Management of mucopolysaccharidosis type · The mucopolysaccharidoses are a group of inherited...
4
Archives of Disease in Childhood 1993; 69: 403-406 PERSONAL PRACTICE Management of mucopolysaccharidosis type III M A Cleary, J E Wraith The mucopolysaccharidoses are a group of inherited metabolic disorders caused by a deficiency of specific lysosomal enzymes. The enzyme deficiency results in interference with cellular function because of excessive accumulation within the cells of partially degraded glycosaminoglycans, which are also excreted to excess in the urine of affected patients.' Mucopolysaccharidosis (MPS) type III, or Sanfilippo's syndrome,2 is characterised by the accumulation and urinary excretion of partially degraded heparan sulphate. At least four different enzyme deficiencies are known to cause the disorder.' Clinically the syndrome is characterised by a mild somatic phenotype combined with a severe neurodegenerative illness with promi- nent behavioural disturbance. Previous large clinical reviews of this condition have included many patients from small geographical areas and may not be representative of the complete clinical spectrum.3 4 We present the clinical details of the 62 patients attending the special clinic for mucopolysaccharidoses at the Willink Biochemical Genetics Unit highlighting the particular problems associated with the clinical diagnosis and management of the disorder. Patients The clinical type and enzyme deficiency of the patients is shown in table 1. In the United Kingdom MPS IIIA is the commonest of the mucopolysaccharidoses, the exact incidence is not known with certainty, but is probably between 1:20-25 000 live births. This may be an underestimate as a number of mildly affected patients will remain undiagnosed. Type B is less common, type C is rare, and no patients with type D attend the clinic. Although the numbers involved are small, we were not able to confirm the previously reported milder clinical course associated with MPS IIIB.5 There appeared to be no significant clinical differences between the different subtypes. Presenting features Accurate details about pregnancy and delivery were obtained for 59 of the 62 children. Three pregnancies ended prematurely at 28, 34, and 36 weeks' gestation, the infants having appropriate birth weights for the period of gestation. The other 56 pregnancies resulted in infants of normal birth weight with a mean of 3400 g and a range of 2700-4700 g. Delivery was normal in 46 cases, six followed forceps extraction, and seven were the result of caesarean section. For the majority of infants the neonatal period was uneventful (excluding those born prematurely). One patient required ventilation for meconium aspiration, but made normal progress subsequently. Five other patients were nursed briefly in the special care baby unit because of transient respiratory or feeding difficulties. The mean age at diagnosis was 4 9 years with a range from 0-8-16 years. In six children a presymptomatic diagnosis was made after establishing the diagnosis in an older sibling. The features present at diagnosis of all the patients are shown in table 2. Most patients had a combination of developmental delay, particularly speech, and recurrent ear, nose, and throat infections. Hearing difficulties were common and a number of patients had failed health visitor screening hearing assessments. Troublesome diarrhoea was a particular problem in 36 patients. The nature of the bowel disturbance was episodic, severe, watery motions that did not usually lead to dehydra- tion, although many patients were admitted to hospital with a presumptive diagnosis of 'gastroenteritis'. In three patients this symptom was severe enough to lead to investi- gation to exclude serious bowel pathology, including sweat test and jejunal biopsy. In one patient a diagnosis of 'multiple food allergy' Willink Biochemical Genetics Unit, Royal Manchester Children's Hospital, Manchester M27 IHA M A Cleary J E Wraith Correspondence to: Dr Wraith. Table 1 Clinical type and enzyme deficiency ofpatients studied MPS III type A B C D Enzyme deficiency Heparan N-sulphatase a-N-acetylglucosaminidase Acetyl-CoA: a-glucosaminide acetyltransferase N-acetylglucosamine-6-sulphatase No of patients Development delay 47 Speech delay 12 Recurrent ear, nose, and throat infections 3 Diarrhoea Behaviour problems 0 Hearing loss Table 2 Presenting features in 62 patients No of Symptom panents 58 53 49 36 34 16 403 4 on October 13, 2020 by guest. Protected by copyright. http://adc.bmj.com/ Arch Dis Child: first published as 10.1136/adc.69.3.403 on 1 September 1993. Downloaded from
Transcript of Management of mucopolysaccharidosis type · The mucopolysaccharidoses are a group of inherited...

Archives of Disease in Childhood 1993; 69: 403-406
PERSONAL PRACTICE
Management of mucopolysaccharidosis type III
M A Cleary, J E Wraith
The mucopolysaccharidoses are a group ofinherited metabolic disorders caused by adeficiency of specific lysosomal enzymes. Theenzyme deficiency results in interferencewith cellular function because of excessiveaccumulation within the cells of partiallydegraded glycosaminoglycans, which are alsoexcreted to excess in the urine of affectedpatients.' Mucopolysaccharidosis (MPS) typeIII, or Sanfilippo's syndrome,2 is characterisedby the accumulation and urinary excretion ofpartially degraded heparan sulphate. At leastfour different enzyme deficiencies are knownto cause the disorder.'
Clinically the syndrome is characterised by amild somatic phenotype combined with asevere neurodegenerative illness with promi-nent behavioural disturbance. Previous largeclinical reviews of this condition have includedmany patients from small geographical areasand may not be representative of the completeclinical spectrum.3 4We present the clinical details of the
62 patients attending the special clinicfor mucopolysaccharidoses at the WillinkBiochemical Genetics Unit highlighting theparticular problems associated with the clinicaldiagnosis and management of the disorder.
PatientsThe clinical type and enzyme deficiency of thepatients is shown in table 1. In the UnitedKingdom MPS IIIA is the commonest of themucopolysaccharidoses, the exact incidenceis not known with certainty, but is probablybetween 1:20-25 000 live births. This may bean underestimate as a number of mildlyaffected patients will remain undiagnosed.Type B is less common, type C is rare, and nopatients with type D attend the clinic.Although the numbers involved are small, wewere not able to confirm the previouslyreported milder clinical course associatedwith MPS IIIB.5 There appeared to be no
significant clinical differences between thedifferent subtypes.
Presenting featuresAccurate details about pregnancy and deliverywere obtained for 59 of the 62 children. Threepregnancies ended prematurely at 28, 34, and36 weeks' gestation, the infants havingappropriate birth weights for the period ofgestation. The other 56 pregnancies resulted ininfants of normal birth weight with a mean of3400 g and a range of 2700-4700 g. Deliverywas normal in 46 cases, six followed forcepsextraction, and seven were the result ofcaesarean section. For the majority of infantsthe neonatal period was uneventful (excludingthose born prematurely). One patient requiredventilation for meconium aspiration, but madenormal progress subsequently. Five otherpatients were nursed briefly in the special carebaby unit because of transient respiratory orfeeding difficulties.The mean age at diagnosis was 4 9 years
with a range from 0-8-16 years. In six childrena presymptomatic diagnosis was made afterestablishing the diagnosis in an older sibling.The features present at diagnosis of all thepatients are shown in table 2. Most patientshad a combination of developmental delay,particularly speech, and recurrent ear, nose,and throat infections. Hearing difficulties werecommon and a number of patients had failedhealth visitor screening hearing assessments.
Troublesome diarrhoea was a particularproblem in 36 patients. The nature of thebowel disturbance was episodic, severe, waterymotions that did not usually lead to dehydra-tion, although many patients were admittedto hospital with a presumptive diagnosisof 'gastroenteritis'. In three patients thissymptom was severe enough to lead to investi-gation to exclude serious bowel pathology,including sweat test and jejunal biopsy. In onepatient a diagnosis of 'multiple food allergy'
Willink BiochemicalGenetics Unit, RoyalManchester Children'sHospital, ManchesterM27 IHAMA ClearyJ E Wraith
Correspondence to:Dr Wraith.
Table 1 Clinical type and enzyme deficiency ofpatientsstudied
MPS IIItype
ABC
D
Enzyme deficiency
Heparan N-sulphatasea-N-acetylglucosaminidaseAcetyl-CoA: a-glucosaminide
acetyltransferaseN-acetylglucosamine-6-sulphatase
No ofpatients
Development delay47 Speech delay12 Recurrent ear, nose, and throat infections3 Diarrhoea
Behaviour problems0 Hearing loss
Table 2 Presentingfeatures in 62 patients
No ofSymptom panents
585349363416
403
4
on October 13, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.69.3.403 on 1 S
eptember 1993. D
ownloaded from

Cleary, Wraith
was made until the extravagant behaviouraldisturbance led to a reconsideration of theprimary pathology. One patient was treatedwith pancreatic supplements for many monthswithout appreciable affect on the bowelproblem.Twenty six patients had various ear, nose,
and throat procedures performed beforediagnosis. In a number of children multiplegrommet insertions were felt to be necessary.
Unlike the other mucopolysaccharidoseshernias were uncommon and were presentin only five children (three inguinal, twoumbilical). Five children were noted to have ahead circumference above the 90th centile (ofthese one was mistakenly diagnosed as Soto'ssyndrome) and only two had significanthepatomegaly at presentation.
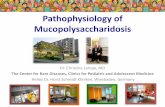
Evolution of the phenotypeSOMATIC ABNORMALITIES (FIGS 1-3)The clinical picture is dominated by the severeneurological disturbance, but a number ofchildren develop other important physicalsigns. A coarse facial appearance develops latein the disorder, if at all, in most patients (fig 1).Stature is not significantly affected and thegood physical growth associated with thebehavioural disturbance accentuates themanagement difficulties. The exceptions areinfants of Asian origin who are often verydysmorphic and hirsute despite having similarlevels of residual enzyme activity (fig 2).Clinical examination in these infants oftenleads to a mistaken diagnosis of MPS I or II,emphasising the need for biochemicalconfirmation of diagnosis in all patients.
..._ _ .c. .
Figure 2 A child ofAsian origin with MPS IIIdemonstrating the coarse facial phenotype often associatedwith this ethnic group.
Cardiac abnormalities are rare. An abnormalechocardiogram was found in five patients, oneof whom had coincidental dextrocardia. Onlyone patient had a severe cardiac lesion (hyper-trophic cardiomyopathy) leading to early death.This patient with type B disease, fromconsanguineous Pakistani parents, had a verysevere dysmorphic phenotype.
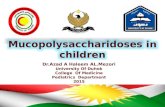
Skeletal disease is mild, but a number ofpatients develop dysplastic hip and pelvicchanges that can be seen on radiography (fig 3).This may be associated with apparent pain andstiffness and often a diagnosis of 'Perthe'sdisease' is made, although the relationshipbetween this condition and MPS III is not clear.
NEUROPSYCHIATRIC ABNORMALITIESThese can be clearly divided into three phases.Firstly, between the ages of 1 and 4 years theclinical pattern is usually one of developmentaldelay alone. In a number of children otherfeatures such as recurrent ear, nose, and throat
Figure 3 Radiograph of hips and pelvis of 6 year old childwith MPS IIIA.
Figure I A white child with MPS III demonstrating anormalfacial appearance.
404
on October 13, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.69.3.403 on 1 S
eptember 1993. D
ownloaded from

Management of mucopolysaccharidosis type III
disease or bowel disturbance may dominate theclinical picture. The lack of somatic abnor-mality typical of mucopolysaccharidoses at thisage means that this diagnosis is not usuallyconsidered. In most patients the developmentalproblems are most noticeable with regard tolanguage development. Gross motor milestonesare usually achieved, though these may bedelayed. Fifty per cent of the affected childrennever completed toilet training.The second phase of the illness, which most
commonly begins around the ages of 3-4, ischaracterised by severe behavioural disturb-ance. The normal growth and good muscularstrength of affected patients makes this phaseof the condition the most difficult to manage.Characteristically the pattern of behaviour isheralded by increasingly frequent and severe
temper tantrums. This is often followed byincreasing hyperactivity and a rapid dimi-nution in attention span. Aggression iscommon and many children are destructive.Panic attacks when placed in a strangeenvironment, such as the consulting room, are
usual. During this phase sleep is often severelydisturbed and in some patients a reversal of thenormal sleep pattern occurs. Some childrenappear to hallucinate at night, which leads tofurther behavioural disturbance and oftenconsiderable personal distress.From the age of about 10 years the nature of
the illness changes again as the children enterthe third and final stage. During this quieterphase frequent falls are common as balance islost. Feeding difficulties due to an impairedswallowing mechanism result in increasingepisodes of aspiration and feed consistency hasto be altered. Ultimately most children requirea nasogastric tube to obtain adequate energyintake. Aspiration of saliva continues to be a
problem for many children and requiresseparate treatment (see later).
Increasing spasticity combined with jointstiffness from the connective tissue deteriora-tion severely impairs mobility and mostchildren are wheelchair bound by their midteenage years. Seizures can become trouble-some during this phase. Of the patientsattending the clinic, 16 developed seizuresmost commonly after the age of 8 years. Theseizure type was generalised, tonic-clonic in allcases, although a mixed seizure type withpartial seizures was noted in some.The disorder, in common with most genetic
conditions, exhibits marked heterogeneity anda number of children did not adhere to theclinical description above, in particular fourpatients are still independently mobile at ages18, 20, 23, and 28 years.
ManagementIn the first phase of the illness attention to ear,nose, and throat problems is necessary.Unlike other mucopolysaccharidoses6 themilder somatic phenotype in MPS III means amuch reduced anaesthetic risk and in ourseries many ofthe children underwent multipleoperative procedures with no anaestheticcomplications.
Special educational assessment becomesessential after diagnosis and in patients whohave recurrent episodes of diarrhoea improvedcontrol can be achieved by the use ofloperamide hydrochloride, 1-2 mg, up to fourtimes a day.Management during the second phase of the
illness is extremely difficult. An approach totreatment should consider the following aspects.
SLEEP DISTURBANCEMost affected children sleep poorly. The onsetof sleep appears to be resisted and onceachieved is disturbed frequently throughoutthe night. This produces additional parentalstrain as they try during the day to cope withthe hyperactivity and aggressive behaviour.Hypnotic medication has a variable effect andoften has to be used in high dosage in attemptsto remedy this problem. Drug regimens thathave had some limited success include acombination of chloral hydrate (500-1000 mgper single dose) and trimeprazine tartrate (2-3mg kg per dose). In some children thisproduces paradoxical overactivity and inothers rebound sedation the next day.Benzodiazepines such as temazepam (5-20mg) or nitrazepam (5-10 mg) can be success-ful, but more often induce rebound sedationthe next day.Many parents use physical restraint at night
utilising an elastic bed belt.* This allows thechild freedom of movement within the bed,but prevents the child from getting out of bed.In some instances this has led to an improvedsleep pattern. The parents sleep betterknowing that the child is unable to get up andcome to harm within the bedroom.
DAYTIME BEHAVIOURThe aggression and hyperactivity respondpoorly to a behavioural approach to treatment.A disciplined environment, such as within asmall group at school, may lead to a temporaryimprovement in behaviour within that setting,but offers little practical help for the home.Drug treatment and alteration to the physicalenvironment within the home have been mostsuccessful in allowing the family to functionas near normal as possible. Most familiesendeavour to create a 'safe environment' forthe affected child. This includes softfurnishings, toughened glass on doors andwindows, wall padding, safety gates on stairs,and the removal of fragile articles. Earlyconsideration of alterations necessary toprovide for a severely physically handicappedchild such as downstairs bedroom andbathroom accommodation are also important.Drug treatment aimed at controlling the
hyperactivity and aggression is necessary toallow many families to cope. The response tosuch treatment is very unpredictable andparents should be warned that a temporaryworsening of behaviour may follow the
*Segufix Bed-Harness System, Segufix-Bandsagen DasHumane System, PO Box 50 1364, D2000 Hamburg 50,Federal Republic of Germany.
405
on October 13, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.69.3.403 on 1 S
eptember 1993. D
ownloaded from

Cleary, Wraith
introduction of any antipsychotic agent.Thioridazine hydrochloride, starting with asmall dose (1 2 5 mg twice a day) and graduallyincreasing over a period of 2-4 weeks to amaximum of 200 mg/day has been the mosteffective agent in our clinic. Haloperidol (0.25mg twice a day increasing slowly to a maxi-mum of 10 mg/day depending on effect) canalso be useful. Extrapyramidal side effects aremore common in children and particularlyif the dose exceeds 10-15 mg/day.Chlorpromazine hydrochloride has not been asuccessful product in our clinic tending toinduce a combination of oversedationinterspersed with periods of excitability. A lesssatisfactory approach to drug treatment is tosedate during the day with benzodiazepines.
RESPITE CAREAt best, drug treatment is only partiallysuccessful and early consideration must begiven to respite care. The parents requireadequate periods of rest to cope with thechildren and this usually involves organisedbreaks away from home. The availabilityof suitable respite accommodation variestremendously throughout the country.
During the third and final stages of thedisorder the child's behaviour becomes easierto manage due to increasing immobility.Different problems assume prominence andfeeding difficulties as a result of swallowingincoordination begin in many patients in earlyteenage life. Food has to be progressivelyliquidised and episodes of aspiration and nasalregurgitation become more common. Aninability to swallow saliva with constantchoking heralds the need for nasogastric tubefeeding combined with medication to inhibitsaliva production. The most successfulmedications are hyoscine patches (placedbehind the ear and replaced every three days)and benztropine mesylate (0.25 mg twice a dayincreasing slowly to a maximum of 1.5 mgtwice a day depending on response).
Increasing spasticity and joint stiffness leadto a wheelchair existence for many patients.Baclofen has not proved to be very successfulin treating the progressive muscle stiffness, butbenzodiazepines can often control painfulspontaneous muscle spasms. Many parentshave used non-steroidal anti-inflammatoryagents to alleviate joint stiffness, but there islittle evidence of therapeutic benefit.
It is often very difficult to assess the degreeofpain experienced by the affected child in thisstage of the illness. Episodes of mood swingwith bouts of crying are very common. Mostoften there does not appear to be an underlyingpainful process responsible for these attacksand parents need to be reassured about theirbehavioural origin.
Seizures can be troublesome, but mostrespond to appropriate anticonvulsant medica-tion. Very occasionally an unusual seizurepattern develops, such as nocturnal bouts oflaughing or 'panting'.
General physical health and strengthdeteriorates with age and many childrenbecome wasted despite adequate energyintake. Death most commonly occurs in mid tolate teenage years usually as a result of arespiratory infection complicating the severedebility. Unlike other mucopolysaccharidoses,cardiac function is preserved until very late inthe illness.The Society for Mucopolysaccharidoses
Diseases has provided tremendous support formany families with affected children.t
Other possible treatmentsBone marrow transplantation has beenattempted as a form of enzyme replacement in afew patients with MPS III. As with MPS I,biochemical correction is readily achieved, butthe results regarding intellectual outcome havebeen disappointing.7 Transplantation has beenperformed on two ofour patients. In one patientlate rejection of the graft occurred 12 monthsafter transplantation that was first performedat age 14 months. Retransplantation wasperformed but the child, now aged 4 years,shows clear evidence of developmental delay aswell as some of the behavioural disturbancetypical ofthe syndrome. The second patient wastransplanted at age 10 months and at age 2years has shown no evidence of deterioration,although this would not be expected in such ayoung child. A longer period of observation isnecessary before one can judge the results oftransplant in this patient.
It is important to remember that all of theMPS III subtypes are inherited as autosomalrecessive and that first trimester prenataldiagnosis should be possible.'
1 Neufeld EF, Muenzer J. The mucopolysaccharidoses. In:Scriver CR, Beaudet AL, Sly WS, Valle D, eds. Themetabolic basis of inherited disease. New York: McGraw-Hill,1989: 1565-87.
2 Sanfilippo SJ, Podosin R, Langer L, Good RA. Mentalretardation associated with acid mucopolysacchariduria(heparitin sulfate type). I Pediatr 1963; 63: 837-8.
3 Van de Kamp JJP, Niermeijer MF, Von Figura K, GiesbertsMA. Genetic heterogeneity and clinical variability in theSanfilippo syndrome (types A, B, and C). Clin Genet 1981;20: 152-60.
4 Wraith JE, Rogers JG, Danks DM. The mucopolysacchari-doses. Australian Paediatric Journal 1987; 23: 329-34.
5 Van Schrojenstein-de Valk HMG, Van de Kamp JJP.Follow-up on seven adult patients with mild SanfilippoB-disease. Am JMed Genet 1987; 28: 125-9.
6 Herrick IA, Rhine EJ. The mucopolysaccharidoses andanaesthesia: a report of clinical experience. Can J Anaesth1988; 35: 67-73.
7 Hoogerbrugge PM, Brouwer OF, Fischer A. Bone marrowtransplantation for metabolic diseases with severe neuro-logical symptoms. Bone Marrow Transplant 1991; 7 (suppl2): 71.
tThe Society for Mucopolysaccharide Diseases, 55 HillAvenue, Amersham, Bucks HP6 5BX.
406
on October 13, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.69.3.403 on 1 S
eptember 1993. D
ownloaded from