Managing Migraine: Primary Care for Primary Headaches · 10/28/2019 1 Managing Migraine: Primary...
20
Managing Migraine: Primary Care for Primary Headaches Jeffrey Unger, MD Disclosures: Speakers Bureau: Novo Nordisk, Abbott Diabetes, Janssen Consultant: Novo Nordisk, Abbott Diabetes, Bayer Research Grants: Novo Nordisk, GSK, Abbott Diabetes, Merck, Sanofi, Lilly, Pfizer Stock Ownership: Novo Nordisk, Tandem Diabetes
Transcript of Managing Migraine: Primary Care for Primary Headaches · 10/28/2019 1 Managing Migraine: Primary...

Managing Migraine: Primary Care for Primary Headaches
Jeffrey Unger, MD
Disclosures: Speakers Bureau: Novo Nordisk, Abbott Diabetes, Janssen Consultant: Novo Nordisk, Abbott Diabetes, Bayer Research Grants: Novo Nordisk, GSK, Abbott Diabetes, Merck, Sanofi, Lilly, Pfizer Stock Ownership: Novo Nordisk, Tandem Diabetes

10/28/2019
1
Managing Migraine: Primary Care for Primary Headaches
Jeff Unger, MD, FAAFP, FACE
Director, Unger Primary Care Concierge Medical Group
Rancho Cucamonga, CA.
Assistant Professor of Family Medicine, UC Riverside School of Medicine
Disclosures
2
Jeff Unger, MD, FAAFP, FACE serves as a speaker for Amgen Pharmaceuticals and a
consultant for Teva Pharmaceuticals
Learning Objectives 1. Utilize evidence-based strategies to diagnose patients presenting with headache;
2. Identify associated conditions (e.g. depression), and red flags for potentially life
threatening causes of headache;
3. Use evidence-based recommendations to prescribe treatment for patients presenting
with acute or emergent headache pain;
4. Develop collaborate management plans, emphasizing patient education on avoiding
triggers that cause headache, and adherence to prescribed treatment strategies;
5. Discuss newer pharmacologic targets for managing patients with Chronic Migraine.
3

10/28/2019
2
Prevalence of Headache in the General Population
Prevalence of any form of headache was 93% in men and 99% in women.
Among men, 8% had, at some point, experienced migraine compared with 25% of women.
Migraine is the 2nd most disabling disease state in the world (low back pain is most disabling).
Rasmussen BK. Epidemiology of headache in a general population- a prevalence study. JClinEpidemiol. 1991: 44 (11):1147-57
U
Primary vs Secondary Headaches
PRIMARY SECONDARY
NO structural or metabolic
abnormality
Structural or metabolic abnormality
Tension type
Migraine
Cluster
Other primary headaches
Extracranial (sinusitis, otitis media,
glaucoma, TMJ)
Intracranial (SAH, vasculitis, dissection,
central vein thrombosis, tumor, abscess,
meningitis
Metabolic (CO2 retention, CO poisoning)
5
Headache Time Course
Minutes Days Weeks/Months Months/Years
Vascular
Infectious
Inflammatory/Neoplastic
Primary
Headaches
Secondary Headaches
6

10/28/2019
3
Diagnostic Red Flags and Comfort Signs Red Flags:
◦ First or worst
◦ Abrupt onset
◦ Fundamental change in pattern
◦ New headache onset in patients < 5 or > 50 years of age
◦ Cancer, HIV, pregnancy
◦ Neurological dysfunction + headache
◦ HA onset with seizure or syncope
◦ HA onset with exertion, sex or Valsalva
◦ Abnormal vital signs
◦ In children, HA get progressively worse over time
Comfort signs:
◦ Stable pattern x 6 months
◦ Long history of same headaches
◦ In children-recurring, INTERMITTENT
◦ Normal neurologic exam
◦ Occur with menstruation
◦ +FH of same
◦ Known consistent triggers
Ravishankar K. Which headaches to investigate. When and How.
Headache. 2016 Nov;56(10):1685-1697 7
Definition of Migraine A stable pattern of recurrent disabling headaches without
evidence of underlying cause.
Migraineurs have a genetic sensitivity towards severe, disabling
headaches.
Migraineurs are born with a very sensitive nervous system
The goal of migraine management is to allow the migraineur to
learn to reduce their neurological sensitivity
Migraine events disrupt normal neurologic brain function which
increases the likelihood of having additional events
Unger J. Migraine prophylaxis. The Pain Practitioner. 17 (1). 32-36. 2007 8
Migraineurs are Born with a Genetically Predisposed Sensitive Neurological System
Triggers:
Stress
Hormonal changes
Skipping meals
Specific food (cheap red wine, caffeine)
Sleep disruptions
Medications and med overuse
Weather
Minor head trauma
Protective factors:
◦ Standardized sleep patterns
◦ Regular meals
◦ Exercise
◦ Stress management
◦ Pro-active treatment for menstrual
migraine and prodromes
◦ Post menopause treatment
◦ Avoidance of triggers
◦ Reduction caffeine usage
9

10/28/2019
4
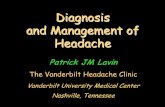
Adapted from Cady RK. Headache. 2008;48(9):1415-1416.
Prodrome Aura 20 %
Mild Moderate to Severe
Postdrome
“Most Bothersome Symptoms”
Mig
rain
e In
ten
sity
Phases of a Migraine Attack (3-5 days Duration)
Migraine symptoms occurring hours/days
prior to headache
Migraine when headache is mild
Migraine when headache is moderate to severe
Migraine symptoms occurring
hours/days after headache resolution
Focal neurological symptoms preceding headache (<1 hour)
Symptoms : • Food cravings • Mood changes • Yawning • Fatigue
Symptoms: • Tiredness • Confusion •Dizzy • Lowered appetite • Stiff or sore muscles
Symptoms: • Same as mild but more intense •Can develop allodynia within 2-4 hours
Symptoms: • Flashing lights or wavy lines • Numbness • Tingling in face • Disturbed senses
Symptoms: • Sensitivity to light • Sensitivity to sound • Nausea • Pain in the back of the head and neck •Loss of cognition
Pre-HA Post-HA Headache
10
Nausea
Vertigo
Vomiting
Confusion
Light and sound sensitivity
Prodrome: Symptoms Irritability - 48 %
Nausea - 43 %
Muscle pain/tenderness - 38 %
Change in energy level - 30 %
Change in mood - 24 %
Change in appetite - 21 %
Yawning - 21 %
Luciani R, et al. Cephalgia 2000; 20:122-126 11
Migraine: Spreading Cortical Depression and Aura
12

10/28/2019
5
Patient Describing Aura
13
Neck Pain During Migraine Prevalence
- 75% of subjects
Descriptions
- 69% - tightness
- 17% - stiffness
- 5% - throbbing
- 5% - other
Kaniecki R. Neurology. 2002;58(Suppl 6):S15-S20.
82% had previously been given a diagnosis of tension-type headache
14
“Even My Hair Hurts” (allodynia)
Cutaneous allodynia ◦ “Hair hurts”
◦Painful when:
- Shaving
- Combing hair
- Touching scalp
- Resting head on pillow
- Pulling hair back (wearing a ponytail)
- Wearing eyeglasses or contact lenses
- Wearing hat or head band
Chen N, et al. Pain Med. 2015 Jun;16(6):1211-20 15

10/28/2019
6
Migraine Pathogenesis Genetic predisposition
Triggers evoke aberrant firing of neurons resulting in
cortical spreading depression (CSD)
CSD activates the release of neurokinins and CGRP
causing vascular dilation and increased platelet
adhesiveness.
Neuronal flow into the nucleus caudalis can eventually
cause nausea, vomiting, dizziness, and severe head pain
Hadjikhani N, Sanchez Del Rio M, Wu O, et al. Mechanisms of migraine aura revealed by
functional MRI in human visual cortex. Proc Natl Acad Sci USA. 2001;98(8):4687-4692
Video courtesy of American Headache Society. With Permission. 16
“PIN” The Migraine Diagnosis | History
2/3 YES = Migraine
Lipton RB, et al. Neurology. 2003;61:375-382.
During the last 3 months, did you have the following with your headaches?
(YES/NO)
P Photophobia
Light bothered you (a lot more than when you don’t have
headaches)
I Impairment
Your headaches limited your ability to work, study, or do
what you need to do
N Nausea
You felt nauseated or sick to your stomach
Episodic Migraine vs Chronic Migraine
Frequency
Severi
ty
Frequent Episodic Migraine
< 15 Headache Days/Month
Headache
Time to Recover
Lipton RB, et al. Managing migraine: A healthcare professional’s guide to collaborative migraine
care. Hamilton, Ontario: Baxter Publishing Inc; 2008:26. 18
Chronic Migraine: > 15 headache days per
month x 3 months with 8 days being
migraine-like headaches
Brain sensitivity is heightened. No time for
neurological recovery between attacks Brain can recover between attacks

10/28/2019
7
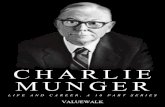
Free Iron Deposition in the PAG In a Patient With CDH
Control Chronic Daily Headache
Welch, et al. Periaqueductal Gray Matter Dysfunction in Migraine: Cause or the Burden of Illness? Headache. 41(7) P 629-637. 2001 With Permission
19
Barriers and Pitfalls in Primary Headache Diagnosis
Headaches evaluated within Primary Care are rarely due to secondary causes
Remember, migraine is a neurologic event, not a pathologic process based
upon vasodilation and constriction
Be cautious of patient directed diagnoses: “Sinus, stress, or allergic
headaches”
Most patients will have tried OTC meds prior to seeking professional
consultation.
“Sinus headaches” and neck pain…think migraine
20
Physical Exam Vital signs!
Look for any focal neurological findings
Listen to the head!
Feel the scalp and neck muscles
21

10/28/2019
8
Listen to the Head!
22
Headache Lab Tests
CBC
ESR
T4, TSH, Thyroid Peroxidase Antibody
Unger Jeff, Cady Roger K, Farmer-Cady Kathleen. Migraine Headaches, Part 1:
Presentation and Diagnosis. The Female Patient. May 2003: Vol.28. 14-21 23
Heather History
Recurrent disabling headaches
Light Sensitivity
Nausea
Vomiting
+ Family History
Lasts 4 -72 hours
Unger J, Cady R, Farmer K. Migraine headaches, Part 1; The Female Patient. 2003. 8; 32-39.
24

10/28/2019
9
Imaging Patients With Migraine
Adapted from Frishberg BM, et al. www.aan.com.
Patients with migraine and normal neurologic exam Meta-analysis
99.82%
0.18% Significant
intracranial pathology
Primary
Secondary
DO NOT perform
neuroimaging studies in
patients with stable
headaches that meet
criteria for migraine (American Academy of Neurology)
One Nerve Pathway: Multiple Symptoms of Migraine
(V3)
26
Does Peter Have Sinus Headaches?
Unger J, Cady R, Farmer K. Migraine headaches, Part 1; The Female Patient. 2003. 8; 32-39.
-
27

10/28/2019
10
Diagnosis of Sinusitis is Based on the Presence of at Least 2 Major or 1 Major + > 2 Minor Symptoms
Purulent nasal discharge
Nasal congestion or obstruction
Facial congestion or fullness
Facial pain or pressure
Loss of taste or smell
Fever (acute sinusitis only)
Headache
Ear pain, pressure or fullness
Halitosis
Dental pain
Cough
Fever (for subacute or chronic sinusitis)
Fatigue
Major Symptoms Minor Symptoms
Chow AW et al. IDSA clinical practice guidelines for acute bacterial rhinosinusitis in children and adults. Clinical Infectious Disease. 2012:
http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-
Patient_Care/PDF_Library/IDSA%20Clinical%20Practice%20Guideline%20for%20Acute%20Bacterial%20Rhinosinusitis%20in%20Children%20and%20Adults.pdf 28
Nasal Endoscopy
No Headache
With a moderate to
severe “sinus” headache
1 hour after
treatment with
sumatriptan
6mg SC
Reference: Schreiber CP et al. Arch Intern Med. 2004;164:1769-1772.
Photos courtesy of Jeff Unger, MD
29
Strategies for Migraine Treatment
Lifestyle interventions Acute treatment
• To stop pain and prevent progression
Preemptive treatment
• To preempt a predictable headache with a time-limited trigger
Preventive treatment
• To decrease frequency
Rescue therapy
• When all else fails
Lipton RB, et al. Headache. 1998;38:87–96; Silberstein SD, et al. Cephalalgia. 1997;17:67-72. 30

10/28/2019
11
Behavioral Approaches to Migraine Treatment
Relaxation exercises No meal skips
Exercise Sleep hygiene
Stop smoking Have a written plan!
Stop analgesics > 2× weekly 2 cups java per day
31
Acute Migraine Treatment Goals
Acute medication
not needed >2
times/week
Relief of
associated
symptoms
Headache does not come back for 24 hours
Headache free in 2 hours
Back to full function
in 2 hours
Little to no side-
effects from
medication
32
Triptans
Sumatriptan
Oral: 25, 50, 100 mg
Nasal: 5, 20 mg
Auto-injector: 4 or 6 mg
Needle-free injector: 6 mg
Zolmitriptan
Oral: 2.5, 5 mg
ODT: 2.5, 5 mg
Nasal: 5 mg
Naratriptan
Oral: 1, 2.5 mg
Rizatriptan
Oral: 5, 10 mg
ODT: 5, 10 mg
Almotriptan
Oral: 6.25, 12.5 mg
Frovatriptan
Oral: 2.5 mg
Eletriptan
Oral: 20, 40 mg
Sumatriptan/ Naproxen
Oral: 85 mg/500 mg ODT, orally
disintegrating
tablet
Physicians' Desk Reference, 2016. 70th ed. Montvale, NJ: PDR Network, LLC; 2016. 33

10/28/2019
12
Triptan Practical Strategies
Treat early after migraine onset
Use highest dose formulation
Expect to be pain free and associated symptom free within 2hrs
Migraine diary
Frequency, intensity, duration
Nausea
- Ondansetron 4-8 mg
- SQ injection or nasal spray
34
Early Intervention: Triptan Efficacy vs. Pain Intensity
0%
20%
40%
60%
80%
Mild Moderate Severe
80%
58%
35%
Pain Intensity When HA Treated
2 Hour Pain Free Response
Adopted from Cady RK et al SPECTRUM Study. Headache 2000 38:173-83 35
When To Consider Preventive Therapy
36
Migraine significantly interferes with patient’s daily routine, despite acute treatment
Attack frequency >1/wk
Acute medication ineffective, contraindicated, over-used, or not tolerated
Patient preference
Presence of uncommon migraine conditions

10/28/2019
13
Preventive Medications for Migraine
ß-blockers
Anticonvulsants
CGRP receptor mAb
CGRP ligand mAb
ACh release inhibitor (OnabotulinumtoxinA)
EPISODIC EPISODIC &
CHRONIC CHRONIC
Dodick DW. Lancet. 2018 Mar 31;391(10127):1315-1330. 37
Traditional vs New Preventive Treatments
TRADITIONAL NEW
Target Designed for other therapeutic areas Designed for primary migraine
prevention (EM, CM, MOH*)
Side Effects &
Tolerability Numerous side effects Minimal; similar to placebo
Time to Onset 2-4 months for effectiveness < 1 week – 1 month
Effectiveness ~ 50% reduction in HA frequency;
may lose effectiveness in MOH*
≥ 75% reduction in HA
frequency; lower all acute
medication use
*MOH: Medication overuse
(1) Stauffer VL, et al. JAMA Neurol. 2018 Sep 1;75(9):1080-1088. (2) Bigal ME, et al. Lancet Neurol. 2015 Nov;14(11):1081-90.
(3) Schwedt T, et al. J Headache Pain. 2018 Oct 1;19(1):92 (4) Dodick DW, et al. Lancet Neurol. 2014 Nov;13(11):1100-1107. 38
American Academy Neurology American Headache Society Preventive Recommendations
Divalproex Sodium
Sodium valproate
Topiramate
Metoprolol
Propranolol
Timolol
Frovatriptan(*)
Level A Level B
Amitriptyline
Venlafaxine
Atenolol
Nadolol
Naratriptan (*)
Zolmitriptan(*)
*= menstrual migraine
39

10/28/2019
14
Basic Rules For Traditional Preventive Medications
TREATMENT LENGTH 2–3 months to determine efficacy
6-months may be necessary for maximal response
TARGET GOALS in frequency, severity, and/or duration of acute attacks
Dodick DW. Lancet. 2018 Mar 31;391(10127):1315-1330.
FAMILY PLANNING Potential adverse fetal effects of antimigraine medications
Herbal Preventives Butterbur (Petadolex) 75 mg twice a day1
B2 (Riboflavin) 400 mg a day*
Magnesium 250-400 mg a day*
Feverfew 3 dried leaves daily*
Coenzyme Q-10 150-300 mg a day
Matchar DB, et al. AAN. US Headache Consortium. 2000:1-58. Level A evidence.
Levin M. Headache 2012;52;S2:76-80.
Markley H. Headache 2012;52:S2:81-87.
*= Effective for pediatric migraine
41
CGRP (Calcitonin-gene related peptide) and Migraine CGRP is released from various locations in the body during times of physiologic or emotional stress
CGRP sensitizes trigeminal afferents recruiting other nerves which can potentiate migraine
As more nerves become sensitized, the thalamus becomes activated and patient develops central
sensitization
CGRP levels sampled from the external jugular vein are increased during migraine compared with controls
who do not have migraine
CGRP infusions can trigger migraine in migraineuers, but NOT healthy controls.
CGRP inhibitors block migraine progression and reduce frequency, intensity and duration of migraine
CRRP inhibition allows brain to recover more fully from a migraine event
A brain which has not fully recovered from a migraine event is more reactive. Another migraine will follow
Frequent migraine, result in more frequent events
Juhasz G, et al. NO-induced migraine attack: strong increase in plasma calcitonin gene- related peptide
(CGRP) concentration and negative correlation with platelet serotonin release. Pain. 2003;106:461–47 42

10/28/2019
15
CGRP and Migraine Trigeminal Nerve activation Migraine trigger
Pain!
43
CGRP Inhibitor Prevents Migraine
Trigeminal Nerve activation Migraine trigger
CGRP Monoclonal Antibodies Prevent Receptor Activation
Trigeminal Nerve activation

10/28/2019
16
CGRP Inhibitors PHARMACOLOGIC TARGET INDICATION
Galcanezumab
(Emgality)
CGRP w/humanized
antibody
Episodic &
chronic migraine
Fremanezumab
(Ajovy)
CGRP w/humanized
antibody (CGRP ligand
binding)
Erenumab
(Aimovig)
CGRP receptor with
humanized antibody
Eptinezumab
(Not approved)
CGRP w/humanized
antibody
46
Cluster Headaches
CGRP Inhibitors | Efficacy
(1) Stauffer VL, et al. JAMA Neurol. 2018 Sep 1;75(9):1080-1088 (2) Skljarevski V, et al. Cephalalgia. 2018 Jul;38(8):1442-1454. (3)
Detke HC, et al. Neurology. 2018 Dec 11;91(24):e2211-e2221. (4) Dodick DW, et al. JAMA. 2018 May 15;319(19):1999-2008. (5)
Silberstein SD, et al. N Engl J Med. 2017 Nov 30;377(22):2113-2122. (6) Dodick DW, Cephalalgia. 2018 May;38(6):1026-1037. (7)
Ashina M, et al. Neurology Apr 2018, 90 (15 Supplement) S32.006. (8) Saper J, et al. Neurology Apr 2018, 90 (15 Supplement) S20.001.
(9) Silberstein S, et al. American Academy of Neurology meeting, Los Angeles, CA, April 25, 2018 (abstract P4‐471).
EPISODIC
MIGRAINE
CHRONIC
MIGRAINE
Galcanezumab 56-62%1-2 27%3
Fremanezumab 48%4 38-41%5
Erenumab 39%6 38-42%7
Eptinezumab
(Not approved) 49-56%8 57-61%9
% of patients with ≥ 50% reduction in the
average number of headache days/month
47
-7.5
-6.5
-5.5
-4.5
-3.5
-2.5
-1.5
-0.5 Placebo (n=281)
Erenumab 70 mg (n=188)
Erenumab 140 mg (n=187)
Specific Migraine Treatment With Anti-CGRP mAb: Effects of
Erenumab in Chronic Migraine
LS=LEAST SQUARES. SE=STANDARD ERROR.
TEPPER S, ET AL. LANCET NEUROL. 2017;16:425-434. 48
-2.7
-3.6
-4.2 -5.0
-6.2 -5.1
-6.5 -6.6 -6.6
Ch
an
ge
in M
on
thly
Mig
rain
e D
ays
Erenumab (Aimovig®)
Week 4 Baseline Week 8 Week 12

10/28/2019
17
†
†
*
†
†
† -6
-5
-4
-3
-2
-1
0
Placebo (n=281)
Galcanezumab 120 mg
Galcanezumab 240 mg
LS
Mea
n C
han
ge
Fro
m B
ase
lin
e (S
E)
-2.7
-4.6 -4.8 *P<0.01
†P<0.001
Month 1 Baseline Month 2 Month 3
Galcanezumab (Emgality®) REGAIN
Specific Migraine Treatment With Anti-CGRP mAb:
Effects of Galcanezumab in Chronic Migraine
DETKE HC, ET AL. NEUROLOGY. 2018;91(24):E2211-E2221. 49
Specific Migraine Treatment With Anti-CGRP mAb:
Effects of Fremanezumab in Chronic Migraine
CM=CHRONIC MIGRAINE.
SILBERSTEIN SD, ET AL. N ENG J MED. 2017;377:2113-2122. 50
-10
-9
-8
-7
-6
-5
-4
-3
-2
-1
0
Placebo (n=371)
Fremanezumab quarterly (N=375)
Fremanezumab monthly (N=375)
LS
Mea
n C
han
ge
Fro
m B
ase
lin
e in
Ave
rag
e
Nu
mb
er o
f H
ead
ach
e D
ays
per
Mo
nth
Baseline
-2.5
-4.6 -4.3
12 4 8
Week After First Injection
Fremanezumab (Ajovy®) HALO
† † †
†
†
†
Fremanezumab was equally effective in preventing EM and CM whether administered subcutaneously monthly or quarterly (primary endpoints)
Difference between fremanezumab quarterly and placebo during 12-week period: -1.8±0.3 days/month (P<0.001)
Difference between fremanezumab monthly and placebo during 12-week period: -2.1±0.3 days/month (P<0.001)
CGRP Inhibitors | Safety
(1) https://www.pi.amgen.com/~/media/amgen/repositorysites/pi-amgen-com/aimovig/aimovig_pi_hcp_english.ashx
(2) https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761089s000lbl.pdf
(3) https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761063s000lbl.pdf (4) Saper J, et al. Neurology Apr 2018, 90 (15 Supplement)
S20.001. (5) Silberstein S, et al. American Academy of Neurology meeting, Los Angeles, CA, April 25, 2018 (abstract P4‐471).
Erenumab1 Fremanezumab2 Galcanezumab3 Eptinezumab4-5
Systemic SEs No systemic effects (vs other biologics)
Injection site reactions
GI (constipation)
Respiratory (nasopharyngitis, URI)
Nausea, UTI,
arthralgia, dizziness,
anxiety, fatigue
51

10/28/2019
18
CGRP Inhibitors | Administration
52
MODE OF DELIVERY FREQUENCY
Galcanezumab
(Emgality)
Self-inject with autoinjector or
prefilled syringe Monthly
Fremanezumab
(Ajovy)
Self-inject with prefilled
syringe Monthly or every 3 months
Erenumab
(Aimovig) Self-inject with autoinjector Monthly
Eptinezumab
(Not approved) IV infusion Every 3 months
Menstrual Migraine Prevention Option
Frovatriptan 2.5 mg BID x 6 days beginning 2 days prior to onset of period
Frovatriptan 10 mg at onset of period
Frovatriptan 2.5 mg qd x 6 days beginning 2 days prior to onset of period
Tepper, SJ. Treatment of menstrual migraine: evidence-based review. Manag Care. 2007 Jul;16(7 Suppl 7):10-4; discussion 15-7.
Cady, RK, et al. Two center randomized pilot study of migraine prophylaxis comparing paradigms using pre-emptive frovatriptan or daily
topiramate: research and clinical implications. Headache. 2012; 52 (5) 749-764
53
Migraine Rescue Strategies Olanzepine 10 mg PO
Quetiapine 100 mg PO
Magnesium Sulfate 1 gram IV Push*
Occipital nerve block*
Sphenopaletine ganglion block*
- Use a “sphenocath”
- *= Office procedure by a family physician
Krusz JC. Aggressive Interventional Treatment of Intractable Headaches In The Clinic Setting.
In: Unger, J (ed). Clinics in Family Practice. Elsevier (Philadelphia). 545-567. Sept. 2005. 54

10/28/2019
19
IV Magnesium-Aborting Migraine Within 15 Seconds! NO KIDDING…
1 gram IV push over 1-2 minutes
Side effect: severe hot flash lasting < 1 minute
Eliminates migraine and migraine associated symptoms within 2-3 minutes
Works best for HA < 24 hour duration. For HA > 24 hour duration use depakon 500 mg IV push over 3-5 minutes
55
Summary Headaches evaluated within primary care are rarely due to secondary causes
Migraine diagnosed when there is presence of nausea, photophobia and/or disability
during headaches
- “Sinus headaches” and neck pain…think migraine
Avoid drugs that contain opioids and Butalbital as they cause MOH (American Academy
of Neurology)
Consider use of CGRP inhibitors for patients who have failed other preventative agents
56