
Maneesh sharma
148
1 management of patient with management of patient with GI disorder GI disorder PRESENTED BY PRESENTED BY Mr. Maneesh Sharma Mr. Maneesh Sharma AIIMS, Rishikesh AIIMS, Rishikesh
-
Upload
manish-sharma -
Category
Health & Medicine
-
view
164 -
download
0
Transcript of Maneesh sharma

1
management of patient management of patient with GI disorder with GI disorder
PRESENTED BY PRESENTED BY
Mr. Maneesh SharmaMr. Maneesh Sharma
AIIMS, RishikeshAIIMS, Rishikesh

2
The Anatomy & physiology of Digestive System

3
Digestive System Organization

4
Anatomy of the Mouth and Throat
5
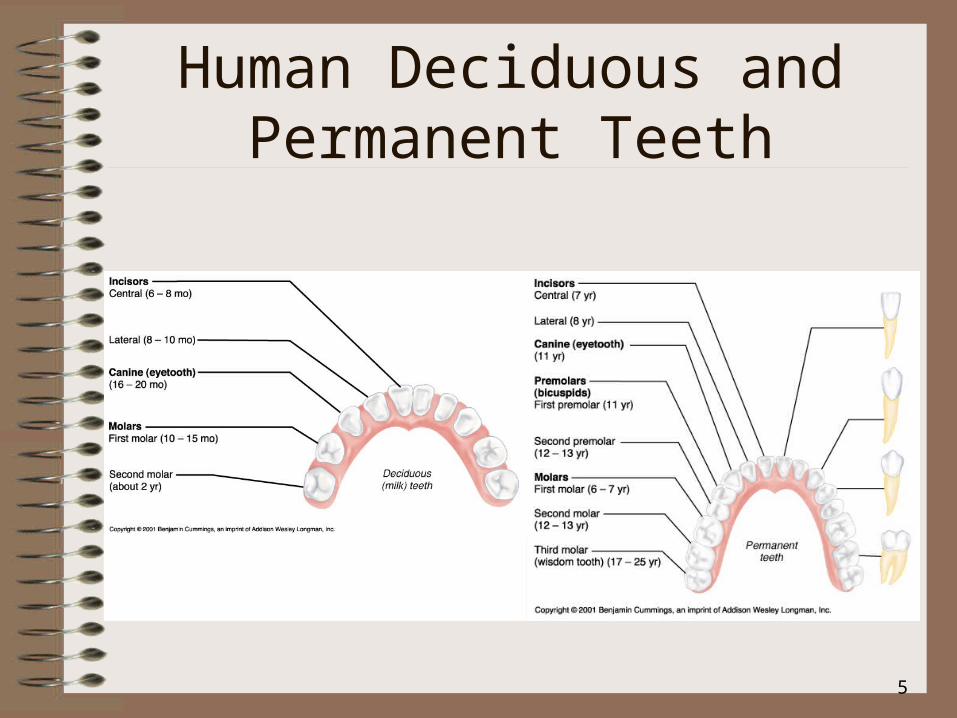
Human Deciduous and Permanent Teeth
6
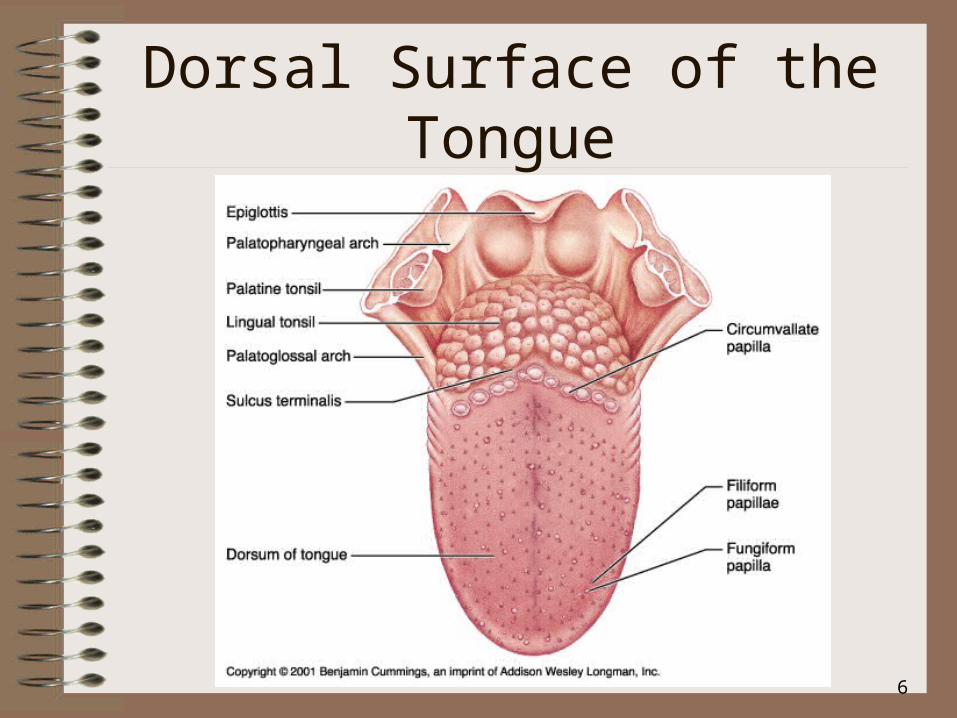
Dorsal Surface of the Tongue

7
The Major Salivary Glands

8
Peristalsis and Segmentation

9
Anatomy of the Stomach

10
Stomach

11
Small Intestine

12
Structure of the Villi in the Small Intestine

13
Anatomy of the Large Intestine

14
Liver

15
Liver

16
Liver
17
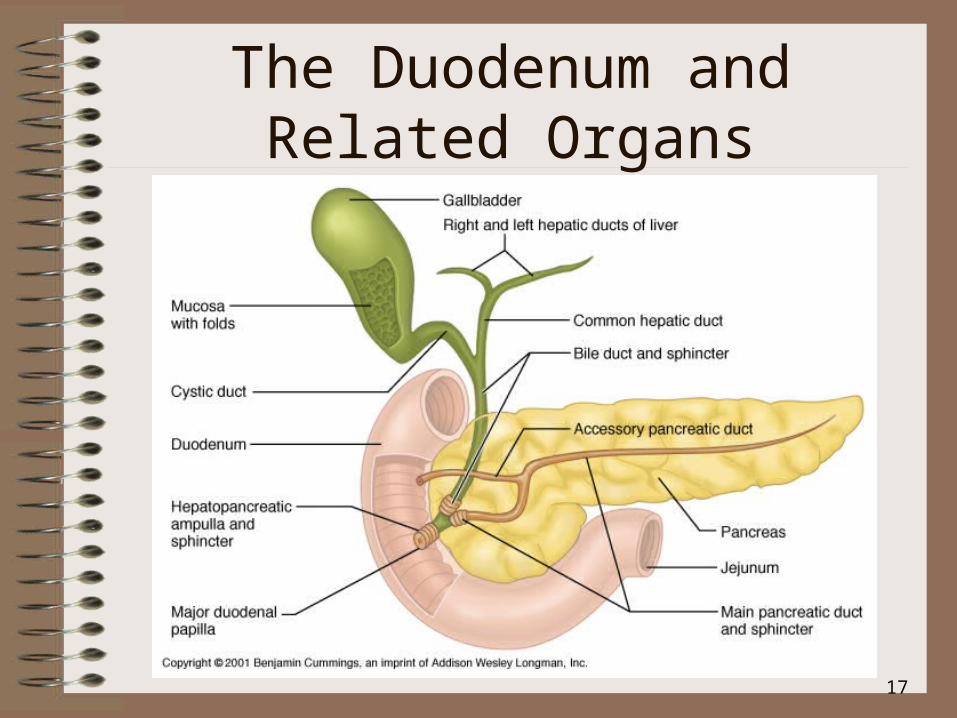
The Duodenum and Related Organs

18
The Organs and Positions in the Abdominal Cavity

19
Structures of the Alimentary Canal

20
•DIAGNOSTIC EXAMINATION OF
GI DISORDER

21
Diagnostic evaluation
• LIST OF EXAMINATIONS
• STOOL TESTS• BREATH TESTS• ABDOMINAL ULTRASONOGRAPHY• DNA TESTING• IMAGING STUDIES• UPPER GASTROINTESTINAL TRACT
STUDY

22
• LOWER GASTROINTESTINAL TRACT STUDY
• COMPUTED TOMOGRAPHY• MAGNETIC RESONANCE IMAGING• SCINTIGRAPHY• GASTROINTESTINAL MOTILITY STUDIES • ENDOSCOPE PROCEDURE• UPPER GASTROINTESTINAL
FIBROSCOPY/
To be cont….

23
To be cont….
• ESOPHAGOGASTRODUDENOSCOPY• ANOSCOPY, PROCTOSCOPY,
SIGMOIDSCOPY• FIBEROPTIC COLONOSCOPY• SMALL BOWEL ENTEROSCOPY• ENDOSCOPY THROUGH OSTOMY• MANOMETRY AND
ELECTROPHYSIOLOGIC STUDIES• DEFECOGRAPHY• LAPAROSCOPY(PERITONEOSCOPY)

24
Management of patient with Upper Gastrointestinal Disorders

25
Care of Clients with Disorder of the Mouth
Disorder includes inflammation, infection, neoplastic lesions
PATHOPHYSIOLOGY 1. Causes include mechanical trauma,
irritants such as tobacco, chemotherapeutic agents
2. Oral mucosa is relatively thin, has rich blood supply, exposed to environment
26
Cont…….
•manifestation

27

28
Cont…….
•Nursing care

29
•ORAL CANCER

30
Client with Oral Cancer
1.Background
•

31
cont……………….
2. Pathophysiology• a. Squamous cell carcinomas• b. Begin as painless oral ulceration or
lesion with irregular, ill-defined borders• c. Lesions start in mucosa and may
advance to involve tongue, oropharynx, mandible, maxilla
• d. Non-healing lesions should be evaluated for malignancy after one week of treatment

32
cont……………..
4. a. Nursing Care b. Nursing Diagnoses• 1. Risk for ineffective airway clearance• 2. Imbalanced Nutrition: Less than body
requirements• 3. Impaired Verbal Communication:
establishment of specific communication plan and method should be done prior to any surgery
• 4. Disturbed Body Image

33
•DISEASE OF ESOPHAGEOUS
• 1. G.E.R.D.

34
Gastroesophageal Reflux Disease (GERD)
1. Definition

35
cont……………..
2. Pathophysiology• a. Gastroesophageal reflux results from transient
relaxation or incompetence of lower esophageal sphincter, sphincter, or increased pressure within stomach
• b. Factors contributing to gastroesophageal reflux 1.Increased gastric volume (post meals) 2.Position pushing gastric contents close to
gastroesophageal juncture (such as bending or lying down) 3.Increased gastric pressure (obesity or tight clothing) 4.Hiatal hernia
36
cont……………..
• c. Normally the peristalsis in esophagus and bicarbonate in salivary secretions neutralize any gastric juices (acidic) that contact the esophagus; during sleep and with gastroesophageal reflux esophageal mucosa is damaged and inflamed; prolonged exposure causes ulceration, friable mucosa, and bleeding; untreated there is scarring and stricture
3. Manifestations

37

38

39

40
cont………………
4. Complication

41
Cont…..
5. Diagnostic examination

42
cont…………….
6. Medications

43
cont………………..
7.Dietary management

44
cont……………..
8.Surgery indicated for persons not improved by diet and life style changes
• a. Laparoscopic procedures to tighten lower esophageal sphincter
• b. Open surgical procedure

45
2. HITAL HERNIA

46
Hiatal Hernia
1.Definition
2.Predisposing factors include: – Increased intra-abdominal pressure– Increased age– Trauma– Congenital weakness– Forced recumbent position

47
cont…………………
TYPES• d. Sliding hiatal hernia: gastroesophageal
junction and fundus of stomach slide through the esophageal hiatus
• e. Paraesophageal hiatal hernia: the gastroesophageal junction is in normal place but part of stomach herniates through esophageal hiatus; hernia can become strangulated; client may develop gastritis with bleeding

48

49
CONT…………CONT…………
3. Manifestations: Similar to GERD
4. Diagnostic Test5. Treatment

50

51
3.ESOPHAGEAL CANCER

52
2. Pathophysiology• a. Squamous cell carcinoma
1.Most common affecting middle or distal portion of esophagus
2.More common in African Americans than Caucasians
3.Risk factors cigarette smoking and chronic alcohol use
• b. Adenocarcinoma1.Nearly as common as squamous cell
affecting distal portion of esophagus2.More common in Caucasians3.Associated with Barrett’s esophagus,
complication of chronic GERD and achalasia

53
CONT………
3. Manifestations

54
CONT……………
4. Diagnostic Tests

55
CONT……………
6. TREATMENTS
56
4.Impaired esophageal motility
57
5.UPPER GI BLEED

58
6.Nursing process of esophageal
disorder

59
•DISORDER OF GASTRIC AND
DUDENAL ULCER

60
1.GASTRITIS

61
Gastritis
1. Definition
2. Types
62
CONT……………
3. Causes of acute gastritis
5. Manifestations

63
CONT……………6.Treatment• a. NPO status to rest GI tract for 6 – 12
hours, • b. Medications: proton-pump inhibitor or
H2-receptor blocker; sucralfate (carafate) acts locally; coats and protects gastric mucosa
• c. If gastritis from corrosive substance: immediate dilution and removal of substance by gastric lavage (washing out stomach contents via nasogastric tube), no vomiting

64
Chronic Gastritis
1.Definition2. Manifestations3. Treatment:
65
CONT……………
4. Diagnostic Tests

66
Cont…….
5.Nursing process of gastritis & gastrostomy

67
2.PEPTIC ULCER
DISEASE

68
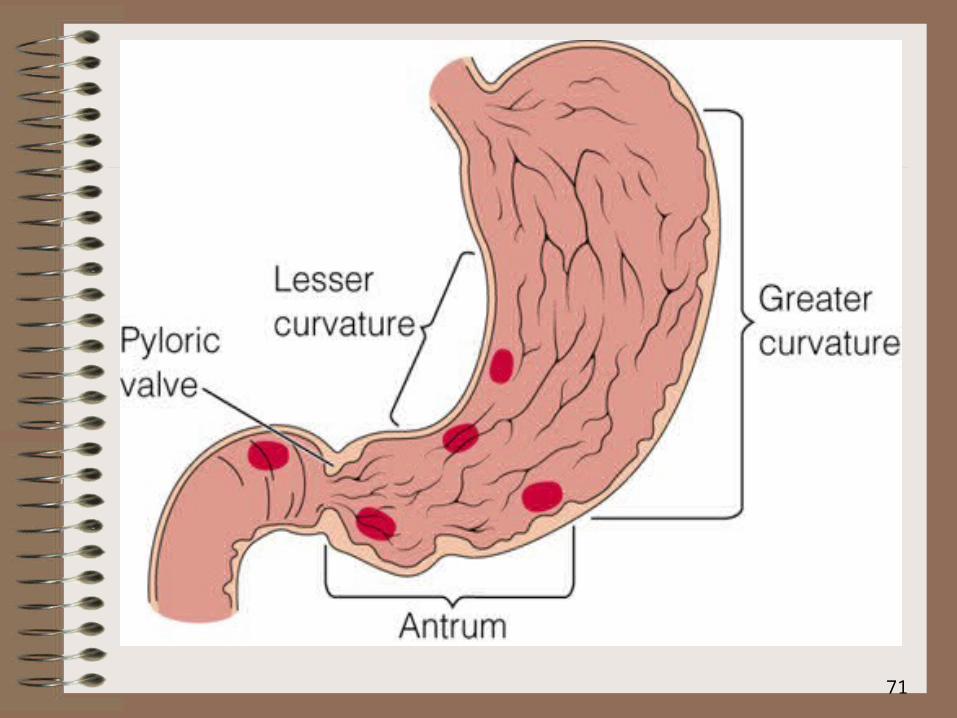
Peptic Ulcer Disease (PUD)
1. Definition and Risk factors

69
CONT……..
2. Pathophysiology• a. Ulcers or breaks in mucosa of GI tract occur
with 1.H. pylori infection (spread by oral to oral,
fecal-oral routes) damages gastric epithelial cells reducing effectiveness of gastric mucus
2.Use of NSAIDS: interrupts prostaglandin synthesis which maintains mucous barrier of gastric mucosa
• b. Chronic with spontaneous remissions and exacerbations associated with trauma, infection, physical or psychological stress

70
71

72

73
CONT……..
74
CONT……..
3. Diagnosis3. Diagnosis3. Diagnosis3. Diagnosis3. Diagnosis

75
CONT……..
3.Manifestations

76
CONT……..
4. Treatment

77
CONT……..
1. Pharmacological management

78
CONT……..
•NG suction
•Surgical intervention

79
Billroth I(GASTRO-DUODNEOSTOMY)

80
Billroth II (GASTRO-JEJUNOSTOMY)

81
CONT……..
5.Complications

82
6.Nursing process of peptic ulcer disease

83
•CANCER OF STOMACH

84
Cancer of Stomach
1. Incidence

85
Colon Cancer
86
CONT……..
3. Risk Factors4.Manifestations

87
CONT……..
6. Diagnostic Tests

88
CONT……..
7.Treatment

89
CONT……..
8. dietary management:
90
Cancer of the Stomach
9. Common post-op complications

91
•MANAGEMENT OF PATIENT WITH
LOWER GI DISORDER

92
•1. abnormalities of fecal elimination
93
2. PATIENT WITH BOWEL DISORDERS

94
Irritable Bowel Syndrome (IBS) (spastic bowel, functional colitis)
1. Definition
95
CONT………
2. Pathophysiology• a. Appears there is altered CNS regulation of
motor and sensory functions of bowel1.Increased bowel activity in response to food
intake, hormones, stress2.Increased sensations of chyme movement
through gut3.Hypersecretion of colonic mucus
• b. Lower visceral pain threshold causing abdominal pain and bloating with normal levels of gas
• c. Some linkage of depression and anxiety

96
CONT………
3. Manifestations

97
CONT………
4. Diagnostic Tests:
•

98
CONT……..
5. Medications
99
CONT……..
6. Dietary Management

100
•PATIENT WITH INFLAMMATORY
DISORDER

101
Client with Inflammatory Bowel Client with Inflammatory Bowel DiseaseDisease
Definition• a. Includes 2 separate but closely related
conditions: ulcerative colitis and Crohn’s disease; both have similar geographic distribution and genetic component
• b. Etiology is unknown but runs in families; may be related to infectious agent and altered immune responses
• c. Peak incidence occurs between the ages of 15 – 35; second peak 60 – 80
• d. Chronic disease with recurrent exacerbations

102
CONT………

103
•CROHN’S DISEASE

104
Crohn’s disease

105
CONT……….
1. Manifestations

106
CONT….
2. Complications

107
CONT……….
3. Diagnostic Tests

108
CONT……….
4. Medications

109
CONT……….
5. Dietary Management
6. Surgery

110
•Ulcerative Colitis

111
Ulcerative Colitis
1. Pathophysiology• 1. Inflammatory process usually confined
to rectum and sigmoid colon • 2. Inflammation leads to mucosal
hemorrhages and abscess formation, which leads to necrosis and sloughing of bowel mucosa
• 3. Mucosa becomes red, friable, and ulcerated; bleeding is common
• 4. Chronic inflammation leads to atrophy, narrowing, and shortening of colon

112
CONT……..
2. Manifestations

113
CONT……..
3. Complications

114
CONT……..
4. Diet therapy

115
CONT……
5. SURGICAL MANAGEMENT Ostomy• 1. Surgically created opening between
intestine and abdominal wall that allows passage of fecal material
• 2. Stoma is the surface opening which has an appliance applied to retain stool and is emptied at intervals
• 3. Name of ostomy depends on location of stoma
•

116
CONT……• Surgical Management
– 25% of patients require a colectomy– Total proctocolectomy with a permanent
ileostomy• Colon, rectum, anus removed
• Closure of anus
• Stoma in right lower quadrant

117
CONT……
•7. Treatment– Medications similar to treatment for
Crohn’s disease

118
8. Nursing process of inflammatory bowel disease

119
• ACUTE INFLAMMATORY
INTESTINAL DISORDER

120
•APPENDICITIS

121
•
• Appendicitis:
• most common reason for abdominal surgery, appendix becomes inflamed from obstruction, may become pus filled– Clinical manifestations: – Assessment and Diagnostic

122
CONT…………
– Complications: – Medical Management: – Nursing Management: – Surgery may be outpatient, if complications of
peritonitis are suspected pt may remain in hospital for several days

123
•DIVERTICULAR DISEASE

124
Client with Diverticular Disease
1. Definition• a. Diverticula are saclike projections
of mucosa through muscular layer of colon mainly in sigmoid colon
• b. Incidence increases with age; less than a third of persons with diverticulosis develop symptoms
2. Risk Factors
125
CONT………….
3. Pathophysiology• a. Diverticulosis is the presence of diverticula
which form due to increased pressure within bowel lumen causing bowel mucosa to herniate through defects in colon wall, causing outpouchings
• b. Muscle in bowel wall thickens narrowing bowel lumen and increasing intraluminal pressure
• c. Complications of diverticulosis include hemorrhage and diverticulitis, the inflammation of the diverticular sac

126
CONT………..
• d. Diverticulitis: diverticulum in sigmoid colon irritated with undigested food and bacteria forming a hard mass (fecalith) that impairs blood supply leading to perforation
• e. With microscopic perforation, inflammation is localized; more extensive perforation may lead to peritonitis or abscess formation

127
Diverticulits

128
Diverticulitis

129
CONT………..
5. Manifestations
6. Complications
130
CONT………..
7. Diagnostic Tests
131
CONT………..
8. Medications

132
CONT………..
9. Dietary Management

133
CONT………..
10. Surgery• a. Surgical intervention indicated for
clients with generalized peritonitis or abscess that does not respond to treatment
• b. With acute infection, 2 stage Hartman procedure done with temporary colostomy; re-anastomosis performed 2 – 3 months later

134
Cont……..
11. Nursing process of Diverticulitis

135
•Patient with intestinal obstruction

136
•Small & large intestine disorder

137
•NEOPLASTIC DISORDER

138
Neoplastic DisordersNeoplastic Disorders
Background• 1. Large intestine and rectum most
common GI site affected by cancer• 2. Colon cancer is second leading cause of
death from cancer in U.S.
Client with Polyps1. Definition

139
CONT……..
2. Manifestations

140
CONT……..
Nursing Care
• a. All clients advised to have screening colonoscopy at age 50 and every 5 years thereafter (polyps need 5 years of growth for significant malignancy)
• b. Bowel preparation ordered prior to colonoscopy with cathartics and/or enemas

141
•COLORECTAL CANCER

142
Client with Colorectal Cancer
Definition• a. Third most common cancer diagnosed• b. Affects sexes equally• c. Five-year survival rate is 90%, with
early diagnosis and treatment Risk Factors

143
CONT……..Pathophysiology• a. Most malignancies begin as
adenomatous polyps and arise in rectum and sigmoid
• b. Spread by direct extension to involve entire bowel circumference and adjacent organs
• c. Metastasize to regional lymph nodes via lymphatic and circulatory systems to liver, lungs, brain, bones, and kidneys
Manifestations

144
Colon Cancer
145
CONT……..
Complications

146
CONT……..
Diagnostic Tests
147
CONT……..
Surgery• a. Surgical resection of tumor, adjacent
colon, and regional lymph nodes is treatment of choice
• b. Whenever possible anal sphincter is preserved and colostomy avoided
• c. Tumors of rectum are treated with abdominoperineal resection (A-P resection) in which sigmoid colon, rectum, and anus are removed through abdominal and perineal incisions and permanent colostomy created

148
•Nursing process of colorectal cancer


















![Monday the 5th January 2015 DAILY CAUSE LIST FOR MONDAY … · vs. shri vinod kumar agrawal maneesh sharma [ on admission] new delhi 4. taxc/58/2014 1 commissioner, central excise](https://static.fdocuments.in/doc/165x107/601f854cdfc947726271b10f/monday-the-5th-january-2015-daily-cause-list-for-monday-vs-shri-vinod-kumar-agrawal.jpg)