Mandibular Growth Anomalies || Tongue Reduction
4
CHAPTER 24 Tongue Reduction 24.1 Historical Background Orthodontists have long realized that the tongue can be an aetiological factor in abnormal toothposition. Many others, orthodontists as well as surgeons, were confront- ed with the tongue as a problem in relapse following their treatment. U. Rheinwald and R. Becker (1962) ex- pressed the opinion that in every case of the then -called mandibular prognathism, reduction in the size of the tongue should be considered before the definitive sur- gery. In the late 1950s we did a series of presurgical tongue reductions before we repositioned the mandible by a bilateral sagittal splitting procedure. In the German literature, the first tongue reduction was reported by H. Pichler (1948), performed at the request of his ortho- dontist L. Petrik. 24.2 Definition and Classification of Macroglossia I will define macroglossia as a tongue which is constant- ly or under certain conditions too large for that space of the oral cavity which is limited by the occluding rows of the teeth when they are normally positioned on the base of the jaw. My classification of macroglossia is the following (M. Mommaerts 1987): Idiopathic Macroglossia. This condition is rather rare. It causes protrusion mainly of the lower front teeth, pro- ducing interdental spaces, but can also shift the bicus- pids and even the molars laterally, producing a circular crossbite. The tongue looks large, is rather voluminous, but only slightly rounded on the dorsum. Macroglossia as a Sign of Acromegaly. Its reduction in size is as equally important before the correction of an acromegalic antemandibulism as is the removal of the causative pituitary gland adenoma. The tongue looks really voluminous. Macroglossia in Cases of Down's Syndrome and Debil- ity. In these cases the tongue has a rather typical form. It does not seem large or flat as in the genuine macroglos- sia case. This tongue looks roundish with a rather high dorsum. Its consistency is harder than that in the two types just mentioned above. It can cause speaking prob- lems and produce an open bite. Functional Macroglossia. In the resting position noth- ing seems to be wrong with the tongue, but it presses with abnormal force against the teeth. The patient is of- ten called a "tongue thruster". Tumorous Macroglossia. The enlargement is due to a tumour or tumour-like condition within its muscula- ture. Any kind of tumour in the tongue can produce such a macroglossia, a pure haemangioma or lympho- ma and mostly a lympho-haemangioma, a neuroma, a fibroma or neurofibromatosis as in cases of von Recklinghausen's disease, etc. Pseudo-macroglossia. This is that type of large, flat, flabby tongue which is often found within the large oral cavity in a case of macromandibulism or antemandibul- ism. It has no influence on the teeth or the position of the jaw. It has filled the space provided by the large jaw. The tongue does not need to be reduced in size when the mandible is pushed back and the oral cavity is re- duced in size. It adapts to the new condition without any negative consequences. 24.3 Surgical Problems As macroglossia was a well-known problem, several surgeons had reported their procedure to reduce the tongue size (Fig. lOla). Some removed just an oval wedge from the dorsum of the tongue. H. Pichler ( 1948) excised an additional oval piece from the tip. A rather large triangular piece of the tip of the tongue was ex- cised by U. Rheinwald (1957). His technique shortened the tongue but did not reduce its breadth. H. Kole (1970a) used a rather narrow excision in the tongue's midline and additionally a triangular excision of the tip. I myself have excised an oval piece from the tongue's midline area and in addition a triangular piece in the front of the tongue. We have published the procedure used, the results and the consequences (Egyedi and Obwegeser 1964). H. L. Obwegeser, Mandibular Growth Anomalies © Springer-Verlag Berlin Heidelberg 2001
Transcript of Mandibular Growth Anomalies || Tongue Reduction

CHAPTER 24
Tongue Reduction
24.1 Historical Background
Orthodontists have long realized that the tongue can be an aetiological factor in abnormal tooth position. Many others, orthodontists as well as surgeons, were confronted with the tongue as a problem in relapse following their treatment. U. Rheinwald and R. Becker (1962) expressed the opinion that in every case of the then -called mandibular prognathism, reduction in the size of the tongue should be considered before the definitive surgery. In the late 1950s we did a series of presurgical tongue reductions before we repositioned the mandible by a bilateral sagittal splitting procedure. In the German literature, the first tongue reduction was reported by H. Pichler (1948), performed at the request of his orthodontist L. Petrik.
24.2 Definition and Classification of Macroglossia
I will define macroglossia as a tongue which is constantly or under certain conditions too large for that space of the oral cavity which is limited by the occluding rows of the teeth when they are normally positioned on the base of the jaw.
My classification of macroglossia is the following (M. Mommaerts 1987):
Idiopathic Macroglossia. This condition is rather rare. It causes protrusion mainly of the lower front teeth, producing interdental spaces, but can also shift the bicuspids and even the molars laterally, producing a circular cross bite. The tongue looks large, is rather voluminous, but only slightly rounded on the dorsum.
Macroglossia as a Sign of Acromegaly. Its reduction in size is as equally important before the correction of an acromegalic antemandibulism as is the removal of the causative pituitary gland adenoma. The tongue looks really voluminous.
Macroglossia in Cases of Down's Syndrome and Debility. In these cases the tongue has a rather typical form. It does not seem large or flat as in the genuine macroglos-
sia case. This tongue looks roundish with a rather high dorsum. Its consistency is harder than that in the two types just mentioned above. It can cause speaking problems and produce an open bite.
Functional Macroglossia. In the resting position nothing seems to be wrong with the tongue, but it presses with abnormal force against the teeth. The patient is often called a "tongue thruster".
Tumorous Macroglossia. The enlargement is due to a tumour or tumour-like condition within its musculature. Any kind of tumour in the tongue can produce such a macroglossia, a pure haemangioma or lymphoma and mostly a lympho-haemangioma, a neuroma, a fibroma or neurofibromatosis as in cases of von Recklinghausen's disease, etc.
Pseudo-macroglossia. This is that type of large, flat, flabby tongue which is often found within the large oral cavity in a case of macromandibulism or antemandibulism. It has no influence on the teeth or the position of the jaw. It has filled the space provided by the large jaw. The tongue does not need to be reduced in size when the mandible is pushed back and the oral cavity is reduced in size. It adapts to the new condition without any negative consequences.
24.3 Surgical Problems
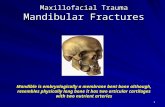
As macroglossia was a well-known problem, several surgeons had reported their procedure to reduce the tongue size (Fig. lOla). Some removed just an oval wedge from the dorsum of the tongue. H. Pichler ( 1948) excised an additional oval piece from the tip. A rather large triangular piece of the tip of the tongue was excised by U. Rheinwald (1957). His technique shortened the tongue but did not reduce its breadth. H. Kole (1970a) used a rather narrow excision in the tongue's midline and additionally a triangular excision of the tip. I myself have excised an oval piece from the tongue's midline area and in addition a triangular piece in the front of the tongue.
We have published the procedure used, the results and the consequences (Egyedi and Obwegeser 1964).
H. L. Obwegeser, Mandibular Growth Anomalies© Springer-Verlag Berlin Heidelberg 2001

434 CHAPTER 24 Tongue Reduction
profound lingual A. + V.
inff'rior longitudinal M.
Pichler lingual N.
submaxillary duct
a Obwegeser Kiile b mylohoid ~. gtmiohyoid M. genioglossus M. s.ublingual A.+ V.
Fig. 101 a-e. Tongue reduction. a Schematic illustration of the principal types of excision for tongue reduction. b Diagram of frontal section through the tongue with surrounding tissues in the molar region ( from Corning 1909). c Large tongue with the desired amount of excision marked w ith blue. d The size a nd shape of the tongue l'/2 years after its reduction. e The s ize and shape of the excised parts of the tongue shown in Fig. !Ole, d

Between 1957 and 1963 we performed tongue reduction on 21 cases, influenced by U. Rheinwald's (1957) philosophy on that subject. P. Egyedi has carried out the follow-up of our cases. He had also investigated cadaver tongues experimentally. We wanted to know why we had occasionally vascularization problems with the tips of the two halves of the reduced tongue. He found that this was most probably due to a sharp bend in the lingual artery towards our resection area.
When performing a tongue reduction, it is wise to remember its anatomy and in particular the location of the lingual artery in relation to the planned surgery (Fig. 101 b).
After we had experienced partial necrosis of the tip of one or the other half in some cases,we reduced the breadth of that oval excision (Fig. 101c) and avoided cutting vertically down to the base of the tongue. The above mentioned sharp bend of the lingual artery, found on angiography of cadaver tongues, was the cause of it by being in the surgical field.
This procedure can produce a very nicely shaped tongue if it is not overdone. That means that not more, but rather less than a third of the tongue's width should be excised and the excision should be such that a good movable tip of the tongue will result (Fig. 101d). Care must be taken not to go too deep with the knife to the bottom of the tongue in the oval excision in the tongue midline. That means the knife should not go vertically down, but should be directed towards the midline of the tongue's lower surface in order to avoid cutting the lingual artery at its kink. It is astonishing the amount of tongue tissue that can be excised without interfering with its function (Fig. 101e).
24.4 Results
We were able to do a follow up on 20 out of 21 cases of tongue reduction, 7 of them had had a tongue reduction prophylactically. One of them ended up with a partial relapse of his presurgically existing open bite. In six cases, we did a tongue reduction when we thought that arelapse of the correction of an antemandibulism seemed to be developing. In one of them an unilateral relapse increased, in spite of the tongue reduction. The histology of the resected condyle proved the existence of condylar hyperactivity. The other cases remained satisfactory. In seven cases, the tongue size was reduced at the request of the orthodontic department. Two of them, one with an antemandibulism, the other with an open bite, remained as they were, in spite of additional orthodontic treatment.
There are two additional interesting cases which I want to mention. We did a mandibular set back operation on a 20-year-old female, using the sagittal splitting procedure. The patient had 6 weeks intermaxillary fixation and did not return for 6 months after removal of
24.6 Complications 435
the wire splints. The occlusion was the same as when she had left. When checking her, we saw that her large tongue was protruding through the bilateral gaps where the second bicuspid and first molars were missing. The crown and bridge department supplied her with a fixed bridge on each side. When she was called in for a check up after 9 months, it was found that on both sides the bridges were pushed laterally, but there was no change in the front tooth situation.
In the second case, a 28-year-old lady, a lower alveolar protrusion was present but there was no antemandibulism. The protruded alveolar segment was surgically repositioned into correct angulation with the anterior base of that mandible and with the upper teeth. Two plates were used to fix the retropositioned alveolar segment in the new position. Within 6 months, the alveolus with its teeth was in its presurgical protruded position again. Now the patient's large tongue was reduced in size and then the lower anterior alveolus was again repositioned (seeM. Mommaerts 1987).
24.5 As I Always Did It (P. Egyedi and H. Obwegeser 1964)
Normally, with the patient under naso-tracheal intubation anaesthesia, the tongue is gently pulled out, holding it with a towel clip inserted in its tip. The amount of oval excision in the midline, beginning just in front of the papillae and ending just behind the tip of the tongue, is marked with ink. Depending on the tongue's size 30-40% of the whole tongue width may be excised. In addition a V-shaped excision is marked, beginning on either side of the tip extending back to about the middle of the tongue (see Fig. 101c). Care must be taken to make a nice tip. For cutting the covering mucosa of the tongue I have given up using the electro-knife as the edges invert much more than when an ordinary knife is used. The bleeding is carefully arrested by electro-coagulation or ligation (preferably the latter). Then the covering mucosa is slightly undermined, as it otherwise inverts towards the tongue musculature. Resorbable material is used for adapting the muscle wounds. These stitches should not go too far inferiorly in order to avoid ligating the lingual artery. For closing the mucosa at the back of the tongue I prefer to use Supramid, placing some stitches of the mattress type. For approximation of the wound edges of the delicate mucosa on the inferior surface of the tip of the tongue this Supramid is also used, but of a very fine gauge. We leave the stitches in for 12 days.
24.6 Complications
During surgery the main problem was severe bleeding from the lingual artery. Although the vessel retracts into

436 CHAPTER 24 Tongue Reduction
the musculature it was clipped and ligated, resulting in partial necrosis of the tip of that half of the tongue.
After surgery we have experienced such massive swelling of the tongue that the patient could not close his teeth. Whenever we tried to evacuate blood through the suture line we had no success. So it must have been a type of parenchymal bleeding rather than a haematoma. This also happened in spite of careful control of haemorrhage during surgery. Within a few days the tongue always returned to the reduced size. We never experienced any infection. There was an occasional partial wound dehiscence. There were, of course, unpleasant results in those cases in which we had a partial tip necrosis of one or even both sides. The tongue looked asymmetrical and was rather hard and too short. There were speech problems for some days or weeks and the patients could never properly clean their vestibular sulci. After we became less radical with our oval excision, the final results did not have these unpleasant consequences.
24.7 Consequences
Based on my and my coworkers' experience I recommend that one should be rather conservative with tongue reduction. There are cases in which it should be recommended to the patient. The surgeon should keep in mind that a short, tethered tip of the tongue is a real disadvan-
tage for the patient, in speaking, in cleaning the teeth and the vestibular sulci with the tongue, and socially.
True, functional and tumorous macroglossia have more power to displace the teeth or even the alveolus than pseudomacroglossia has. It is my opinion that the tongue itself can rarely be the cause of a skeletal relapse after a setback operation for the correction of antemandibulism. When we reduced the tongue of every antemandibulism case prophylactically before the setback operation, we soon learned that this was totally unnecessary. Even in cases of true macroglossia the relapse may not be a skeletal relapse but an occlusal relapse because it is only the alveolus with the contained teeth which is tilted by the pressure of the tongue. Even screws and plates cannot prevent the relapse of a corrected ante-alveolism in cases of macroglossia, unless the tongue is primarily reduced in size.
Summarizing my experience with the tongue and its reduction, I have to say that there is no question that the tongue can have an influence on the position of the teeth and the alveolus. When functional or true or tumorous macroglossia is proven, then a tongue reduction should be advocated. Whenever one is in any doubt as to whether or not the tongue is or may be the cause of an occlusal or skeletal disturbance, I suggest performing the treatment first, be it orthodontic or surgical, and wait and see. If there is a tendency to relapse, the tongue should be reduced in its width and length by an experienced surgeon.