Management of the Patient Presenting with Wide Complex Tachycardia Samir Saba, MD Director, Cardiac...
49
Management of the Patient Presenting with Wide Complex Tachycardia Samir Saba, MD Director, Cardiac Electrophysiology
-
Upload
jerome-cullipher -
Category
Documents
-
view
223 -
download
3
Transcript of Management of the Patient Presenting with Wide Complex Tachycardia Samir Saba, MD Director, Cardiac...

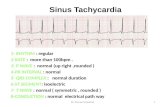
Management of the Patient Presenting with Wide Complex Tachycardia
Samir Saba, MD
Director, Cardiac Electrophysiology

Definition
• Heart rate > 100 b/min• QRS > 120 ms

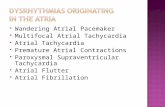
Differential Diagnosis
• Supraventricular tachycardia with aberrancy• Pre-excited tachycardia• Motion artifact• Paced rhythm• Ventricular tachycardia
– Idiopathic– Non-idiopathic

Importance of diagnosing VT
1. Sensitivity versus Specificity
2. In all patients with WCT, VT is the diagnosis in 80% of cases

SVT with aberrancy
• Typical RBBB• Typical LBBB

Typical bundle morphology
LBBB RBBB

LBBB in AVRT

RBBB and AVRT

Pre-excited Tachycardia
• Manifest versus concealed AP

WPW

WPW

Antidromic AVRT

Atrial Flutter with Preexcitation

AF with Preexcitation

Motion artifact
• Failure to recognize artifact is common:
– 94% of internists– 58% of cardiologists– 38% of EP

Motion Artifact
Recognize artifact by:• Marching the high frequency signal across the WCT• Looking at other available leads

Paced ECG

Paced ECG
PacedNot Paced

Ventricular Tachycardia
• Idiopathic– RVOT VT– LVOT VT– Lt fascicular VT
• Non-idiopathic– ICM– NICM– HCM– Channelopathy
(LQTS, Brugada, etc…)

RVOT VT

LVOT VT

Left fascicular VT

Other Classifications for VT
• Morphology:– Monomorphic – Polymorphic– Bidirectional
• Mechanisms:– Reentry– Automaticity– Triggered activity
• Drug susceptibility:– Verapamil sensitive– Adenosine sensitive

Repetitive VT

MMVT

Non-idiopathic VT

Ventricular Tachycardia

Bidirectional VT

Mechanisms of VT

Approach to Management
• History
• Physical Exam
• ECG
• EP Study

History
• Age (if >35 yrs, VT>85%) • Symptoms (palpitations, syncope, LH,
diaphoresis, angina, seizures, CA…)• Circumstances: N/V/D (electrolytes)• PMH: Cardiac disease, MI, CHF, ICD, RF• Family history: SCD, arrhythmias• Medications: QT prolongation, digoxin, diuretics,
etc…• Habits: Drugs

Physical Examination
• Hemodynamic Stability• Signs of acute CHF• Sternal wound• PVD• Stroke• PM/ICD• Evidence of AV dissociation (cannon A waves,
marked fluctuations in BP, variable S1 intensity)• Maneuvers: CSM, pharmacologic interventions
(lidocaine, adenosine, BB, verapamil)

Other tests
• Laboratory tests: K, Mg, plasma concentrations of drugs (dig, procan, etc…)
• CXR: cardiomegaly
• Echo: structural abnormalities

ECG
During WCT:
• AV dissociation• Fusion beats• Capture beats• Morphology
– Width of QRS– Morphology of the
bundles– Electrical axis– Precordial concordance
In NSR:• Ischemia• Acute MI• Old MI• Long QT• Brugada pattern• LVH• Epsilon waves

AV dissociation

Fusion beat

ECG

ECG

Therapy
• Acute Management:– For the Unstable patient:
• Emergent synchronized cardioversion• If QRS and T cannot be distinguished then defibrillation• Cautious use of sedatives and analgesics
– For the Stable patient:• Class I or III AAD• Treatment of associated conditions (ischemia,
electrolytes,…)• Elective cardioversion• Interrogation of ICD or PM if present

Therapy
• Chronic Management:• AAD:
– class IC or III, if structurally normal hearts– class III, if structurally abnormal hearts (with
ICD)
• EPS+/-RFA – Stand alone therapy in idiopathic VT– Adjunctive therapy (+/-AAD) in ischemic VT
• ICD– For primary and secondary prevention of SCD

Indication for EPS

EP Study
• Induce the arrhythmia
• Activation or Pace mapping
• Ablation

Activation Map for VT

RVOT VT: pace map

Special Case: NSVT
• EF≤35%, then ICD
• EF>40%, no ICD
• 35%<EF≤40%, then EPS and ICD if EPS+ (MUSTT trial)
In all these cases, -blockers and other AAD can be used if NSVT is symptomatic.

Summary
• DDX of WCT includes VT, SVT with aberrancy, preexcited tachycardia, artifact, and paced rhythm. VT accounts for 80%
• Diagnosis hinges of good history, PE, ECG• Acute management depends on stability of
patient. In the unstable patient, immediate cardioversion or defibrillation is recommended
• Long term management armamentarium includes: AAD, Ablation, ICD

Holter Monitor in a Mouse

EPS in a Mouse

Question?…