Managing Opportunistic Infection - · PDF fileManaging Opportunistic Infection: Focus on...
28
Managing Opportunistic Infection: Focus on TB-HIV Rudi Wisaksana Departement of Internal Medicine Hasan Sadikin Hospital HIV Working Group, Padjadjaran University
Transcript of Managing Opportunistic Infection - · PDF fileManaging Opportunistic Infection: Focus on...
Managing Opportunistic Infection: Focus on TB-HIV
Rudi Wisaksana Departement of Internal Medicine
Hasan Sadikin Hospital HIV Working Group, Padjadjaran University
Getting To Zero
• Zero new infection – Sexual transmission reduced by half – Vertical transmission eliminated – IDU have access to preventive measures
• Zero AIDS-related death – Universal access to ART for PLHIV who eligible – TB related death reduced by half
• Zero discrimination – Countries with punitive laws reduced by half – HIV related travel restriction eliminated in half of countries – HIV-women specific need addressed in half of nations – Zero tolerance for gender-based violence

TB-HIV
• HIV and TB: strongly associated – HIV: 25% of deaths due to TB
– TB: 33% of deaths due to HIV
• Indonesia: – 3rd largest HIV cases in Asia
– 5th largest TB case in world
• Bandung: – HIV patients 30% treated for TB
– TB inpatients 10% HIV infected

Factors associated with mortality
Died during follow-up (n=124)
Still alive (n=1221)
Age 30 (26-34) 29 (26-32)
Male 72.6% 63.6%
History IDU 46.8% 47.9%
Oral candida at baseline
55.6% 31.6%
Haemoglobin at baseline
10.4 (9.1-12.1) 12.4 (10.8-14.0)
CD4 at baseline 15 (6-43) 85 (19-304)
Previous TB treatment
41.9% 24.7%
TB treatment during follow-up
28.2% 15.9%
Whaltman, 2012
TB
No TB

TB-HIV management

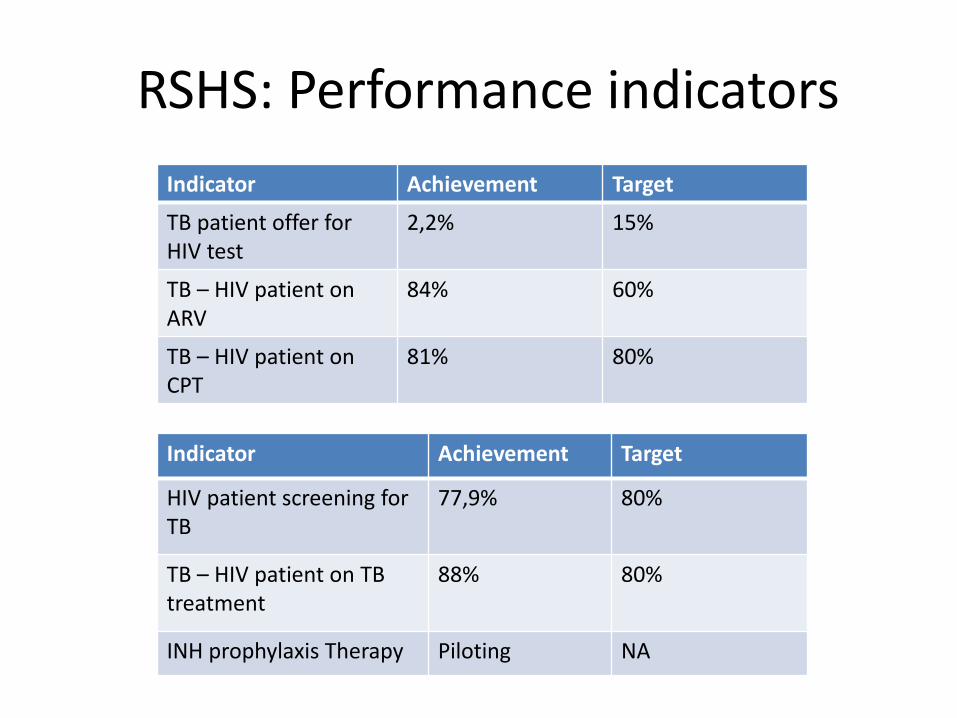
RSHS: Performance indicators
Indicator Achievement Target
TB patient offer for HIV test
2,2% 15%
TB – HIV patient on ARV
84% 60%
TB – HIV patient on CPT
81% 80%
Indicator Achievement Target
HIV patient screening for TB
77,9% 80%
TB – HIV patient on TB treatment
88% 80%
INH prophylaxis Therapy Piloting NA
HIV positif pada penderita TB ?
• WHO 2009: – Indonesia TB HIV: 2.8%
• Kohort TB di Bandung – ~1000 patients
– HIV + 1%
• RS Hasan Sadikin: 2008 – TB dirawat : 14%
– TB extraparu : 25%

HIV in Extra Pulmonary TB
Early Death in TBM Patients
0 10 20 300
50
100HIV-positive
HIV-negative
days
Perc
en
t su
rviv
al
Ganiem, 2009
Adult N=185
Male 60%
Median age 30 yo
HIV (+) 25%
Median CD4 13 cells/ml

200
Typical Tuberculosis
Atypical PTB
EPTB
Diagnosis TB ?
50
500
HIV awal
HIV lanjut
CD4

Diagnosing TB
• Common Procedure
– Sputum microscopy
– Chest radiography if sputum negative
– Culture
• Con’s
– Time consuming
– Multiple journey
– Insensitive

TB diagnosis affected by CD4
Whaltman, 2012

Microscopic Observed Drug Sensitivity (MODS)
Positivity of Ziehl
Neelsen
23% (39/167)
Positivity of MODS
34% (56/167)
Positivity of Ogawa
31% (51/167)
Days
Perc
en
t o
f p
osit
ivit
y
0 20 40 600
20
40
60
80
100OGAWA
MODS
MODS VS OGAWA
Chaidir, 2011
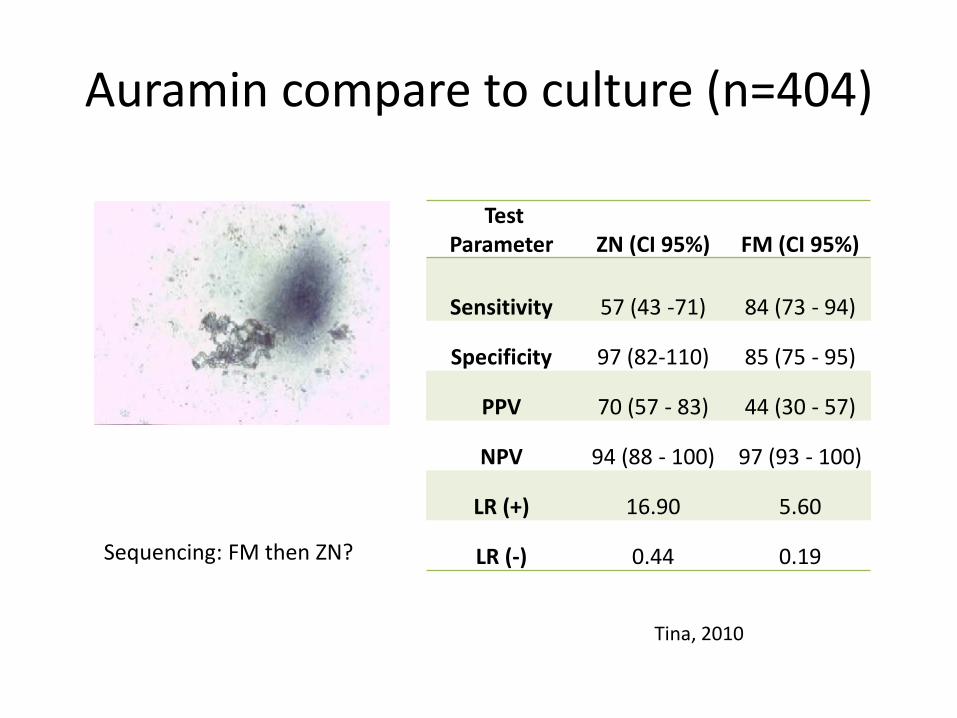
Auramin compare to culture (n=404)
Test Parameter ZN (CI 95%) FM (CI 95%)
Sensitivity 57 (43 -71) 84 (73 - 94)
Specificity 97 (82-110) 85 (75 - 95)
PPV 70 (57 - 83) 44 (30 - 57)
NPV 94 (88 - 100) 97 (93 - 100)
LR (+) 16.90 5.60
LR (-) 0.44 0.19 Sequencing: FM then ZN?
Tina, 2010

0
10
20
30
40
50
60
70
80
90
TW3 TW4 TW1 TW2 TW3 TW4
Number of new HIV pts
Number of TB suspects
Number of sputum examination
Number of smear pos
Number of HIV pts with TBtreatment
Source: TB Register in HIV clinic - 2012
2011 2012
X-pert
Xpert MTB/RIF assay for diagnosis TB
LAM
• Urine lipoarabinomannan (LAM)
• Cell wall components of MTB
• Cost $3.50/strip in 30 minutes
• Sensitifity: 95%
• More sensitive in CD4
< 50 cells/ml

Pengobatan TB-HIV

TB Treatment
• Generally same as non HIV
• Duration:
– 6 months for majority
– 9 – 12 months for patients with delayed responses, cavitary, EPTB, CNS TB
• Intermittent dosing in continuation phase
– Preferable to complete treatment
– Twice weekly : higher risk of relaps

Starting ART in TB
• Clinical and survival benefit of starting ART within the first 2 weeks treatment for an acute OI, excluding TB (Zolopa A, et al. ACTG A5164)
• Initiating ART 2 weeks after the start of tuberculosis treatment significantly improved survival (Camelia, Sapit, Stride) Except for meningitis TB (Torok ME, et al)

TB IRIS
• Diagnosis of HIV and TB – WHO criteria • Response to TB treatment – improved/stabilised • On ART
– Response documented by >1 log decrease in HIV RNA, though seldom available
• Onset within 3 months (up to 6) of starting/changing ART • Exclusion of alternative explanation
TB treatment failure due to drug resistance Another opportunistic infection or neoplasm Drug toxicity or reaction Complete non-adherence to ART
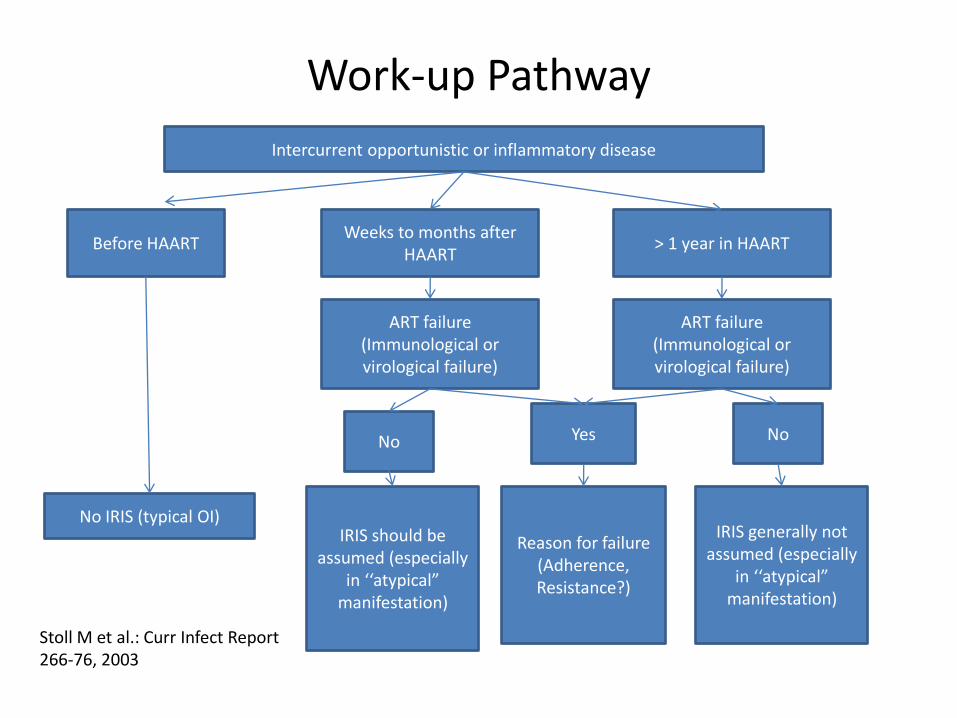
Work-up Pathway
Intercurrent opportunistic or inflammatory disease
Before HAART Weeks to months after
HAART > 1 year in HAART
ART failure (Immunological or virological failure)
ART failure (Immunological or virological failure)
Yes No No
No IRIS (typical OI) IRIS should be
assumed (especially in ‘‘atypical”
manifestation)
IRIS generally not assumed (especially
in ‘‘atypical” manifestation)
Reason for failure (Adherence, Resistance?)
Stoll M et al.: Curr Infect Report 266-76, 2003

TB-HIV patients
registered in HIV clinic
56 TB-HIV 25
TB-HIV patients
registered in
DOTS clinic
7
Need Good TB-HIV Collaboration
RSHS TB register 2012

Isoniazide Prophylactic Therapy (IPT)
• Dianjurkan WHO
– Reduksi risiko TB: 33-64%
– Terutama untuk TST (+)
• OAT: INH, Rif,
• Durasi: ? 6 – 36 bulan, tergantung tingkat transmisi TB
• Hambatan:
– Kesulitan menyingkirkan TB aktif pada CD4 rendah

ARV as TB prevention
• ARV strongly associated with reduce TB incidence
• Combined ARV and IPT superior than ARV or IPT alone
Suthar, 2012

Pelaksanaan IPT di RSHS
HIV (+)
Belum ARV
TB aktif No TB aktif
IPT
Terapi TB* (OAT)
Terapi TB* (OAT)
Sudah ARV > 3 bln
No TB aktif TB aktif
Belum indikasi ARV
Indikasi ARV
Skrining TB * Skrining TB *
Selesai terapi TB Selesai terapi TB
Teratai, 2012

TB latent: TST vs IGRA
Tuberculin Skin Test
IGRA (+) IGRA (-)
>10 mm 16 7
< 10 mm 8 48
> 5 mm 18 8
< 5 mm 6 47
IGRA:Overall prevalence: 25.5%
Meijerink, 2012-13

Conclusion
• TBHIV collaboration is essential
• Early Finding
• Diagnosis:
– Difficult, need new tools
• Treatment:
– TB treatment same as non HIV
– ART: 2 weeks after TB treatment
• Prevention: IPT and early ART