Managing Anovulatory Infertility - The Medical...
43
Managing Anovulatory Infertility Patience, controversy, options, and surveillance Edward D. Tarnawa, M.D. Reproductive Endocrinology & Infertility THEGOS Annual Meeting, 2017
Transcript of Managing Anovulatory Infertility - The Medical...

Managing Anovulatory Infertility Patience, controversy, options, and surveillance
Edward D. Tarnawa, M.D. Reproductive Endocrinology & Infertility
THEGOS Annual Meeting, 2017

I have no conflicts of interest to disclose
Off-label use of drugs will be specified as such

PCOS
PolyCYSTic Ovarian Syndrome
I have one bias to make clear:
I don’t like the name …
Munch, The Scream, 1893
As Shakespeare said, “What’s in a name?”

PCOS What’s in a name??
P C O S
oly
ystic
varian
yndrome

PCOS What’s in a name??
P C O S
atience
ontroversy
ptions
urveillance
Compare and contrast treatment options for ovulation induction Review considerations for both pre- and post-treatment surveillance/monitoring Understand the risks and prognosis associated with ovulation induction Develop a strategy for approaching the challenging anovulatory infertility patient
Learning Objectives

Approaching the Patient
Explain, in simple terms, what PCOS is
Determine the goal
Make a plan for pretreatment evaluation
(and why it matters)
: Cycle control or pregnancy achievement
Educate - Plant the seed re: long-term implications
Educate - Plant the seed re: long-term implications

Pretreatment Evaluation
Rule-out uncommon causes of chronic anovulation Determine if additional endometrial evaluation is indicated Counsel regarding obesity Consider AMH testing Consider other causes of infertility

Pretreatment Evaluation Rule-out uncommon causes of chronic anovulation
Thyroid disease Hyperprolactinemia Nonclassic congenital adrenal hyperplasia Clinically significant androgen excess Chronic anovulation with estrogen absent
-Excess or deficiency -Serum TSH level suffices
-Standard ovulation induction approach would be ineffective -Serum prolactin level (and brain MRI if elevated)
-Not necessary for every patient -Early follicular phase 17-OH-progesterone (add a progesterone level if elevated)
-Primary indication for testing: Ruling-out androgen-secreting tumor -Key tests: Total testosterone and DHEA-S (no indication for free testosterone)
-History and exam will typically help to differentiate -Serum estradiol and gonadotropins
(i.e. hypogonadotropic hypogonadism)

Pretreatment Evaluation Determine if additional endometrial evaluation is indicated
Have a low threshold for EMB
Cheung AP, Green Journal, 2001 -56 consecutive women with PCOS underwent ultrasound and EMB
-20 (36%) had endometrial hyperplasia (25% of cases featured atypia)
-Both endometrial thickness and intermenstrual interval were significant predictors -Endometrial thickness >7mm
-Intermenstrual interval >3 months
Key Points -Understudied, but significance is unquestioned
-Incidence 30-50% in other studies
-Immediate and ongoing concern for these patients
-Predictive values of the above thresholds still far from ideal
-Provides some framework for decision-making

Pretreatment Evaluation Acknowledge the implications of obesity
November 2015
Weight loss improves success rates in those seeking pregnancy The impact of obesity on maternal/fetal obstetric morbidity is dose-dependent
What does ASRM say?
Obese women wishing to conceive should consider a weight management program that focuses on preconception weight loss
(to a BMI less than 35 kg/m2)

Does Pretreatment Weight Loss Improve Response to Ovulation Induction?
The OWL-PCOS Trial -149 women randomly assigned to pre-clomid OCP, lifestyle modification, or combo -BMI 27 - 42
-Lifestyle intervention: 16 weeks, caloric restriction + exercise + anti-obesity Rx
-Ovulation induction: Clomid (50 - 150mg) for up to 4 cycles
-Intercourse every 2-3 days (no OPKs, IUI, or sono monitoring)

The OWL-PCOS Trial
26%
24%
10%
How much weight did they lose? 6.5% of pre-intervention weight (goal 7%)
2-3 BMI units Legro et al, JCEM, 2016

What About Pretreatment Weight Loss vs. Immediate Treatment?
-Post hoc analysis comparing outcomes in the lifestyle group in previous study to those in a RCT which included a clomid arm (the PPCOS II trial) -N=142 for the former and 187 for the latter
-Intentionally identical treatment/monitoring protocols and enrollment criteria
-Age- and BMI-matched

What About Pretreatment Weight Loss vs. Immediate Treatment?
PPCOS II OWL - PCOS
Immediate Clomid
Weight Loss Prior to Clomid
Ovulation
Cumulative Ovulation Rate
44.7% 62%
Comparison to Immediate
Clomid
*** RR = 1.4 (95% CI: 1.1 – 1.7)
Live Birth
Cumulative Live Birth Rate
10.2% 25%
Comparison to Immediate Clomid
*** RR = 2.5 (95% CI: 1.3 – 4.7)
Legro, NEJM, 2007 Legro, JCEM, 2016

Pretreatment Evaluation Consider AMH testing
Rationale -Women with very high AMH levels more likely to be clomid resistant -Pretreatment measurement/detection may aid in counseling re: potential for success -May help to determine optimal starting dose of clomid
ROC Curve Analysis (AUC 0.87) -Cut-off of 3.4 ng/mL -Sensitivity 73% and specificity 78% in predicting anovulation
Mahran A, JCEM, 2013

Pretreatment Evaluation Consider other causes of infertility
Make sure to check a semen analysis -The incidence of a coexisting male factor is significant
-If normal, intrauterine insemination (IUI) is not indicated Consider HSG -Not necessary for everyone
-Indications:
-Age >35
-Other risk factors for tubal disease

Treatment Options
Metformin
Ovulation Induction With Oral Agents
Ovulation Induction With Gonadotropins
IVF

Standard Ovulation Induction (Clomid) Choosing the dose
-Responsiveness correlates with body weight (but predictive value is suboptimal) -In general, start at 50mg (1 tablet) for 5 days (50% of women will respond)
-Disclaimer: I tend to start at 100mg in obese patients
-Most providers will not exceed 150mg (and few require it)
-Some will be exquisitely responsive (doses of 12.5 or 25mg may be sufficient) Goal: Monofollicular Ovulation
Doses in excess of 100mg are not FDA approved
-Reviewing records (if available) is helpful
-Increase in 50mg increments until ovulation induction achieved
-Overall, response is consistent, but don’t be alarmed by intermittent anovulatory cycles

Standard Ovulation Induction (Clomid) Prognosis
-Approximately 80% of women will achieve regular ovulation
-Cumulative pregnancy rate 55-73%
Don’t be in a hurry to recommend more aggressive treatment
50mg 100mg 150mg 3 cycles 50% 45% 33% 6 cycles 62% 66% 38%
Cumulative Pregnancy Rates Imani B, JCEM, 84, 1999
ASRM: Therapy beyond 6 months is generally not recommended
Gonadotropin-based ovulation induction is risky
IVF is expensive and complex

Standard Ovulation Induction (Clomid) Side Effects and Risks
-Mood swings are the most common side effect (64-78%) -Vasomotor symptoms occur in only 10%
-Visual disturbances are rare (<2%) and transient: Consider alternative options -Blurred vision and diplopia
-Scotomata
-Light sensitivity
-Less specific: Breast tenderness, pelvic discomfort, nausea (2-5%)
By far, the most significant risk to discuss is multiple pregnancy
-Baseline risk of twins: 1% -Incidence of twins in pregnancies following clomid use: 8-10%
-Note: A good time to educate re: relative vs. absolute risk
-Higher-order: 0.08-1.1%
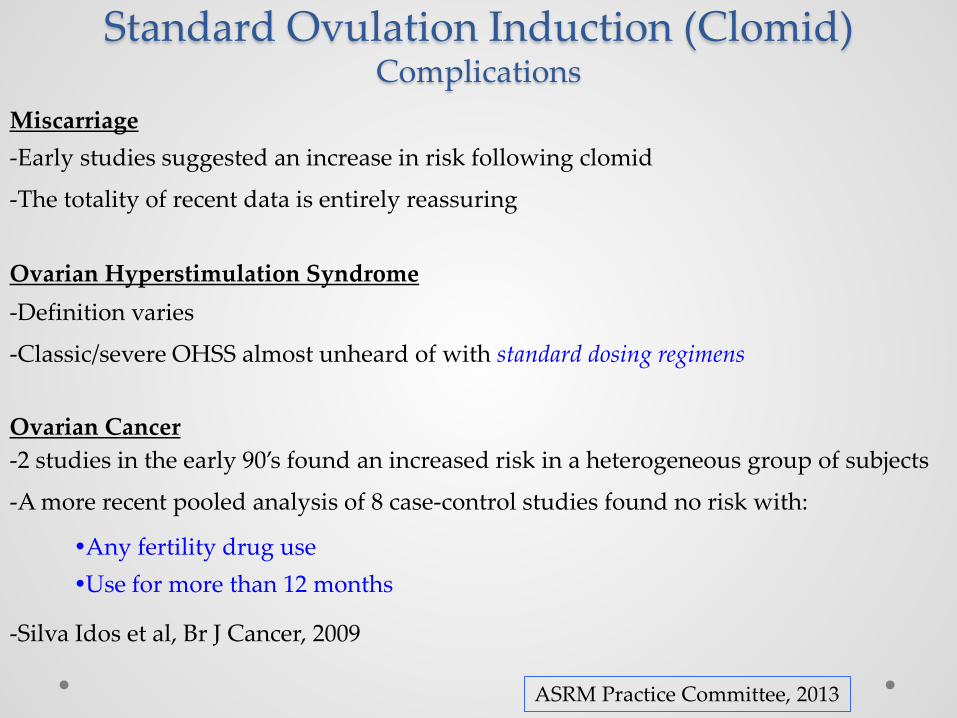
Standard Ovulation Induction (Clomid) Complications
Miscarriage
Ovarian Hyperstimulation Syndrome
Ovarian Cancer
Any fertility drug use Use for more than 12 months
-Silva Idos et al, Br J Cancer, 2009
ASRM Practice Committee, 2013
-Early studies suggested an increase in risk following clomid
-The totality of recent data is entirely reassuring
-Definition varies
-Classic/severe OHSS almost unheard of with standard dosing regimens
-2 studies in the early 90’s found an increased risk in a heterogeneous group of subjects
-A more recent pooled analysis of 8 case-control studies found no risk with:

Standard Ovulation Induction (Clomid) Practical Tips: Sonographic Monitoring
ASRM: Provides insight, but is costly, logistically demanding, and best reserved for those in whom less complicated methods fail to provide “the necessary information”
What is the necessary information?
-Is it OK to start? -Does she respond? -What is the pace of her cycle? -Are ovulation predictor kits (OPKs) providing reliable guidance? -Does she over-respond? -Does the dose need to be adjusted? -Is it time to cancel the cycle? Disclaimer: I like answers to all the above, and routinely utilize it -At least initially (I care about cost-efficiency, too) -If response is relatively predictable and OPKs are reliable, it may be tailored/limited -At a minimum: Baseline clearance and mid-follicular scan to rule-out over-response

Standard Ovulation Induction (Clomid) Practical Tips
Ovulation Predictor Kits -They can be used effectively in most women -False positivity may be a problem: Can be recognized early with a basal serum LH level
-BID use can be helpful when the pretest probability of a (+) result is greater
-Once positive: Daily IC x 2-3 days, or IUI the next day
hCG Trigger Injections
-Costly and simply not necessary for most patients -A meta-analysis (>1000 subjects) reported lower odds of pregnancy when utilized
-Best reserved for those in whom IUI is planned and OPKs are unreliable
-If using, pregnancy rates are highest when the leading follicle is >23mm in diameter
ASRM Practice Committee, 2013

More Tips Is IUI beneficial?
Starting a cycle or transitioning to a new one
-Not if partner’s SA is normal and the indication is anovulatory infertility -Unexplained infertility is a different scenario
-Reasonable to consider after 3-4 failed cycles, especially if IVF isn’t an option
-As before, hCG trigger isn’t an automatic indication in this setting
-Ovulation/pregnancy rates are similar regardless of day of cycle start (2, 3, 4, or 5) -May start at any time if at anovulatory baseline -Estradiol, progesterone, and hCG levels may be helpful -Pay attention to endometrial thickness
-Progestin withdrawal not always necessary -Live birth rate higher when a progestogen was NOT used -Diamond et al, Green Journal, 2012
My Practice: Start immediately if at anovulatory baseline and endometrium <8mm

Does Metformin Improve Outcomes When Combined with Clomiphene?
The PPCOS Trial
-626 women assigned to clomid (up to 150mg), metformin (ER, 1g BID), or combo -Intercourse every 2-3 days (no OPKs, IUI or sono monitoring)
-Treated for up to 6 cycles, or 30 weeks

The PPCOS Trial
26.8%
22.5%
7.2%
CC vs combination therapy: P=0.31 Metformin vs. both CC and combination: P<0.001
Legro et al, NEJM, 2007

Take-Home Points from PPCOS
Clomid significantly more likely to lead to live birth than metformin Addition of metformin did not increase the likelihood of achieving pregnancy with clomid -Equal fecundity per ovulated patient (~30%) -Equal fecundity per ovulated cycle (~10%) Incidence of clomid resistance: 25% (never ovulated during the study) Approxiately 75% of women taking clomid did not have a baby
Legro et al, NEJM, 2007
-Note: Mean BMI in all groups ~35 -Note: The protocol

Metformin Pretreatment for Obese Women? -Multicenter European RCT: 320 women -Randomized to 3 months of metformin (1000mg BID) pretreatment or placebo
-Followed by 4-6 cycles of clomid, if indicated
Morin-Papunen et al, JCEM, 2012

ADA Recommendations -PCOS is an additional risk factor that should prompt screening for T2DM in asymptomatic overweight (BMI ≥ 25) adults -Hemoglobin A1c is considered an appropriate screening test
Prediabetes: A1c 5.7 – 6.4% Diabetes: A1c ≥ 6.5%
-Consider metformin for T2DM risk reduction in those with prediabetes, especially if: -BMI ≥ 35
-Age < 60yo
-History of GDM
So …
-PCOS is not an automatic indication for metformin for T2DM risk reduction -PCOS is an indication for T2DM screening
-Metformin may be considered if A1c > 5.7% and BMI ≥ 35
ADA Standards of Medical Care in Diabetes - 2016

What About Letrozole?
-It (along with anastrozole) is a 3rd generation, reversible aromatase inhibitor -Potent: Reduces estrogen levels by ≥ 97%
-Half-life 45hr, cleared by the liver
Rationale
Mechanism of Action -Prevents estrogen’s exertion of negative feedback at the hypothalamus/pituitary
Augments FSH release
-Leads to temporary accumulation of intraovarian androgens
Augments follicular FSH-receptor expression
Stimulates IGF-I expression (augments FSH action)
-May have favorable endometrial effects
Blockade of estrogen synthesis leads to upregulation of estrogen-receptor expression
Favors robust endometrial development once estrogen secretion is restored
Casper and Mitwally, JCEM, 2006
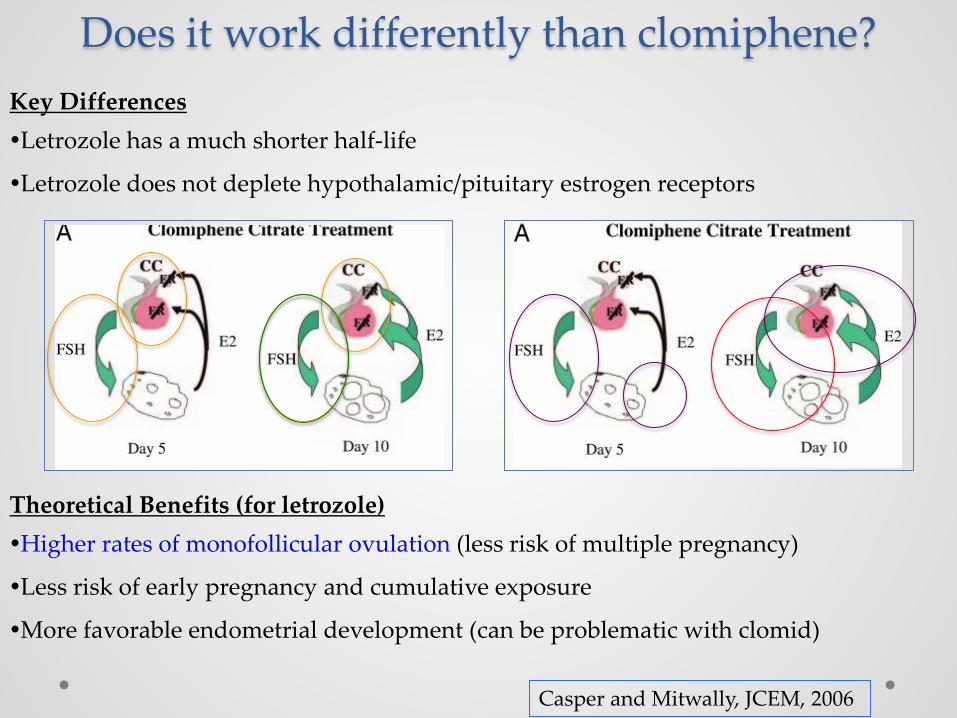
Does it work differently than clomiphene? Key Differences Letrozole has a much shorter half-life
Letrozole does not deplete hypothalamic/pituitary estrogen receptors
Theoretical Benefits (for letrozole) Higher rates of monofollicular ovulation (less risk of multiple pregnancy)
Less risk of early pregnancy and cumulative exposure
More favorable endometrial development (can be problematic with clomid)
Casper and Mitwally, JCEM, 2006

Is Letrozole Better than Clomiphene?
The PPCOS II Trial
-750 women assigned to clomid (up to 150mg) or letrozole (up to 7.5mg) [CD3 start] -Intercourse every 2-3 days (no OPKs, IUI, or sono monitoring)
-Treated for up to 5 cycles

PPCOS II Trial
Rate ratio for live birth (LTZ vs. CC) 1.44; 95% CI 1.10 - 1.87
27.5%
19.5%
Legro et al, NEJM, 2014

What About Letrozole?
More take-home points from PPCOS II -Ovulation rates per cycle superior to clomid
-Improved fecundity with letrozole per subject who ovulated
-Significantly more hot flashes with clomid (33% vs. 20% with letrozole)
Letrozole vs. Clomid: Meta-Analysis
-Franik et al, Cochrane Database, 2014 -9 RCTs
-n=1783
-Superior live birth rate with letrozole
-OR 1.63; 95% CI 1.31 – 2.03

Letrozole: Why the controversy?
Two Primary Reasons It is not FDA-approved for ovulation induction
Ill-informed concern re: risk of fetal anomalies
FDA-Approval: Safety + Efficacy Off-label use of drugs is common
I doubt that FDA-approval will ever be sought
We now have Level I evidence that letrozole is not only efficacious, but also likely superior to clomiphene
What about safety?

Letrozole: Safety Concerns? November 29, 2005
Manufacturer warned that letrozole should not be used for ovulation induction
[Letrozole] “should not be used in women who may become pregnant, during pregnancy and/or while breast-feeding, because there is a potential risk of harm to the mother and the fetus, including risk of fetal malformations”
Based on a single abstract presented at the 2005 ASRM annual meeting
Biljan MM et al, ASRM O-231 -Retrospective “cohort” study -150 births resulting from letrozole -Compared with 36,050 “mostly low risk babies” not born after maternal letrozole use Overall anomaly rate was not increased Significant increase in locomotor and cardiac anomalies in letrozole-related births
This work was never published The FDA never took any action

Letrozole: Safety Concerns? A Few Thought/Comments -The reaction to the abstract was much like the media response to the first WHI paper -Small number of exposed cased and wide confidence intervals -Can’t specifically comment, but unaddressed bias is highly likely
One that is certain: The unexposed group did not consist of infertile women The work did not survive peer review
A better (published) study (soon after controversy arose): -Tulandi et al, 2006 -911 live births from women who conceived following clomiphene or letrozole -Overall anomaly rate: Equal -Significantly fewer cardiac anomalies in the letrozole group
No difference in anomaly rates (CC vs. letrozole) in the two largest RCTs
No peer-reviewed data have ever demonstrated a higher anomaly rate after conception preceded by letrozole use
Just consider: Time of use and half-life

Approaching the Difficult Patient Not Getting Pregnant
Be patient, but expand evaluation/surveillance after 3 cycles
Complete the fertility evaluation (i.e. HSG and SA if not already performed)
Implement monitoring
-Impaired endometrial development in up to 30% of CC users
-Confirm that ovulation is being induced
No need to increase dose if ovulation is occurring
Consider IUI
Refer to REI if pregnancy not achieved after 4-6 ovulatory cycles

Approaching the Difficult Patient Clomiphene Resistance
Easy on the dose, beware progesterone levels, and implement monitoring Treatment Options -Extend treatment duration (7-8 days)
-Consider metformin pretreatment in obese patients
-Add dexamethasone (0.5-2mg beginning on day of CC start) -Use for up to 10 days -May be best in those with elevated DHEA-S levels -Promptly discontinue if not successful
-Switch to letrozole (will be successful in about half)
-Consider sequential therapy with gonadotropins -Begin low dose (37.5 – 75 IU daily) immediately following letrozole or clomid -Requires diligent monitoring -Be careful: The goal is monofollicular ovulation

Summary Develop a routine plan for pretreatment patient evaluation and counseling
Emphasize the long-term health implications of PCOS
Encourage weight loss prior to initiation of ovulation induction (minimum 5%)
Explain per-cycle and cumulative prognosis: Prepare to be patient
Metformin is best reserved for obese patients with prediabetes
While not, yet, endorsed as first-line therapy, letrozole appears superior to clomiphene
Be prepared to provide proper counseling and obtain consent if Rx letrozole
Refer if response (ovulation) is concerning, unclear, or after 4-6 cycles

Thank You

References 1. Cheung AP. Ultrasound and menstrual history in predicting endometrial hyperplasia in polycystic ovary
syndrome. Obstet Gynecol 2001; 98: 325-31 (PMID 11506853).
2. Practice Committee of the American Society of Reproductive Medicine. Obesity and reproduction. Fertil Steril 2015; 104: 1116-26 (PMID 26434804).
3. Legro RS et al. Randomized controlled trial of preconception interventions in infertile women with polycystic ovary syndrome. J Clin Endocrinol Metab 2015; 100: 4048-58 (PMID 26401593).
4. Legro RS et al. Benefit of delayed fertility therapy with preconception weight loss over immediate therapy in obese women with PCOS. J Clin Endocrinol Metab 2016; 101: 2658-66 (PMID 27172435).
5. Mahran A et al. The predictive value of circulating anti-Müllerian hormone in women with polycystic ovarian syndrome receiving clomiphene citrate: a prospective observational study. J Clin Endocrinol Metab 2013; 98: 4170-5 (PMID 23979947).
6. Imani B et al. Predictors of chances to conceive in ovulatory patients during clomiphene citrate induction of ovulation in normogonadotropic oligoamenorrheic infertility. J Clin Endocrinol Metab 1999; 84: 1617-22 (PMID 10323389).
7. Practice Committee of the American Society of Reproductive Medicine. Use of clomiphene citrate in infertile women. Fertil Steril 2013; 100: 341-8 (PMID 23809505).
8. Silva Idos S et al. Ovulation-stimulation drugs and cancer risks: a long-term follow-up of a British cohort. Br J Cancer 2009; 100: 1824-31 (PMID 19436296).

References 9. Diamond MP et al. Endometrial shedding effect on conception and live birth in women polycystic ovary
syndrome. Obstet Gynecol 2012; 119: 902-8 (PMID 22525900).
10. Legro RS et al. Clomiphene, metformin, or both for infertility in the polycystic ovary syndrome. N Engl J Med 2007; 356: 551-66 (PMID 17287476).
11. Morin-Papunen L et al. Metformin improves pregnancy and live-birth rates in women with polycystic ovary syndrome (PCOS): a multicenter, double-blind, placebo-controlled randomized trial. J Clin Endocrinol Metab 2012; 97: 1492-500 (PMID 22419702).
12. American Diabetes Association. Standards of Medical Care in Diabetes. Diabetes Care 2016; 39: S1-1.http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf
13. Casper RF and Mitwally MF. Review: aromatase inhibitors for ovulation induction. J Clin Endocrinol Metab 2006; 91: 760-71 (PMID 16384846).
14. Legro RS et al. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med 2014; 371: 119-29 (PMID 25006718).
15. Franik S et al. Aromatase inhibitors for subfertile women with polycystic ovary syndrome. Cochrane Database Syst Rev 2014; (2):CD010287. doi: 10.1002/14651858.CD010287 (PMID 24563180).
16. Biljan MM et al. The outcome of 150 babies following the treatment with letrozole or letrozole and gonadotropins. Fertil Steril 2005; 84 (Suppl 1): S95 (ASRM O-231).
17. Tulandi T et al. Congenital malformations among 911 newborns conceived after infertility treatment with letrozole or clomiphene citrate. Fertil Steril 2006; 85: 1761-5 (PMID 16650422).