
Management of Respiratory Distress in · PDF fileSilverman-Anderson Index Feature Score 0...
91
Management of Respiratory Distress in Preterm Infants Albert Owusu-Ansah, MD, FAAP Medical Director of NICU BryanLGH Medical Center ment of Respiratory Distress in Infants Owusu-Ansah, MD, FAAP al Director of NICU LGH Medical Center
Transcript of Management of Respiratory Distress in · PDF fileSilverman-Anderson Index Feature Score 0...
Management of Respiratory Distress in
Preterm Infants
Albert Owusu-Ansah, MD, FAAP
Medical Director of NICU
BryanLGH Medical Center
Management of Respiratory Distress in
Preterm Infants
Albert Owusu-Ansah, MD, FAAP
Medical Director of NICU
BryanLGH Medical Center
Objectives
• Identify and interpret signs of respiratory
distress in the newborn
• Differentiate between respiratory and
cardiac causes of cyanosis
• Identify the indications for assisted
ventilation in the neonate
• Discuss recent trends in CPAP use in
infants

Disclosures
• None
Respiratory Distress
• Cause of significant morbidity and mortality
• Indicates abnormal pulmonary function
• Incidence depends on • gestational age, mode of delivery, sex,
maternal diabetes, asphyxia, etc
• Early recognition and appropriate management essential
Respiratory Distress
• Tachypnea- RR>60/min
• Retractions
• Subcostal
• intercostal
• Grunting
• Nasal flaring
• Cyanosis

Retractions

Retractions
Respiratory Distress
Causes
• Pulmonary– Most common cause
• Cardiac- Congenital heart disease
• CNS- Asphyxia, IC bleed
• Other Causes-Hypoglycemia, acidosis, hypervolemia, hyperviscosity (polycythemia), anemia, hypothermia, metabolic acidosis
Respiratory Distress - Ruling out Cardiac Disease
• Differentiating cardiac and respiratory causes of cyanosis is a common clinical problem.
• A hyperoxia test may assist in differentiating between the two.
• Pulse oximetry may help to decide whether a formal hyperoxic test is useful.
• A neonate who exhibits cyanosis without marked respiratory distress and has an O2 saturation of less than 85% in both room air and 100% oxygen likely has an intracardiac shunt.
• If the O2 saturation increases to more than 85% on 100% oxygen, a full hyperoxia test should be performed
Hyperoxia Test
• The test consists of obtaining a baseline right radial (preductal) arterial blood gas measurement with the child breathing room air and repeating the measurement while the infant is receiving 100% O2. A PaO2 measurement greater than 300 mm Hg on 100% oxygen is normal, more than 150 mm Hg suggests pulmonary disease, and 50 to 150 mm Hg suggests cardiac disease (or severe pulmonary hypertension).
• Echocardiography is the definitive investigation.
Respiratory Distress- Pulmonary
Obstructive problems
• Anything obstructing airway from nose to air sacs
• Mucus in nasal cavity
• Misplaced photherapy mask
• Congenital abnormalities of the airway
• Choanal atresia, Pierre Robin Syndrome
• Conditions restricting lung expansion within chest
cavity
• Pneumothorax, diaphragmatic hernia
Respiratory Distress –Pulmonary causes
• Respiratory Distress Syndrome (RDS)
• Pneumonia (Sepsis)
• Meconium Aspiration Syndrome (MAS)
• Transient Tachypnea ofNnewborn (TTN)
• Persistent Pulmonary Hypertension of the Newborn
(PPHN)
Respiratory Distress-Other Causes
• Tracheo-esophageal fistula
• Diaphragmatic hernia
• Congenital Cystic Lung Diseases
• Congenital Cystic Adenomatoid Malformation
• Lobar emphysema
• Pulmonary sequestration
• Bronchogenic cysts
• Lung hypoplasia
History • Good History important
• Gestation
• Antenatal Steroids
• PROM
• Onset of respiratory distress
• Apgar score
• MSAF?
• Feeding problems and relation to respiratory distress
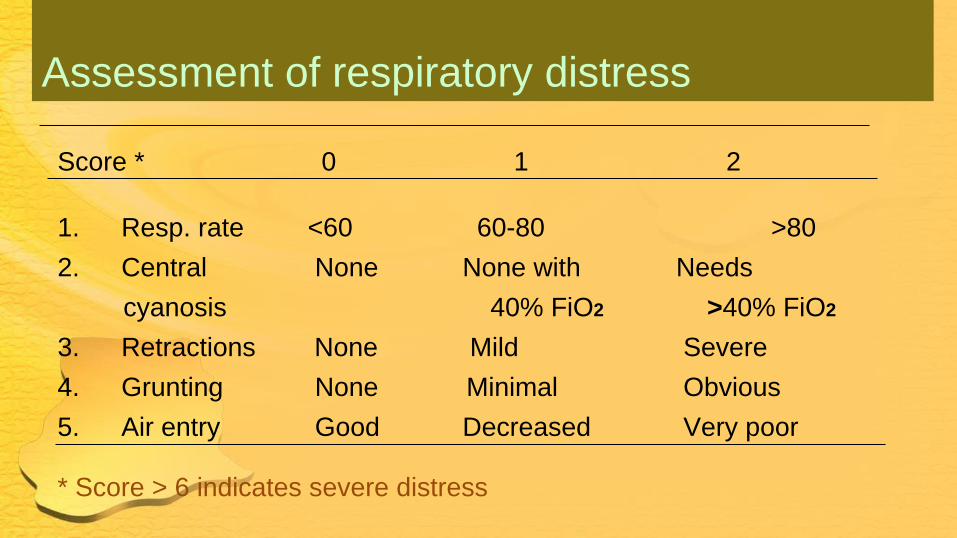
Assessment of respiratory distress
Score * 0 1 2
1. Resp. rate <60 60-80 >80
2. Central None None with Needs
cyanosis 40% FiO2 >40% FiO2
3. Retractions None Mild Severe
4. Grunting None Minimal Obvious
5. Air entry Good Decreased Very poor
* Score > 6 indicates severe distress
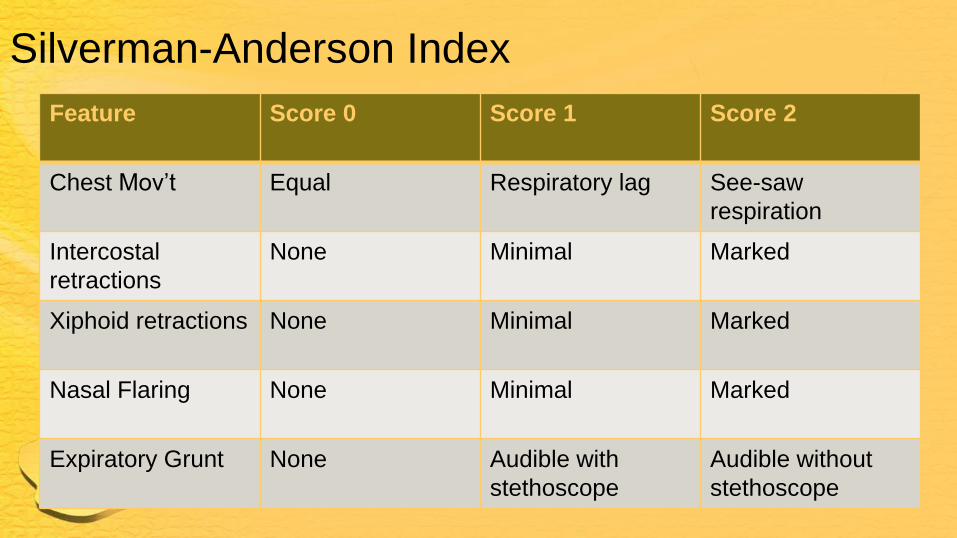
Silverman-Anderson Index
Feature Score 0 Score 1 Score 2
Chest Mov’t Equal Respiratory lag See-saw
respiration
Intercostal
retractions
None Minimal Marked
Xiphoid retractions None Minimal Marked
Nasal Flaring None Minimal Marked
Expiratory Grunt None Audible with
stethoscope
Audible without
stethoscope
• Respiratory Distress
Syndrome
• RDS
Respiratory Distress Syndrome RDS
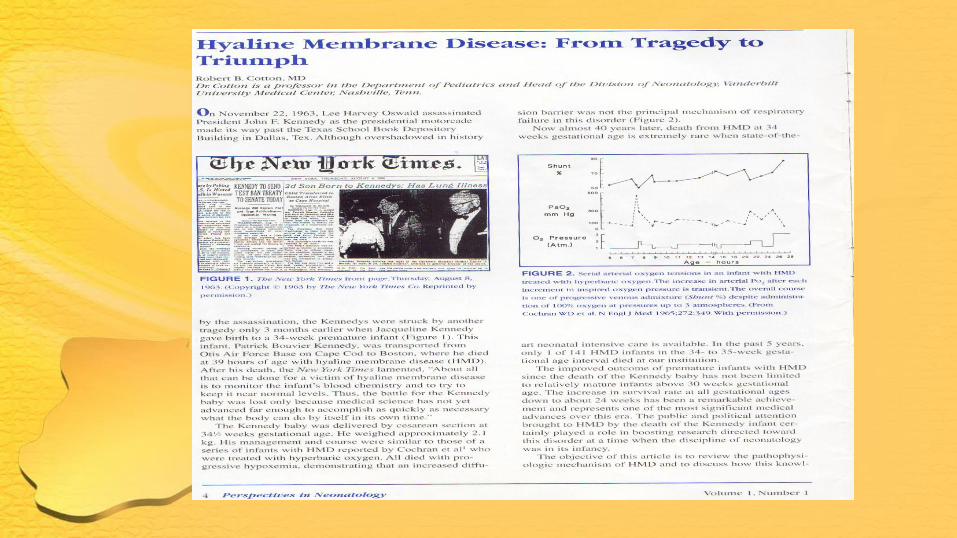
• RDS aka HMD is the major cause of respiratory distress in preterm infants.
• Onset is early and it is progressive.
• RDS is a result of surfactant deficiency, which leads to increase in surface tension in the air-liquid interface of the terminal respiratory units.
Respiratory Distress Syndrome • Surfactant deficiency leads to atelectasis, increases
ventilation perfusion mismatch, and leads to lung injury,
which is mediated by a marked pulmonary inflammatory
response
• In 1950s RDS developed in 14% of infants weighing 1 to 2.5
kg, and 56% of them died.
Clinical features • Risk factors:
• Prematurity
• maternal diabetes, maternal bleeding, perinatal asphyxia,
C-section without labor
• White race, male sex
• Features :
• Early onset, from birth to four hours
• Uncomplicated clinical course with progressive worsening
until day 2-3 and onset of recovery by 72 hours
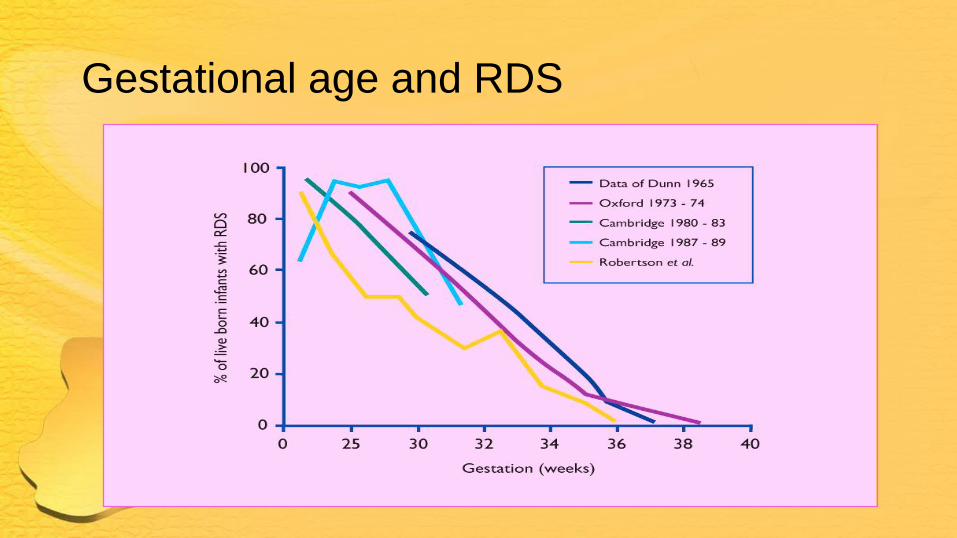
Gestational age and RDS
Clinical features (contd)
• Physical Examination
• Brief but thorough
• Signs of respiratory distress :
• Cyanosis
• Tachypnea ( >60/min, shallow, rapid )
• Grunting ( delayed expiration maintains FRC )
• Retraction ( Subcostal, substernal, intercostal )
• Flaring ( 50% airway resist in nose& pharynx)
• Temperature, Blood pressure, Skin perfusion
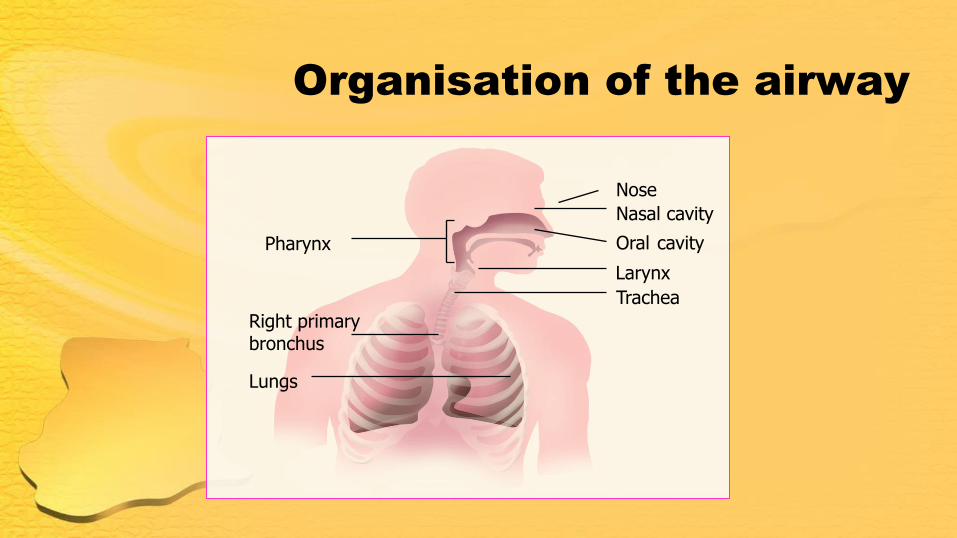
Organisation of the airway
Pharynx
Right primary bronchus
Nose
Nasal cavity
Oral cavity
Larynx
Trachea
Lungs
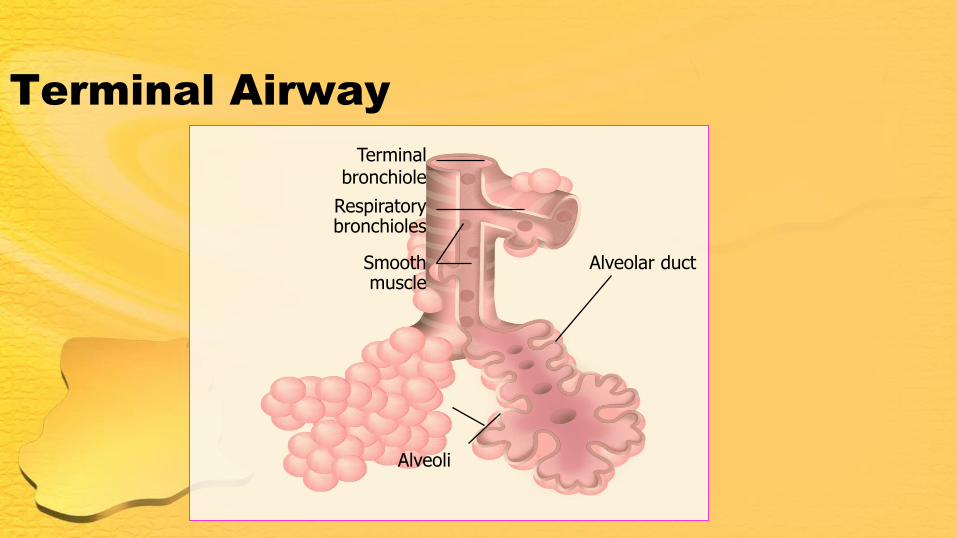
Terminal Airway
Terminal bronchiole
Alveolar duct
Respiratory bronchioles
Smooth muscle
Alveoli
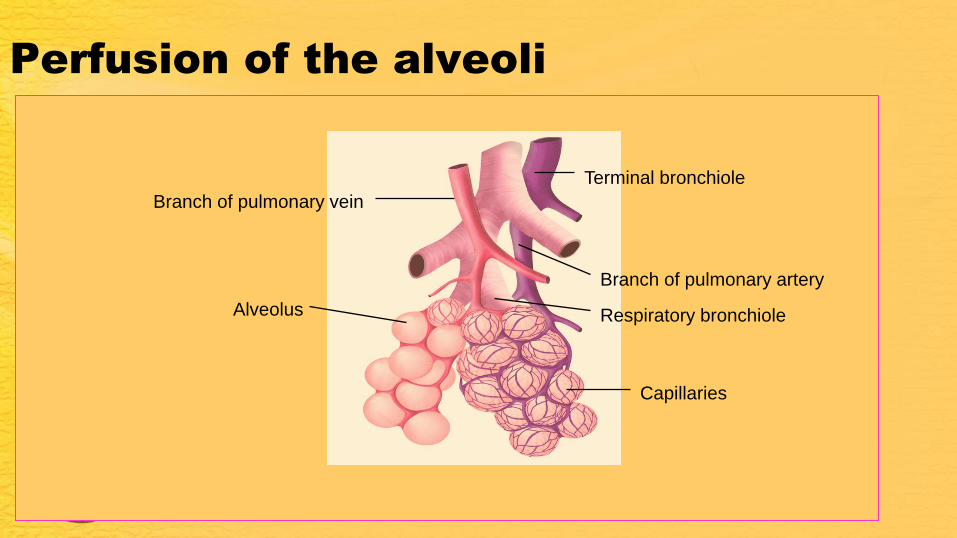
Perfusion of the alveoli
Capillaries
Terminal bronchiole
Branch of pulmonary artery
Alveolus
Branch of pulmonary vein
Respiratory bronchiole
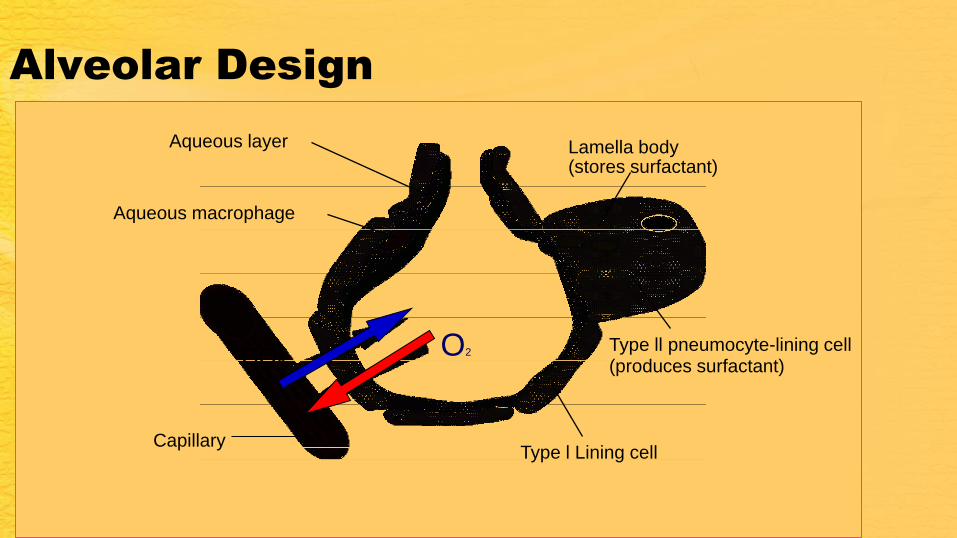
Alveolar Design
Aqueous layer
Aqueous macrophage
Lamella body (stores surfactant)
Type ll pneumocyte-lining cell (produces surfactant)
Type l Lining cell
Capillary
CO2 O2
Lung Development
• Knowledge of lung development central to
understanding pathophysiology of RDS
Lung development
Embryonic (4-7 weeks)
Pseudoglandular (5-17 weeks)
Canalicular (16-26 weeks)
Alveolar period (36 weeks) – post natal years
Saccular period (24-38 weeks)
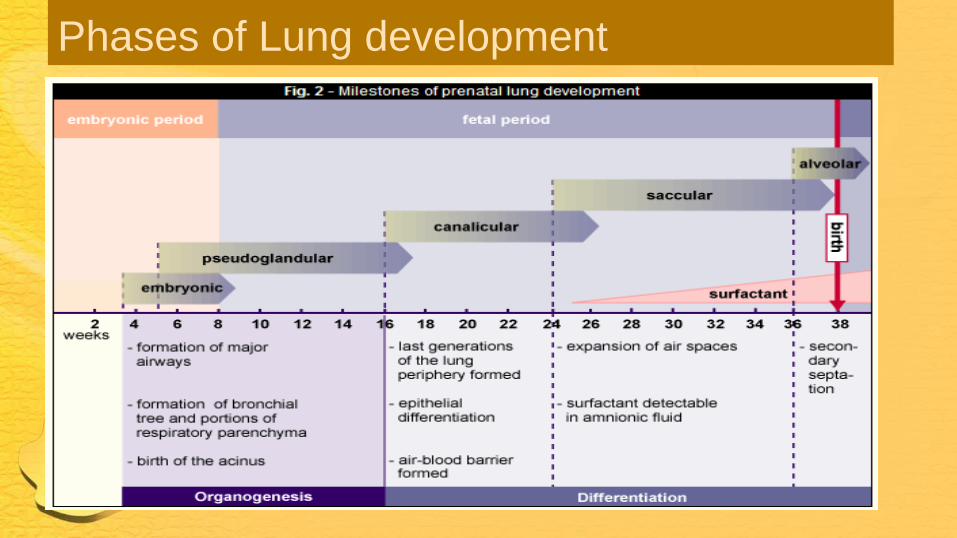
Phases of Lung development
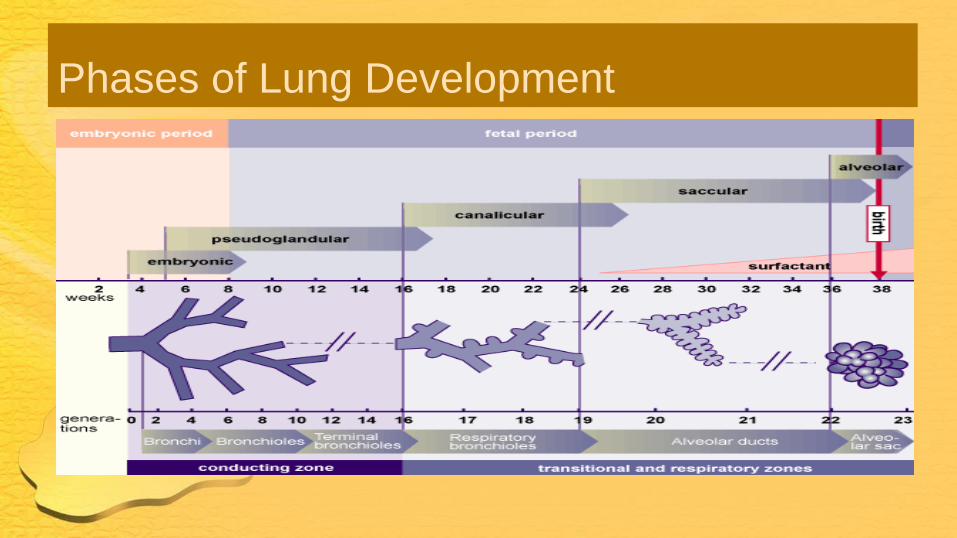
Phases of Lung Development
Canicular period
Diameter of airway increases
Primitive alveolus is formed
Type I and Type II cells differentiate
Surfactant production begins
Pulmonary Surfactant
• A complex mixture composed mostly of lipids, 90%
(primarily phospholipids), and about 10% proteins
• Lipid - ~70% is phosphatidylcholine species
• Protein – Four surfactant-specific proteins identified:
SP-A, SP-B, SP-C, SP-D
• SP-A, SP-D: Host defence
• SP-B, SP-C: Facilitates surface absorption and
spreading of lipids
1 2 3 4 5
6
7
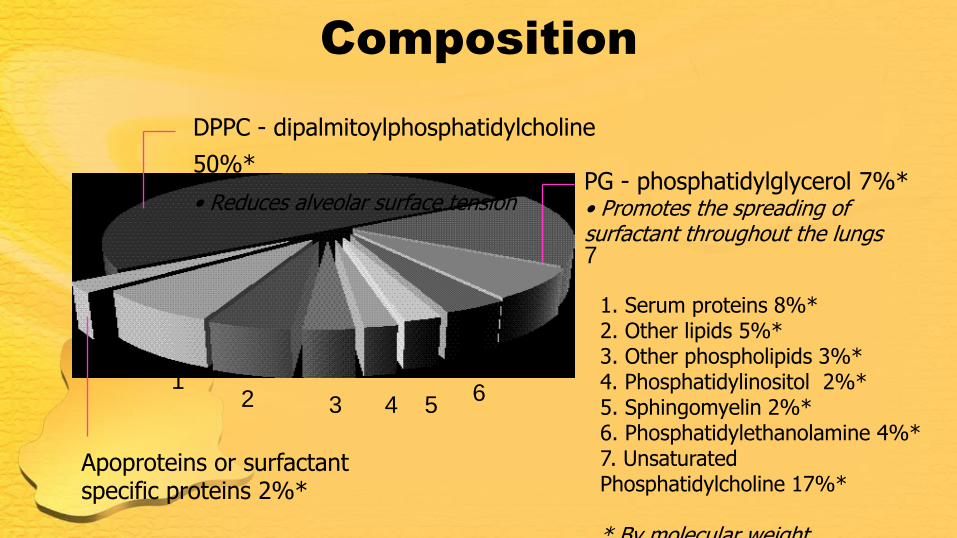
DPPC - dipalmitoylphosphatidylcholine
50%* • Reduces alveolar surface tension
PG - phosphatidylglycerol 7%* • Promotes the spreading of surfactant throughout the lungs
Apoproteins or surfactant specific proteins 2%*
1. Serum proteins 8%* 2. Other lipids 5%* 3. Other phospholipids 3%* 4. Phosphatidylinositol 2%* 5. Sphingomyelin 2%* 6. Phosphatidylethanolamine 4%* 7. Unsaturated Phosphatidylcholine 17%* * By molecular weight
Composition
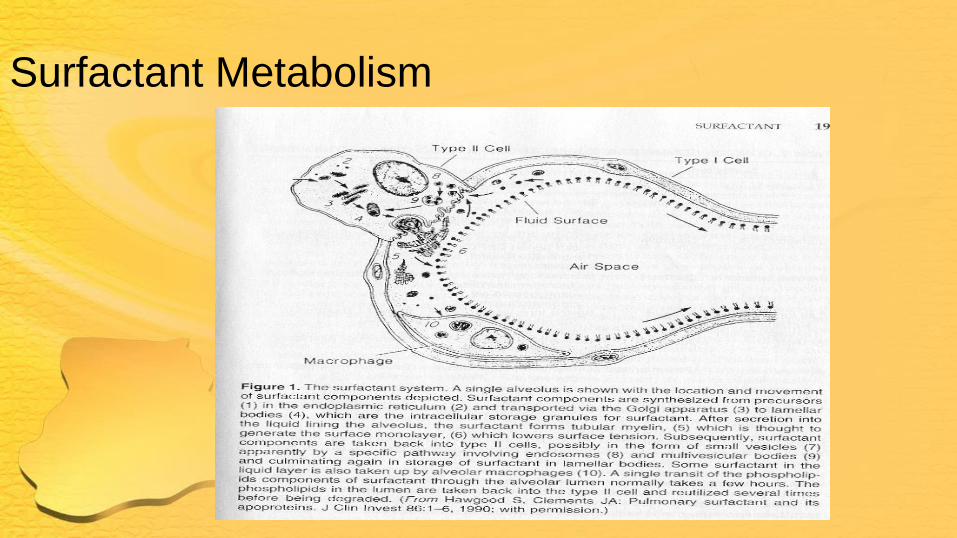
Surfactant: Synthesis and
secretion
• Synthesized within the alveolar type II cells
and stored as lamellar bodies
• Lamellar bodies secreted into alveoli to
contribute to formation of surface film
which reduces surface tension
• Secreted surfactant moves back into type
II cells where it is recycled back into the
cell.
Surfactant Metabolism
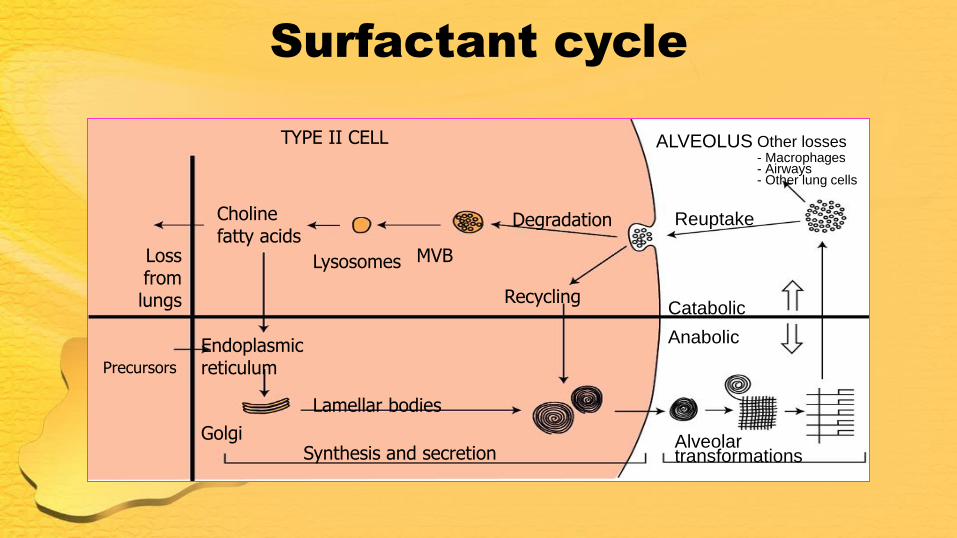
TYPE II CELL
Loss from lungs
Choline fatty acids
Lysosomes MVB
Degradation
Endoplasmic reticulum
Golgi Synthesis and secretion
Lamellar bodies
Recycling
Precursors
Reuptake
Catabolic
Anabolic
Alveolar transformations
ALVEOLUS Other losses - Macrophages - Airways - Other lung cells
Surfactant cycle
Pathophysiology of RDS
• Surfactant deficiency leads to:
• Increased surface tension which leads to
instability of the lung at end-expiration, low lung
volume, decreased compliance
• Hypoxemia due to ventilation-perfusion mismatch
due to atelectasis and intrapulmonary and
extrapulmonary shunts
• Lung inflammation and respiratory epithelial injury
leading to pulmonary edema and increased airway
resistance

where:
P = pressure ST = surface tension r = radius of the
bubble
P = 2ST/r
Laplace’s law

P = 2x1 = 0.2
10
P = 2x1 = 0.4
5
10
5
Connected bubbles
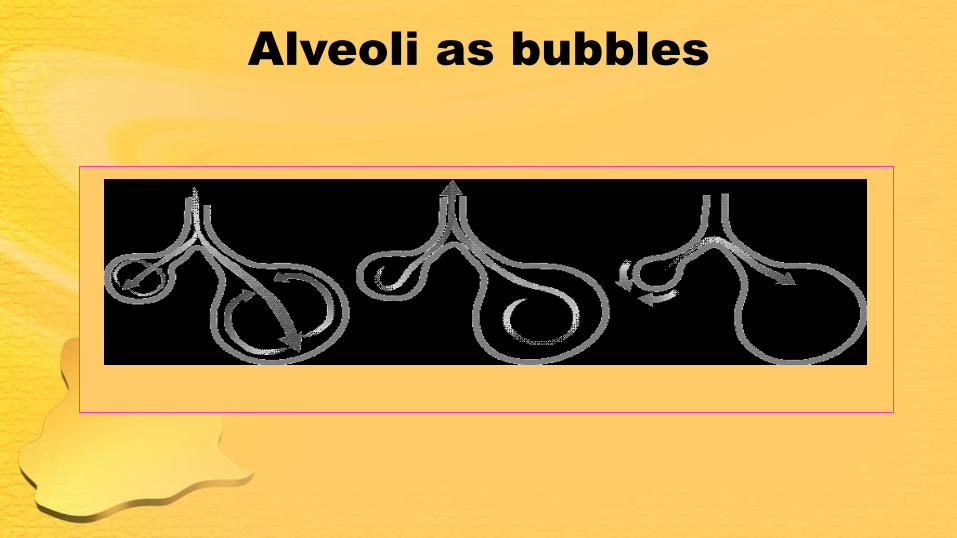
Alveoli as bubbles
Pulmonary Function and Gas
Exchange
• Surfactant deficiency leads to:
• Low compliance and low lung volume
(FRC), and increased lung resistance
• Exogenous surfactant prevents or corrects
these pulmonary functional abnormalities


Surfactant Therapy
• Prior to the introduction of exogenous surfactant RDS was
associated with significant morbidity and mortality
• In a large multicenter blinded controlled trial 789 infants (b
wt 600g -1750g) who developed RDS within 6 hours were
randomly assigned to either placebo or surfactant.
Surfactant was associated with significantly lower mortality
rate (18 vs 27 percent) and a lower risk of developing
pulmonary interstitial emphysema (19 vs 39 percent) and
other pulmonary leak complications including
pneumothorax (12 vs 26 percent).
Properties of surfactant
Rapid adsorption
Efficient spreading
Lower surface tension
Stimulus for release
Gas entering lungs
Alveolar stretch (inspiration)
Adrenergic innervation
Prostaglandins
Hypoxemia
• Hypoxemia in RDS due to:
• Mismatch of ventilation and perfusion
with intrapulmonary shunting
• Extrapulmonary shunting across the
foramen ovale and patent ductus
arteriosus
Diagnosis
• Clinical picture
• Preterm, progressive respiratoy distress
soon after birth, increase oxygen
requirement
• Chest X-ray
• Low lung volume and
reticulogranular groung glass
appearance, air bronchograms


Other lab findings
• Blood gas shows hypoxemia
• Hyponatremia may develop from fluid
retention
Management
• Specific RDS management
• Adequate oxygenation, ventilation, and
possible administration of exogenous
surfactant
• General supportive measures
• Optimize the neonates metabolic and
cardiorespiratory status
Specific RDS Management
• Administration of antenatal corticosteroids
• Administration of exogenous surfactant
• Provision of assisted ventilation

Antenatal Corticosteroid Therapy
• Given to pregnant women at risk of preterm labor to
prevent or decrease the severity of neonatal RDS
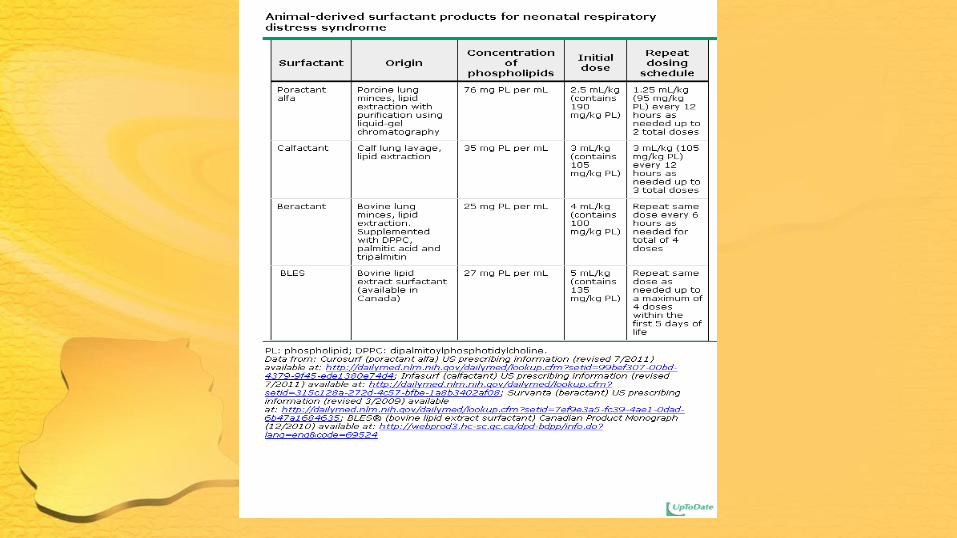
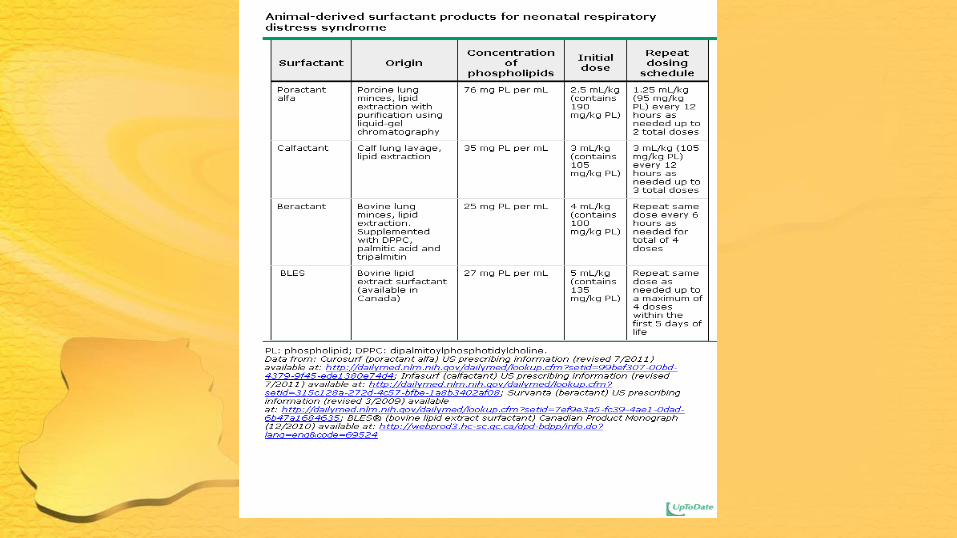
Surfactant Therapy
• Selection of surfactant preparation
• Indications for surfactant therapy
• Timing of administration
• Technical aspects of administration
Selection of Surfactant
• Types of Surfactant
• Natural
• Synthetic
• Lucinactant: first peptide containing surfactant to
be approved by FDA (March 2012)

Indications and Timing for
Surfactant
• Rescue
• Surfactant given when the diagnosis of RDS is established (based on oxygen requirement (paO2< 80 with FiO2 >0.4), clinical examination, chest radiograph).
• Prophylactic (Early therapy)
• Infants <30 weeks
• Continued therapy • Surfactant administered a total 3 or 4 doses based on
continued oxygen needs and the specific surfactant preparation
Surfactant Administration Techniques
• Endotracheal intubation and instillation
surfactant
• Complicated by transient airway
obstruction

Surfactant deficiency - ―vicious cycle‖
Respiratory acidosis
Severe hypoxia
Further inhibition of surfactant by serum proteins
Epithelial damage occurs through suction effect of gasping
Depleted surfactant
Decreased FRC Increased dead space Alveolar collapse
Reduced compliance
Increased work of breathing
Assisted Ventilation Techniques • Continuous Positive Airway Pressure (CPAP)
• Nasal Intermittent Positive Pressure Ventilation (NIPPV)
• Mechanical Ventilation
• Intubation and mechanical ventilation should still be performed in
infants in respiratory failure, verified by one of the following:
respiratory acidosis (pH <7.2), hypoxemia, severe apnea.
Continuous Positive Airway Pressure (CPAP)
• Several studies have shown benefits
• SUPPORT trial in US
• 1316 ELBW 24 to 26 6/7 weeks, randomized to
CPAP or intubation with survanta. No difference
b/n groups re death or BPD
• COIN trial, Australia
• 610 infants 25 to 28 weeks, CPAP or intubation
with ventilation at 5 minutes of age . No difference
b/n groups re death and need for O2 at 36 weeks
GA
CPAP
• VON trial 648 infants GA 26 to 296/7
weeks, no difference in the primary
outcome of combined death or BPD in
CPAP v intubation and prophylactic
surfactant. Both groups did better than
third group with intubation, prophylactic
surfactant and a period of mechanical
ventilation.

CPAP
• These data demonstrate an initial CPAP-
based approach in which surfactant is not
administered is a reasonable option for
preterm infants without respiratory failure.
• Success of this approach may be
enhanced by early onset of caffeine
therapy to increase respiratory drive
Indications for CPAP
• Hypoxemia is the most universally accepted indication for using cPAP (to maintain paO2 > 50-60mmHg)
• To decrease use of mechanical ventilation
• cPAP has a variable effect on CO2
• Optimum cPAP is that at which SaO2 and PaO2 are optimized without adverse effect on cardiac output
CPAP
• CPAP increases lung vol by
• Increasing alveolar size
• Preventing atelectasis
• Recruiting collapsed alveoli
• Increase lung vol increase oxygenation by improving V-Q mismatch
• Makes breathing slower and more regular while grunting generally ceases

The CPAP delivery system consists of three components:
the circuit for continuous flow of inspired gases, the interface connecting the CPAP circuit to the
infant’s airway, and a method of creating positive pressure in the CPAP circuit.
CPAP Delivery Systems
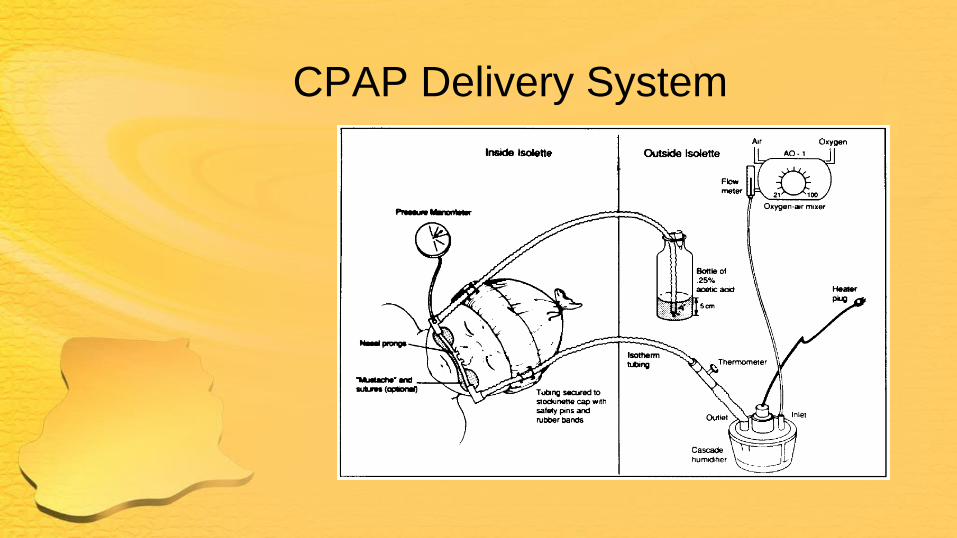
CPAP Delivery System
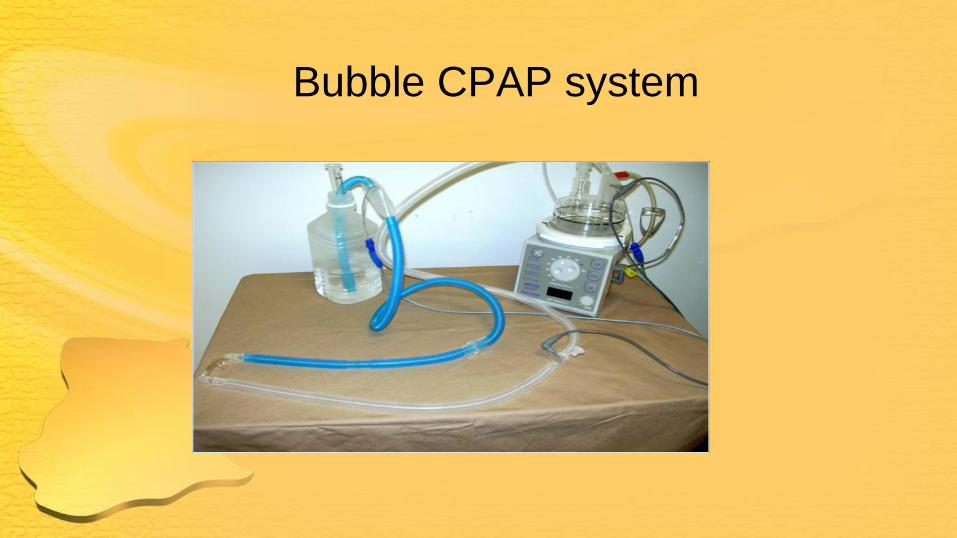
Bubble CPAP system
Techniques- Interface
• Nasal prongs
• ET tube
• Face mask
• Nasal mask
Problems with cPAP
• Local
• mucosal necrosis
• Overdistension leading to decreased
venous return, decreased cardiac output
and decreased oxygen transport
Care of babies on CPAP
• Interface care
• Humidification
• Suctioning
• Gastric decompression
• Monitoring
Initiating CPAP
• Start with PEEP of 5 cm H2O pressure, flow
5-10 lpm, FiO2 0.40-0.60
• Increase pressure in steps of 1-2 cm H2O till
8 depending on resp effort and PO2.
Weaning of CPAP
• Wean by decreasing FiO2 in
steps of 0.05 till 0.40, then
wean CPAP in steps of 1-2 cm
H2O till 4-5, then discontinue.
CPAP….Advantages
• Less Invasive than mechanical ventilation
• Less barotrauma
• Early Lung recruitment in RDS
• Helpful in management of Obstructive and
Mixed apnea

CPAP
• Problems:
• High CPAP may decrease venous return
• High CPAP may decrease minute ventilation
• Abdominal distension, open mouth, crying

Disadvantages
• CPAP does not improve ventilation, High pressures may worsen it
• Technically difficult to maintain in large active infants
• Inadequate in severe changes in Pulm Resistance and compliance
• Swallowed air causes elevation of the diaphragm
How is CPAP given…
• CPAP mode on a conventional ventilator
• Manually- anesthesia bag, T- Piece
resuscitator
• CPAP machines
• Bubble CPAP
Nasal Intermittent Positive Pressure
Ventilation
• Augments CPAP by delivering ventilator
breaths via nasal prongs (or nasal mask)
• Metaanalysis from 3 clinical trials suggest
infants treated with NIPPV less likely than
infants treated with CPAP to require
mechanical ventilation at 72 hours
History of Assisted Ventilation
Elisha was come into the house, Behold
the child was dead… he went up and lay
upon the child and put his mouth upon his
mouth …. Stretched himself upon the
child and the flesh of the child waxed
warm
Mechanical Ventilation
• Several modalities:
• Pressure control
• Volume control
• High Frequency Ventilation
• Regardless of choice of ventilator, goal is to use
settings that minimize volutrauma, barotrauma and
oxygen toxicity, thereby reducing the risk of BPD

Complications of Mechanical
Ventilation
• Endotracheal tube complications
• Pulmonary air leak
• Bronchopulmonary Dysplasia
Target oxygen saturation and pCO2 levels
• Oxygen saturation—A range of oxygen
saturation so that bothe hypoxia and the
excess use of oxygen can be avoided.
• paCO2 levels– In preterm infants target 45
to 60mmHg to keep pH above 7.25

Supportive Care
• Thermoregulation
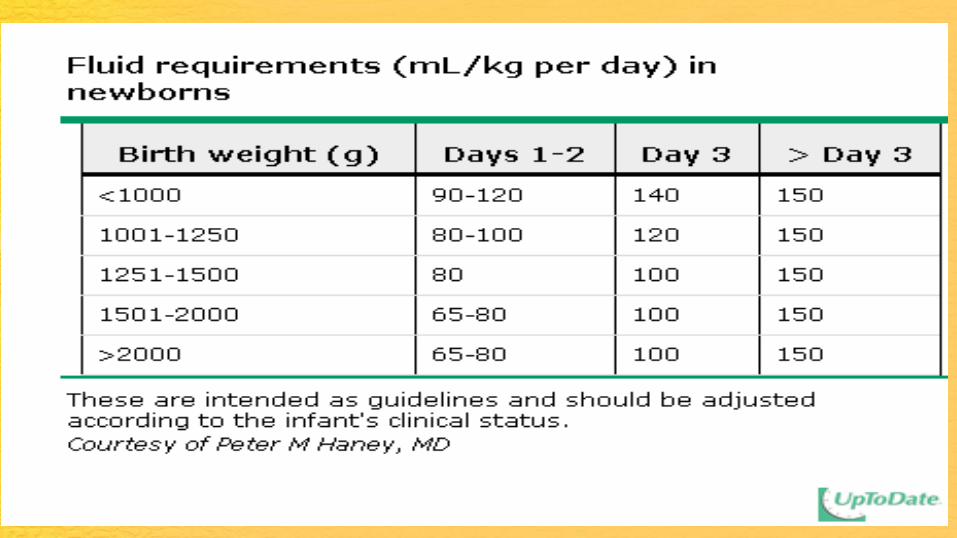
• Fluid management
• Cardiovascular management
• Nutrition
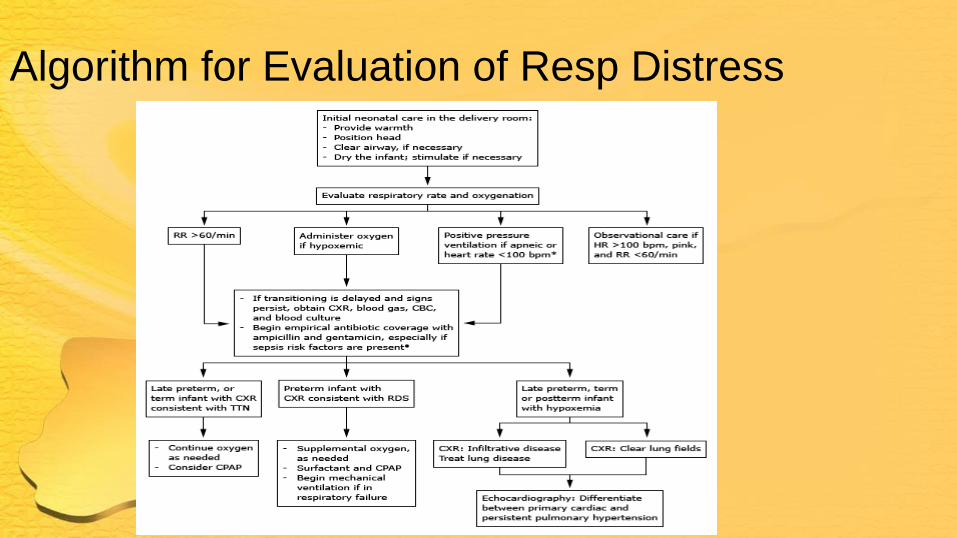
Algorithm for Evaluation of Resp Distress
Prevention of Respiratory Distress
Syndrome
• Since RDS is due to lung immaturity, the
best prevention is to prevent premature
birth. Potential therapies include:
• Cervical cerclage, use of tocolytic
agents, prevention and treatment of
infections
Prevention of RDS
• If premature birth can’t be prevented
• Antenatal corticosteroids to accelerate
fetal lung maturation and surfactant
production
• Use of exogenous surfactant

Voice mail in Heaven • Imagine praying
and hearing the following: Thank you for calling Heaven. For English, Press 1. For Spanish, press 2. For all other languages, press 0. Please select one of the following options: Press 1 for Requests. Press 2 for Thanksgiving. Press 3 for Complaints. Press 4 for all other inquiries.

Voice mail in Heaven
• I am sorry. All of our angels and saints are busy helping
other sinners right now. However, your prayer is important
to us, and we will answer it in the order it was received.
Please stay on the line.
• If you would like to hear King David sing a Psalm while
you are holding, press 1.
Voice mail in Heaven • For reservations at Heaven, please enter J-O-H-N, followed by
the numbers 3-1-6. If you receive a negative response, please hang up and try area code 666.
• For answers to nagging questions about dinosaurs, the age of the earth, life on other planets, and where Noah's Ark is, please wait until you arrive. Our computers show that you have already prayed today. Please hang-up and try again tomorrow.
• The office is now closed for the weekend to observe a religious holiday. Please pray again on Monday after 9:30 am.
• If you are calling after hours and need emergency assistance, please contact your local pastor.
• If this is a true emergency hang up and dial 911
• Thank you and have a heavenly day









![RESPIRATORY SCORE (RS) }µv }Híì] v · RS 1-4 Discharge Urgent Care Transfer Criteria · Score >8 following first hour of nebulized albuterol- send by ALS · Score 5-8 following](https://static.fdocuments.in/doc/165x107/5e18e2189f8e6e77fe4d999f/respiratory-score-rs-v-h-v-rs-1-4-discharge-urgent-care-transfer-criteria.jpg)





