
Management of Subcutaneous Infusions in Palliative Care · Management of Subcutaneous Infusions in...
71
Management of Subcutaneous Infusions in Palliative Care Centre for Palliative Care Research and Education
Transcript of Management of Subcutaneous Infusions in Palliative Care · Management of Subcutaneous Infusions in...
Management of
Subcutaneous Infusions
in Palliative Care
Centre for Palliative CareResearch and Education
Palliative Care AustraliaPO Box 24Deakin WestACT 2600t: +61 2 6232 4433f: +61 2 6232 4434e: [email protected]: www.palliativecare.org.au
© 2010
Developed in conjunction withCentre for Palliative Care Research and EducationQueensland HealthLevel 7, Block 7Royal Brisbane & Women’s HospitalHerston QLD 4029t: +61 7 3636 1449f: +61 7 3636 7942e: [email protected] w: www.health.qld.gov.au/cpcre
Thanks to the Syringe Driver Replacement Program Advisory Committee for their contribution towards the 'Management of Subcutaneous Infusions in Palliative Care' education materials: Vlad Alexandric, Deputy Chief Executive Officer, Palliative Care AustraliaCathy Bennett, Clinical Services Coordinator – Palliative Care, Country Health SAPatrick Cox, Community Nurse, South Adelaide Palliative ServicesHelen Walker, Program Manager – Palliative Care, WA Cancer and Palliative Care Network
Funded by the Australian Government Department of Health and Ageing
HMMU Nov’10 1287 Griffin_jk

Management of
Subcutaneous Infusions
in Palliative Care
Centre for Palliative CareResearch and Education
Palliative Care AustraliaPO Box 24Deakin WestACT 2600t: +61 2 6232 4433f: +61 2 6232 4434e: [email protected]: www.palliativecare.org.au
© 2010
Developed in conjunction withCentre for Palliative Care Research and EducationQueensland HealthLevel 7, Block 7Royal Brisbane & Women’s HospitalHerston QLD 4029t: +61 7 3636 1449f: +61 7 3636 7942e: [email protected] w: www.health.qld.gov.au/cpcre
Thanks to the Syringe Driver Replacement Program Advisory Committee for their contribution towards the 'Management of Subcutaneous Infusions in Palliative Care' education materials: Vlad Alexandric, Deputy Chief Executive Officer, Palliative Care AustraliaCathy Bennett, Clinical Services Coordinator – Palliative Care, Country Health SAPatrick Cox, Community Nurse, South Adelaide Palliative ServicesHelen Walker, Program Manager – Palliative Care, WA Cancer and Palliative Care Network
Funded by the Australian Government Department of Health and Ageing
HMMU Nov’10 1287 Griffin_jk
1
Contents
A Guide To The Training Manual And Learning Package....................................................3 Someadultlearningprinciples..............................................................................5 Somelearningresources.......................................................................................7 Combinedreferencelistfrom ManagementofSubcutaneousInfusionsinPalliativeCare....................................7
Management of Subcutaneous Infusions in Palliative Care.............................................11 Introduction........................................................................................................12 LearningAim......................................................................................................13 LearningObjectives............................................................................................13 Howtousethisself-directedlearningpackage....................................................15 WhyareSubcutaneousInfusionsUsedinPalliativeCare?....................................15 WhataretheAdvantagesandLimitations ofSubcutaneousInfusionDevices?.....................................................................16 IndicationsandContraindications.......................................................................17
Section 1:The Patient and Family/Carer Experience.......................................................19Quiz: Section 1-ThePatientandFamily/CarerExperience..............................................22
Section 2:General Equipment........................................................................................23QUIZ: Section 2 - EquipmentGuidelinesandPrinciples..................................................27
Section 3: Selection and Preparation of the Site.............................................................28QUIZ: Section 3 -Selection,PreparationandMaintenanceoftheSite.............................35
Section 4:Drugs and Diluents........................................................................................37QUIZ: Section 4.1-DrugsandDiluents...........................................................................42QUIZ: Section 4.2 -DrugsandDiluents(Calculations).....................................................45
Section 5: Patient and Family/Carer Education...............................................................47Quiz: Section 5 -PatientandFamily/CarerEducation.....................................................52
Section 6:Patient Assessment and Troubleshooting......................................................54Quiz: Section 6 -PatientAssessmentandTroubleshooting................................................66
Self Assessment............................................................................................................67
Conclusion.....................................................................................................................68
Quiz Answers.................................................................................................................69
Patient and Family/Carer Statements.............................................................................71

2
This page is intentionally left blank
4
A Guide to the Training Manual and Learning Package
Thismanualprovidesguidancetoparticipantsinthe‘TraintheTrainer’
workshopinuseoftheManagementofSubcutaneousInfusionsinPalliative
Carelearningpackage,aswellassometeachingandlearningprinciples
andresources.
Useofsubcutaneousinfusiondeviceshasbecomestandardpractice
inpalliativecareandimprovespatientcomfortbyadministrationof
medicationsataconstantratetoassistinsuccessfulcontrolofavarietyof
symptoms.
Therearesomelimitationsandrisksinuseofthesedevicesincluding
inflexibilityofprescription,technicalproblemsandskinreactionsatthe
subcutaneouscannulainsertionsite.Subcutaneousinfusiondevices
shouldbemanagedinaccordancewithlocalpoliciesandprocedures,by
knowledgable,appropriatelytrainedstafftominimiseriskspresentedbythe
limitationsofindividualdevicesandtheiruse.
Informationcontainedinthelearningpackageispresentedtopromotea
standardapproachtoclinicalcareinvolvingasubcutaneousinfusion.It
isnotintendedaseducationinanyspecificdevice.Itprovidesbaseline
informationtobeusedtodevelopknowledgeforbeginnerlevelpractice
withsubcutaneousinfusiondevicesorrevisionforthemoreexperienced
practitioner.
Healthprofessionalsareatalltimesaccountableandresponsiblefortheir
ownactionsandshouldbeawareofthelimitsoftheirknowledge,skillsand
competenceandactwithinthoselimits.
Acquisitionofbasicknowledgeaboutsubcutaneousinfusionsinpalliative
careshouldbefollowedbydemonstrationsandsupervisedpracticeto
attainbeginnerlevelcompetencyinthatdevice.Settingupandmanaging
asubcutaneousinfusiondeviceisaskillthatmaylapseifnotpractised
1CruikshankS,AdamsonE,LoganJ,BrackenridgeK.2010.Usingsyringedriversinpalliativecarewithinarural,communitysetting:capturingthewholeexperience.InternationalJournalofPalliativeNursing;16(3):126-132.
5
regularlyandmaintainingcompetencycanbedifficultforpractitionerswho
havevariableexposuretodevicesandtheiruse.1
Thepackageispresentedinthreedifferentforms–website,DVD,andhard
copy–tocaterfordifferentlearningstylesandpreferencesandthefact
thatsomehealthprofessionalswillnothavegoodinternetaccessand/or
webnavigationskills.Thepackagepresentsintroductoryinformationabout
subcutaneousinfusionsanddevicesincludingrecentchangesinAustralia,
andsixsectionsbasedontheCentreforPalliativeCareResearchand
Education’s‘Guidelinesforsubcutaneousinfusiondevicemanagementin
palliativecare’.
Itissuggestedparticipantsworkthrougheachofthesectionsinturn.They
shouldreadtheinformationineachsection,readorwatchgivenlinksand
completeactivities.Attheendofeachmodule,aseriesofquestionsinthe
formofashortquizwillbepresentedtoenableparticipantstotesttheir
understanding.Theanswerstothesequestionsarecoveredbythecontent,
linksandactivitiesineachsection.Thepackagealsorequiresparticipantsto
sourcecertaininformationfromtheirownorganisation.
Completionofallsectionsofthelearningpackageprovidesbaseline
informationforbestpracticeuseofsubcutaneousinfusiondevices,allowing
forcompetencydevelopmentandmaintenance.Completionoftheself
assessmentincludingdiscussionwithaknowledgablehealthprofessionalis
recommended.
Some Adult Learning Principles
Thereisavastamountofinformationavailableaboutteachingandlearning
principles.Aselectionisprovidedheretosupportyouinyoureducationof
healthprofessionalsaboutsubcutaneousinfusiondevices.Knowles’theory
ofadultlearning2isbasedonseveralassumptions:
2KnowlesMS,HoltonEF,SwansonRA(2005).Theadultlearner(Sixthed).London:Elsevier.
6
1. Theneedtoknow.Adultsneedtoknowwhytheyneedtolearnsomething beforecommittingtolearnit.
2. Thelearners’self-concept.Adultshaveaself-conceptofbeing responsiblefortheirownlivesanddecisions,andresentsituations wheretheyfeelanotherisimposingtheirwillonthem.Thiscanpresent challengesinadulteducation.Itisimportanttohelpthelearnerbeand feelasself-directedaspossible.
3. Theroleofthelearners’experience.Learnerscomewithalltheirlife experiencewhichmeansthatformanykindsoflearning,theadult learnersthemselvesalreadyhaverichresourcesforlearning.However thatcanproducebiases,mentalhabitsandpreconceptionsthatclose ourmindstofreshperceptions,newideasanddifferentwaysofthinking. “…inanysituationinwhichtheparticipants’experiencesareignored ordevalued,adultswillperceivethisasrejectingnotonlytheir experience,butrejectingthemselvesaspersons.”2
4. Readinesstolearn.Adultsarereadytolearnthethingstheyneedto knowandbeabletodoinordertobeeffectiveinreal-lifesituations, suchastheirwork.
5. Orientationtolearning.Adultsarelife-centred,ortask-centredor problem-centredintheirlearningorientation.Theyaremotivatedto learntotheextenttheyperceivethelearningwillhelpthemsolve problemsorperformtasksinreallife.Adultslearnnewknowledge mosteffectivelywhenpresentedinthecontextofareallifesituation.
6. Motivation.Themostpotentmotivatorsforadultsareinternal,such asthedesireforincreasedjobsatisfaction,qualityoflife,andself- esteem.Externalmotivatorssuchasbetterjob,promotion,highersalary areimportantbutlessso.Adultsaremotivatedtokeepgrowingand developingbutthismaybeblockedbynegativeself-concept,time constraints,andeducationalprogramsthatviolateadultlearning principles.
Adultlearnershavearichbackgroundoflifeexperiences,bothpersonaland
workrelated.Trytotapintothatexperiencewhenteaching–forexample
• whatexperiencedoesthepersonalreadyhavewithinfusiondevices?
• dotheyhaveanyconcernsaboutusingthedevicese.g.apre-
conceptionthatasubcutaneousinfusionwillhastendeath?
2KnowlesMS,HoltonEF,SwansonRA(2005).Theadultlearner(Sixthed).London:Elsevier.
7
Forthesesortsofreasons,startwithidentifyingthebeginninglevelof
knowledgeofyourparticipants.
Adultsenjoytheopportunitytoapplynewknowledge–apractical
demonstrationaccompaniedbythechancetoactuallyusethedeviceallows
themthatopportunity.
Some learning resources
EgleC(2007).Adultlearningprinciplesforfacilitators.RuralHealth
EducationFoundation.Availablefromhttp://www.rhef.com.au/wp-content/
uploads/userfiles/716_alp_lr.pdf
KnowlesMS,HoltonEF,SwansonRA(2005).Theadultlearner(Sixthed).
London:Elsevier.
Combined reference list from ‘Management of Subcutaneous Infusions in Palliative Care’
AbbasS,YeldhamM,BellS.Theuseofmetalorplasticneedlesincontinuoussubcutaneousinfusioninahospicesetting.AmericanJournalofHospiceandPalliativeMedicine2005;22(2):134-138.
BreckenridgeA.Reportoftheworkingpartyontheadditionofdrugstointravenousinfusionfluids[HC(76)9][Breckenridgereport].London:DepartmentofHealthandSocialSecurity;1976.
BritishNationalFormulary.Syringedrivers.<www.bnf.org>.Accessed26January2005.
CentreforPalliativeCareResearchandEducation.Guidelinesforsubcutaneousinfusiondevicemanagementinpalliativecare(RevisedEdition).Brisbane,Queensland:QueenslandHealth;2010.
CHRISP(CentreforHealthcareRelatedInfectionSurveillanceandPrevention).Occupationalexposurestobloodandbodyfluids:Recommendedpracticesforpreventinghollow-boreneedlestickinjuries(Recommendation2:Wingedinfusionsetsforsubcutaneousandintravenousinfusions).QueenslandGovernment(QueenslandHealth);2007.<http://www.health.qld.gov.au/chrisp/resources/hollbore_rec_prac.pdf>.Accessed28June2010.
8
Coleridge-SmithE.TheuseofsyringedriversandHickmanlinesinthecommunity.BritishJournalofCommunityNursing1997;2(6):292,294,296.
GovernmentofWesternAustralia,DepartmentofHealth.Palliativecaremedicineandsymptomguide.WACancerandPalliativeCareNetwork;2010.Availablefrom:http://www.healthnetworks.health.wa.gov.au/cancer/docs/Consumer_Book.pdf
CruikshankS,AdamsonE,LoganJ,BrackenridgeK.Usingsyringedriversinpalliativecarewithinarural,communitysetting:capturingthewholeexperience.InternationalJournalofPalliativeNursing2010;16(3):126-132.
DickmanA,LittlewoodC,VargaJ.Thesyringedriver:continuoussubcutaneousinfusionsinpalliativecare.Oxford:OxfordUniversityPress;2002.
DickmanA,SchneiderJ,VargaJ.Thesyringedriver:continuoussubcutaneousinfusionsinpalliativecare.2nded.Oxford:OxfordUniversityPress;2005.
DriscollA.Managingpostdischargecareathome:ananalysisofpatients’andtheircarer’sperceptionsofinformationreceivedduringtheirstayinhospital.JournalofAdvancedNursing2000;31(5):1165-1173.
FletcherC.ReportoncomparativeevaluationofGrasebysyringedriverreplacements.Auckland,NZ:NorthShoreHospiceTrust;2009.Retrieved4October2010fromhttp://www.cme-infusion.com/documents/pub/Report%20on%20Comparative%20Evaluation%20of%20Graseby%20Syringe%20Driver%20Replacements.pdf
FlowersC,McLeodF.Diluentchoiceforsubcutaneousinfusion:asurveyoftheliteratureandAustralianpractice.InternationalJournalofPalliativeNursing2005;11(2):54-60.
GomezY.Theuseofsyringedriversinpalliativecare.AustralianNursingJournal2000;(2):suppl1-3.
GrahamF.Thesyringedriverandthesubcutaneousrouteinpalliativecare:theinventor,thehistoryandtheimplications.JournalofPainandSymptomManagement2005;29(1):32-40.
JointTherapeuticsCommission.Asurveyofdoctorsontheirpreferredmedicationsforvarioussymptomsinpalliativecare.Brisbane:Unpublisheddata;2005.
LichterI,HuntE.Drugcombinationsinsyringedrivers.TheNewZealandMedicalJournal1995;108(1001):224-226.
Lloyd-WilliamsM,RashidA.Ananalysisofcallstoanout-of-hourspalliativecareadviceline.PublicHealth2003;117(2):125.
9
McNeillyP,PriceJ,McCloskeyS.Theuseofsyringedrivers:apaediatricperspective.InternationalJournalofPalliativeNursing2004;10(8):399-404.
MittenT.Subcutaneousdruginfusions:areviewofproblemsandsolutions.InternationalJournalofPalliativeNursing2001;7(2):75-85.
MorganS,EvansN.Asmallobservationalstudyofthelongevityofsyringedriversitesinpalliativecare.InternationalJournalofPalliativeNursing2004;10(8):405-412.
NegroS,SalamaA,SanchezY,AzuaratM,BarciaE.Compatibilityandstabilityoftramadolanddexamethasoneinsolutionanditsuseinterminallyillpatients.JournalofClinicalPharmacyandTherapeutics2007;32:441-444.
O’DohertyC,HallE,SchofieldL,ZeppetellaG.Drugsandsyringedrivers:asurveyofadultspecialistpalliativecarepracticeintheUnitedKingdomandEire.PalliativeMedicine2001;15:149-154.
PalliativeCareExpertGroup.Therapeuticguidelines:palliativecare.Version3.Melbourne:TherapeuticGuidelinesLtd;2010,p.292.
PalliativeCareMatters.<www.pallcareinfo>.Accessed10August2010
PalliativeCareOutcomesCollaborative(PCOC)websitehttp://chsd.uow.edu.au/pcoc/
PalliativeCareOutcomesCollaborative.<http://chsd.uow.edu.au/pcoc/>.Accessed13August2010.
PalliativeDrugs.com.‘Syringedrivers.’<www.palliativedrugs.com>.Accessed25January2005.
PetersonG,MillerK,GallowayJ,DunneP.Compatibilityandstabilityoffentanyladmixturesinpolypropylenesyringes.JournalofClinicalPharmacyandTherapeutics1998;23:67-72.
RatcliffeN.Syringedrivers.CommunityNurse1997;3(6):25-26.
ReymondE,CharlesM.Aninterventiontodecreasemedicationerrorsinpalliativepatientsrequiringsubcutaneousinfusions:BrisbaneSouthPalliativeCareServiceandAdverseDrugEventPreventionProgram;unpublishedreportpresentedtoClinicalServicesEvaluationUnit;PrincessAlexandraHospital.Brisbane,Queensland;2005
ReymondL,CharlesMA,BowmanJ,TrestonP.Theeffectofdexamethasoneonthelongevityofsyringedriversubcutaneoussitesinpalliativecarepatients.MedicalJournalofAustralia2003;178:486-489.
10
RossJR,SaundersY,CochraneM,ZeppetellaG.Aprospective,within-patientcomparisonbetweenmetalbutterflyneedlesandTefloncannulaeinsubcutaneousinfusionofdrugstoterminallyillhospicepatients.PalliativeMedicine2002;16:13-16.
WorldHealthOrganization.http://www.who.int/cancer/palliative/definition/en/Accessed28July2010.
Yatesetal.2004inCruikshankS,AdamsonE,LoganJ,BrackenridgeK.Usingsyringedriversinpalliativecarewithinarural,communitysetting:capturingthewholeexperience.InternationalJournalofPalliativeNursing2010;16(3):126-132.
12
Management of Subcutaneous Infusions in Palliative Care
Introduction
Thisinformationispresentedtopromoteastandardisedapproachto
clinicalcareinvolvingasubcutaneousinfusiondevice.Suchanapproach
shouldminimisepracticeerrorsthatcanresultinseriousadverseevents
andanongoingrisktopatientsafety.Itprovidesbasicinformationfor
beginnerlevelpracticewithsubcutaneousinfusiondevicesorrevisionfor
themoreexperiencedpractitioner.Thepackageisnotdevicespecific,and
inanorganisationalsettingshouldbecomplementedbycomprehensive
informationaboutthesubcutaneousinfusiondevicebeingusedwithinthat
organisationorservice.
Healthprofessionalsareatalltimesaccountableandresponsiblefortheir
ownactionsandshouldbeawareofthelimitsoftheirknowledge,skillsand
competenceandactwithinthoselimits.Competencyhasbeendescribed
asanabilitytothinkinactionandmakeconfident,cleardecisionsbased
onsoundknowledge.Settingupandmanagingasubcutaneousinfusion
deviceisaskillthatmaylapseifnotpractisedregularly,andmaintaining
competencycanbedifficultforpractitionerswhohavevariableexposureto
thedeviceanditsuse.1
Theacquisitionofbasicknowledgeaboutsubcutaneousinfusiondevices,
reasonsfortheiruseandthedrugscommonlyadministeredinthecareof
apalliativepatientshouldbefollowedbydemonstrationsandsupervised
practicetoattainbeginnerlevelcompetencyinaparticulardevice.
Aswithallmedicaldevices,theoperationofasubcutaneousinfusiondevice
shouldonlybeundertakenby,orunderthesupervisionof,appropriately
trainedstaffandinaccordancewithlocalpoliciesandproceduresand
manufacturers’guidelines.
13
Learning Aim
Theaimofthislearningpackageistoassistthecliniciantodevelop
knowledgeandskillsofthebasicprinciplesofcareforpeoplewith
subcutaneousinfusiondevicesinpalliativecaresettings.
Thispackageisdesignedtoprovideself-directedlearning;completiondoes
notprovideformalaccreditation.Supervisedpracticewithappropriately
trainedstaffmanagingthedeviceusedbyyourserviceisrecommended.
Learning Objectives
Following successful completion of this package, you should be able to:
• discusstheindicationsandcontraindicationsforsubcutaneous
infusionsinpalliativecare;
• explainmanagementandsafetyprincipleswhenusinginfusion
devices;
• discussprinciplesofappropriateandinappropriatesiteselectionfor
insertionofacannula;
• describestrategiesforpreventingsiterelatedproblems;
• identifydrugscommonlyusedinsubcutaneousinfusions,andtheir
indicationsforuse;
• provideaccurateinformationandeducationtopatientsandfamilies/
carersusingsubcutaneousinfusiondevices;
• safelymonitorthepatientwithasubcutaneousinfusioninsitu.
14
Disclaimer
Theinformationcontainedinthismanualhasbeencompiledbythe
CentreforPalliativeCareResearchandEducation(CPCRE)andPalliative
CareAustralia(PCA)foreducationalandinformationpurposesonly.
Itisintendedtoassisthealthcareprofessionalsindevelopingtheir
knowledgeofkeyprinciplesconcerningtheuseofsubcutaneous
infusiondevicesinpalliativecare.
WhileCPCREandPCAhavetakenparticularcareincompilingthis
manual,errorsmayoccur.Therefore,CPCREandPCAgivenowarrantyas
toitsaccuracyorcompleteness.
Themanualisnotintendedtoreplaceorconstitutemedicaladvice
andshouldnotbeconstruedasspecificinstructionsforthedelivery
ofmedicaltreatmentorcareortheuseofanyparticulardevice
forprovidingasubcutaneousinfusion.Itisnotasubstitutefor
independentprofessionalmedicaladviceandshouldnotbereliedupon
tosolveissuesthatmayariseinindividualcases.
CPCREandPCAdonotacceptliabilityforanydirect,incidentalor
consequentiallossordamagearisingfromtheuseoforrelianceupon
theinformationcontainedinthismanual.
Healthcareprofessionalsshouldalsoseektraining,supervisionand
advicefromappropriatelyqualifiedandexperiencedcliniciansinorder
todeveloptherequiredlevelofclinicalcompetencetoproperlytreat
patients,whereappropriate,usingsubcutaneousinfusiondevices.

15
How to Use this Self-Directed Learning Package
TheCentreforPalliativeCareResearchandEducation’s‘Guidelinesfor
subcutaneousinfusiondevicemanagementinpalliativecare’(theGuidelines)
areanimportantcomplementarydocumenttothislearningpackage.
Itissuggestedyouworkthrougheachofthesectionsinturn.Readthe
information,readorwatchgivenlinksandcompleteactivities.Thepackage
alsorequiresyoutosourcecertaininformationfromyourownorganisation.
Attheendofeachsection,aseriesofquestionsintheformofashortquiz
willbepresentedtoenableyoutotestyourunderstanding.Theanswers
tothesequestionsarecoveredbythecontent,linksandactivitiesineach
section.Completionoftheselfassessment,includingdiscussionwitha
knowledgablehealthprofessional,isrecommended.
Why are Subcutaneous Infusions Used in Palliative Care?
TheWorldHealthOrganisation(2004)statedthatpalliativecareis“an
approachtocarewhichimprovesqualityoflifeofpatientsandtheirfamilies
facinglife-threateningillness,throughthepreventionandreliefofsuffering
bymeansofearlyidentificationandimpeccableassessmentandtreatment
ofpainandotherproblems,physical,psychosocialandspiritual”.2Palliative
careisprovidedaccordingtotheneedsoftheindividualandmayhappen
days,weeksormonthsbeforedeath.Itshouldbeavailablewhereverthe
personchooses–athomeorinahospital,hospiceorresidentialagedcare
facilityandbesupportedbyateamofhealthprofessionalsincludinga
specialistpalliativecareteamifneeded.
Theadministrationofmedicationusingasubcutaneousinfusiondeviceis
commonpracticeinpalliativecareforthemanagementofpainandother
distressingsymptomswhenotherroutesareinappropriateorineffective.3
Thesedevicesarepowerdriven,deliveringmedicationsatacontrolledrate
toprovidesymptomcontrol.Subcutaneousinfusiondeviceshavebecome
animportantpartofcaretoensurecomfortformanypatients.4
Formanyyears,theGrasebysyringedriverwastheprimarydevicefor
16
subcutaneousadministrationofarangeofdrugsinpalliativecare.Inearly
2007themanufactureroftheGrasebyMS16AandMS26syringedrivers
informedtheTherapeuticGoodsAdministration(TGA)oftheirintentionto
withdrawthedevicesfromsaleinAustralia.InOctober2007thenewTGA
regulatorystandardsregardingmedicalinfusiondevicesbecamemandatory.
GrasebysyringedriverspurchasedpriortoOctober2007continuetobe
supportedbythemanufacturerfordevicemaintenance,allowingservices
totransitiontodevicesthatmeetthenewregulatorystandards.Information
containedinthislearningpackageisrelevanttodevicesnowinusein
Australia.5
What are the Advantages and Limitations of Subcutaneous Infusion Devices?
Subcutaneous delivery of medication via an infusion device:
• allowsthecontinuoussupplyofarangeofdrugsbypassingthegutand
associatedproblemswithswallowingandmalabsorption3;
• canprovidemorestableplasmalevelsofdrugsandbettersymptom
controlaspeaksandtroughsofintermittentdrugadministrationare
avoided3;
• generallyinvolvesasmall,portableorrelativelyportablebatteryoperated
pumpthatdeliversmedicationsatanaccuratelycontrolledrate6;
• providesversatilityofferingaconvenient,accessiblealternativefor
continuousadministrationofmedications;
• canbeusedforambulantpatientswithmostdevicesabletobeworn
relativelyunobtrusively,notinterferingwithpatientswantingto
continuewiththeirnormaldailyactivities;
17
• canprovidecontinuedmanagementofsymptomsremovingtheneed
forfrequentinterventionslikerepeatedoralmedicationsorinjections
atendoflife.
Indications and Contraindications
Indications for commencement of a subcutaneous infusion include:
• inabilitytoswallowduetodysphagiafromphysicalobstruction/
tumourinthemouth,throatoroesophagus;
• persistentnauseaandvomiting;
• severeweakness;
• unconsciousness;
• bowelobstruction.3
Contraindications for use of this route include:
• lackofpermissionfromthepatientand/orfamily/carerasproxy;
• whereotherviableroutesofadministrationareavailable;
• wherecontraindicationsexistrelatedtothedrugstobeinfused.
Thedecisiontocommenceasubcutaneousinfusionofmedicationshouldbe
madeaftercarefulassessmentandreviewbyhealthprofessionalsinvolved
inthepatient’scare,thepatient,andfamily/carer.
18
References
1. CruikshankS,AdamsonE,LoganJ,BrackenridgeK.Usingsyringedriversinpalliative carewithinarural,communitysetting:capturingthewholeexperience.International JournalofPalliativeNursing2010;16(3):126-132.
2. WorldHealthOrganization.http://www.who.int/cancer/palliative/definition/en/ Accessed28July2010.
3. DickmanA,LittlewoodC,VargaJ.Thesyringedriver:continuoussubcutaneous infusionsinpalliativecare.Oxford:OxfordUniversityPress;2002.
4. MittenT.Subcutaneousdruginfusions:areviewofproblemsandsolutions. InternationalJournalofPalliativeNursing2001;7(2):75-85.
5. CentreforPalliativeCareResearchandEducation.Guidelinesforsubcutaneous infusiondevicemanagementinpalliativecare(RevisedEdition).Brisbane, Queensland:QueenslandHealth;2010.
6. McNeillyP,PriceJ,McCloskeyS.Theuseofsyringedrivers:apaediatricperspective. InternationalJournalofPalliativeNursing2004;10(8):399-404.
19
Section 1: The Patient and Family/Carer Experience
Healthprofessionalsinvolvedinendoflifecarehaveforalongtime
assumedthatpatientsfinduseofasubcutaneousinfusiondeviceacceptable
becauseofitscompactsizeandthatitsusefacilitatesindependenceandthe
optionofbeingcaredforathome.Howevertherehasbeenlittleresearchinto
patients’attitudestosupportthisassumptionaboutsubcutaneousinfusion
devices.1Althoughitistruethesedeviceshaveallowedmanypatientstobe
athomewiththeirfamily,healthcareprofessionalsneedtobemindfulof
howthepatientandfamily/carerperceivetheexperienceofasubcutaneous
infusiondevice.
Learning Objectives
At the completion of this section, you should be able to:
• describeaspectsoftheexperienceofhavingasubcutaneousinfusion
fromthepatientandfamily/carerpointofview;
• demonstrateanunderstandingofthepotentialimpactonpatientand
family/carerofhavingasubcutaneousinfusion.
Somestudieshavereportedthatsubcutaneousinfusionsarewellaccepted
andcanachievealmost100%complianceamongstpeoplewithalife
limitingillness2,butbeingattachedtoasubcutaneousinfusiondevicecan
posedifficultiesforthepatientandfamily/carer.Inpracticaltermsofnormal
dailyactivities,considerationneedstobegivento:
• choosingclothestowear;
• bathing;
• wearingaseatbeltinrelationtocannulaposition;
• thesizeandweightofthedeviceanditsabilitytobeworndiscreetly;
20
• sleepingpositioninrelationtocannulaposition;
• devicesthatmayrequirefrequentbatterychangesorfrequentaccess
toapowerpointforchargingmaycreateareluctancetoleavethehome;
• reportsbysomepatientsthatthedevicesarenoisy3andinconvenient;
• questionsaboutfoodandalcoholintake;
• patientsandfamily/carerswhoperceivethesechangesasanegative
impactontheirlifestyle.
Patientandfamily/carerperceptionsorexperiencesofasubcutaneous
infusiondevicearevariedandindividualtotheperson,theenvironmentand
theunderlyingcauseforuseofthedevice.Beingmindfulthatthedevicewill
beperceiveddifferentlydependentuponthesefactorswillaidthehealth
professionaltoprovideapositiveexperienceforthepatientandfamily/carer.
Rememberingthatthepatientandfamily/carermaynothaveconsidered
advancecareplanninggoals,negativeperceptionsoftheinfusiondevice
maybeinfluencedbythefollowing:
• thedevicemaybeviewedasaninvasionofbodyprivacy;
• thedevicemaybeperceivedasanindicatorofapoorprognosis4;
• thepatientandfamily/carermayhavefearsassociatedwithdrugs
commonlyusedinpalliativecare;
• thedevicemaybecomethefocusoffearofimpendingdeath.
Thoughtfulexplanationgivenwithcaretoprovideinformationandsupport
appropriatetotheindividualpatientandfamily/carermayassistthehealth
professionaltounderstandthesignificancethattheyattachtothechange
incareandanyassociatedemotionaldistress.5Goodanticipatorycarewith
welltimedinformationensuringpatientandfamily/carerunderstandingcan
beassociatedwithapositiveexperienceforpatient,family/carerandhealth
professional.
21
Links
Section1‘Guidelinesforsubcutaneousinfusiondevicemanagementin
palliativecare’
Activity
ReadClientandFamily/CarerStatementsattheendofthisbooklet,about
theexperienceofasubcutaneousinfusiondevice.
WatchexcerptfromChapter2–‘WhoNeedsone?’ofBrisbaneSouth
PalliativeCareCollaborative’sGuideforClinicians–HowtoUseaSyringe
DriverforPalliativeCarePatients.
References
1. GrahamF.Thesyringedriverandthesubcutaneousrouteinpalliativecare:the inventor,thehistoryandtheimplications.JournalofPainandSymptomManagement 2005;29(1):32-40.
2. MorganS,EvansN.Asmallobservationalstudyofthelongevityofsyringedriversites inpalliativecare.InternationalJournalofPalliativeNursing2004;10(8):405-412.
3. FletcherC.ReportoncomparativeevaluationofGrasebysyringedriverreplacements. NorthShoreHospiceTrust;2009.Retrieved4October2010fromhttp://www.cme- infusion.com/documents/pub/Report%20on%20Comparative%20Evaluation%20 of%20Graseby%20Syringe%20Driver%20Replacements.pdf
4. Coleridge-SmithE.TheuseofsyringedriversandHickmanlinesinthecommunity. BritishJournalofCommunityNursing1997;2(6):292,294,296.
5. CruikshankS,AdamsonE,LoganJ,BrackenridgeK.Usingsyringedriversinpalliative carewithinarural,communitysetting:capturingthewholeexperience.International JournalofPalliativeNursing2010;16(3):126-132.
22
Quiz: Section 1 - The Patient and Family/Carer Experience
ThisquizwilltesttheobjectivesandcontentinSection1oftheLearning
Packageandthe‘Guidelinesforsubcutaneousinfusiondevicemanagement
inpalliativecare’document.
Q1) Whenstartingasubcutaneousinfusion,whichofthefollowingshould beconsideredwhenpreparingthepatientandfamily/carerfor
theexperience:
Changesinlevelofalertness
clothing
alcoholintake
driving
alloftheabove
Q2) Commencingasyringedriverisperceivedbysometomean? Goodprognosis
Poorprognosis
Doctorshave‘givenup’onthem
Nothingisworking
Alloftheabove
Q3) Infusionsareonlycommencedwhendeathislikelytohappens withindays
True
False
Q4) Commencingasubcutaneousinfusionviaadevicemeansthatthe personcannotattendtonormalADLs
True
False
Q5) Providinggoodinformationaboutasubcutaneousinfusiondevicecan changetheexperienceforpatientorfamily/carer
True
False
23
Section 2: General Equipment
Learning Objectives
Atthecompletionofthissection,youshouldbeableto:
• describesubcutaneousinfusiondevicescurrentlyinuseinpalliative
careinAustralia;
• explainmanagementprincipleswhencaringforpatientswiththese
devices;
• describeimportantsafetyprincipleswhenusingthisequipment.
Types of Subcutaneous Infusion Devices
Subcutaneousinfusiondevicesaregenerallyelectronic,batterydriven
deviceswithasyringe,cassetteorreservoirtoholdmedicationstobe
deliveredviathesubcutaneousroutetothepatient.Devicescurrentlyinuse
inAustraliaincludetheNikiT34,Graseby,CADDLegacyPCA,GemStarand
WalkMed350LX.
Important Principles when using Subcutaneous Infusion Devices
TheGuidelinesdiscussthefollowingprinciplesregardingequipment
usedforsubcutaneousinfusions.Whensettinguptheequipmentfora
subcutaneousinfusion,itisalwaysimportanttoconsultthemanufacturer’s
guidelinesandverifytheindividualorganisation’sprotocolregardingthe
preparationandset-upforchangingthedevice.
24
General Principles
General management principles for all subcutaneous infusion devices include:
• alwaysusethemanufacturer’sguidelinesandyourorganisation’s
protocolregardingpreparationandset-upforchangingthedeviceto
guideyourpractice;
• anaseptictechniqueshouldbeusedwhenpreparingandsettingup
theinfusion1;
• subcutaneousinfusiondeviceshavetraditionallybeenusedtodeliver
medicationsovera24hourperiodtoreducetheriskoferrorsinsetting
upthedevice1,2-4;
• microbiologicalstabilityandphysicalandchemicalcompatibilitydata
mostcommonlyrelatetoa24hourperiodanditisforthisreasonthat
a24hourinfusionperiodisstillrecommended5;
• documentationofvolumetobeinfused(inthesyringeorreservoir)is
recommendedattimeofset-upandregularchecks;
• considerusingatamper-proof‘lock-box’ifthereisapossibilityofthe
patientorotherstamperingwiththedeviceorusingtheboost
facility;itispossiblethatatamper-proofboxismandatorywithinyour
organisationasariskmanagementstipulation;
• ensurethatthepatientandfamilyhavereceivedafullexplanationof
howthesubcutaneousinfusiondeviceworks,itsindicationsforuse,
anda24-hoursupportnumber;
• devicesshouldbeservicedannuallybythemanufacturerora
biomedicaltechnician.
25
Syringe Related Principles
• whereasyringeisnecessary,aLuer-Lok®syringeshouldbeusedto
preventriskofdisconnection3,6;20mlistherecommendedminimum
syringesize7toreducetheriskofincompatibilityandadversesite
reactions,andminimisetheeffectofprimingtheline;
• thesamebrandofsyringeshouldbeusedeachtimetominimiseerrors
insettingupthedeviceandcalculatingtherate3,6(Grasebyonly);
Cannula Related Principles
BecauseaTeflonorVialoncannulaisassociatedwithlesssiteinflammation,
itshouldbeusedratherthanametalneedle.
Dosage Related Principles
• whenchangingtheextensionsetand/orcannula,primethelineafter
drawinguptheprescribedmedications,andbeforeconnectingtothe
patient.Afterprimingtheline,notethevolumetobeinfusedand
documentthelinechangeandthetimetheinfusioniscalculatedto
finish;
• aminimumvolumeextensionsetshouldbeusedtominimisedead-
spaceintheline7;
• fortheGraseby,itisthelengthofthesolutionwithinthesyringe–not
thevolume–thatwilldeterminetherate,i.e.thesyringedriver
deliveryrateisameasureofdistance,notameasureofvolume
administered.
26
References
1. RatcliffeN.Syringedrivers.CommunityNurse1997;3(6):25-26.
2. O’DohertyC,HallE,SchofieldL,ZeppetellaG.Drugsandsyringedrivers:asurveyof adultspecialistpalliativecarepracticeintheUnitedKingdomandEire.Palliative Medicine2001;15:149-154.
3. DickmanA,LittlewoodC,VargaJ.Thesyringedriver:continuoussubcutaneous infusionsinpalliativecare.Oxford:OxfordUniversityPress;2002.
4. PalliativeDrugs.com.‘Syringedrivers.’<www.palliativedrugs.com>.Accessed25 January2005.
5. BreckenridgeA.Reportoftheworkingpartyontheadditionofdrugstointravenous infusionfluids[HC(76)9][Breckenridgereport].London:DepartmentofHealthand SocialSecurity;1976.
6. MittenT.Subcutaneousdruginfusions:areviewofproblemsandsolutions. InternationalJournalofPalliativeNursing2001;7(2):75-85.
7. DickmanA,SchneiderJ,VargaJ.Thesyringedriver:continuoussubcutaneous infusionsinpalliativecare.2nded.Oxford:OxfordUniversityPress;2005.

27
QUIZ: Section 2 - Equipment Guidelines and Principles
ThisquizwilltesttheobjectivesandcontentinSection2oftheLearning
Packageandthe‘Guidelinesforsubcutaneousinfusiondevicemanagement
inpalliativecare’document.
Q1) Itisnotnecessarytoverifyyourworkplaceprotocolregarding
preparationandset-upforsubcutaneousinfusiondevice.
True
False
Q2) Therecommendedsubcutaneousinfusionperiodis24hours. True
False
Q3) Thepatientandfamilydonotneedanexplanationofhowthe subcutaneousinfusiondeviceworks,orindicationsforuse.
True
False
Q4) Therecommendedminimumsyringesizeis10ml. True
False
Q5) Alwaysemployanaseptictechniquewhenchangingthecannula. True
False
Q6) Thevolumetobeinfused,i.e.thevolumeinthesyringeorreservoir, shouldbedocumentedatthetimeofset-upandregularchecks.
True
False
28
Section 3: Selection, Preparation and Maintenance of the Site
Learning Objectives
At the completion of this section, you should be able to:
• explainthemostappropriatesitesforsubcutaneousinfusion;
• explainwhichsitesareinappropriateforsubcutaneousinfusion;
• describetechniquesthatmayassistinminimisingsiteirritation;
• describeimportantprinciplesforsiteinspection.
General principles for appropriate site selection
• useanareawithagooddepthofsubcutaneousfat;
• useasitethatisnotnearajoint;
• selectasitethatiseasilyaccessiblesuchasthechestorabdomen;
• selectandusesitesonarotatingbasis1;
• siteselectionwillbeinfluencedbywhetherthepatientisambulatory,
agitatedand/ordistressed;
• thechestorabdomenarepreferredsites2,specificallytheupper,
anteriorchestwallabovethebreast,awayfromtheaxilla.Ifthepatient
iscachectic,theabdomenisapreferredsite2;
• sitelongevitycanvaryfrom1–14days;manyvariablesinfluencesite
longevity,suchastypeofmedicationandtypeofcannulaused;
• factorsthatcausesitereactionsincludetonicityofthemedication,
solutionpH,infection,andprolongedpresenceofaforeignbody.3
29
Inappropriate site selection includes4
• lymphoedematousareas;
• areaswherethereisbrokenskin;
• skinsitesthathaverecentlybeenirradiated;
• sitesofinfection;
• bonyprominences;
• incloseproximitytoajoint;
• sitesoftumour;
• skinfolds;
• inflamedskinareas;
• whereverascitesorpittingoedemaarepresent;
• wherescarringispresent;
• areaswherelymphaticdrainagemaybecompromised1,forexamplein
womenwhohavehadamastectomy.
Site related problems
Remember,anysiteproblemswillcausethepatientdiscomfortandmayalso
interferewithdrugabsorptionandcompromiseeffectivesymptomcontrol.
Therefore,theselectionofanappropriatesiteforsubcutaneousinfusions
viaasyringedriverhasimplicationsforthepatient.
Siteproblemsmaybeassociatedwithinappropriatesiteselection,ordueto
siteirritation.
30
Factors contributing to site irritation/reactions include:
• thetonicity(concentration)ofthemedication;
• thepHofthesolution;
• infection;
• prolongedpresenceofaforeignbody3;
• somemedicationsincluding:
! cyclizine2,5
! levomepromazine
! methadone
! promethazine
! morphinetartrate
! ketamine4
Techniques that may be considered in consultation with the treating physician to minimise site irritation include:
• dilutingthemedicationsbyusingalargersyringesize2;
• usingnormalsaline(0.9%)ifapplicable,insteadofwaterforinjection2;
• adding1mgofdexamethasonetothesyringe6-oneAustraliantrial
foundthattheadditionof1mgofdexamethasonetosyringedrivers
cansignificantlyextendthelongevityofthesubcutaneousinfusionsite7;
• useofaTeflon®orVialon®cannula,e.g.theBDSaf-T-Intima,reduces
siteinflammation.2,8-10
31
Site Inspection
Meticuloussiteinspectionisintegraltoearlyidentificationandprevention
ofsiterelatedcomplications,andshouldbeperformedaspartofroutine
care.6,11,12Anysiteproblemscanpotentiallycausepatientdiscomfort.Theyalso
interferewithdrugabsorptionandcompromiseeffectivesymptomcontrol.
When inspecting the site, check for:
• tendernessorhardnessatthesite;
• presenceofahaematoma;
• leakageattheinsertionsite;
• swelling—asterileabscesscanoccurattheinsertionsite,causinglocal
tissueirritation12;
• erythema(redness);
• thepresenceofbloodinthetubing;
• displacementofthecannula.4
In addition to checking the site regularly (4 hourly is recommended), other important patient checks include:
• askingthepatienthowtheyfeel(orfamilymember/carer,ifthepatient
isunabletocomprehend):aretheirpainandothersymptomscontrolled?
• ensuringthattheinfusiondeviceisworkinge.g.
! ontheNikiT34theLEDlightflashesgreen;
! ontheGemStararrowsprogressacrossthescreen;
! ontheWalkMedLX350,squaresprogressacrossthescreenand
‘infusing’isseenonscreen;
32
! ontheGrasebythelightflashesgreenanda‘whirring’soundcanbe
heardasthedevicedeliverstheinfusion;
• checkingthevolumeremaininginthesyringe,andthatthedeviceis
runningtotime;
• ensuringtherearenoleakages,andthatconnectionstothesyringe
andcannulaarefirm.
Principles for site preparation and cannula insertion include:
• anaseptictechniquemustbeemployed,asmanypatientswhorequire
asubcutaneousinfusionareimmuno-compromised.Ensurehandsare
washedthoroughly12;
• inconsultationwiththepatientandfamily,selectasuitablesite12
usingtheprinciplesforappropriatesiteselection;
• selectandusesitesonarotatingbasis1;
• preparetheskinusinganantisepticwithresidualactivity,e.g.asolution
containing0.5%to2%chlorhexidinegluconatein>70%ethylor
isopropylalcohol13,andwaitforskintodry.NB:‘Thesolutionshould
beappliedvigorouslytoanareaofskinapproximately15cmindiameter,
inacircularmotionbeginninginthecentreoftheproposedsiteand
movingoutward,foratleast30seconds’13;
• thepointofthecannulashouldbeinsertedjustbeneaththe
epidermis.Forthinpeopletheangleofthecannulaoninsertionmay
needtobeless(30degrees)thanforapersonwithmore
subcutaneoustissue(45degrees).Adeeperinfusionmayprolongthe
lifeoftheinfusionsite.
33
To insert:
• grasptheskinfirmlytoelevatethesubcutaneoustissue.Insertthe
cannulaandreleasetheskin;
• removethestyletifusingaBDSaf-T-Intima®andtakecaretohold
thedeviceinsituwhenremovingthestyletsothattheentiredeviceis
notaccidentallyremovedfromthepatient.
Note:Ifametalcannulaisbeingused,placethebevelofthemetaldevicedownwardstodeliverthedrugsmoredeeplyintotheskin,andminimise
irritation.
• theextensiontubingischangedwhenthecannulaischanged;
• whenthetubingisplacedagainsttheskin,formalooptoprevent
dislodgementifthetubingisaccidentallypulled6.Useatransparent,
semi-occlusivedressingtocoverthesite,asthispermitsinspectionof
thesitebythecaregiver6,8;
• whererelevant,placethesyringeinthesyringedriver;
• recordanddocumentthattheinfusionhasbeencommenced,and
volumetobeinfused,asperlocaldrugadministrationpolicies.
Activity
Choosingthesite:WatchexcerptfromChapter2–‘WhoNeedsOne?’of
BrisbaneSouthPalliativeCareCollaborative’sGuideforClinicians–Howto
UseaSyringeDriverforPalliativeCarePatients.
Insertionofcannula:WatchexcerptfromChapter2–‘WhoNeedsOne?’of
BrisbaneSouthPalliativeCareCollaborative’sGuideforClinicians–Howto
UseaSyringeDriverforPalliativeCarePatients.
34
References
1. GomezY.Theuseofsyringedriversinpalliativecare.AustralianNursingJournal 2000;(2):suppl1-3.
2. DickmanA,LittlewoodC,VargaJ.Thesyringedriver:continuoussubcutaneous infusionsinpalliativecare.Oxford:OxfordUniversityPress;2002.
3. MorganS,EvansN.Asmallobservationalstudyofthelongevityofsyringedriversites inpalliativecare.InternationalJournalofPalliativeNursing2004;10(8):405-412.
4. DickmanA,SchneiderJ,VargaJ.Thesyringedriver:continuoussubcutaneous infusionsinpalliativecare.2nded.Oxford:OxfordUniversityPress;2005.
5. McNeillyP,PriceJ,McCloskeyS.Theuseofsyringedrivers:apaediatricperspective. InternationalJournalofPalliativeNursing2004;10(8):399-404.
6. MittenT.Subcutaneousdruginfusions:areviewofproblemsandsolutions. InternationalJournalofPalliativeNursing2001;7(2):75-85.
7. ReymondL,CharlesMA,BowmanJ,TrestonP.Theeffectofdexamethasoneonthe longevityofsyringedriversubcutaneoussitesinpalliativecarepatients.Medical JournalofAustralia2003;178:486-489.
8. PalliativeDrugs.com.‘Syringedrivers.’<www.palliativedrugs.com>.Accessed25 January2005.
9. AbbasS,YeldhamM,BellS.Theuseofmetalorplasticneedlesincontinuous subcutaneousinfusioninahospicesetting.AmericanJournalofHospiceand PalliativeMedicine2005;22(2):134-138.
10.RossJR,SaundersY,CochraneM,ZeppetellaG.Aprospective,within-patient comparisonbetweenmetalbutterflyneedlesandTefloncannulaeinsubcutaneous infusionofdrugstoterminallyillhospicepatients.PalliativeMedicine2002;16:13-16.
11.Coleridge-SmithE.TheuseofsyringedriversandHickmanlinesinthecommunity. BritishJournalofCommunityNursing1997;2(6):292,294,296.
12.RatcliffeN.Syringedrivers.CommunityNurse1997;3(6):25-26.
13.CHRISP(CentreforHealthcareRelatedInfectionSurveillanceandPrevention). Occupationalexposurestobloodandbodyfluids:Recommendedpracticesfor preventinghollow-boreneedlestickinjuries(Recommendation2:Wingedinfusion setsforsubcutaneousandintravenousinfusions).QueenslandGovernment (QueenslandHealth);2007.<http://www.health.qld.gov.au/chrisp/resources/ hollbore_rec_prac.pdf>.Accessed28June2010.
35
QUIZ: Section 3 - Selection, Preparation and Maintenance of the Site
ThisquizwilltesttheobjectivesandcontentinSection3oftheLearning
Packageandthe‘Guidelinesforsubcutaneousinfusiondevicemanagement
inpalliativecare’document.
Q1) YouarepreparingtoinsertacannulaforMrs.BettySmith,whorequires asubcutaneousinfusionviaasyringedriver.Whatisgenerallythe
preferredsiteforinsertionofthecannula?
UpperArm
Thigh
ChestorAbdomen
Backofthehand
Q2) YouarepreparingtoinsertacannulaforMrs.BettySmith,whorequires asubcutaneousinfusion.Ifshewascachectic,whatmaybethe
preferredsite?
Backofthehand
Abdomen
Thigh
UpperArm
Q3) IfMrs.Smithisdistressedoragitated,andthereisariskof
dislodgement,whichsitemightbeconsidered?
Scapula
Thigh
Abdomen
UpperArm
36
Q4) Eachofthefollowingisanimportantconsiderationinselectingan appropriatesiteEXCEPT:
Choosinganareawithagooddepthofsubcutaneoustissue
Avoidingoedematousareas
Selectingasitethatisclosetoajoint
Selectingasitethatiseasilyaccessible
Q5) Whichofthefollowingmayassistinminimisingsiteirritation? Ensuringthesyringedriverissafelysecuredtopreventdisconnection
Usingametalneedle
Dilutingthemedicationsbyusingalargersyringesize
Changingthecannulatoanothersite
Q6) KeyPrincipleswheninspectingtheinsertionsitewouldincludeallthe followingEXCEPT:
Ensuringthesyringedriverissafelysecuredtopreventdisconnection
Inspectingforrednessatthesite
Inspectingfortendernessorhardnessatthesite
Ensuringthepatientdoesn’tgetoutofbedwhenthesyringedriver
isoperational
37
Section 4: Drugs and Diluents
Learning Objectives
Atthecompletionofthissection,youshouldbeableto:
• describethemostcommonlyuseddrugsinsubcutaneousinfusions,
andtheirindicationsforuse;
• explainwhichdrugsarecontraindicatedinsubcutaneousinfusions;
• statethemostcommonlyuseddiluentinsubcutaneousinfusions.
Drug administration via a subcutaneous infusion device
• aprescriptionfromamedicalofficerorappropriatelycredentialled
nursepractitionerisrequiredbeforeadministeringanymedication;
• subcutaneousinfusiondevicescanbeusedtodeliverdrugstotreat
avarietyofsymptoms,particularlywhenotherdrugroutesareno
longeravailable,orareunacceptabletothepatient;common
symptomsincludepain,nausea,vomiting,breathlessness,agitation,
deliriumand“noisybreathing”1;
• awidevarietyofdrugscanbeusedtogetherindifferentcombinations
withnoclinicalevidenceoflossofefficacy2;
• themoredrugsthataremixedtogether,thegreatertheriskof
precipitationandreducedefficacy3;
• 2–3drugsmaybemixedinasubcutaneousinfusion(occasionallyup
to4drugs4,5);
• ifcompatibilityisanissue,theuseoftwosubcutaneousinfusion
devices3orregularorprnsubcutaneousinjectionsshouldbe
considered;
38
• beforemixinganydrugstogetherinasubcutaneousinfusion,checkfor
stabilityandcompatibilityinformation3,4,6-8e.g.withhospital
pharmacists;othersourcesincludeTheSyringeDriver1and
PalliativeDrugs.com12;
• useoftheboostfacility,whereavailable,isnotadvocated;aboost
doserarelyprovidessufficientanalgesiatorelieveuncontrolledpain,
andmayleadtooverdosingofotherdrugsbeinginfused4;
• itisbettertousebreakthroughmedicationtotreatuncontrolled
symptomsthantheboostfacility9;
• normalsalineisthemostcommonlyuseddiluentinAustralia10;
• theuseofwaterforinjectionhasbeenlinkedtopainduetoits
hypotonicity,althoughnormalsalinemaybemorelikelytocause
precipitation11;
• 5%dextroseisusedonlyoccasionallyasadiluent4,andisnot
commonlyusedinAustralia.12
In the Australian context, symptoms that are encountered at the end of life are generally well controlled by the use of nine commonly used medications.13 These include:
• morphinesulphate/tartrate(anopioid);
• hydromorphone(Dilaudid,anopioid);
• haloperidol(Serenace,anantipsychotic/antiemetic);
• midazolam(Hypnovel,ashortactingbenzodiazepine);
• metoclopramide(Maxolon,anantiemetic);
• hyoscinehydrobromide(hyoscine,anantimuscarinic/antiemetic);
• clonazepam(Rivotril,abenzodiazepine);
• hyoscinebutylbromide(Buscopan,anantimuscarinic);and
• fentanyl(anarcotic).
39
Temperaturemayaffectthestabilityofdrugs.Thiscanbeovercomeby
ensuringtheinfusiondeviceisplacedontopofbedclothesandoutsideof
clothing,ratherthanbeneaththem.4
Medications contraindicated for use via subcutaneous infusion due to severe localised reactions3,11:
• prochlorperazine(Stemetil,anantiemetic);
• diazepam(Valium,ananxiolytic);and
• chlorpromazine(Largactil,anantipsychotic)
Medications linked to abscess formation when used in subcutaneous infusions:
• pethidinehydrochloride(pethidine,ananalgesic);
• prochlorperazine(Stemetil,anantiemetic);and
• chlorpromazine(Largactil,anantipsychotic).1
Diluents
Thechoicebetweenwaterforinjectionand0.9%(normal)salineasadiluent
isamatterofdebate.Theliteratureisdividedwithsomerecommending
waterforinjectionasthediluent3,4,10,12,andrecentliteraturerecommending
normalsaline.1Normalsalinecanbeusedformostdrugs,themain
exceptionbeingcyclizine.4
NormalsalineismostcommonlyusedwithinAustraliafortworeasons1:
• firstly,themajorityofdrugscanbedilutedwithnormalsalinewithonly
40
twoexceptions:cyclizineanddiamorphine(neitherofwhichare
commonlyusedinAustralia);
• secondly,normalsalineisisotonic,asaremostinjectableformulations.
Bydilutingwithnormalsaline,thetonicityofthesolutionisunaltered.
Waterforinjectionishypotonic;usingitasadiluentwillpotentially
produceahypotonicsolution,whichtheliteraturesuggestscan
contributetothedevelopmentofsitereactions.1Forexample,theuse
ofwaterforinjectionhasbeenlinkedtopainduetoitshypotonicity,
althoughnormalsalineismorelikelytocauseprecipitation.11
References
1. DickmanA,SchneiderJ,VargaJ.Thesyringedriver:continuoussubcutaneous infusionsinpalliativecare.2nded.Oxford:OxfordUniversityPress;2005.
2. LichterI,HuntE.Drugcombinationsinsyringedrivers.TheNewZealandMedical Journal1995;108(1001):224-226.
3. MittenT.Subcutaneousdruginfusions:areviewofproblemsandsolutions. InternationalJournalofPalliativeNursing2001;7(2):75-85.
4. DickmanA,LittlewoodC,VargaJ.Thesyringedriver:continuoussubcutaneous infusionsinpalliativecare.Oxford:OxfordUniversityPress;2002.
5. McNeillyP,PriceJ,McCloskeyS.Theuseofsyringedrivers:apaediatricperspective. InternationalJournalofPalliativeNursing2004;10(8):399-404.
6. Coleridge-SmithE.TheuseofsyringedriversandHickmanlinesinthecommunity. BritishJournalofCommunityNursing1997;2(6):292,294,296.
7. NegroS,SalamaA,SanchezY,AzuaratM,BarciaE.Compatibilityandstabilityof tramadolanddexamethasoneinsolutionanditsuseinterminallyillpatients.Journal ofClinicalPharmacyandTherapeutics2007;32:441-444.
8. PetersonG,MillerK,GallowayJ,DunneP.Compatibilityandstabilityoffentanyl admixturesinpolypropylenesyringes.JournalofClinicalPharmacyandTherapeutics 1998;23:67-72.
9. Lloyd-WilliamsM,RashidA.Ananalysisofcallstoanout-of-hourspalliativecare adviceline.PublicHealth2003;117(2):125.
10.FlowersC,McLeodF.Diluentchoiceforsubcutaneousinfusion:asurveyofthe literatureandAustralianpractice.InternationalJournalofPalliativeNursing 2005;11(2):54-60.

41
11.BritishNationalFormulary.Syringedrivers.<www.bnf.org>.Accessed26January2005.
12.PalliativeDrugs.com.‘Syringedrivers.’<www.palliativedrugs.com>.Accessed25 January2005.
13.JointTherapeuticsCommission.Asurveyofdoctorsontheirpreferredmedicationsfor varioussymptomsinpalliativecare.Brisbane:Unpublisheddata;2005.
42
QUIZ: Section 4.1 - Drugs and Diluents
ThisquizwilltesttheobjectivesandcontentinSection4oftheLearning
Packageandthe’Guidelinesforsubcutaneousinfusiondevicemanagement
inpalliativecare’document.
Q1) Whichtwoofthefollowingdrugsarecontraindicatedforsubcutaneous infusions?
MorphineTartrate
Fentanyl
Chlorpromazine
Pethidine
Q2) Normalsalineisthemostcommonlyuseddiluentforsubcutaneous infusionsinAustralia.
True
False
Q3) ThegenericnameforDilaudidis: Serenace
Hypnovel
Durogesic
Hydromorphone
Q4) Thebrandnameforhaloperidolis: Maxolon
Durogesic
Buscopan
Serenace
43
Q5) Thebrandnameformidazolamis: Hypnovel
Metaclopramide
Serenace
Dilaudid
Q6) ThegenericnameforBuscopanis: Durogesic
HyoscineButylbromide
Hypnovel
HyoscineHydrobromide
Q7)ThegenericnameforMaxolonis: Morphine
Buscogesic
Metoclopramide
Hydromorphone
Q8) Whataretwoindicationsfortheuseofmorphinesulphate/tartratein subcutaneousinfusions?
Morphineiswellabsorbed
Itisoftenusedtodryterminalsecretions
Higherdosesmaycontrolagitationandconfusion
Itisanopioidforpaincontrol
Q9) Whataretwoindicationsfortheuseofhydromorphonein subcutaneousinfusions?
Itisanopioidforpaincontrol
Itmaybeusedwhenmorphineisnoteffective
Itisusedasanantiemetic
Itiseffectiveforcontrollinganxietyorterminalrestlessness

44
Q10)Whataretwoindicationsfortheuseofhaloperidolinsubcutaneous infusions?
Itisnotdirectlyanantiemetic,butdoesreducegastrointestinal
secretions
Itisanantipsychoticagentanddopamineantagonist
Itisanopioidforpaincontrol
Itmaybeusedinlowdosestocontrolnauseaandvomiting
Q11)Whataretwoindicationsfortheuseofmidazolaminsubcutaneous infusions?
Itisanantiemetic
Itisanarcotic
Itisashort-actingbenzodiazepine,usedtocontrolanxietyor
terminalagitation
Itisashort-actingbenzodiazepine,usedtocontrolseizures
Q12)Whataretwoindicationsfor/characteristicsoftheuseof metoclopramideinsubcutaneousinfusions?
Itisusefulinthetreatmentofnauseaandvomiting
Itmaybeusedwhenmorphineisnoteffective
Higherdosesmaycontrolagitationandconfusion
Itiscontraindicatedincompleteorsuspectedintestinal
obstruction
Q13)WhataretwoindicationsfortheuseofBuscopaninsubcutaneous infusions?
Itisanopioidforpaincontrol
ForthetreatmentofGITspasm
Higherdosesmaycontrolagitationandconfusion
Itreducesgastrointestinalsecretions
45
Q14)Whatwouldbeanindicationforusingfentanylinasubcutaneous infusion?
Itisoftenusedtodryterminalsecretions
Itisoftenusedtocontrolseizuresandanxiety
Itisanarcoticforseverepain
Itisusedasanantiemetic
QUIZ: Section 4.2 - Drugs and Diluents (Calculations)In the following 6 questions, calculate the volume for each of the break-through drugs ordered, using the strengths indicated.
Q15)(morphine10mgin1ml)morphine2.5mg=?ml
Q16)(morphine10mgin1ml)morphine25mg=?ml
Q17)(morphine120mgin1.5ml)morphine80mg=?ml
Q18)(midazolam5mgin1ml)midazolam2.5mg=?ml
Q19)(midazolam5mgin1ml)midazolam7.5mg=?ml
Q20)(haloperidol5mgin1ml)haloperidol1.5mg=?ml
In the next 4 questions you should calculate the volume required of each medication for the following subcutaneous infusion order over 24 hours: midazolam 10mg; morphine 15mg; metoclopramide 20mg. Note: the strength of available drug is shown in each question.
Q21)10mgofmidazolam(15mg/3ml)=?ml
Q22)15mgofmorphinesulphate(30mg/1ml)=?ml
Q23)20mgofmetoclopramide(10mg/2ml)=?ml
46
Q24)Whatisthetotalvolumeofthemedication?=?ml
For the next 4 questions, the subcutaneous infusion order has now changed: re-calculate using the following medication order.
Q25)25mgofmidazolam(15mg/3ml)=?ml
Q26)45mgofmorphinesulphate(30mg/1ml)=?ml
Q27)25mgofMaxolon(10mg/2ml)=?ml
Q28)Whatisthetotalvolumeofthemedication?=?ml
47
Section 5: Patient and Family/Carer Education
Carefulexplanationandeducationaboutwhatthedevicewilldo,its
advantagesandpossibledisadvantages,aswellasa24-hoursupport
number,isrequiredforpatientswithsubcutaneousinfusiondevicesand
theirfamilies.1Whenhealthprofessionalsprovideeducationtopatients
andfamily/carersitpromotessafetyandacceptanceoftheinfusiondevice
asameansofprovidingimprovedsymptomcontrol.2Good,welltimed
informationcanpreparethefamily/carerfortheroletheyaretakingon,
minimisingpotentialadverseconsequences.3
Learning Objectives
At the completion of this section, you should be able to:
• outlinethekeyelementsofpatient/familyeducationtopromotesafe
useofsubcutaneousinfusiondevicesbythepatient/family;
• describestrategiestosupportpatient/familydecisionmaking
regardingsymptommanagement.
Strategies for Providing Effective Education and Support
Thepatientandfamily/carershouldbegivenverbalandpracticalguidance
aboutlivingwithasubcutaneousinfusiondevice.Healthprofessionals
shouldbemindfulthatinformationandeducationgivenwhenthepatient
isunwellandthefamily/carerisanxiousmayneedtoberepeatedand
reinforced.
Explanation, demonstration and practice should be:
• simpleandfocusonneededmotorskillse.g.changingthebattery;
48
• repeatedasneeded;
• reassuringtothepatientandfamily/carerabouttheirabilitytomanage
thedevice.
Written information should:
• beclearandunderstandable;
• includeinformationaboutmanagementofcommonissueswiththe
deviceinuse;
• includewhattodoifthedevicealarms;
• includehowtocontactaknowledgeablehealthpractitionerout
ofhours.
Topics for Education
Information about the device
Subcutaneousinfusiondevicesareveryreliable.Itisimportantthatthe
patientandfamily/carerareinformedaboutindicatorsofnormaldevice
functioningsuchasa‘whirring’noise,asmallflashinglightorascreenwith
arrowsrunningacrossit.
Thepatientand/orfamily/carershouldbeencouragedtocheckthedevice
regularlytoensureitisfunctioningnormally,buttheyshouldalsobe
encouragednottoworryaboutcheckingitovernight.
Thepatientandfamily/carershouldbereassuredthatiftheybelieve
somethingiswrongwiththeinfusiondeviceorifthealarmsounds,itis
likelytobeaproblemthatiseasilyrectified.Forthesedevicesitisimportant
thepatientandfamily/carerareconfidentintheirabilitytomanagesimple
issuesthatmayariseinthenormalfunctioningofthedevice.
49
Daily Living
Thepatientandfamily/carershouldbeencouragedandguidedinwaysto
incorporatethesubcutaneousinfusiondeviceintotheireverydaylife.These
devicesaredesignedtomakethepatient’slifemorecomfortableandtobe
abletocontinuewithdailyroutines.
• thepatientmayshowerorbatheasnormal;
• instructionandclearwritteninformationregardingdisconnectionfrom
theinfusiondeviceforshowering,andreconnectionafterwards,
shouldbegivenbythehealthprofessional.Theperiodofdisconnection
shouldbeasbriefaspossible;
• patientsandfamily/carersshouldbegiveninformationaboutgeneral
careofthedevicetoallayfearsofdroppingordamagingthedevice4;
• thepatientshouldbeprovidedwithabagorencouragedtopurchasea
beltbagtoconcealandcarrytheinfusiondevice;
• alockedboxorperspexcovershouldbeprovidedaspatientsand
family/carershavereportedfeelingsofinsecurityandconcernabout
therobustnessofthedevice.
Medications
Patientsandfamily/carersshouldbeinformedtheremaybeachangein
thepatient’slevelofalertnessasaconsequenceofadministeringsome
medicationssubcutaneously.Theyshouldbereassuredthattheresponseis
generallytransitory,dependentonthegeneralconditionofthepatient,and
thedrugscanbetitratedappropriatelyifitremainsaproblemafterafewdays.
Thepatientandcarershouldbegivenclearinstructionsaboutmanagement
ofbreakthroughpainorothersymptomsandbereassuredabouttheuse
ofmedicationsonthoseoccasions.5Breakthroughmedicationisdefined
50
asextramedicationthatmayberequiredforsymptomsnotcontrolledby
medicationsprescribedforcontinuousdelivery.
Drug Storage and safety
Thepatientandfamily/carershouldbeadvisedaboutappropriatesafetyand
storagemeasuresformedicationsincludinginformationaboutthesupply
tobeheldinthehome,safestorageinalockedcupboardifappropriate,as
wellastemperatureandmoisturecontrol.
Carer Support
Educationandinformationconcerningtheprovisionofcareathomehas
beenrecognisedasemotionallybeneficialforfamily/carers6,reducingthe
riskofcareranxietyandstress.Thefamily/carermaydescribeadditional
concernsasthepatient’sconditionchangesandtheyarecalleduponto
makeproxydecisionsaboutsymptomsandbreakthroughmedications.
Thefamily/carershouldbeprovidedwithappropriateinformationabout
adjustmentstocareasthepatient’sconditionchangesandbereassured
abouttheircapabilitytomakeproxydecisionsandcontinueprovidingcare.
Equallytheyshouldbereassuredthatiftheycannolongercareforthe
patientwithasubcutaneousinfusiondevice,theywillbeassistedinseeking
outacarealternative.
Simpleinformationstrategiessuchaswrittenguidance,supervisedpractice
andprofessionalcontactwhenneededcandecreasethefamily/carer’s
anxiety,reducethechancesofforgettinginformation,andmaycontributeto
alowerincidenceofproblems.7Goodinformationwillassistthefamily/carer
tobeconfidentindecisionmaking,maintainthepatient’scomfortandhave
apositiveexperienceofcare.
51
Links
Section5of‘Guidelinesforsubcutaneousinfusiondevicemanagementin
palliativecare(RevisedEdition)’
Consumermedicineandsymptomguide,availablefrom:
http://www.healthnetworks.health.wa.gov.au/cancer/docs/Consumer_Book.pdf
(GovernmentofWesternAustralia,DepartmentofHealth.Palliativecare
medicineandsymptomguide.WACancerandPalliativeCareNetwork;2010.)
Activity
Reviewyourorganisation’swritteninstructions/guidelines/informationfor
patientsandfamily/carers.
References
1. PalliativeDrugs.com.SyringeDrivers.<www.palliativedrugs.com>.Accessed25January 2005.
2. MorganS,EvansN.Asmallobservationalstudyofthelongevityofsyringedriversites inpalliativecare.InternationalJournalofPalliativeNursing2004;10(8):405-412.
3. Yatesetal.2004inCruikshankS,AdamsonE,LoganJ,BrackenridgeK.Usingsyringe driversinpalliativecarewithinarural,communitysetting:capturingthewhole experience.InternationalJournalofPalliativeNursing2010;16(3):126-132.
4. FletcherC.ReportoncomparativeevaluationofGrasebysyringedriverreplacements. Auckland,NZ:NorthShoreHospiceTrust;2009.
5. Lloyd-WilliamsM,RashidA.Ananalysisofcallstoanout-of-hourspalliativecare adviceline.PublicHealth2003;117(2):125.
6. CentreforPalliativeCareResearchandEducation.Guidelinesforsubcutaneous infusiondevicemanagementinpalliativecare(RevisedEdition).Brisbane, Queensland:QueenslandHealth;2010.
7. DriscollA.Managingpostdischargecareathome:ananalysisofpatients’andtheir carer’sperceptionsofinformationreceivedduringtheirstayinhospital.Journalof AdvancedNursing2000;31(5):1165-1173.
52
Quiz: Section 5 – Patient and Family/Carer Education
ThisquizwilltesttheobjectivesandcontentinSection5oftheLearning
Packageandthe‘Guidelinesforsubcutaneousinfusiondevicemanagement
inpalliativecare’document.
Q1) Maintainingpersonalhygienewithasubcutaneousinfusiondevicecan beanissueforpatientsandfamily/carers.Whatadvicewouldyougive?
a.Don’tworry,patientscanhaveashowerbecausethedeviceis
waterproof
b.Theinfusioncanbedisconnectedforabriefamountoftimefor
showering
c. Patientswillneedtohavespongebathsaftertheinfusionis
commenced
Q2) Patientsandfamily/carersmaybecomeconcernedthatpainandother symptomsstillwon’tbecontrolledasthesamedrugshavebeentried
byotherroutes.Whatreassurancewouldyougive?
a.Ifthereisbreakthroughpainorothersymptomsthenextra
medicationcanbegiven
b.Allpainandsymptomswillbemanaged,therewillbenomore
problems
c. Ifthesubcutaneousinfusiondoesn’twork,nothingwill
Q3) Patientsmayhaveafeelingofsedationoroverwhelmingtiredness whenreceivingmedicationsviaasubcutaneousinfusion.Whatwould
youtellthem?
a.Thisisnormalandtheywilladjustinfewdaysafter
commencing/changingdoseintheinfusion
b.Sedationisasideeffectofthedrugs,nothingcanbedoneaboutit
c.Oncesymptomsarecontrolled,thedosecanbeadjustedifit
remainsaproblemforthem
d.Alloftheabove
53
Q4) Patientsandfamily/carersneedtotakeinalotofinformationwhena subcutaneousinfusiondeviceisbeingused.Whatkindofeducation
strategiescouldyouusetoensurethattheyareabletosafelymanage
thedevicewithconfidence?
a.Provideunderstandable,writtenguidelinesforthemtofollow
b.Explain,demonstrateandallowtimetopracticeanymotorskills
eg.changingthebattery
c. Provideinformationaboutoutofhourspointofcontactwitha
trainedhealthprofessional
d.Alloftheabove

54
Section 6: Patient Assessment and Troubleshooting
Thoroughassessmentisimportantwhencaringforpatientswitha
subcutaneousinfusionandshouldincludemonitoringofthepatient1
andthesubcutaneouscannulasite2,thedeviceandequipment3,and
compatibilityofdrugsbeingadministered.4,5
Whentroubleshootingequipmentusedinsubcutaneousinfusionsof
medicationviaapowerdrivendevice,itisimportanttounderstandthe
normalfunctioningofthedevice.6Theuseofonlyonetypeofdeviceineach
settinghasbeensuggestedtopreventconfusionwhichmayleadtoerrors.7
Learning Objectives
At the completion of this section, you should be able to:
• demonstrateanunderstandingofrelevantprinciplestoguide
assessmentofthepatienthavingasubcutaneousinfusion;
• describestrategiestodealwithcommonissuesthatarisewith
subcutaneousinfusionsandassociatedequipment.
Patient Assessment
Symptom assessment
Symptommanagementandcontrolisthekeyreasonforcommencinga
subcutaneousinfusionsoitisreaonablethatasignificantamountoftime
shouldbespentuponassessmentofthepatient’ssymptomsandefficacyof
theintervention.Assessmentshouldinclude:
• askingthepatienthowtheyfeelandtoratetheirsymptoms,orifthe
patientisnotabletorespondduetoconditionorcomprehension,ask
55
thecarerasanappropriateproxytorateobservablesignsof
symptoms;
• askingaboutpatternsofsymptomsexperienced,unrelievedorpoor
controlofsymptoms;
• observationforanddocumentationofsideeffectsofdrugsbeingused.
Useofavailable,validatedtoolstoassistintheassessmentofsymptoms
andconditionofpatientandfamily/carerisrecommended.Sometoolsin
commonusetoaidassessmentanddocumentationoffindingscanbefound
atthePalliativeCareOutcomesCollaborative(PCOC)website
http://chsd.uow.edu.au/pcoc/.8ServicesdonotneedtobeenrolledinPCOC
toaccessorusethetools.
Unrelieved symptoms
Breakthroughmedicationisdefinedasextramedicationthatmaybe
requiredforsymptomsnotcontrolledbymedicationsprescribedfor
continuousdelivery.9Administrationofbreakthroughdoseswillaidgood
painandsymptomcontrolandshouldbeusedwhen:
• asubcutaneousinfusioniscommencedasitmaytakeupto48hours
fordruglevelstoreachasteadystate;
• apatientcontinuestoreportunrelievedorpoorcontrolofpain/
symptoms;and
• deviceandsiterelatedproblemshavebeenexcluded.
Itisimportanttothesuccessfulcommencementofaninfusionthat
breakthroughmedicationisprovidedandusedasneededinthefirst48
hoursaftercommencement.Ifsymptomscontinuetobeunrelieveda
reviewofmedicationsbeinginfusedshouldbemade.Checktoensurethe
56
medicationisappropriate,thatanappropriatedosehasbeenprescribed
andthatthecorrectdosagehasbeenpreparedandisbeinginfused.
Adverse effects
Subcutaneousinfusiondeviceshavebeenusedtodelivermedications
traditionallyovera24hourperiodtoreducetheriskoferrorsinsettingup
theGraseby.7AlthoughtheGrasebyisnowbeingphasedout,evidenceon
microbiologicalstability,andphysicalandchemicalcompatibilitystillmost
commonlyrelatestoa24hourperiod.Itisforthisreasonthata24hour
infusionperiodisstillrecommended.9Tominimisetheriskofasignificant
siterelatedadverseevent,carefulinspectionofthesiteandprompt
responsetoanynotedchangeshouldformpartofgoodcare.
Adverseeventsrelatedtothedrugsbeinginfused,thoughrelatively
uncommon,shouldbenoted.Theinfusionshouldbestoppedand
followedbyobservationofthepatientandteamdiscussionaboutongoing
management.
Subcutaneous cannula site
Ideally,siteinspectionsshouldbeperformedatleast4hourly,notingsigns
ofinflammationandlocalsitereaction2andthenbedocumentedonthe
relevantorganisationalform.Forcommunityserviceswhenthisisnot
practical,considerpatientandfamily/carereducationregardingobservable
signsanddirectionsformanagementofchanges.
Inspectionofthesubcutaneouscannulasiteshouldbepartofroutinecare
andincludechecksfortendernessandpresenceofahaematomaatthe
cannulainsertionsite.1,4,6
57
Othersiteissuesmayinclude:
Inflammationofthecannulainsertionsite:
• couldbealocalisedskinreactionoraninflammatoryresponseata
previousareaofradiotherapy;
• thedrugsbeinginfusedshouldbereviewedtoconfirmtheyare
appropriateforsubcutaneousadministrationandthat;
• thedrug/drugsarenotataconcentrationthatmaycauseirritation.
Suggested solutions to manage site inflammation depend on the likely cause and may involve:
• removalandresitingofthesubcutaneouscannula;
• increasingthediluentinthedevicereservoirtoreducethedrug
concentration;
• additionofdexamethasonetothereservoirtoreducelocalisedsite
irritation;
• observationandmanagementofconsequencesthatmayinclude
infection.9
Painatthecannulainsertionsitecouldbedueto:
• inflammationforoneofthereasonsdiscussedabove;
• shallowcannulainsertionwhichmayalsobeacauseoflocalised
inflammation.
Painattheinsertionsiterequiresremovalandresitingofthesubcutaneous
cannula.
58
Leakageofinfusionfluidatthecannulainsertionsiteindicates:
• anunstablecannulaposition;
• allconnectionsshouldbecheckedtoensuretheyaresecure;
• changecomponentsasneeded;
• thecannulamayneedtoberemovedandresited.
Leakageoffluidwillcontributetounrelievedpain/symptoms.
Bleedingatthecannulainsertionsite:
• maybecausedbytraumaoracoagulationproblem;
• requiresremovalandresitingofthecannula.
Pressureshouldbeappliedtotheoldsitewhichshouldbeobservedfor
furtherbleeding.
Limited cannula accesspoints:
• maybeduetooedema,infectionorcachexia;
• requireconsiderationanddiscussionwithcolleaguestoconfirm
appropriatenessofsubcutaneousmedicationinfusion;
• indicateneedtoconsiderappropriatesiteselection(Section3ofthis
package).
If the patient is restless,showingsignsofdelirium,confusionorimpairedcognition:
• potentialunderlyingcausesshouldbeinvestigatedandtreated;
• thepossibilityofterminalrestlessnessshouldbeconsidered;
59
• causesofagitationlikepain,fullbladderorbowelshouldbechecked
andmanagedappropriately;
• sitingofthecannulaaroundthescapulashouldbeconsideredto
minimiseriskofdislodgement;
• abreakthroughdoseofanantipsychoticsuchashaloperidol,
risperidoneorolanzapinecanalsobeconsidered.10
Documentation
Symptomcontrolandefficacyofintervention/infusionshouldbenotedon
theappropriateformsofyourservice.Itissuggesteddocumentationshould
include:
• notationsreferringtotimes;
• volumesloaded;
• patientresponse;
• anyadverseincidentsorevents;
• thecapacityforthepatientandfamilytocontinuemanagementofthe
infusiondevice.
Family/Carer
Thecapabilityofthefamily/carertoparticipateincareofthepatientwitha
subcutaneousinfusiondeviceshouldbecheckedbeforecommencement
oftheinfusionandassessedregularlyafterthat.Thestatusofthecarer
–employment,physicalandemotionalhealth–shouldbeconsideredas
potentiallyimpactingontheoutcomeoftheintervention.
60
Device
Itisimportantthatyouunderstandthenormalfunctioningofthedevice
beingusedinyourservicearea.6Thesmallflashinglightonthefrontofthe
NikiT34andtheGraseby,theintermittent‘whirring’soundoftheGraseby
andthearrowsrunningconstantlyacrossthescreenoftheGemStarall
indicatethedeviceisfunctioningnormally.
Priming the line
Ensurethatorganisationalprotocolregardingprimingoftheextension
tubing/devicelineisfollowedwhensettingupasubcutaneousinfusion(see
section1ofthispackage).
Alarms
Eachdevicehasdifferentsettingsfortriggeringitsalarms.Analarmwillsoundif:
• theinfusionreservoir(syringeorcassette)isempty;
• thebatteryorpowersourceisexhaustedrequiringbatterychangeor
placementinachargingcradle;
• tubingiskinked,thecassetteisunseatedorthesyringeisjammed;
• airisdetectedintheGemStarlineorcassette(correctionwillrequire
clearingtheairfromthelineandre-priming).
Thedeviceshouldbemonitoredforashorttimeaftercorrectiontoconfirm
normalfunctioning.
61
Battery/Power
Batterylifeisvariable.Toreducethepotentialforaslowedorstopped
infusion,batteriesshouldbecheckedregularlytoensuretheyarenot
exhausted.Ifthedeviceusedbyyourserviceusesachargingcradle,ensure
itispluggedintomainspower,thatthedevicesitseasilyandproperlyinto
thecharger,andtheindicatorlightconfirmingitisonmainspower‘flicks’on.
Delivery of Medication
Inspectionofthevolumeremaining7ideallyshouldbeatleast4hourlywith
findingsdocumentedontherelevantorganisationalform.Whenthisisnot
practical,considerpatientandfamily/carereducationregardingobservation
ofinfusionvolumeandmanagementoffindings.
Aswithanymedication,thedeliveryoftherightdrugattherighttimeis
essential.
Regular assessment is required to identify any of the following concerns:
Infusion has not run to time
Careshouldbetakenatsetuporrefillingthatcorrectmeasures(syringe
andcassettevolume)andrateofinfusionareused.Iftheinfusiondoesnot
end‘ontime’orwithinacceptedparameters,eitherearlyorlatefinish,basic
checksshouldbemadeensuringthat:
• theratehasbeensetcorrectlyandnotbeenaltered;
• thesyringelengthandvolumetobeinfusedhasbeenmeasured
correctly;
• thesyringeorcassettereservoirisloadedproperlyintothedevice;
• therearenoimpedimentstothetubing/linee.g.kinks,orclampslefton;
62
• thedevicehasnotsustainedanywaterdamage;
• thedevicehasnotbeenpurposefullystopped;
• thedevicebatteryhaspowerandisnotflatwhichcouldcausethe
infusiontobeslowedorstopped6;
• the‘boostbutton’hasnotbeenactivated;
• estimatedandprescribedbreakthroughdoseshavenotbeen
exceededortheGemStar.
ForissueswiththeGemStarrepeatedlyfinishingearlyduetomorethan
expectedbreakthroughdoses,theprescriptioncanbealteredtoprovide
highervolumeforinfusionwhilemaintainingthesamedrugconcentration.
Infusion has stopped
Themostlikelyreasonfortheinfusiontostopisthatthereisnoremaining
fluidtobeinfusedandreloadingaccordingtothemedicalprescriptionis
required.Iffluidforinfusionremainsthencheckthat:
• thedevicebatteryisnotflatcausingtheinfusiontostop6;
• neitherthelinenorcannulaareblocked;
• thedrugsintheinfusionmixturehavenotprecipitated(crystallised)
blockingthetubing;
• thereisnomechanicalmalfunctioncausingfailureoftheinfusion.
Tubing
Carefulinspectionoftubingforpatency6shouldideallybedoneatleast4
hourlynotingtwists,kinks,signsofprecipitationandsecureconnections.
Findingsshouldbedocumentedontheappropriateformforyourservice.
63
Tampering
Ifitissuspectedthattherehasbeenpurposefultamperingwiththedevice
settingsorundirecteduseofthe‘boost’facility,atamperproof‘lockbox’7or
lockingofthedevice’skeypadshouldbeconsideredtomaintaininfusion/
drugsecurity.
Drugs
Calculations
Whenasubcutaneousinfusionviaadeviceisbeingsetuporreloaded,
alldrugcalculationsshouldbecheckedaccordingtolocallegislative
requirements,organisationalpolicyandprotocol.
Drug Choice and Dosage
Thereareanumberofdrugssuitableandcommonlyprescribedfor
subcutaneousinfusioninpalliativecaresettings(Section4).Prescriptions
shouldbecheckedtoensurethat:
• drugstobeinfusedareappropriateforsubcutaneousadministration;
• thedrugisnotataconcentrationthatmaycauselocalisedirritationat
thecannulainsertionsite;
• thedrugwillprovidecomfortforthepatient.
Compatibility
Whenadrugistobeinfused,orifmorethanonedrugistobeinfusedin
combination,itisimportanttocheckthecompatibilityofthedrug/drugsand
thediluenttobeused5,7topreventproblemswith:
64
• precipitation/crystallisationintubingorthesyringewhichwould
requirethesyringeorcassetteandtubingtobediscardedandinfusion
setupcommencedagain;
• skinirritationfromknowndrugirritantswhichwouldrequirechangeof
cannulainsertionsite,butcouldbeavoidedbyusingalargervolume
ofdiluent.7
Links
Section6of‘GuidelinesforSyringeDriverManagementinPalliativeCare’
Activity
Identifythetoolscurrentlyusedinyourservice/organisationforassessment
ofpeoplereceivingpalliativecare.
References
1. RatcliffeN.Syringedrivers.CommunityNurse1997;3(6):25-26.
2. ReymondE,CharlesM.Aninterventiontodecreasemedicationerrorsinpalliative patientsrequiringsubcutaneousinfusions:BrisbaneSouthPalliativeCareService andAdverseDrugEventPreventionProgram;unpublishedreportpresentedtoClinical ServicesEvaluationUnit;PrincessAlexandraHospital.Brisbane,Queensland;2005
3. PalliativeDrugs.com.SyringeDrivers.<www.palliativedrugs.com>.Accessed25January 2005.
4. Coleridge-SmithE.TheuseofsyringedriversandHickmanlinesinthecommunity. BritishJournalofCommunityNursing1997;2(6):292,294,296.
5. PalliativeCareMatters.<www.pallcareinfo>.Accessed10August2010
6. MittenT.Subcutaneousdruginfusions:areviewofproblemsandsolutions. InternationalJournalofPalliativeNursing2001;7(2):75-85.
7. DickmanA,LittlewoodC,VargaJ.Thesyringedriver:continuoussubcutaneous infusionsinpalliativecare.Oxford:OxfordUniversityPress;2002.
65
8. PalliativeCareOutcomesCollaborative<http://chsd.uow.edu.au/pcoc/>.Accessed13 August2010.
9. CentreforPalliativeCareResearchandEducation.Guidelinesforsubcutaneous infusiondevicemanagementinpalliativecare(RevisedEdition).Brisbane, Queensland:QueenslandHealth;2010.
10.PalliativeCareExpertGroup.Therapeuticguidelines:palliativecare.Version3. Melbourne:TherapeuticGuidelinesLtd;2010,p.292.
11.DriscollA.Managingpostdischargecareathome:ananalysisofpatients’andtheir carer’sperceptionsofinformationreceivedduringtheirstayinhospital.Journalof AdvancedNursing2000;31(5):1165-1173.
66
Quiz: Section 6 - Patient Assessment and Troubleshooting
ThisquizwilltesttheobjectivesandcontentinSection6oftheLearning
Packageandthe‘Guidelinesforsubcutaneousinfusiondevicemanagement
inpalliativecare’document.
Q1) YourpatientMrsSmithhasasubcutaneousinfusiondeviceinsitu.Her symptomshavebeenwellcontrolledhowever,sheisnowcomplaining
ofanexacerbationofhersymptoms.Possiblereasonsmayinclude:
a.Devicemalfunction
b.Medicationrequiresreview
c.MrsSmith’sconditionischangingordeteriorating
d.Alloftheabove
Q2) MrsSmith’sinfusionisnotrunning‘ontime’.Whatkeyareasshould beassessed?
a.Correctvolume(moreorlessthanrequired)addedtoreservoirat
preparation
b.Failuretoaccountforinfusionvolumerequiredtoprimethe
tubing
c. Infusiondevicesetatcorrectrate
d.Alloftheabove
Q3) Whichtwoofthefollowinginfusionsitecharacteristicswouldindicate problems?
a.Pinkskin
b.Tenderness/redness
c. Swelling/hardness
d.Absenceoftenderness
Q4) Regularassessmentofapatientwithasubcutaneousinfusionshould include:
a.Effectivenessofsymptommanagement
b.Siteinspection/assessment
c. Checkingpatencyoftubingandsyringevolumeremaining
d.Alloftheabove
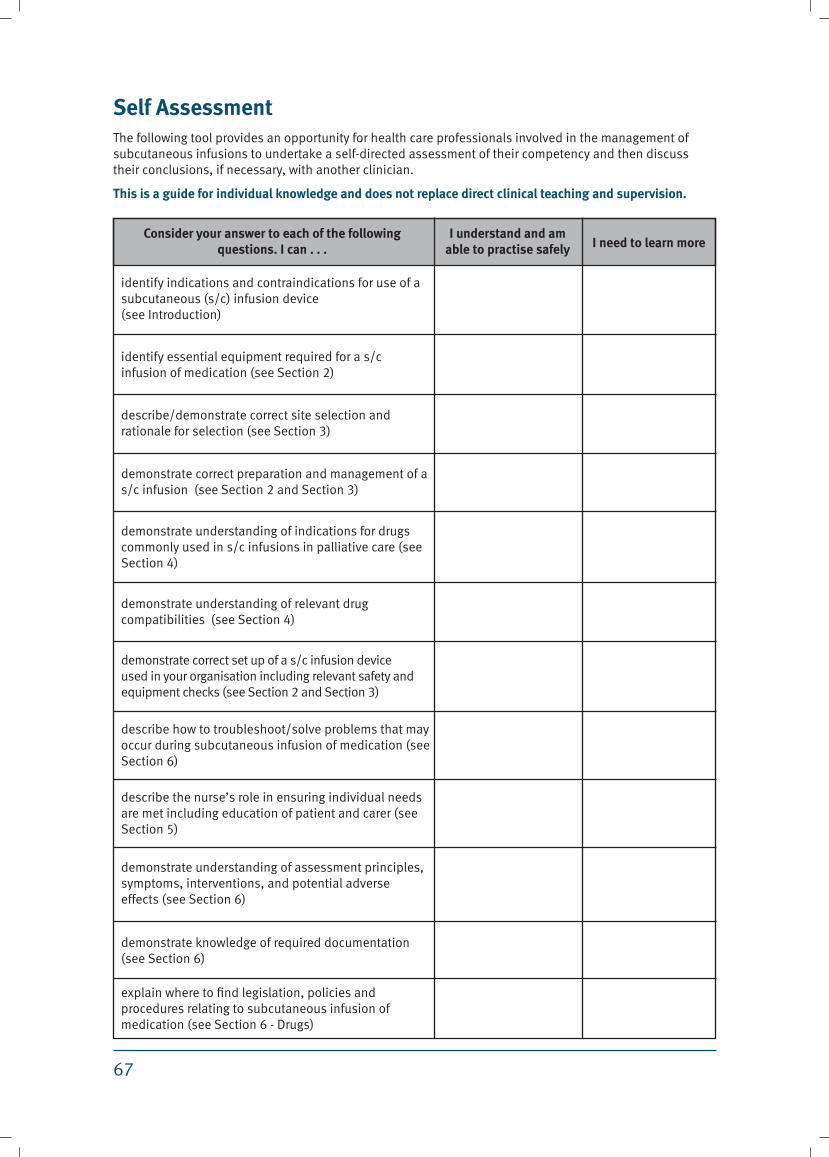
67
Self AssessmentThefollowingtoolprovidesanopportunityforhealthcareprofessionalsinvolvedinthemanagementofsubcutaneousinfusionstoundertakeaself-directedassessmentoftheircompetencyandthendiscusstheirconclusions,ifnecessary,withanotherclinician.
This is a guide for individual knowledge and does not replace direct clinical teaching and supervision.
Consider your answer to each of the following questions. I can . . .
I understand and am able to practise safely I need to learn more
identifyindicationsandcontraindicationsforuseofasubcutaneous(s/c)infusiondevice(seeIntroduction)
identifyessentialequipmentrequiredforas/cinfusionofmedication(seeSection2)
describe/demonstratecorrectsiteselectionandrationaleforselection(seeSection3)
demonstratecorrectpreparationandmanagementofas/cinfusion(seeSection2andSection3)
demonstrateunderstandingofindicationsfordrugscommonlyusedins/cinfusionsinpalliativecare(seeSection4)
demonstrateunderstandingofrelevantdrugcompatibilities(seeSection4)
demonstratecorrectsetupofas/cinfusiondeviceusedinyourorganisationincludingrelevantsafetyandequipmentchecks(seeSection2andSection3)
describehowtotroubleshoot/solveproblemsthatmayoccurduringsubcutaneousinfusionofmedication(seeSection6)
describethenurse’sroleinensuringindividualneedsaremetincludingeducationofpatientandcarer(seeSection5)
demonstrateunderstandingofassessmentprinciples,symptoms,interventions,andpotentialadverseeffects(seeSection6)
demonstrateknowledgeofrequireddocumentation(seeSection6)
explainwheretofindlegislation,policiesandproceduresrelatingtosubcutaneousinfusionofmedication(seeSection6-Drugs)
68
Conclusion
Theuseofsubcutaneousinfusiondeviceshasbecomestandardand
commonpracticeinpalliativecare.Theiruseenhancespatientcomfort
byadministrationofmedicationsataconstantratetoassistinsuccessful
controlofvarioussymptoms.
Appropriateuseofasubcutaneousinfusiondeviceallowspatientsand
familiesthechoiceofcareathomebyfamilyandfriendswiththesupport
oftheirGeneralPractitioner,visitingnurses,andthelocalspecialist
palliativecareteamasrequired.Itallowseffectivesymptommanagement
withreductionofinterventionssuchasrepeatedinjections.However
healthcareprofessionalsshouldconsiderthatpatientandfamily/carer
knowledgeandunderstandingofasubcutaneousinfusiondevicemaybe
limited,contributingtopossiblenegativeperceptionsofsuchdevices.
Comprehensiveeducationaboutsubcutaneousinfusiondevicesby
healthprofessionalsinvolvedinthecareofthesepatientsandfamilies
mayimprovetheirknowledgeandunderstanding,andreducenegative
perceptions.
Aswithallmedicaldevicestherearesomelimitationsandtheiruseisnot
withoutrisksincludingtechnicalproblems,medicationincompatibilities,
andskinreactionsatthesiteofcannulainsertion.Subcutaneousinfusion
devicesshouldbemanagedbyknowledgable,appropriatelytrainedstaff
tominimisetheriskspresentedbythelimitationsofindividualdevicesand
theiruse.
Completionofallsectionsofthislearningpackageprovidesbaseline
informationforbestpracticeuseofsubcutaneousinfusiondevicesin
palliativecare,allowingforcompetencydevelopmentandmaintenance.
Completionoftheselfassessmentincludingdiscussionwithaknowledgable
healthprofessionalisrecommended.
69
Quiz Answers
Section 1 - The Patient and Family/Carer Experience
Q1) Alloftheabove
Q2) Poorprognosis
Q3) False
Q4) False
Q5) True
Section 2 - Equipment Guidelines and Principles
Q1) False
Q2) True
Q3) False
Q4) False
Q5) True
Q6) True
Section 3 - Selection, Preparation and Maintenance of the Site
Q1) Chestorabdomen
Q2) Abdomen
Q3) Scapula
Q4) Selectingasitethatisclosetoajoint
Q5) Dilutingthemedicationsbyusingalargersyringe
Q6) Ensuringthepatientdoesn’tgetoutofbedwhentheinfusiondeviceisoperational
Section 4.1 - Drugs and Diluents
Q1) 3and4-chlorpromazineandpethidine
Q2) True
Q3) hydromorphone
Q4) Serenace
Q5) Hypnovel
Q6) hyoscinebutylbromide
Q7) metoclopramide
Q8) 1and4–morphineiswell-absorbedanditisanopioidforpaincontrol.
70
Q9) 1and2–itisanopioidforpaincontrolanditmaybeusedwhenmorphineisnot
effective
Q10) 2and4–itisanantipsychoticagentanddopamineantagonistanditmaybe
usedinlowdosestocontrolnauseaandvomiting.
Q11) 3and4–itisashort-actingbenzodiazepine,usedtocontrolanxietyorterminal
agitationanditisashort-actingbenzodiazepine,usedtocontrolseizures.
Q12) 1and4–itisusefulinthetreatmentofnauseaandvomitinganditis
contraindicatedincompleteorsuspectedintestinalobstruction
Q13) 2and4–forthetreatmentofGITspasmanditreducesgastrointestinalsecretions
Q14) 3–itisanarcoticforseverepain
Section 4.2 - Drugs and Diluents
Q15) 0.25ml
Q16) 2.5ml
Q17) 1ml
Q18) 0.5ml
Q19) 1.5ml
Q20) 0.3ml
Q21) 2ml
Q22) 0.5ml
Q23) 4ml
Q24) 6.5ml
Section 5 - Patient and Family/Carer Education
Q1) b–theinfusioncanbedisconnectedforabriefamountoftimeforshowering
Q2) a–ifthereisbreakthroughpainorothersymptomsthenextramedicationcanbe
givenforthis
Q3) d–Alloftheabove
Q4) d–Alloftheabove
Section 6 - Patient Assessment and Troubleshooting
Q1) d–Alloftheabove
Q2) d–Alloftheabove
Q3) bandc–tendernessandrednessandswelling/hardness
Q4) d–Alloftheabove
71
Patient and Family/Carer Statements
‘Ifeltfine,[abouthavingthes/cinfusion]Ifeltquitegoodaboutitbecause
Ithoughtratherthangettinganinjection–becauseIwasgettingoneevery
night–Ithoughtwellthat’sfinebecauseit’sover24hours,it’sboundto
helpratherthantakingtabletsandstillbeingsick.’(Patient)
‘Oncehegotthe[s/cinfusion]hestoppedbeingsick,soitwasgrand.Life
waseasierforhimandforme.’(Carer)
‘Soifhehadn’thadthe[s/cinfusion],hemaybewouldn’thavebeenableto
stayathome.’(Carer)
‘Ireallydidn’twantit.Ithoughttheonlytimetheyhookyouuptothings
likethiswaswhenyourtimewasup.Mydoctortalkedtomeforalongtime
aboutwhyIneedit–butIstilldon’tliketheideaofneedingapumpjustto
getthroughtheday.’(Patient)
‘Itmeansthatwedon’tleavethehousemuchnow.Thenurseskeeptelling
methatwecangooutbutwhatifsomethinghappens...thebatterywent
flattheotherday–whatifwehadbeensomewhereandcouldn’tgetit
changed.It’stoomuchofaworrysowestayhome.’(Carer)















![CARE PATHWAY GUIDE - has-sante.fr · SC Subcutaneous SFAP ... [Home nursing care service] PCU Palliative care unit WTHD Wish to hasten death. ... CARE PATHWAY GUIDE](https://static.fdocuments.in/doc/165x107/5ce0af6188c99337398b6481/care-pathway-guide-has-santefr-sc-subcutaneous-sfap-home-nursing-care.jpg)


