Thyroid Nodule Diagnosis and Surgical Management of Solitary
Upload
prudence-weaverCategory
view
239download
1
Management of thyroid nodule
Introduction. Guidelines recommendation. Thyroid nodule work up. Genetic work up Medical therapy in thyroid nodule Thyroid nodule in children Thyroid nodule in pregnancy .
Introduction
It is a common clinical problem, ( 50% in adult) . Female : 5% & male : 1%. High-resolution ultrasound (US) can detect thyroid nodules in
19–67%. Thyroid Carcinoma occurs in 5-15% of any thyroid nodule (1). Well differentiated thyroid CA represent 90% of all thyroid CA.
(1) Hegedus L 2004 Clinical practice. The thyroid nodule. N Engl J Med 351:1764–1771.
Occult carcinoma in 6 – 35 % of glands at autopsy
(usu 4-10 mm)
– Biologic behavior difficult to predict 12,000 new thyroid cancers / year 1000 deaths / year Surgically removed nodules:
– 42-77 % colloid nodules
– 15-40 % adenomas
– 8-17 % carcinomas
Carcinoma ( subtypes)
Histological subtype Papillary 70% Follicular 15% Medullary 5-10% Anaplastic 5% Poorly differentiated 1% Lymphoma 5% Mets ( breast , lung ,GI , melanoma)
Radiation : as risk factor Appears to be dose-dependent :
– ERR 7.7 at 100 cGy
Maximum risk approximately 30 years later
Nodule in radiated patient: 35-40% cancer
Data suggest no more agggresive behavior over spontaneously-occuring cancers, but may be larger at presentation.
Only unequivocal environmental cause of thyroid cancer
Radiation : as risk factor
Younger age – greater risk
Suppression may help decrease risk:
– One study: 35.8% 8.4%
I-131: risk of leukemia with high doses
Thyroid nodule work up
What is the appropriate evaluation of clinically or incidentally
discovered thyroid nodule(s)? What laboratory tests and imaging modalities are
indicated? What is the role of fine-needle aspiration (FNA)? What is the role of medical therapy of patients with
benign thyroid nodules? How should thyroid nodules in children and pregnant
women be managed?
Strength of Panelists’ Recommendations
(A) : Strongly recommends. The recommendation is based
on good evidence that the service or intervention can improve important health outcomes.
(B) : The recommendation is based on fair evidence that the service or intervention can improve important health outcomes.
Eitology of thyroid nodule ( Others) :
Higher rate of nodules found in patients: Who have hyperparathyroidism Are undergoing hemodialysis
Strength of Panelists’ Recommendations
(C) : based on expert opinion.
(D) : Recommends against : based on expert opinion.
(E) : Recommends against : based on fair evidence that the service or intervention does not improve important health outcomes or that harms outweigh benefits.
(F) : Strongly recommends against: based on good evidence that the service or intervention does not improve important health outcomes or that harms outweigh benefits
Strength of Panelists’ Recommendations
(I) : Recommends neither for nor against:
If the evidence is lacking that the service or intervention improves important health outcomes, the evidence is of poor quality, or the evidence is conflicting. As a result, the balance of benefits and harms cannot be determined.
Thyroid nodule Discrete lesion within the
thyroid gland that is radiologically distinct from the surrounding thyroid parenchyma.
What is Incidentalomas?
Nonpalpable nodules detected on US or other anatomic imaging studies.
PET 1-2 % thyroid nodule
risk of malignancy is 33%
Thyroid nodule work up size as a factor
Thyroid nodule site as risk factor
Isthmus (carcinoma proven biopsy )LN Mets ( isthmus vs lobes) (83% vs. 66%).LN involvement on the both sides of the neck
(50%)
Thyroid nodule work up
Complete history & physical exam . Risk factors . Serum TSH US thyroid . Radionuclide Thyroid scan if TSH low normal or subnormal. If TSH high normal : increased risk of malignancy in a
thyroid nodule.
Boelaert K, Horacek J, Holder RL, Watkinson JC, Sheppard MC, Franklyn JA 2006 Serum thyrotropin concentration as a novel predictor of malignancy in thyroid nodules investigated by fine-needle aspiration. J Clin Endo Metab91:4295–4301.
History : Age Gender Exposure to Radiation Signs/symptoms of hyper- / hypo-
thyroidism Rapid change in size
– With pain may indicate hemorrhage into nodule
– Without pain may be bad sign
Gardner Syndrome (familial adenomatouspolyposis)– Association found with thyroid ca– Mostly in young women (94%) (RR 160)– Thyroid ca preceded dx of Garners 30% of time
Cowden Syndrome– Mucocutaneous hamartomas,keratoses,fibrocystic breast changes & GI polyps– Found to have association with thyroid ca (8/26patients in one series)
History
Familial h/o medullary thyroid carcinoma
– Familial MTC vs MEN II Family hx of other thyroid ca H/o Hashimoto’s thyroiditis (lymphoma
History
Elements suggestive of malignancy:Progressive enlargement HoarsenessDysphagiaDyspnea High-risk (fam hx, radiation)Cervical lymphadenopathy Fixation into adjsent structures Vocal cord paralysis PET (high uptake)
• Not very sensitive / specific
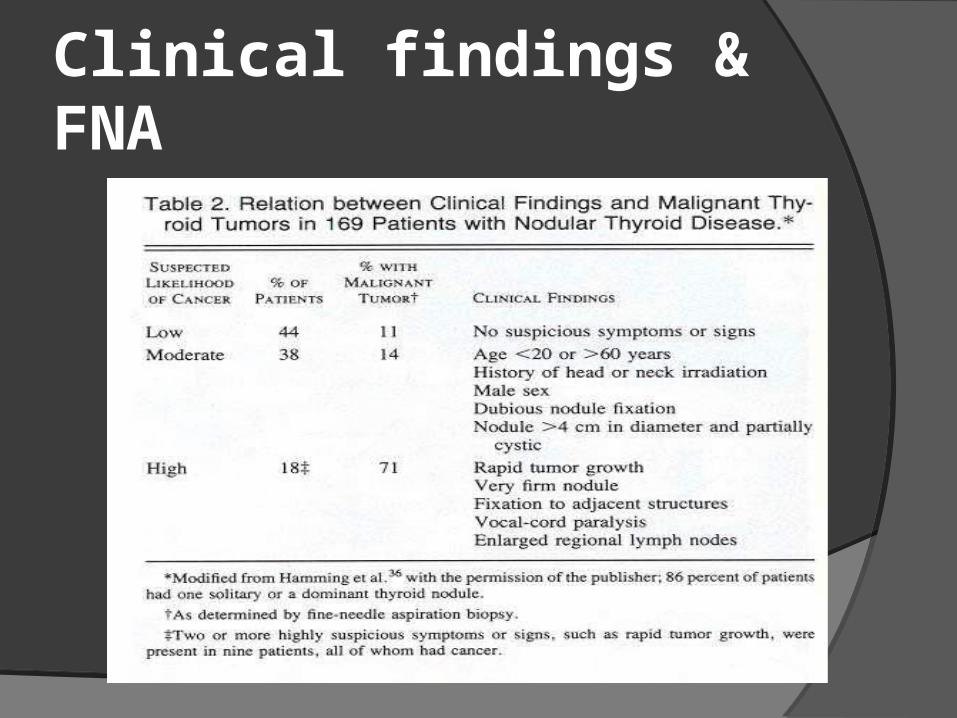
Clinical findings & FNA
Recommendation
Measure serum TSH . If subnormal, a radionuclide thyroid scan.( A)
US thyroid should be performed in all patients
with known or suspected thyroid nodules.(A)
Laboratories investigations: TSH – first-line serum test
– Identifies subclinical thyrotoxicosis T4, T3 Calcium ( MTC) Thyroglobulin (post cancer Rx surveillance) Calcitonin (MTC) Antibodies – Hashimoto’s RET proto-oncogene
Imaging
U/S CT vs MRI Radio nucleotide scan PET
U/S Neck ( Thyroid)
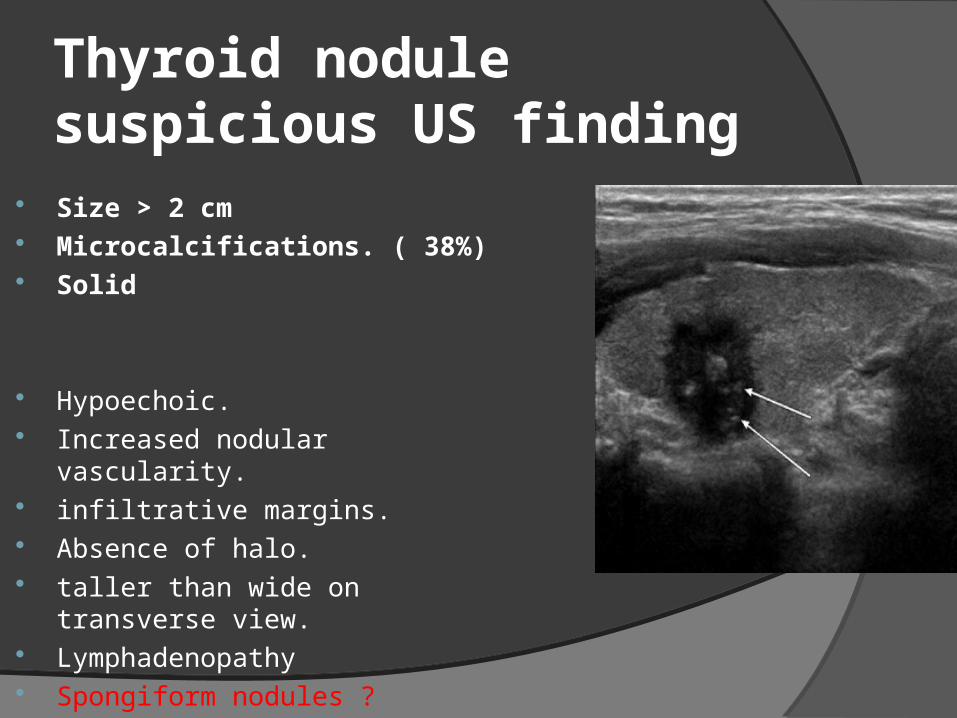
Thyroid nodulesuspicious US finding
Size > 2 cm Microcalcifications. ( 38%) Solid
Hypoechoic. Increased nodular vascularity. infiltrative margins. Absence of halo. taller than wide on transverse view. Lymphadenopathy Spongiform nodules ?
Malignant LN ( US finding) Round Hilum not visible Hypoechoic/heterogeneous Micro calcifications Irregular margins Multiple Invasion of surrounding tissues
Imaging :CT scan indications
Lymphadenopathy Revision cases ( selected)
CT/MRI
Retrosternal extension Soft tissue invasion ( trachea ,
esophagus ,vessels) ultrasound expertise is not available.
Radionuclide Thyroid scan:
Concept Uses
Metabolic studies Imaging
Iodine is taken up by gland and organified Technetium trapped but not organified Follicular cell only.
Radioisotope
I-131 I-123 I-125 Tc-99m Thallium-201 Gallium 67
Tc-99m
Most commonly used isotope (some authors) 99m: “m” refers to metastable nuclide
•Decay product of Molybdenum-99
•Long half-life before decaying into Tc-99 Administered as pertechnate (TcO4-) Images can be obtained quickly
• “One-Stop” evaluation Hot nodules need f/u Iodine scan Discordant nodules higher risk of malignancy
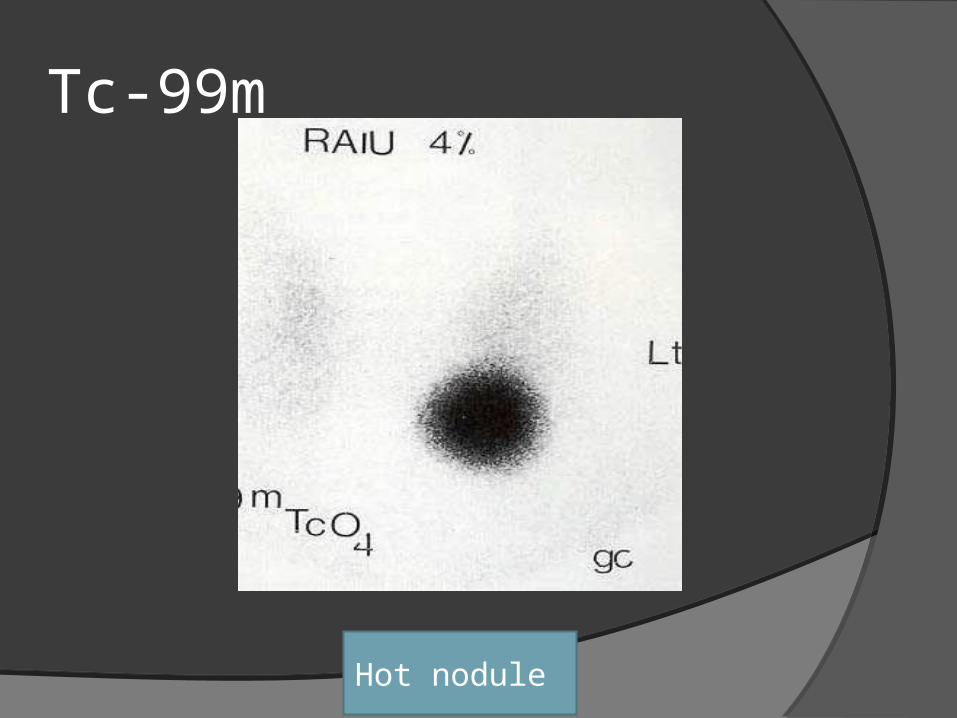
Tc-99m
Hot nodule
Iodine scan
127 – only stable isotope of iodine
123 – cyclotron product
• Half-life 13.3 hr
• Expensive, limited availability
• Low radiation-exposure to patient
Iodine scan 131 – fission product
• Half-life 8 days
• Cheap, widely available
• Better for mets (diagnostic and therapeutic) (high radiation exposure)
125 – no longer used
• Long half-life (60 days); high radiation exposure with poor visualization
Radionuclide Thyroid scan:99mTcO4 Thyroid Scintigraphy
FDG-PETMain indication
Post therapy surveillance ( localization) : Positive tumor markers (stim Tg> 10 ng /ml)
& Negative anatomical & functional imaging
FDG-PET relative indication Initial staging & follow up in poorly
differentiated thyroid CA. Disease specific mortality ( known cases
of distant metastasis ). Identification of patient with poor
response to RAI Rx . Post Rx response ( EBRT, surgery ,
chemotherapy or embolization)
Recommendation
FNA is the procedure of choice in the evaluation of thyroid nodules. (A)
US guidance FNA: .(B)o > 50% cystic, o Nonpalpable, o Located posteriorly in the
thyroid lobeo Initial FNA non diagnostic
FNA Biopsy
Technique:25-gauge needle Multiple passesIdeally from periphery of lesion Reaspirate after fluid drawnImmediately smeared and fixed Papanicolaou stain common
FNA Biopsy Hamberger study: addition of FNA
– Changed # pts undergoing surgery (67 43%)
– Carcinoma yield 14 - 29%
– Reduced cost per pt 25% Campbell & Pillsbury: pooled 10 studies
– All pts operated on regardless of FNA:
• False neg rate: 2.4%
• False pos rate: 1.2%
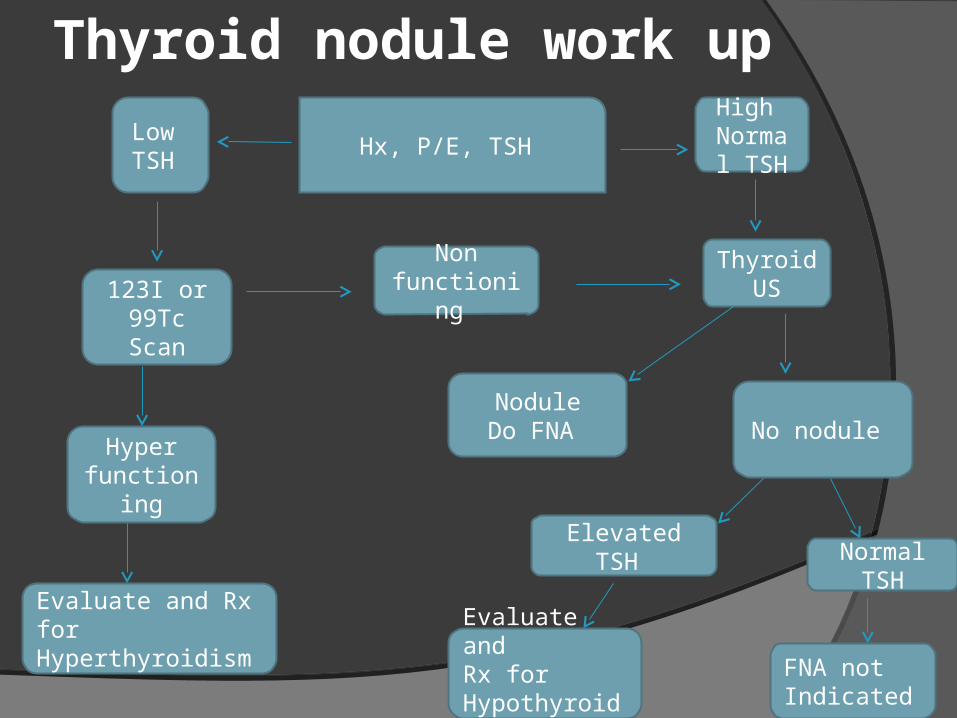
Thyroid nodule work up
Hx, P/E, TSH Low TSH
123I or 99Tc Scan
Hyperfunctioning
Evaluate and RxforHyperthyroidism
High Normal TSH
Thyroid US
Non functioning
NoduleDo FNA No nodule
Elevated TSH Normal TSH
Evaluate andRx forHypothyroidism
FNA notIndicated
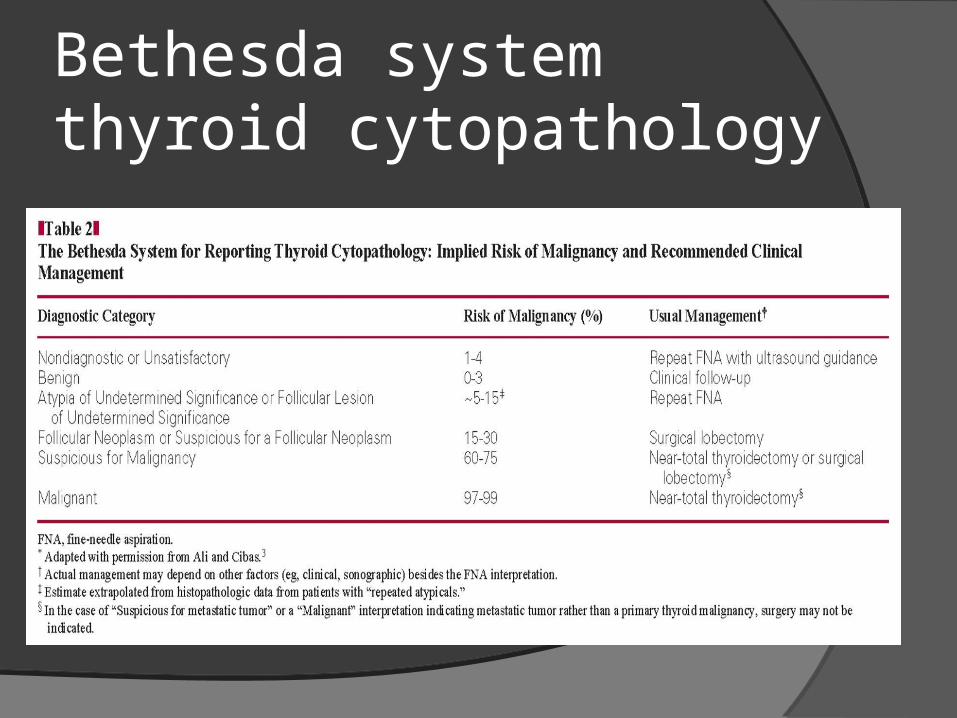
Bethesda systemthyroid cytopathology
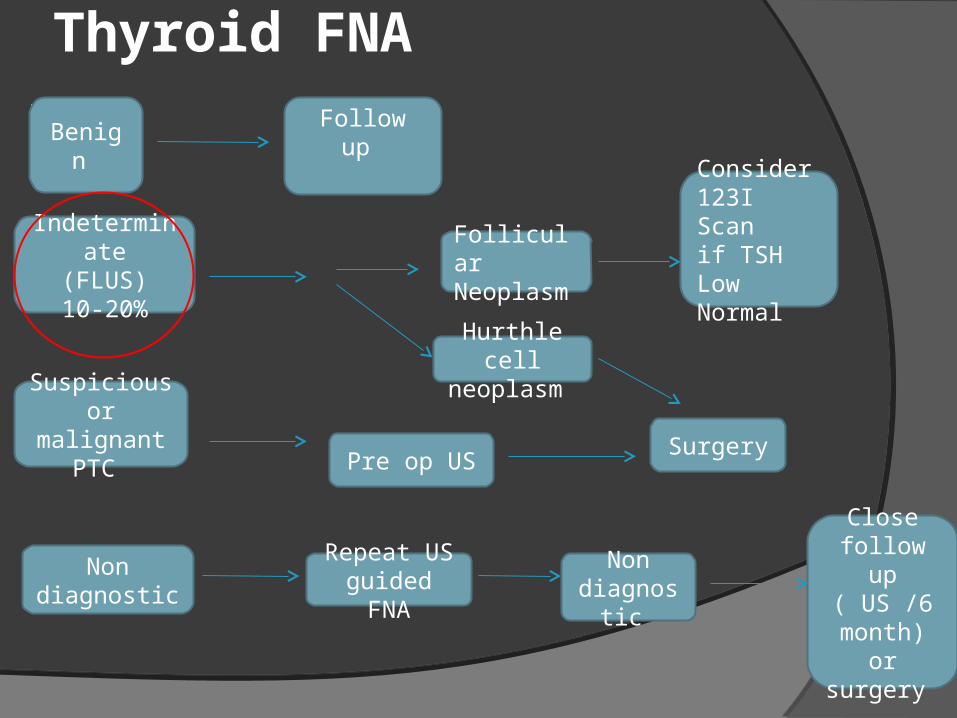
Thyroid FNA
beBenign
Follow up
Indeterminate(FLUS)10-20%
FollicularNeoplasm
Hurthle cell neoplasm
Consider 123I Scanif TSHLow Normal
Suspicious or malignant
PTC Pre op US Surgery
Non diagnostic
Repeat US guided FNA
Non diagnostic
Close follow up ( US /6
month) or surgery
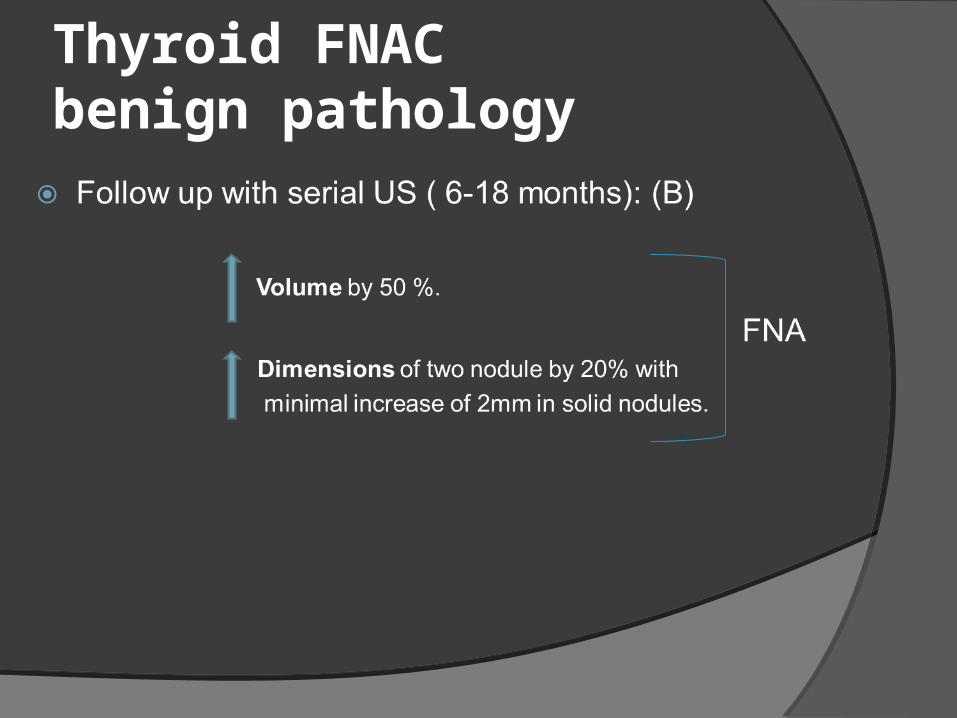
Thyroid FNACbenign pathology
Benign FNA : Long term F/u Disadvantages:
Does not improve the cancer detection rate Increase the use of U/S or repeat fine
needle aspirations,
consideration should be given to stopping further follow-up after 3 years.
FNA & Gentic work up (Afirma)
Specialized cytopathology with unique molecular analysis. Advantage:
Avoid unnecessary surgeries ( 90% reduction in number of surgeries)
Single clinic visit ( One FNA) Reduce healthcare costInform surgery choice ( TT&level VI ND, TT or hemi
thyroidectomy) Afirma BRAF & MTC
Afirma ( GEC)
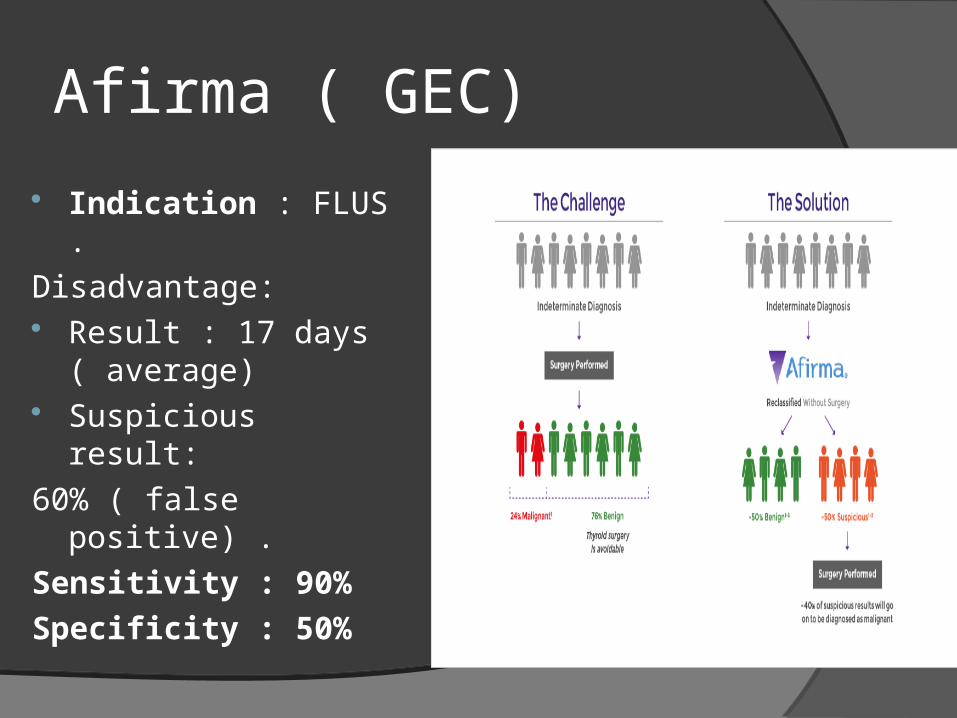
Indication : FLUS .
Disadvantage: Result : 17 days
( average) Suspicious result:
60% ( false positive) .
Sensitivity : 90%
Specificity : 50%
Medical therapy benign thyroid nodule
Thyroid nodule in children
Thyroid CA 1.5-2.0% all pediatric malignancies Malignant nodule 15-20%. 10% thyroid cancer age <21 More likely to present with neck mets Most common cause thyroid enlargement is
chronic lymphocytic thyroiditis
Thyroid nodule in children Medullary Thyroid Carcinoma:FMTC, MEN 2A, MEN 2BRET proto-oncogene (chromosome 10)Calcium / Pentagastrin stimulationProphylactic thyroidectomy recommended age 2-6
Thyroid nodule in children The diagnostic and therapeutic approach to
one or more thyroid nodules in a child should be the same as it would be in an adult (clinical evaluation, serum TSH, US, FNA).
( A)
Thyroid nodule in pregnancy
Pregnancy increases riskOne study: u/s detection nodules :
• 9.4% nulliparous women
• 25% women previously pregnantAttributed to increased renal iodide excretion
and basal metabolic rate Rosen: Nodules presenting during pregnancy :
• 30 patients, 43% were cancer
• HCG may be growth promoter (TSH-like activity)
Thyroid nodule in pregnancy
Nodules discovered in pregnant women are more likely to
be malignant than those found in nonpregnant women. Euthyroid Hypothyroid FNA should be performed in pregnancy . Hyperthyroid Radionuclide scan after pregnancy &
cessation of lactation .
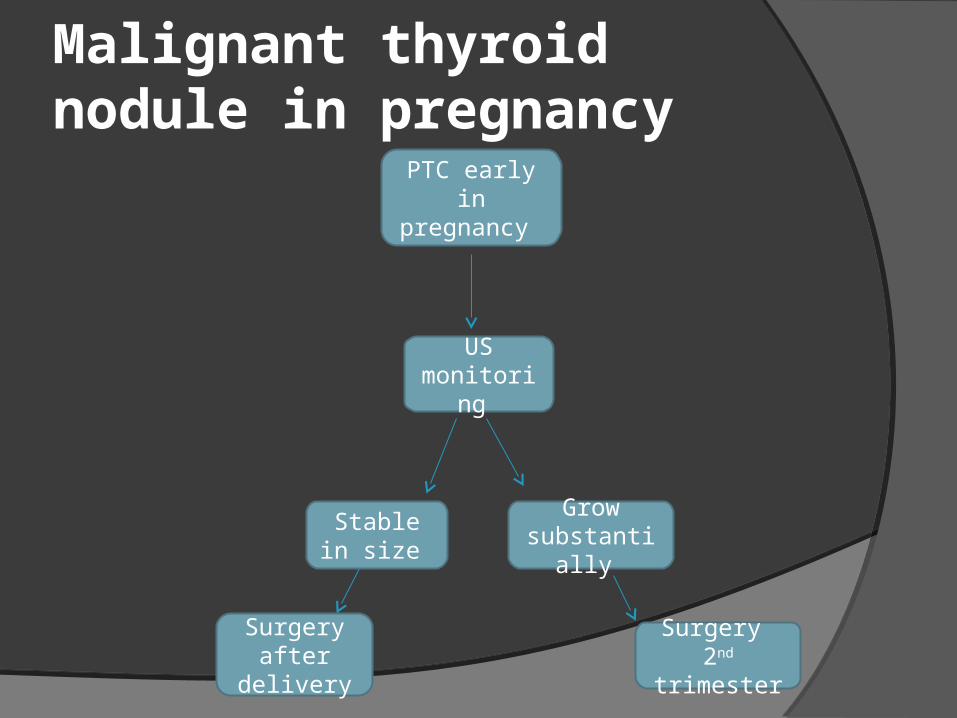
Malignant thyroid nodule in pregnancy
PTC early in pregnancy
US monitoring
Grow substantially
Surgery 2nd trimester
Stable in size
Surgery after
delivery
Malignant thyroid nodule in pregnancy If suspicious for PTC :
LT4 to keep TSH 0.1–1mU/L
Case :
35 YOF Cc: L thyroid nodule Risk : none No Compressive symptoms Clinically euthyroid Exam unremarkable except ( L thyroid
lobe nodule 3 cm )
Case
TSH : 1.7 U/S neck : well defined hypoechoic L
lobe nodule (2.5 * 0.9 * 1 cm ), no calcifications , increase vascularity , presence of halo . No lymphadenopathy
FNA : AUS
what is the management ?
Case
L hemithyroidectomy Pathology : Follicular thyroid carcinoma (2 vascular
invasion & micro capsular invasion ) , size : 3 cm
What is your proposed plan ?
Case Completion thyroidectomy. Completion & Central compartment
dissection. I 131 abltion. Observation.
FTC subtypes :
MIFTC with capsular invasion only, with limited (< or =3) vascular invasion.
Rx : hemithyroidectomy Encapsulated FTC with extensive (>3)
vascular invasion Broadly invasive FTC with extensive
invasive growth.
Rx : Total thyroidectomy
2005 by Rosai