Management of respiratory emergencies
74
MANAGEMENT OF RESPIRATORY EMERGENCIES Dr. SUJAY PATIL
-
Upload
dr-sujay-patil -
Category
Health & Medicine
-
view
471 -
download
0
Transcript of Management of respiratory emergencies
MANAGEMENT OF RESPIRATORY EMERGENCIES
Dr. SUJAY PATIL
DefinitionRespiratory emergencies are medical emergencies characterized by difficulty in breathing or inability to breathe.
In such emergencies :
Patient take frequent shallow/irregular or slow breaths
Immediate medical help/hospitalization required
Patient is extremely agitated
Can be fatal, if not treated
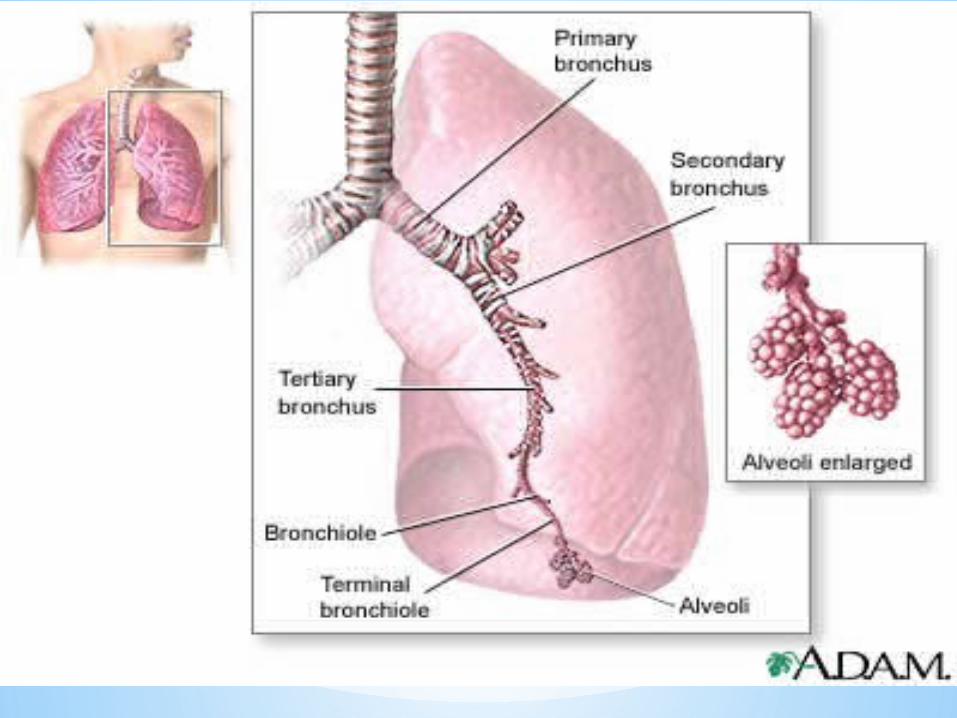
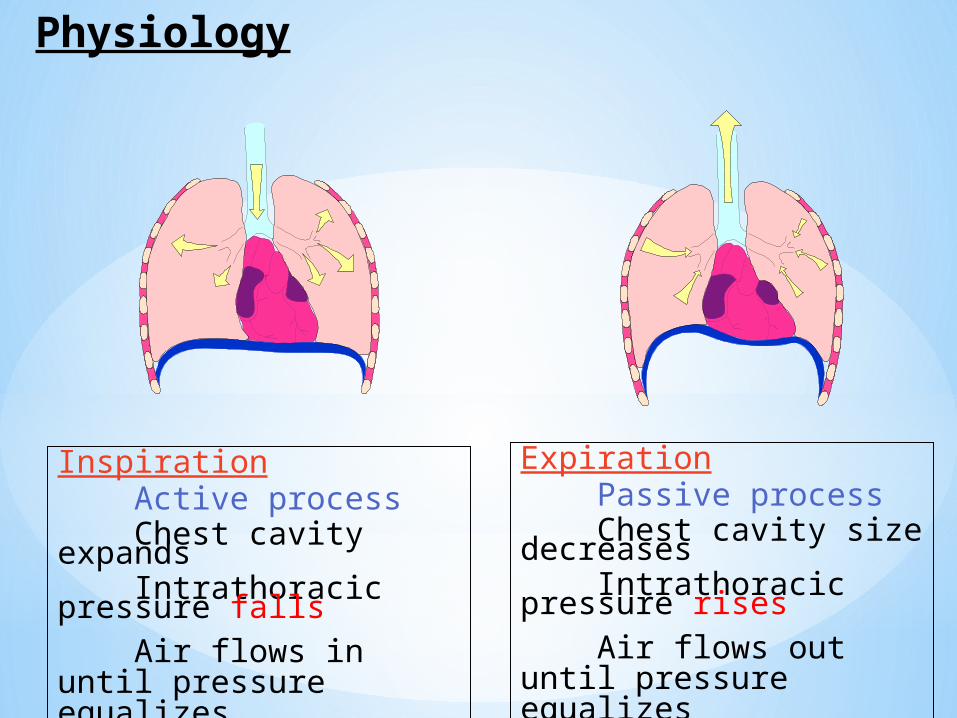
Physiology
Inspiration Active process Chest cavity expands Intrathoracic pressure falls Air flows in until pressure
equalizes
Expiration Passive process Chest cavity size decreases Intrathoracic pressure rises Air flows out until pressure
equalizes
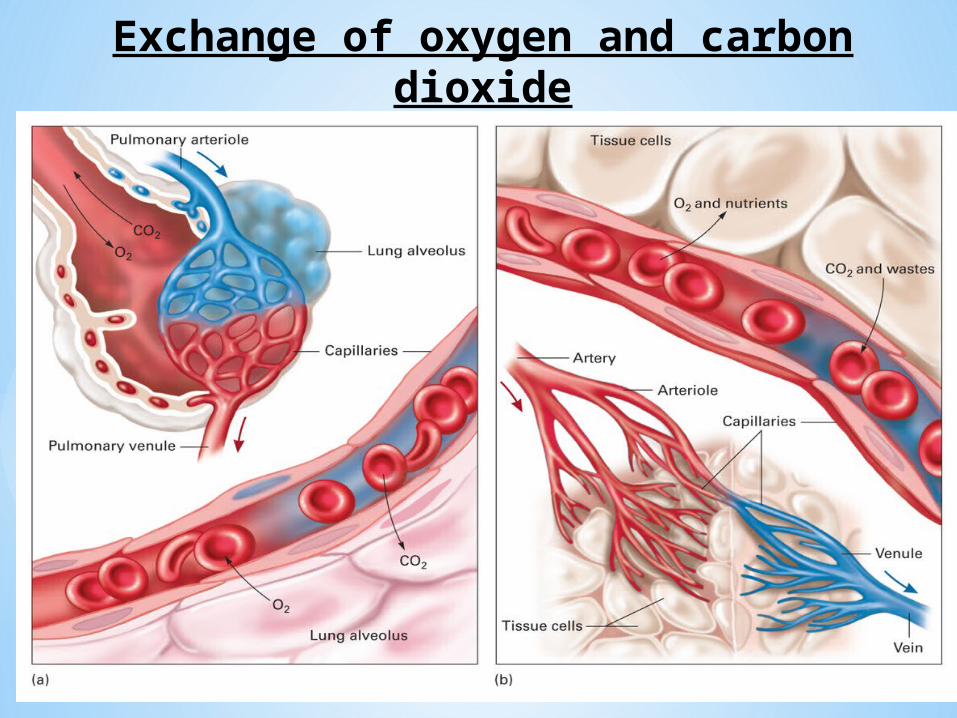
Exchange of oxygen and carbon dioxide
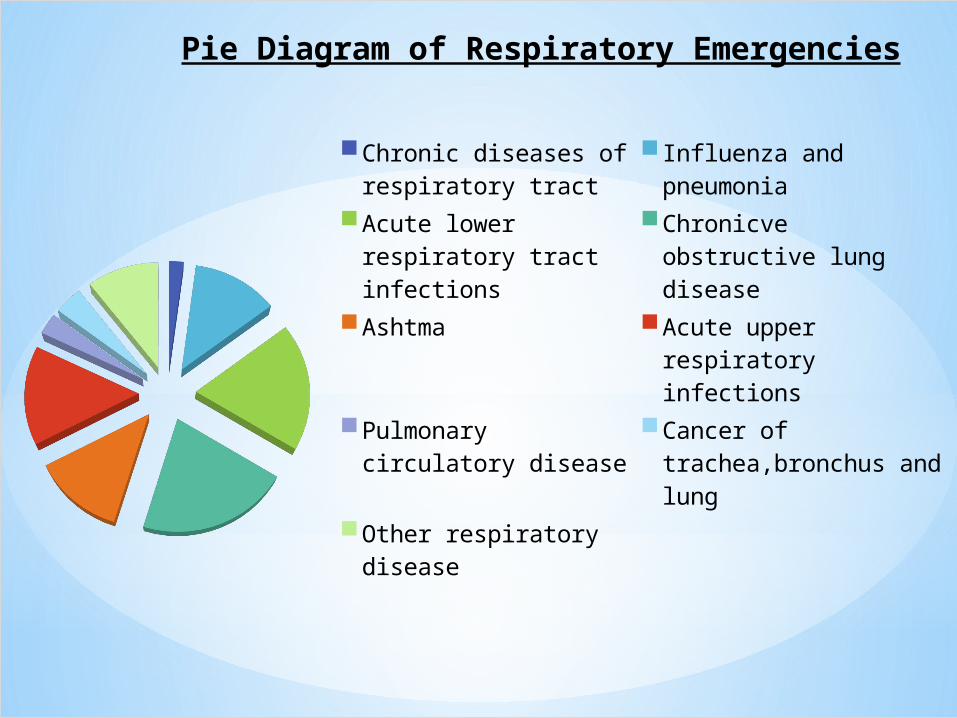
Pie Diagram of Respiratory Emergencies
Chronic diseases of respiratory tract
Influenza and pneu-monia
Acute lower respiratory tract infections
Chronicve obstructive lung disease
Ashtma Acute upper respiratory infections
Pulmonary circulatory disease
Cancer of trachea,bronchus and lung
Other respiratory disease
Failure of:Ventilation: air in/ air outDiffusion: movement of gasesPerfusion: movement of blood
Relieved by: epinephrine based medications (such as Beta 2 agonist– albuterol, terbutaline)
Compounded by:Inflammation/mucus production
Causes of Respiratory Emergencies
Assessment of Respiratory Emergency
A. Primary(Initial) Assessment
to identify immediate threats to patients life.
Patients of any age who are talking or crying have a patent airway while presence of snoring or gurgling may indicate potential problems with airway.
Patient who speak only 2-3 words & pause to take breath show sign of respiratory distress.
Use of accessory muscles of respiration is also sign of respiratory distress.
Altered mental status/asymmetrical movement of chest suggest respiratory problems.
B. Secondary(Detailed) Assessment History about recent trauma, food intake & drinking.
Determine whether problem slow or rapid
Ask about allergies and anaphylaxis
Physical Examination Inspect patient to note any signs of trauma. Assess skin color as indicator of oxygen status Note any decrease or increase in respiratory rate Look for use of accessory muscles of respiration, intercostal
retractions, nasal flaring and grunting(in children) indicate respiratory distress
Auscultate patient to listen any harsh sounds and air movement in lungs.
Palpate lung area for movement of air over lungs with the back of your hand.
Various Respiratory Emergencies are :-1) Status Asthmaticus
2) Acute exacerbation of COPD
3) Acute Respiratory Distress Syndrome (ARDS)
4) Acute Pulmonary Edema
5) Acute Pulmonary Embolism
6) Pulmonary Hypertension in Newborn and Adults
7) Acute Mountain Sickness (AMS) 10) Tension Pneumothorax
8) Decompression Syndrome 11) Respiratory Acidosis
9) Acute Respiratory Failure 12) Aspiration Pneumonia
Status Asthmaticus (Severe Acute Asthma):
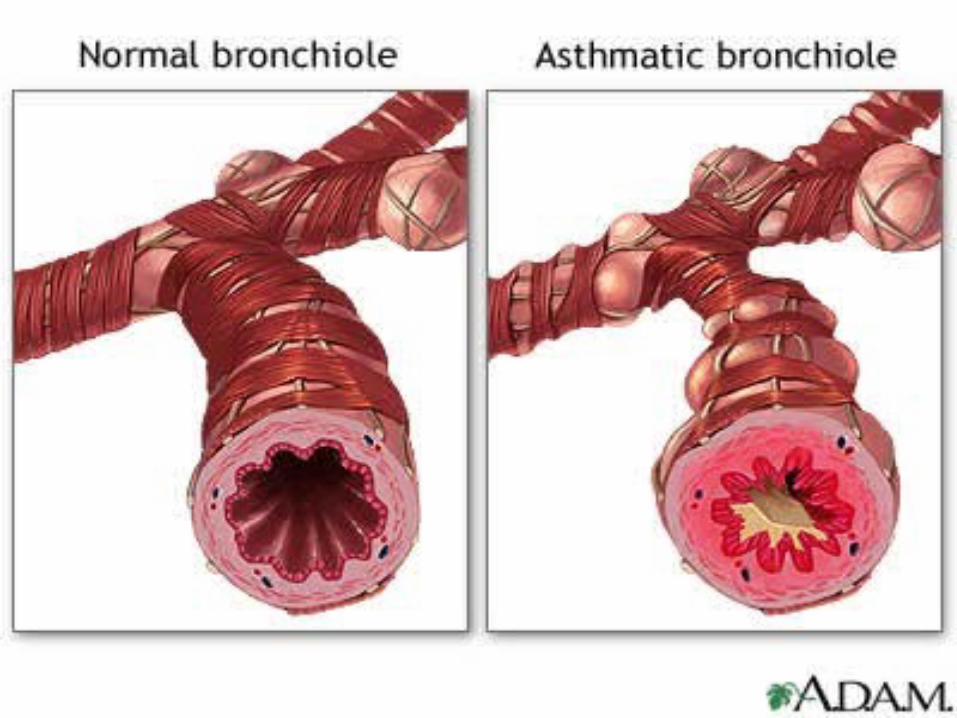
Asthma is characterized by paroxysmal and reversible obstruction of the airways.
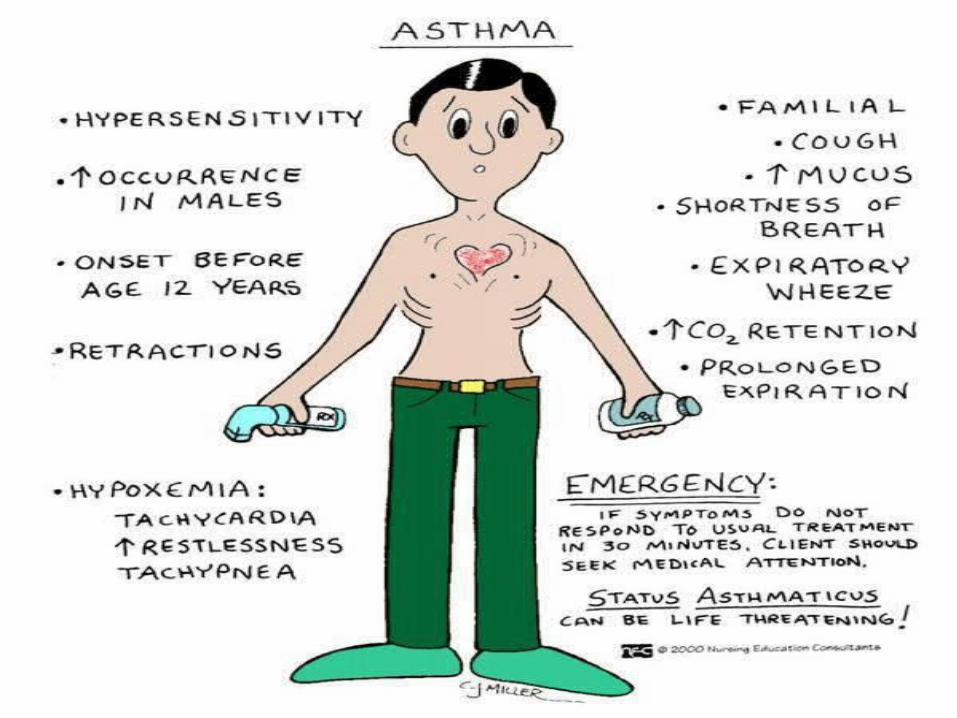
Status asthmaticus is severe, prolonged asthma exacerbation not responding to usual doses of inhaled bronchodilators & associated with symptoms of potential respiratory failure.
Sudden onset(resulting from spasm of airways) or may be more insidious.
Precipitated by viral respiratory infection / prolonged exposure to allergen.
Requires early recognition and immediate treatment, if not danger of respiratory failure.
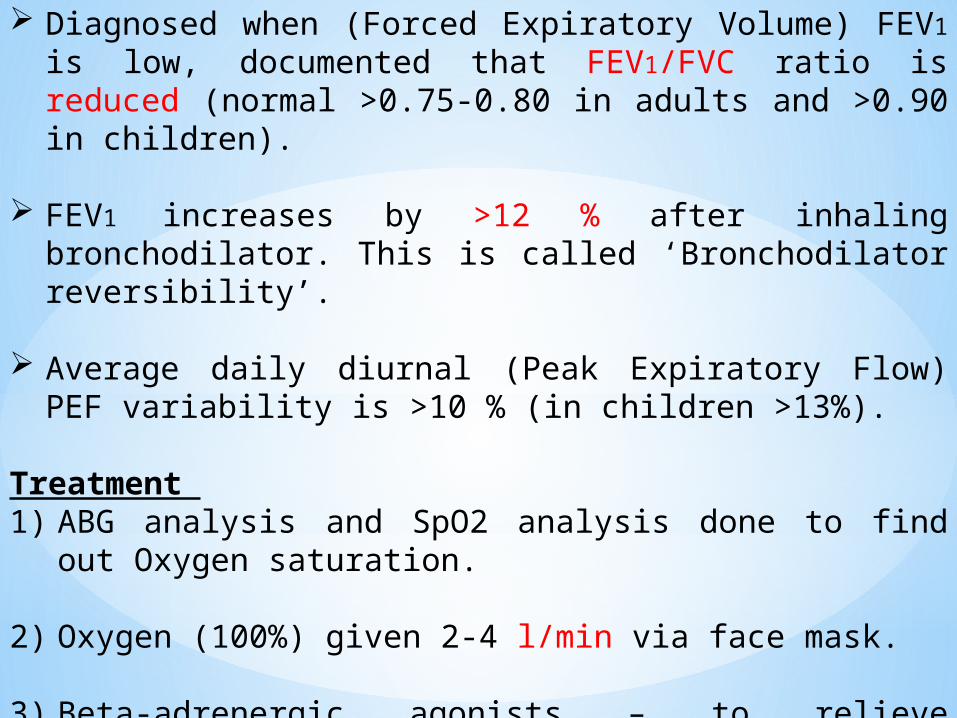
Diagnosed when (Forced Expiratory Volume) FEV1 is low, documented that FEV1/FVC ratio is reduced (normal >0.75-0.80 in adults and >0.90 in children).
FEV1 increases by >12 % after inhaling bronchodilator. This is called ‘Bronchodilator reversibility’.
Average daily diurnal (Peak Expiratory Flow) PEF variability is >10 % (in children >13%).
Treatment 1) ABG analysis and SpO2 analysis done to find out Oxygen
saturation.
2) Oxygen (100%) given 2-4 l/min via face mask.
3) Beta-adrenergic agonists – to relieve bronchospasm
Levo-Salbutamol 5 mg by nebuliser with oxygen and repeat every 30 mins if necessary (or give continously in severe asthma).
3) Anticholinergics – synergistic effect with beta-adrenergic agonists. Anticholinergics relax smooth muscle whereas B2 agonist increase levels of cAMP to cause bronchodilation.
Ipratropium bromide 250-500 µg by nebulizer and repeat every 4 hours if necessary.
4) Corticosteroids – reduce inflammation of airways, effects delayed for at least 4 hours but important to prevent relapse.
Hydrocortisone 100-200 mg IV repeat after half hour & then 6-8 hourly.
Inhaled steroids – Budesonide 1 to 2 inhalations 200 – 400
mcg twice daily. Max. dose: 2 inhalations (400 mcg) twice daily.
5) Aminophylline (therapy carefully monitored to avoid toxicity) 5 mg/kg (max 250 mg) IV drip over 3-4 hours. If IV bolus, then given over 20 mins. Theophylline is given if patient is not improving or after 2 days. IV stat dose is 2-4 mg/kg over 15 mins
6) Antibiotics – Amoxicillin 500 mg IV 8 hourly to control infections. Doxycyline/Azithromycin alternatively.
7) If patient is in severe acidosis – shift to ICU and ventilated if needed.
8) ECG – to know cardiac status and control arrythmias. X-ray & HGT status done along with 2 D-Echo if patient is in failure.
9) In severe spasm and respiratory failure, BiPAP given if not controlled then intubate patient.
Recent Advances in Bronchial Asthma treatment
Olodaterol (2 inhalations once daily) & Velanterol are newer long acting B2 agonists (LABA) and are better tolerated.
Tiotropium (18 mcg oral inhalation once daily) & Oxytropium are newer long acting muscarinic antagonists (LAMA) but are expensive and more commonly used in COPD patients.
Mepolizumab (monoclonal antibody) is IL5 antagonist given IV/SC & used in severe asthma with eosinophilia.
Omalizumab is Anti IgE, a monoclonal antibody used in Rx of Asthma.
Rolfumilast (500 mcg orally OD) is Phosphodiesterase - 4 inhibitor which increases CAMP & have bronchodilator action. More commonly used in COPD patients.
Umeclidinium inhalation powder is a long acting muscarinic antagonist (LAMA). Inhibits M3 receptors at smooth muscle leading to bronchodilation. Dose is 1 inhalation once daily by oral route.
Fluticasone furoate, a synthetic trifluorinated inhalational corticosteroid with anti-inflammatory activity. Used for maintenance & prophylactic Rx of Asthma. Dose is 100 mcg 1 puff once daily by orally inhaled route.
Bronchothermoplasty is a new method in which bronchial mucosa is stimulated once a week electrically.
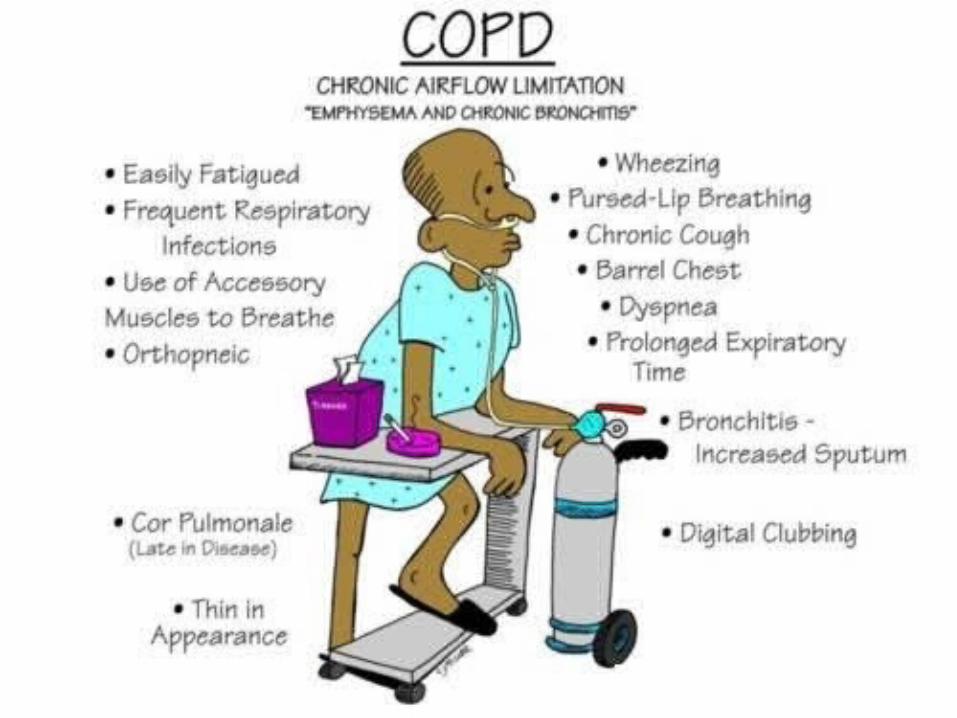
Acute Exacerbation of COPD (Chronic Obstructive Pulmonary Disease)
COPD is common and preventable disease characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in airways and lungs to noxious particles or gases.
An exacerbation of COPD is an acute event characterized by a worsening of patient’s respiratory symptoms that is beyond normal day to day variations.
Diagnoses of exacerbation relies exclusively on clinical presentation of patient complaining of an acute change of symptoms (dyspnea, cough, and/or sputum production) that is beyond day to day variation.
Occur due to disruption of airways, alveoli and pulmonary blood vessels.
Refers to group of conditions associated with chronic obstruction of air flow entering or leaving lungs.
It includes:1) Bronchitis2) Emphysema
Causes:3) Smoking - most common in India4) Genetic - deficiency of alpha-1 antitrypsin5) Age and Gender - >50 years and male more predominant6) Air Pollution7) Infections – HIV/Tuberculosis and history of severe childhood
respiratory infection leading to reduced lung function.
Severity of exacerbation can be done by pulse oximetry. Measurement of arterial blood gas is vital if coexistence of acute or acute on chronic respiratory failure suspected. PaO2 < 8.0 kPa (60 mmHg) with or without PaCO2 > 6.7 kPa (50 mmHg).
Emergency Care:1. ABG analysis and SpO2 analysis done to find out Oxygen
saturation. 84 % FiO2 for 2 ltr O2.
2. Position patient - sitting and loosen restrictive clothing
3. Assist ventilation if required and shift to intensive care unit.
4. Oxygen therapy (100 %) to be titrated to improve patients hypoxaemia with a target saturation of 88-92 % then low flow oxygen given.
7. Bronchodilators Salbutamol & Ipratropium bromide given in combination via nebulization every 6-8 hourly.
8. Corticosteroids Hydrocortisone 100-200 mg IV stat then 6 hourly and repeated every 6-8 hours.
9. Antibiotics antibiotics should be given when infection is underlying cause
of exacerbation.Amoxycillin 500 mg orally or Ampicillin 500 mg IV every 8 hours
OR if penicillin sensitiveErythromycin 500 mg orally every 6 hours.If patient is having severe pneumonia by atypical bacteria or old
age patient then use antibiotics like Imepenum, Tazobactum or Piperacillin.
10. Lasix 40 mg IV stat given as single bolus dose imrpoving biventricular failure.
11. Advice patient to stop smoking.
12. Maintenance of hydration is very important in COPD attack. DNS is used and Electrolyte imbalance restored by giving Cl, Na and K salts.
13. HGT & ECG done along with 2 D ECHO for cardiac re-modeling if any.
14. If patient is having CO2 narcosis / Poor consciousness / pH is 7.2 or less intubate patient. If pH > 7.2 BiPAP can be given. If patient not improved with BiPAP, more secretions & not tolerating then give mechanical ventilation.
15. If severe bronchospasm – IV drip of magnesium 4 amp 2 gm
In 100 ml NS can be used. Given very 4-6 hours.
16. Tab Deviry (Medroxy-progesterone) 10 mg for 15 days can be given by RT tube which acts as a respiratory stimulant.
Recent advances Combination of Umeclidinium ( long acting anticholinergic) &
Vilanterol ( long acting B2 agonist) are also available with once daily dose for maintenance of airflow in obstruction cases.
Aclidinium bromide (LAMA) in dry powder form for oral inhalation. Used for maintenance Rx of bronchospasm in cases of COPD. Dose is 400 mcg twice daily.
Tiotropium bromide (18 mcg oral inhalation once daily) & Oxytropium are newer long acting muscarinic antagonists (LAMA) more commonly used in COPD patients.
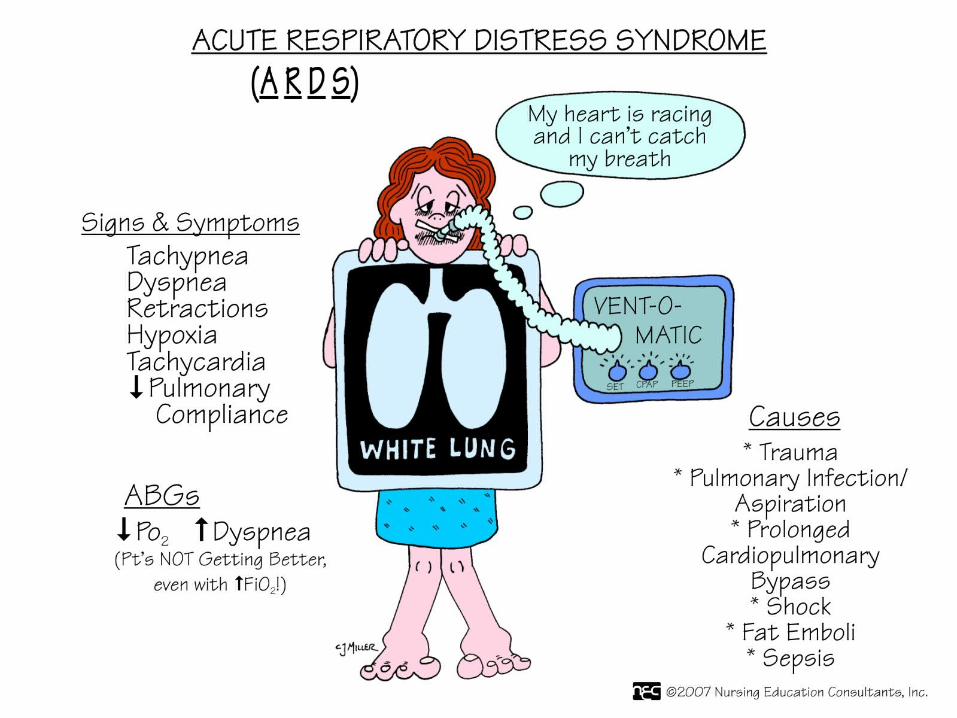
Acute Respiratory Distress Syndrome ( ARDS)
Fulminant form of respiratory failure characterized by acute lung inflammation and diffuse alveolar-capillary injury.
Syndrome develops as a complication of injury or illness such as trauma, gastric aspiration, cardiopulmonary bypass surgery, gram-negative sepsis, multiple blood transfusions, oxygen toxicity, toxic inhalation, drug overdose, pneumonia.
Increased capillary permeability, causing high-permeability noncardiogenic pulmonary edema occurs in which lungs are wet and heavy, congested, hemorrhagic, and stiff, with decreased perfusion capacity across alveolar membranes.
Pulmonary edema associated with ARDS causes severe hypoxemia, intrapulmonary shunting, reduced lung compliance and irreversible parenchymal lung damage in some cases.
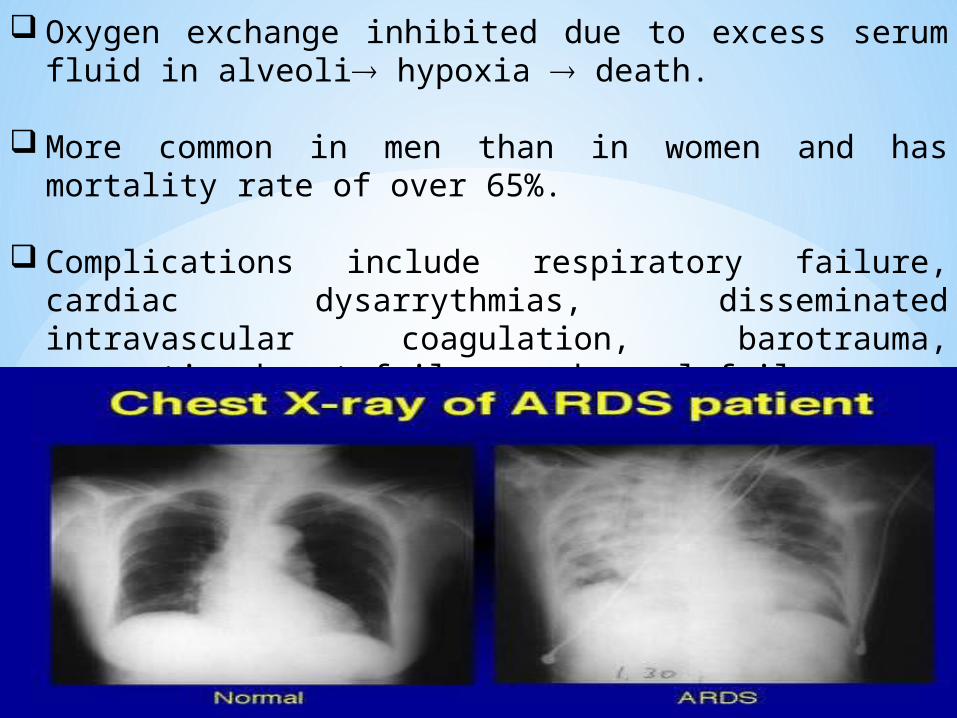
Oxygen exchange inhibited due to excess serum fluid in alveoli hypoxia death.
More common in men than in women and has mortality rate of over 65%.
Complications include respiratory failure, cardiac dysarrythmias, disseminated intravascular coagulation, barotrauma, congestive heart failure and renal failure.
Emergency Care:1. Immediate hospitalization along with 100 % high concentration
oxygen and ventilatory support.
2. Initial fluid replacement to maintain cardiac output and peripheral perfusion.
3. Surfactant therapy by its local action Reduces surface tension within alveoli facilitating aeration
at lower ventilatory pressures; increasing lung compliance and reduces work of breathing.
Aids in keeping alveoli dry (antiedema action) Enhances oxygenation of blood at lower intra-alveolar,
partial oxygen pressure; and Play role in immune defence system of lungs.
4. Surfactants available are bovine lung derived Calfactant and Beractant, porcine-lung derived poractant alpha; and
recombinant calfasceril.
5. Corticosteroids- Methyprednisolone (Solu-Medrol) ranging from 1 to 120 mg per kg as anti inflammatory drug is given and it reduces the number of days on a ventilator.
6. Additionally patients should receive low molecular-weight heparin (40 mg of enoxparin) or (5,000 units of dalteparin) subcutaneously per day or low dose, unfractioned heparin (5,000 units SC twice daily) to prevent thromboembolism.
7. Nutritional support preferably enteral, within 24 to 48 hours of admission to ICU.
8. Surfaxin (lucinactant) a synthetic formulation of pulmonary surfactant is indicated for prevention of RDS in infants. Supplied as intra-tracheal administration. Dose is 5.8 mL/kg birth weight. 4 doses administered in first 48 hours.
9. Higher antibiotics should be used as ARDS occurring due to sepsis need effective antibiotics like Piperacillin, Imepenum.
Acute Pulmonary Edema It is a condition caused by excess fluid in lungs with collection
of fluid in numerous air sacs making it difficult to breathe.
A medical emergency requiring immediate care & if untreated leads to respiratory failure.
Oxygen exchange inhibited due to excess serum fluid in alveoli hypoxia death
Presentationtachypneaabnormal breath sounds
crackles (rales) at both bases. rhonchi - fluid in larger airways of the lungs wheezing – lung’s protective mechanisms
-bronchioles constrict to keep additional fluid from entering the airway.
Causes may be cardiac or non cardiac
Cardiac include
1. Coronary artery disease
2. Cardiomyopathy
3. Heart valve problems
4. High blood pressure
Non Cardiac include
1. ARDS
2. High Altitudes
3. Pulmonary embolism
4. Near drowning
5. Lung injury
6. Exposure to certain toxins – ammonia, chlorine
7. Adverse drug reaction to certain drugs like heroin or cocaine
8. Viral Infections
Treatment
1) Immediate hospitalization
2) Place patient in position of comfort. Often patient chooses to sit upright posture.
3) Oxygen therapy
4) Monitor IV fluids and Blood pressure changes.
5) Give Continuous Positive Airway Pressure (CPAP) - a means of providing high flow, low pressure oxygenation. An effective way to treat and prevent intubation of patient. Allows better gas diffusion and re-expansion of collapsed alveoli. Also buys time for administered medications to work.
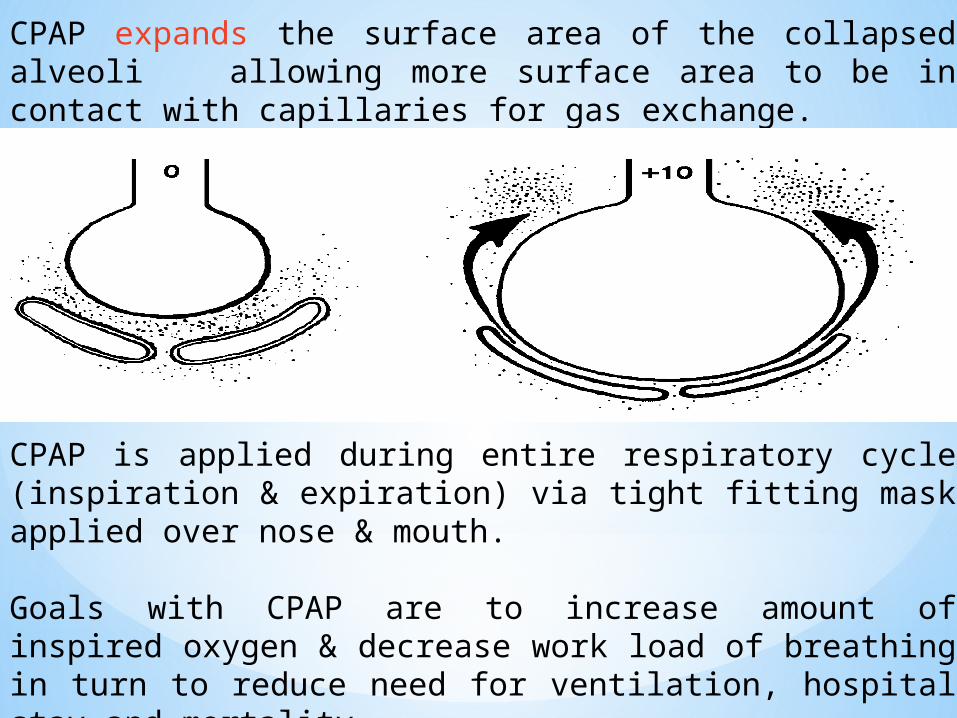
CPAP expands the surface area of the collapsed alveoli allowing more surface area to be in contact with capillaries for gas exchange.
CPAP is applied during entire respiratory cycle (inspiration & expiration) via tight fitting mask applied over nose & mouth.
Goals with CPAP are to increase amount of inspired oxygen & decrease work load of breathing in turn to reduce need for ventilation, hospital stay and mortality.
7) Nitroglycerin sublingual 0.4 mg, can repeat every 5 mins upto 3 doses if BP remains ≥ 100 mmHg. Its a venodilator, reduce cardiac workload & dilates coronary vessels. Do not use in presence of Hypotension. Onset in 1-3 mins.
8) Lasix 40 mg by IV infusion & repeat dose if needed. Causes venous dilation decreasing venous return to heart. Vascular effect within 5 mins and diuretic effect in 15-20 mins.
9) Morphine sulphate given 2 mg IV, titrate to response and vital signs, repeated every 2 mins to a maximum of 10 mg. Increases venous capacity and decrease venous return to heart.
10) Albuterol 2.5 mg in 3ml solution is administered via nebulizer to reverse bronchospasm.
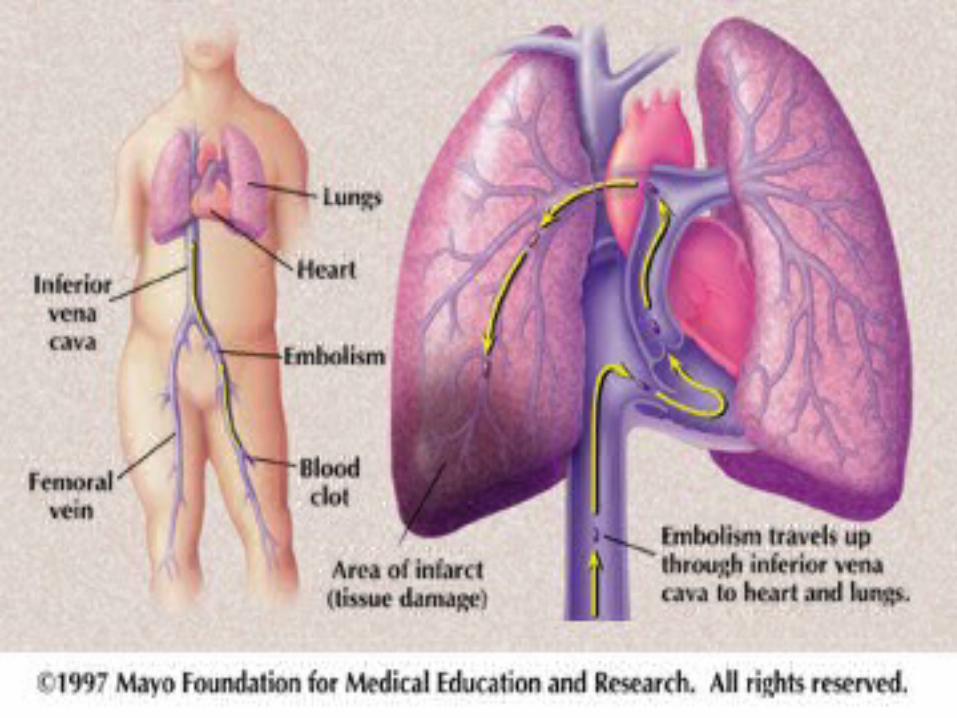
Acute Pulmonary Embolism It is a clot that forms in the deep venous system, usually in
thigh or pelvis, breaks off and travels to lungs, where it lodges in pulmonary vasculature.
Leads to hypoxemia and increase workload on heart.
Injury to blood vessels, decreased venous blood flow and alterations in coagulation system all increase risk of pulmonary embolism.
Signs & symptoms:• Dypsnea/tachypnea• Cyanosis• Acute pleuritic chest pain• Hemoptysis• Hypoxia
Emergency Care1) Immediate hospitalization and oxygen therapy (100 %) to all
hypoxaemic patients to restore arterial oxygen saturation to over 90%.
2) Opiates (Morphine) 4 to 10 mg every 4 hours administered IV over 4-5 mins to relieve pain and distress.
3) Obtain IV access, monitor closely vital parameters including Blood Pressure. Massive PE suspected if there systolic BP <90 mmHg or there is a fall of 40 mmHg for 15 mins not due to other causes.
4) Anticoagulation – LMW Heparin or Fondaparinux or Unfractioned Heparin is started and continued for 5 days or until INR ratio is 2 or above for at least 24 hours. UFH continuous IV Infusion: 5000 units IV one time as a bolus dose followed by 1300 units/hour by continuous IV infusion.
Alternatively, a bolus dose of 80 units/kg IV one time followed by 18 units/kg/hour by continuous IV infusion may be used.
In massive PE - initial dosage may be an IV bolus of 10,000 units followed by 1500 units/hour.
Heparin effective in reducing mortality in PE by reducing propagation of clot and further risk of emboli. Administered for at least 5 days and later anticoagulation continued with oral Warfarin for at least 6 weeks.
5) Thrombolytic therapy is useful adjunct in patients with severe pulmonary embolism and right ventricular dysfunction.
6) Surgical Procedure – Embolectomy in massive PE.
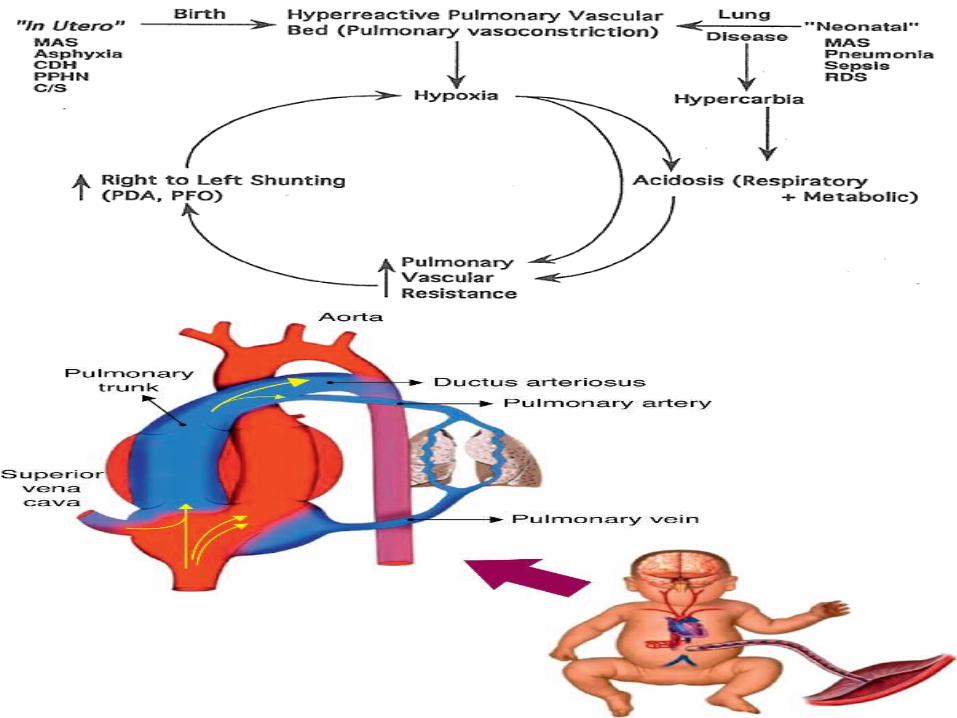
Pulmonary Hypertension in Newborn
It is defined as increased pulmonary vascular resistance & presence of right-left shunt at foramen ovale &/or ductus arteriosus level.
A serious disorder in which arteries to lungs remain constricted after delivery, limiting amount of blood flow to lungs & therefore amount of oxygen to blood stream.
Can occur due to severe respiratory distress in term or post-term newborns or by certain drugs (Aspirin or Indomethacin) taken by mother before delivery.
Symptoms include dyspnea, rapid breathing, fatigue, fainting spells, coughing up blood, progressive cyanosis.
Treatment
1) Oxygen therapy (100 %) is given.
2) Inhaled Nitric Oxide is used to relax blood vessels in lungs without any effect on blood vessels of rest of body.
3)Diuretics such as furosemide (1 mg/kg/dose) 1 to 2 times a day IV to get rid of excess fluid and reduce workload on heart.
4)Calcium channel blockers such as Nifedipine (0.25 to 0.5 mg/kg/day) sublingually in 1 to 2 divided doses to relax muscles in blood vessel wall and help function of right side of heart.
5)Phosphodiesterase-5 inhibitors (PDE-5) such as sildenafil, loading dose of 0.1 mg/kg IV/oral via feeding tube for 30 minutes, followed by maintenance dose of 0.03 mg/kg/hr up to 14 days and tadafil are medications that result in relaxation of blood vessels in lungs, to allow blood flow more easily.
6) Endothelin Receptor Antagonists (ERA’s) such as Bosentan (1mg/kg/dose) BD for short term use 2-16 days & Ambrisentan (5 mg and 10 mg) are oral drugs which block Endothelin (substance in wall of blood vessels that cause narrowing of vessel). Allow blood flow more easily. ERAs are often combined with PDE-5 inhibitors.
7) Prostacyclins a drug class shown to slow progression of pulmonary hypertension. Eg. Epoprostenol (2-4 ng/kg/min IV).
8) Antiplatelet and anticoagulant therapies such as low dos aspirin 75 mg and warfarin 20 mg are used to minimize blood clot formation in the pulmonary blood vessels.
Pulmonary Hypertension in Adults
It is defined as pulmonary arterial pressure > 25 or 30 mmHg during exercise and “pulmonary wedge pressure” < 15 mmHg.
Pulmonary hypertension begins when tiny arteries in lungs, called pulmonary arteries, and capillaries become narrowed, blocked or destroyed.
Can be idiopathic or sometimes or due to pulmonary emboli, COPD, scleroderma, congenital heart defects, cirrhosis, AIDS, pulmonary fibrosis, left sided heart failure, climbing to high altitudes >8000 feet & narcotics such as cocaine.
Eisenmenger syndrome (a congenital heart defect) also causes pulmonary hypertension.
Causes Diet drug (fen-phen) appetite suppressant containing
dexfenfluramine & phentermine. Liver diseases, rheumatic disorders, lung conditions Heart diseases- aortic valve disease, left heart failure, mitral
valve disease & congenital heart disease Thromboembolic disease Low-oxygen conditions Genetic
Symptoms Shortness of breath (1st symptom) with routine activity. Fatigue Fainting spells Swelling in ankles/abdomen/legs Bluish lips Chest pain
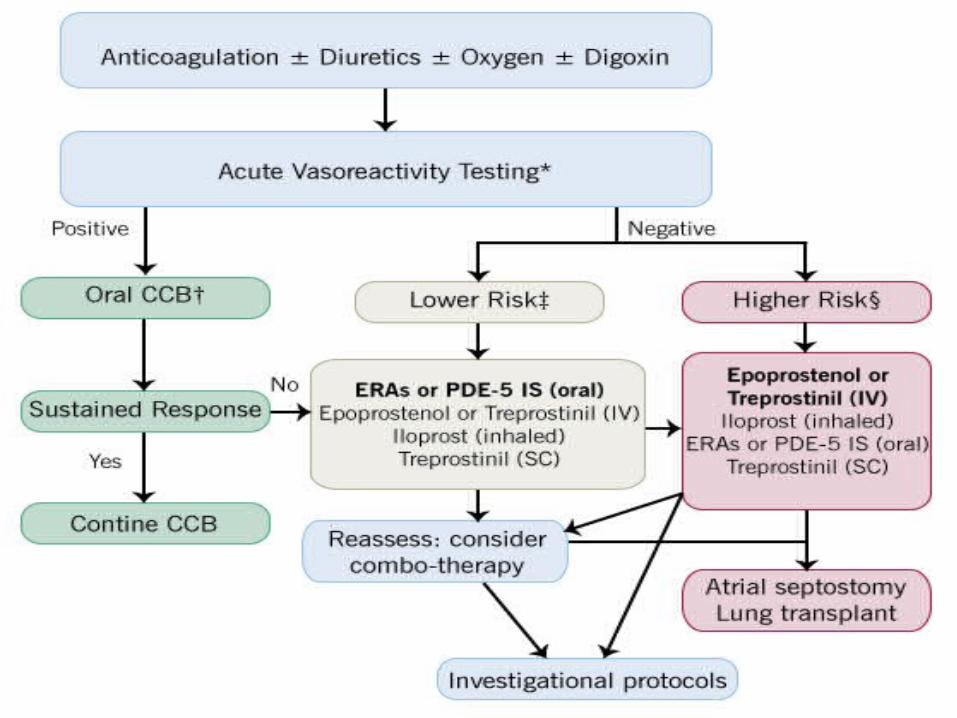
Treatment
1) Oxygen therapy (100 %)
2) Inhaled Nitric Oxide is used to relax blood vessels in lungs without any effect on blood vessels of rest of body.
3)Diuretics such as furosemide 20 to 40 mg/dose every 4-6 hours to get rid of excess fluid and reduce workload on heart.
4)Calcium channel blockers like Nifedipine 30 to 60 mg OD sublingually or Diltiazem 30 – 60 mg orally TDS to relax muscles in blood vessel wall and help function of right side of heart.
5)Phosphodiesterase-5 inhibitors (PDE-5) such as sildenafil 5 to 20 mg TDS (IV – 2.5 to 10 mg as bolus) and tadalafil 40 mg OD are oral medications that result in relaxation of blood vessels in lungs to allow blood flow more easily.
6) Inotropic agents like digoxin 8-12 mcg/kg IV improve hearts pumping ability.
7) Bosentan (62.5 mg BD orally for 4 weeks) followed by maintenance dose of 125 mg daily or Ambrisentan (5 mg OD orally) or Macitentan (10 mg OD orally) are ERA’s blocking actions of endothelin.
8) Epoprostenol (2ng/kg/min IV), Treprostinil sodium (0.25-0.5 mg orally BD with food) & Iloprost (2.5 mcg via inhaler or nebulizer taken 6 to 9 times a day) dilate pulmonary arties and prevent blood clot from forming.
9) Anticoagulants or blood thinners such as Warfarin Sodium (2-5 mg orally) decrease blood clot formation & blood to move more freely.
10) Riociguat a stimulator of guanylate cyclase, an enzyme in cardiopulmonary system & receptor for nitric oxide. Stimulators help arteries to relax increasing blood flow and decreasing blood pressure. Indicated for persistent/recurrent Chronic Thromboembolic Pulmonary Hypertension (CTEPH). Dose is 1 mg TDS orally.
11)Macitentan (Opsumit) a Endothelin receptor antagonist preventing binding of ET-1 to both ETA & ETB receptors specially indicated for Rx of Pulmonary arterial hypertension. Dose is 10 mg OD orally. Other drugs are Atrasentan, Zibotentan, Tezotentan & Siladtentan.
12)Tolazoline non-selective short acting alpha blocker also used in treatment.
Acute Mountain Sickness (AMS)
A syndrome comprising headache (principal symptom) together with fatigue, anorexia, nausea and vomiting, difficulty sleeping and dizziness.
Ataxia and peripheral edema may be present.
Aetiology not clearly understood but though that hypoxaemia increases cerebral blood flow and hence intracranial pressure.
Symptoms occur within 6-12 hours of an ascent and vary in severity.
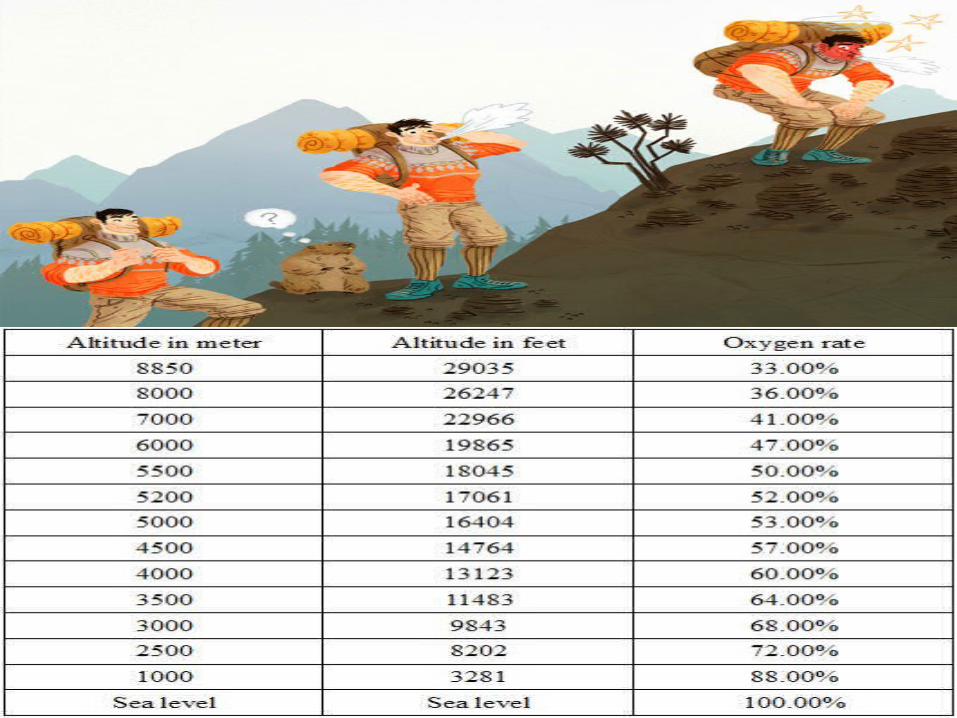
Incidence in travellers who ascent 3000 m above ground level and may be 40-50% dependent on rate of ascent.
Treatment
Rest & simple analgesia
Symptoms usually resolve after 1-3 days at a stable altitude but may reoccur with further ascent.
Avoidance of over exertion at high altitude.
Supplementary oxygen can be given.
Descent the patient from high altitude.
Prophylactic Acetazolamide is the drug of choice given at dose of 250mg 8 hourly day before, during and for 5 days after ascent. Acetazolamide helps by causing Mild Respiratory Acidosis, which increases respiratory drive, prevents hypoxaemia. It ameliorates symptoms.
Dexamethasone in dose of 4 mg 6 hourly begun on day of onset, continued for 3 days at high altitude & then tapered. Useful in reducing symptoms & incidence of acute mountain sickness.
Nifedipine (30-60 mg OD orally sublingually) preferred for prevention & treatment of pulmonary hypertension. Acts by lowering pulmonary arterial pressure, critical in development of pulmonary edema.
Beta-adrenergic agonists for bronchodilatory action.
Phosphodiesterase-5 inhibitor like Sildenafil (5 – 20 mg TDS orally) to increase blood flow to lungs.
NSAIDS and Anti-emetics when necessary.
Decompression Sickness
Most common in Scuba Divers
Ambient pressure under water increases by 101kPa (1atmp) for every 10 m of sea water depth. As divers descend, partial pressure of gases they breathe increase and blood/tissue concentration of dissolved gas increase.
Symptoms usually present during or within 4 hours of dive.
Exposure of individuals to increase partial pressure of nitrogen ( inert gas) result in additional nitrogen dissolved in body tissues, amount dissolved depends on depth/pressure & duration of dive.
On fast ascent, tissues get supersaturated with nitrogen placing diver at risk of producing critical quantity of gas(bubbles) in
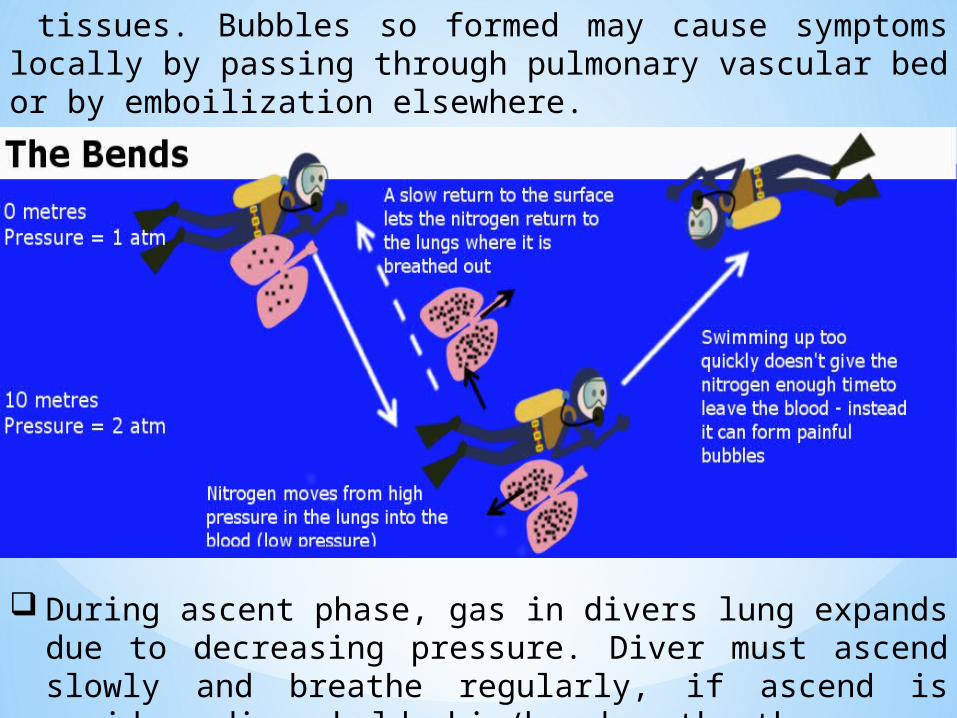
tissues. Bubbles so formed may cause symptoms locally by passing through pulmonary vascular bed or by emboilization elsewhere.
During ascent phase, gas in divers lung expands due to decreasing pressure. Diver must ascend slowly and breathe regularly, if ascend is rapid or diver holds his/her breath, the
expanding gas may cause lung explode (pulmonary barotrauma) resulting in pneumomediastinum, pneumothroax or arterial gas embolism.
Management
1) Patient nursed in horizontal position
2) Recompression requiring transfer of patient to surface or air provided the altitude remains low (<300 m) and patient continues to breathe 100% oxygen. Recompression reduces volume of gas within tissues & puts nitrogen back into solution.
3) High flow oxygen to be given by tight fitting mask. Assists in wash out of excess inert gas & reduce extent of local tissue hypoxia which can result from focal embolic injury.
4) Neurological & pulmonary symptoms, marked skin lesions to be treated by hyperbaric oxygen(100 % Oxygen delivered in high pressure chamber) if seen in 10-14 days.
5) Intravenous fluid replacement with 0.9 % saline or Hartmann’s solution to correct intravascular fluid loss from endothelial bubble injury & dehydration associated with immersion.
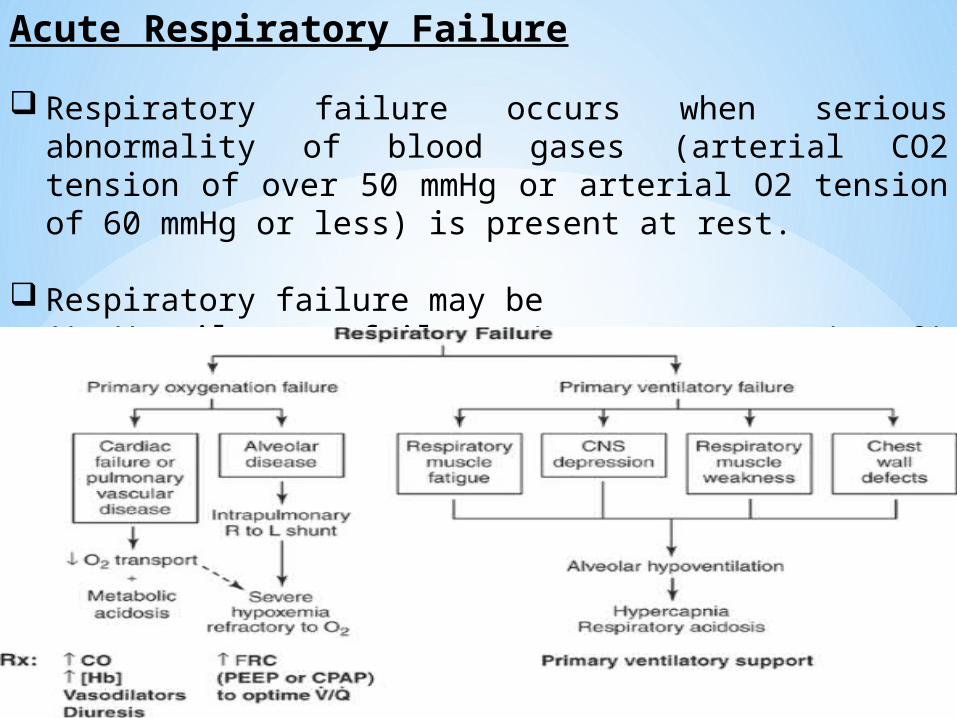
Acute Respiratory Failure
Respiratory failure occurs when serious abnormality of blood gases (arterial CO2 tension of over 50 mmHg or arterial O2 tension of 60 mmHg or less) is present at rest.
Respiratory failure may be1) Ventilatory failure (commonest type) 2) Oxygenation failure
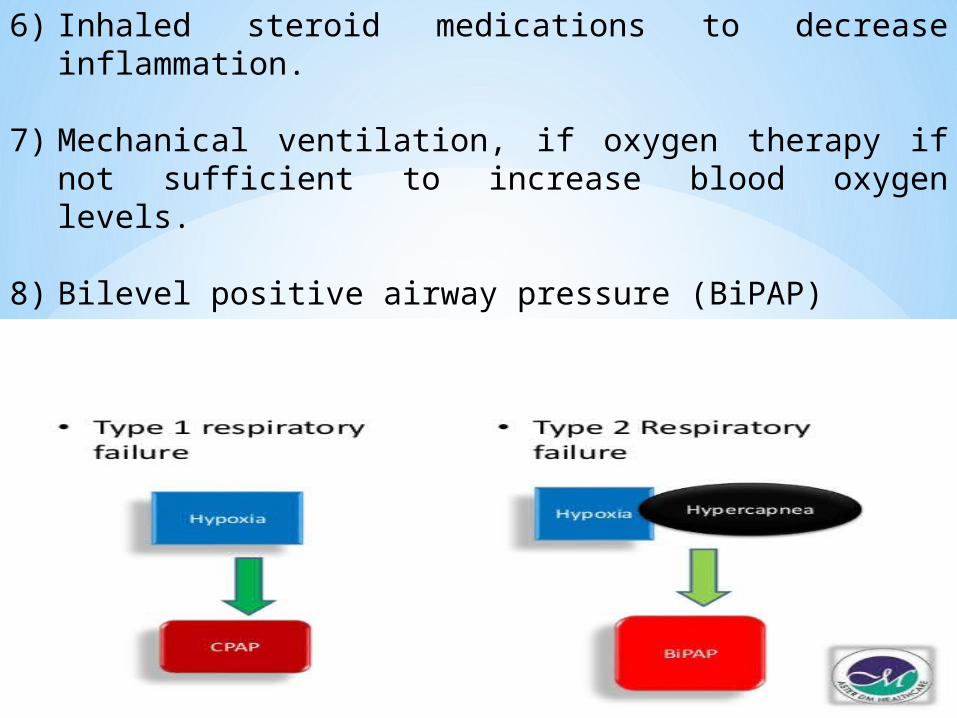
Respiratory Failure can also be classified as Type 1 & Type 2.
Type 1 Respiratory Failure Has low level of oxygen in blood (hypoxaemia) without
increased carbon dioxide level (hypercapnia)
Caused by ventilation / perfusion mismatch i.e. volume of air in and out of lungs is not matched with flow of blood to lungs
PaO2 - decreased (< 60 mmHg (8.0 kPa) PaCO2 - normal or decreased (<50 mmHg (6.7 kPa) PA-aO2 - increased
Type 2 Respiratory Failure Hypoxemia (PaO2 <8kPa) with hypercapnia (PaCO2
>6.0kPa).
PaO2 - decreased (< 60 mmHg (8.0 kPa)
PaCO2 - increased (> 50 mmHg (6.7 kPa) PA-aO2 - normal Ph - decreased
Treatment1) Treatment of the underlying cause.
2) Goals are to increase oxygenation and improve ventilation.
3) Oxygen to be given continuously to maintain oxygen saturation at 85 to 90 % just enough to correct hypoxaemia without causing hypercapnia.
4) Antibiotics to treat respiratory infections.
5) Bronchodilators including anticholinergics such as tiotropium 18 mcg via inhalation and beta agonists such as albuterol 200 mcg by inhalation every 4-6 hours.
6) Inhaled steroid medications to decrease inflammation.
7) Mechanical ventilation, if oxygen therapy if not sufficient to increase blood oxygen levels.
8) Bilevel positive airway pressure (BiPAP)
9) Continuous positive airway pressure (CPAP)
10) Respiratory stimulants (Analeptics) used to increase ventilation in patients in whom oxygen therapy is followed by reduction in ventilation.
Stimulate coughing and help patient to expel secretions.
Satisfactory response characterized by return of deeper breathing & consciousness & reduction in carbon dioxide tension in blood.
Doxapram 1.5 – 4 mg/min IV is given as respiratory stimulant along with assisted mechanical ventilation.
Almiprine bismethylate, a piperaizne derivative selectively stimulates peripheral chemoreceptors & claimed to stimulate ventilation in hypoxia patients.
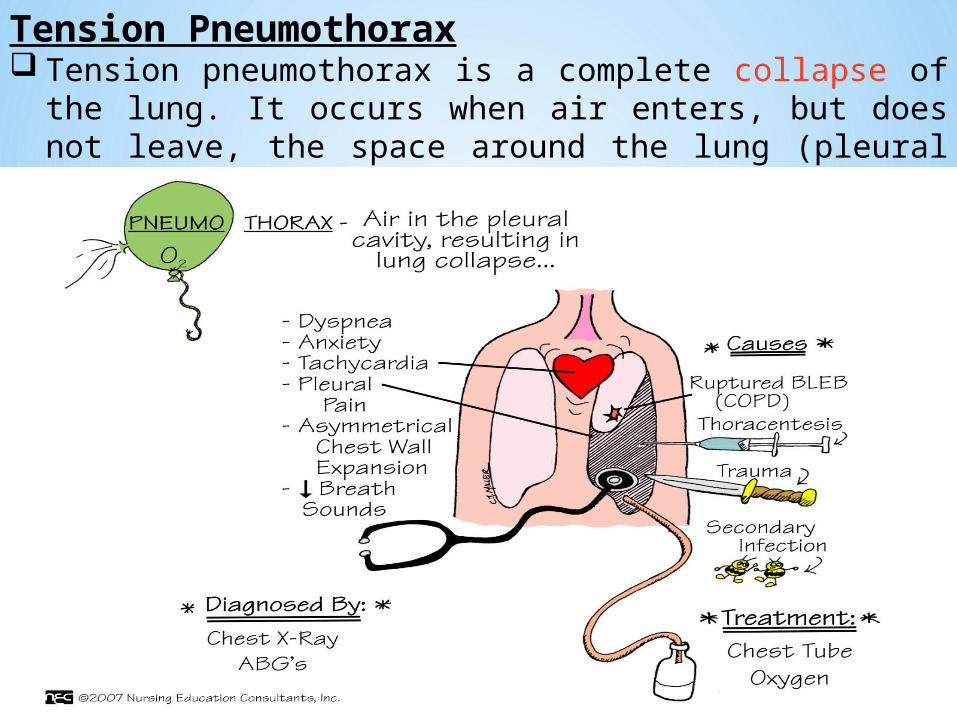
Tension Pneumothorax Tension pneumothorax is a complete collapse of the lung. It
occurs when air enters, but does not leave, the space around the lung (pleural space).
Treatment
1) Immediate Hospitalization
2) Main aim is to remove air from pleural space allowing lung to re-expand.
3) In emergency, a small needle (IV needle) is placed in chest cavity through the ribs to relieve pressure.
4) Standard treatment is a chest tube, a large plastic tube is inserted through the chest wall between 4th, 5th or 6th Intercostal space to remove air. The chest tube is attached to a vacuum bottle that slowly removes air from the chest cavity. This allows the lung to re-expand. As the lung heals and stops leaking air, the vacuum is turned down and then the chest tube is removed.
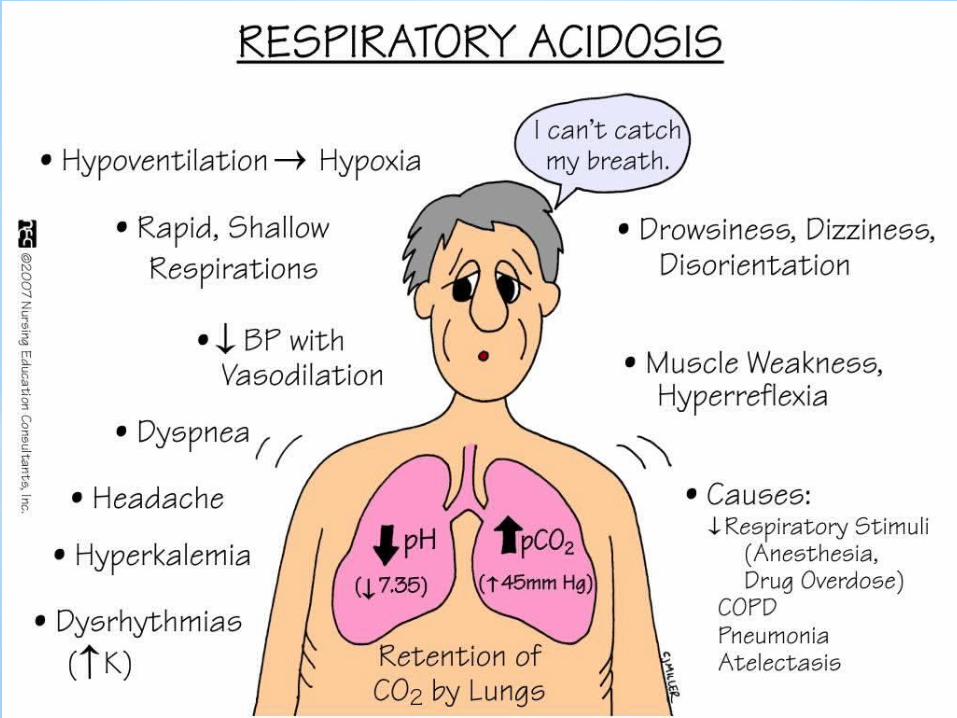
Respiratory Acidosis
Acidosis is defined as increase in either potential &/or nonvolatile hydrion content of body.
It is due to increased retention of potential hydrion (CO2) in blood leading to rise in plasma carbonic acid content.
Usually occurs in chronic lung diseases with cor-pulmonale, in diseases with respiratory muscle paralysis and following respiratory centre depression.
Plasma bicarbonate and pCO2 are raised.
Treatment1) Immediate hospitalization and care
2) Admission to medical ICU if patient is confused, lethargic, respiratory muscle fatigue and pH <7.24. Endotracheal intubation with mechanical ventilation when needed.
3) Treatment of underlying cause & rapid correction of hypercapnea is prevented to avoid patient landing up in alkalemia.
4) Oxygen therapy used with caution by titrating oxygen delivery to maintain oxygen saturation in the low 90% range and partial arterial pressure of oxygen (PaO2) in range of 60-65 mm Hg.
5) Bronchodilators like beta agonists (salbutamol/albuterol), anticholinergics (ipratropium bromide & tiotropium) & methyxanthines ( theophylline) used to revere bronchspasm.
6) Acidosis corrected by slow infusion of 7.5 % sodium bicarbonate (1 mMol/kg over 20-30 mins) to raise bicarbonate level to about 15-20 mMol/L.
7) Antibiotics to treat any respiratory infections.
8) Electrolyte disturbances of sodium and potassium depletion should be corrected.
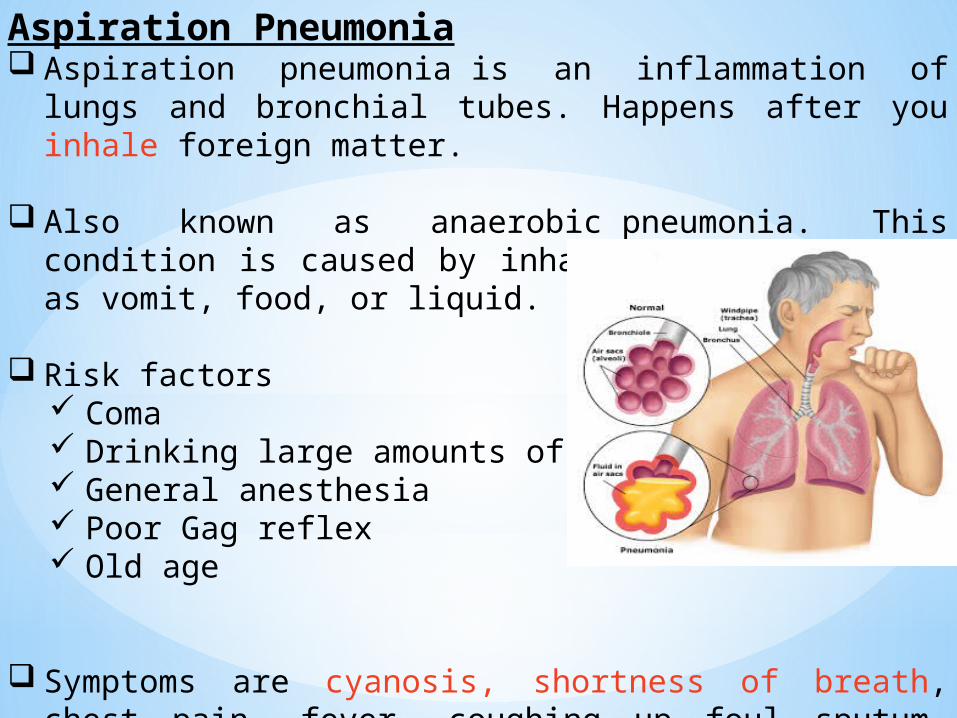
Aspiration Pneumonia Aspiration pneumonia is an inflammation of lungs and bronchial
tubes. Happens after you inhale foreign matter.
Also known as anaerobic pneumonia. This condition is caused by inhaling materials such as vomit, food, or liquid.
Risk factors Coma Drinking large amounts of alcohol General anesthesia Poor Gag reflex Old age
Symptoms are cyanosis, shortness of breath, chest pain, fever, coughing up foul sputum. Bronchoscopy is helpful in diagnosing the condition.
Treatment
1) Immediate Hospitalization
2) Oxygen supplementation, cardiac monitoring & pulse oximetry.
3) Oropharyngeal / tracheal suctioning may be indicated to further remove aspirate.
4) Reassess the need for intubation on frequent basis depending on patient’s oxygenation, mental status, signs of increased work of breathing, or impending respiratory failure. IV fluids & electrolyte replacement.
5) Bronchoscopy helpful when aspiration of foreign body or food material suspected, also helpful in guiding antibiotic therapy.
6) Thoracentesis (pleural fluid aspiration) is a diagnostic therapeutic procedure in which fluid (or air) is removed from between the pleura and chest wall.
7) Antibiotics to treat respiratory infections & Mechanical ventilation if needed.
ConclusionEvery patient diagnosed with life threatening respiratory emergency should receive the emergency care as early as possible including oxygenation, ventilatory support and appropriate pharmacotherapy which would help in saving patients life and preventing complications.