
Mandibulofacial dysostosis Bauru type syndrome: A new case
3
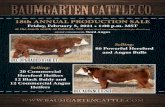
Letter to Editor Mandibulofacial Dysostosis Bauru Type Syndrome: A New Case To the Editor: Recently, Marc ¸ano and Richieri-Costa [1998] de- scribed a new autosomal dominant mandibulofacial dysostosis in a Brazilian family with five affected indi- viduals, in three generation comprising malar hypopla- sia, cleft lip with or without cleft palate, mild up- slanting palpebral fissures, and abnormal ears. Here, we report on a girl with mandibulofacial disostosis that resembles the patients described by Marc ¸ano and Rich- ieri-Costa [1998]. ACP (Fig. 1A and B) is the second child of young, healthy, nonconsanguineous parents with a normal sis- ter and no similar cases in the family. She was born normally after an uncomplicated pregnancy. Birth weight and length were 2,100 g (<3rd centile) and 46.0 cm (3rd centile), respectively. Neuropsychological de- velopment was normal. Evaluation at age 6 7/12 years showed weight of 22 kg (50th centile), height of 118 cm (50th centile), OFC of 50 cm (<50th centile). She had up-slanting palpebral fissures, high nasal bridge, ma- lar hypoplasia, Robin sequence with severe microgna- Fig. 1. Clinical aspects of the patient. *Correspondence to: R. M. Zechi-Ceide, Servic ¸o de Gene ´tica Clı ´nica, Hospital de Reabilitac ¸a ˜ o de Anomalias Craniofaciais, USP, CEP 17043-900, Bauru, SP, Brazil. Received 26 February 1999; Accepted 20 April 1999 American Journal of Medical Genetics 86:199–201 (1999) © 1999 Wiley-Liss, Inc.
-
Upload
maria-leine -
Category
Documents
-
view
225 -
download
0
Transcript of Mandibulofacial dysostosis Bauru type syndrome: A new case

Letter to Editor
Mandibulofacial Dysostosis Bauru Type Syndrome:A New Case
To the Editor:
Recently, Marcano and Richieri-Costa [1998] de-scribed a new autosomal dominant mandibulofacialdysostosis in a Brazilian family with five affected indi-viduals, in three generation comprising malar hypopla-sia, cleft lip with or without cleft palate, mild up-slanting palpebral fissures, and abnormal ears. Here,we report on a girl with mandibulofacial disostosis thatresembles the patients described by Marcano and Rich-ieri-Costa [1998].
ACP (Fig. 1A and B) is the second child of young,healthy, nonconsanguineous parents with a normal sis-ter and no similar cases in the family. She was bornnormally after an uncomplicated pregnancy. Birthweight and length were 2,100 g (<3rd centile) and 46.0cm (3rd centile), respectively. Neuropsychological de-velopment was normal. Evaluation at age 6 7/12 yearsshowed weight of 22 kg (50th centile), height of 118 cm(50th centile), OFC of 50 cm (<50th centile). She hadup-slanting palpebral fissures, high nasal bridge, ma-lar hypoplasia, Robin sequence with severe microgna-
Fig. 1. Clinical aspects of the patient.
*Correspondence to: R. M. Zechi-Ceide, Servico de GeneticaClınica, Hospital de Reabilitacao de Anomalias Craniofaciais,USP, CEP 17043-900, Bauru, SP, Brazil.
Received 26 February 1999; Accepted 20 April 1999
American Journal of Medical Genetics 86:199–201 (1999)
© 1999 Wiley-Liss, Inc.

Fig. 2. Patient 1 of the Marcano and Richieri-Costa study. Courtesy ofMarcano and Richieri-Costa.
Fig. 3. Patient 2 of the Marcano and Richieri-Costa study (mother ofpatient 1). Courtesy of Marcano and Richieri-Costa.
Fig. 4. Patient 3 of the Marcano and Richieri-Costa study (aunt of pa-tient 1). Courtesy of Marcano and Richieri-Costa.
Fig. 5. Patient 4 of the Marcano and Richieri-Costa study (uncle ofpatient 1). Courtesy of Marcano and Richieri-Costa.

thia, and hypoplastic tragus and ear lobes. Orthopan-tomography was normal.
The facial appearance of our patient was similar ofthat described by Marcano and Richieri-Costa [1998]with typical signs of mandibulofacial dysostosis (Figs.2–6). Concerning differential diagnosis, research inLondon Dysmorphology Database [Winter and Barait-ser, 1996], and Pictures of Standard Syndromes andUndiagnosed Malformations [Danks and Bankier,1998] yielded several mandibulofacial dysostoses with-out anomalies limb, which should be differentiatedfrom the present case, such as Treacher-Collins syn-drome (MIM-154500 [McKusick, 1997]), Hutteritemandibulofacial dysostosis [Lowry et al., 1985], Ver-loes-Lesenfants mandibulofacial dysostosis [Verloesand Lesenfants, 1997], and mandibulofacial dysostosisToriello type [Toriello et al., 1985; Zelante et al., 1993].Findings that distinguish our case from Treacher-Collins syndrome and Hutterite mandibulofacial dys-ostosis are, mainly, the absence of coloboma in theouter third of the lower lid and hypoplastic zygomata.In Verloes-Lesenfants mandibulofacial dysostosis, thestriking facial changes with macroblepharon and mac-rostomia clearly differentiates it from our case. Despitesimilar facial appearance of our patient and those withmandibulofacial dysostosis Toriello type (mainly withthe patient described by Zelante et al. [1993]), the lackof microcephaly and hearing loss are strong argumentsagainst it. Considering the similarity of the facial as-pect and clinical signs between our patient and those
previously reported by Marcano and Richieri-Costa, wesuggested that they have the same condition with vari-able expressivity. The absence of clinical findings inparents of our patient supports the possibility of a newmutation leading to this condition.
REFERENCESDanks D, Bankier A. 1998. POSSUM: pictures of standard syndromes and
undiagnosed malformations. Melbourne, Australia: Computer PowerGroup and The Murdock Institute for Research into Birth Defects.
Lowry RB, Morgan K, Holmes TM, Metcalf PJ, Stauffer GF. 1985. Man-dibulofacial dysostosis in Hutterite sibs: a possible recessive trait. AmJ Med Genet 22:501–512.
Marcano ACB, Richieri-Costa A. 1998. A newly recognized autosomal dom-inant mandibulofacial dysostosis (Bauru Type): report on a Brazilianfamily. J Dysmorph Speech Hear Dis 1:37–41.
McKusick VA. 1997. MIM: Mendelian inheritance in man. Baltimore: TheJohns Hopkins University Press and Aries Systems Corporation.
Toriello HV, Higgins JV, Abrahamson J, Waterman DF, Moore WD. 1985.X-linked syndrome of branchial arch and other defects. Am J MedGenet 21:137–142.
Verloes A, Lesenfants S. 1997. A new form of mandibulofacial dysostosiswith macroblepharon and macrostomia. Clin Dysmorph 6:21–24.
Winter RM, Baraitser M. 1996. LDDB: London dysmorphology database.Oxford: Oxford University Press.
Zelante L, Vigliaroli L, Mingarelli R, Dallapiccola B. 1993. Confirmation ofthe mandibulofacial dysostosis, Toriello Type. Am J Med Genet 45:534–535.
Roseli Maria Zechi-Ceide*Maria Leine Guion-AlmeidaHospital de Reabilitacao de Anomalias CraniofaciaisUniversidade de Sao PauloBauru, SP, Brazil
Fig. 6. Frontal view of the grandmother of patient 1 with patient 3 when child. Courtesy of Marcano and Richieri-Costa.
Letter to Editor 201










![PLANO DIRETOR DE ÁGUA DO MUNICÍPIO DE BAURU/SP€¦ · apresentado no Volume 02 Tomo I (Figura 3.2), conclui-se que o volume diário recalcado [PLANO DIRETOR DE ÁGUA – BAURU/SP]](https://static.fdocuments.in/doc/165x107/5f3f250013ec472fc161665a/plano-diretor-de-gua-do-municpio-de-baurusp-apresentado-no-volume-02-tomo-i.jpg)





