health, PLLC is required by law to maintain the privacy of your health information, to provide you with this Notice of our legal duties and privacy practices, and to abide by the terms of this Notice currently in effect. We may share your health information for purposes of providing you with treatment, obtaining payment for medical services, and for health care operations. Examples of sharing information for purposes of treatment, payment, and health care operations are described below.
OUR PLEDGE TO YOU:
We understand that health information about you and your health care is personal. We are committed to protecting health information about you. We create a record of the care and services you receive from us. We need this record to provide you with quality care, bill for your care, and comply with legal requirements. This Notice applies to all of the records of your care that we maintain, whether made by our staff, or by the physicians and other health care professionals working with us.
HOW WE MAY USE AND DISCLOSE HEALTH INFORMATION ABOUT YOU.
Our doctors, nurses, and other health care professionals may use health information about you to provide you with health care treatment or services. We may also disclose health information about you to others who are involved in taking care of you. For example, we may send health information about you to a physician specialist as part of a referral. Or, we may share information with a local nursing home in order to continue your care. We may use and disclose health information about you to obtain payment for the treatment and services you receive from us or from the doctors and other health care professionals that treat you. For example, we may send billing information to your insurance company or Medicare. We may use and disclose health information about you to support our health care operations. For example, we may use health information to review the treatment and services we provide to you and to evaluate the performance of our staff in caring for you. Unless you object, we may disclose information to a family member or other person responsible for your care about your condition, status, and location. Unless you tell us otherwise, we will include your name, location, your general condition (good, fair, etc.), and religious affiliation in our patient directory and make this information available to anyone who asks for you by name. Unless you object, we may disclose this information to a member of the clergy. We may use and disclose health information to contact you for an appointment reminder, to tell you about health-related services or to recommend possible treatment options or alternatives that may be of interest to you. We may contact you about supporting our fund raising efforts. Subject to certain requirements, we may use or disclose health information about you without your prior authorization for other reasons:

We may give out health information about you for public health purposes; to report abuse or neglect; for health oversight reviews; in research studies, so long as provision is made for the protection of your health information; to medical examiners; for funeral arrangements and organ donation; in response to special law enforcement requests, valid judicial or administrative orders, or for authorized national security and intelligence activities; for workers’ compensation purposes; to avert a serious threat to your health or safety or those of the public or another person; and when required by law (for example, state law requires certain reports to cancer registries). If you are or were a member of the armed forces, we may release information about you as required by military command authorities or the Department of Veterans Affairs. If you are an inmate of a correctional institution or under the custody of a law enforcement official, we may release health information about you to the correctional institution or law enforcement official. We must also release your health information when required by the Department of Health and Human Services to investigate our compliance with the privacy laws. Both federal and state laws protect your health information. In situations where both laws apply, we will comply with the law that is most protective of your health information and/or gives you additional rights. For example, in some situations Michigan law gives more protection to information contained in mental health records. For any other purpose not covered by this Notice, we will ask for your written authorization before using or disclosing your health information. You may revoke this authorization at any time by notifying us in writing, except to the extent we have taken an action in reliance on your authorization.
YOUR RIGHTS REGARDING HEALTH INFORMATION ABOUT YOU.
You have the right to request in writing that you inspect and obtain a copy of the health information we maintain. We may charge a fee for the costs of copying, mailing or other supplies and services associated with your request. In certain circumstances, we may deny your request. You may request that this denial be reviewed. If you believe that health information we have about you is incorrect or incomplete, you may ask us to amend your health information. The request must be in writing, and should state the reason for the amendment and the specific information to be amended. You have the right to make a written request for a list of disclosures we have made of your health information. This list will not include disclosures made for treatment, payment, and health care operations, to your family, or those disclosures you authorized. You have the right to request a restriction on the health information we use or disclose about you, including a right to request restrictions on disclosures to family members or friends. You must submit this request in writing. We are not required to agree to your request for restrictions. If we do agree, we will comply with your request unless the information is needed to provide you emergency treatment, or we are otherwise required by law to make a disclosure. You have the right to request that confidential communications with you be made in an alternative manner or location. This request must be in writing, but you do not need to state the reason for your request. For example, you may ask us to send information to your work address instead of your home address, or in a blank envelope with no distinguishing marks. We will accommodate all reasonable requests. Your request must specify how or where you wish to be contacted.
WRITTEN REQUESTS
All written requests should be submitted to our Privacy Officer, Dr. Mark Walker at 215 East Mansion Street, Suite 3D, Marshall, MI 49068.
COPIES OF NOTICE AND CHANGES
You have the right to obtain a paper copy of this Notice at any time, upon request, even if you have agreed to accept this Notice electronically. You may also obtain a copy of this Notice at our website, www.mansionstreetwh.com
We reserve the right to change this Notice, and to make the changed Notice effective for health information we already have about you as well as any information we receive in the future. Upon your request, we will provide you with any revised Notice. A revised Notice will also be posted in waiting areas throughout our facilities and at our website, www.mansionstreetwh.com
COMPLAINTS
If you are concerned that your privacy rights may have been violated or you disagree with a decision we make about your health information, you may file a complaint with our Privacy Officer, Dr. Mark Walker. You may also send a written complaint to the U.S. Department of Health and Human Services. Our Privacy Officer, Dr. Mark Walker can provide you with the address.
Under no circumstances will we ever ask you to waive your rights under this Notice or retaliate against you in any manner for filing a complaint.
EFFECTIVE DATE
This Notice was published and became effective on February 1, 2014.
Patient Rights--These rights apply to our patients and/or their legal representatives.
1. Be informed of their rights prior to the institution or discontinuance of care. 2. Receive information in a language that can be understood. 3. Be given considerate and respectful care in a safe setting, without discrimination. 4. Personal privacy in a confidential and secure environment, in accordance with HIPAA regulations. 5. Exercise civil and religious liberties. 6. Be informed of choices. 7. Participate in the plan of care, make decisions regarding that care, and accept or refuse treatment, the
risks, benefits, other options and prospects for recovery. 8. Participate in ethical questions, conflict resolution, organ donation, withdrawal of life-sustaining
treatment and withholding resuscitation. 9. Effective pain management. 10. The use of advance directives. 11. Access personal medical records. 12. Protective services. 13. Be informed of and refuse to participate in human experimentation or other research. 14. Charges and billing information. 15. Be informed of unanticipated outcome.
Patient Responsibilities
• A patient is responsible for following the office rules and regulations affecting patient care and conduct. • A patient is responsible for providing a complete and accurate medical history. • A patient is responsible for making it known whether he or she clearly comprehends a contemplated
course of action, consents to it, and understands the actions expected. • A patient is responsible for following the recommendations and advice prescribed in a course of
treatment by the physician. • A patient is responsible for providing information about unexpected complications that arise in an
expected course of treatment. • A patient is responsible for being considerate of the rights of other patients and office personnel and
property. • A patient is responsible for providing the office with accurate and timely information concerning his or
her sources of payment and ability to meet financial obligations. • A patient is responsible for any personal property brought into the office.
Mansion Street Women’s Health, P.L.L.C. ACKNOWLEDGMENT OF RECEIPT OF PRIVACY NOTICE
By signing below, I acknowledge that I have received Mansion Street Women’s Health, P.L.L.C.’s Notice of Privacy Practices. This document may be scanned into an electronic format and such printed copy of the electronic record shall be deemed an original.
_________________________________ Date________________Signature: (Patient or Authorized Representative)
_________________________________Printed Name: (Patient or Authorized Representative)
_________________________________MSWH Employee Signature
MSWH Acknowledgment of Receipt of Privacy Notice 01/01/2011
AcknowledgmentReceiptPrivacyNotice.pdf 1 2/13/15 2:24 PM

Welcome to Mansion Street Women’s Health. This form contains questions about your medical, obstetrical, family, and social histories. This information is vital to us. Please answer the questions to the best of your knowledge. We realize that some of our patients have previously filled out this information; however, we need this to update our records. Leave blank any questions you do not know. Your answers are kept confidential. Thank you very much!
Name: ______________________________ ____________________________ _________
Today's Date: _____________________
(last) (first) (MI)
How old is the father of the baby? ______________ Does he have any health issues?________________________
Father of the baby’s full name: _________________________ Is this the same father as your previous children? Yes / No
Are you and the father of the baby related to each other at all? ie cousins, etc? Yes / No
Is there any family history on either sides of your families of: (Please circle yes or no. If yes, say whom.)
Cerebral Palsy Yes / No If yes, whom? __________________
Cleft Lip or palate Yes / No If yes, whom? __________________
Congenital anomalies (birth defects) Yes / No If yes, whom? __________________
Heart Defects Yes / No If yes, whom? __________________
Down syndrome Yes / No If yes, whom? __________________Huntington’s Chorea Yes / No If yes, whom? __________________Alpha or Beta Thalasemia Yes / No If yes, whom? __________________Cystic Fibrosis Yes / No If yes, whom? __________________Hemophilia Yes / No If yes, whom? __________________Mental Retardation Yes / No If yes, whom? __________________Muscular Dystrophy Yes / No If yes, whom? __________________Neural Tube Defect like Spina Bifida Yes / No If yes, whom? __________________ Sickle Cell Yes / No If yes, whom? __________________Radiation Exposure Yes / No If yes, whom? __________________Tay Sach’s disease Yes / No If yes, whom? __________________Other chromosomal abnormalities I.E. Trisomy 18
Yes / No If yes, whom? __________________
Do you follow a vegetarian, vegan or other specific diet?! ! Yes / NoDo you feel your basic needs are met? ie Home, food, clothing?! Yes / NoAny guns in the house? !! Yes / No! Are they locked up? ! ! Yes / NoDo you feel safe with your current partner?! Yes / No If no, explain: ___________________________________Who do you live with?! __________________________________Are you up to date on your vaccinations? ! Tetanus? ! Yes / No Flu? ! Yes / No
Previous OB history:Any problems with your previous pregnancies? Yes / No If yes, explain: _______________________________! Preterm labor/delivery! ! ! Yes / No If yes, how many weeks were you? _______________________________________
! Baby did not grow well or was too big ! Yes / No What did he / she weigh? _____________________________________________________________________________
! Diabetes! ! ! ! Yes / No Diet only or Insulin? ____________________________! High blood pressure! ! ! Yes / No! Infections! ! ! ! Yes / No If yes, what kind? ______________________________! Health problems with baby after birth! Yes / No If yes, explain: ________________________________! Heavy bleeding after delivery requiring meds or surgery! ! Yes / No! Low platlet count! ! ! Yes / No! Clotting problems ie DVT/PE! ! Yes / NoPrevious problems with anesthesia! ! Yes / No If yes, explain: ___________________________________Family history of severe anesthesia problems ie Malignant Hyperthermia !! ! Yes / NoAny other clotting disorders you are aware of ie Factor 5, antiphospholipid syndrome! Yes / NoHistory of severe anemias like Sickle Cell! ! ! ! ! ! Yes / No
Mansion Street Women’s Health, P.L.L.C. PREGNANCY QUESTIONNAIRE
DOB: ___________________