Management of Hypertention
33
1 THE DYNAMIC OF MANAGEMENT THE DYNAMIC OF MANAGEMENT OF HYPERTENSION OF HYPERTENSION
-
Upload
anita-amanda-prayogi -
Category
Documents
-
view
221 -
download
2
description
laaaaaaaaaaaaaaaaaaaaa
Transcript of Management of Hypertention
-
THE DYNAMIC OF MANAGEMENT OF HYPERTENSION
-
Lifetime Risk of HypertensionHypertension is an increasingly important medical and public health issue.
The prevalence of hypertension increases with advancing age, to the point where affecting : 50% of people aged 60 - 69 yrs old 75% of those aged 70 yrs and older
Burt, et al. Hypertension. 1995
-
Update in hypertensionGlobal mortality 2000: impact of hypertension and other health risk factorsAdapted from Ezzati et al, Lancet, 2002.
-
Prevalence of high blood pressure, 140/90 mm Hg, rises with ageUS 1988-91NHANES3, Burt et al 1995
-
Prevalence of high blood pressure, 140/90 mm Hg, rises with ageUS 1988-91NHANES3, Burt et al 1995
-
Definition of HypertensionWHO-ISH definitions CategoryBlood Pressure (mm Hg)SystolicDiastolic
Optimal< 120< 80Normal< 130< 85High-normal130 13985 89Grade 1 hypertension (mild)140 15990 99Subgroup : borderline140 14990 94Grade 2 hypertension (moderate)160 179100 109Grade 3 hypertension (severe) 180 110ISH 140< 90Subgroup : borderline140 149< 90Adapted from Guidelines Subcommittee. J. Hypertens. 1999:17:151-183
-
Definition and classification of blood pressure levels (mm Hg)
CategorySystolicDiastolic
Optimal< 120< 80Normal120 - 12980 - 84High-normal130 13985 89Grade 1 hypertension (mild)140 15990 99Grade 2 hypertension (moderate)160 179100 109Grade 3 hypertension (severe) 180 110ISH 140< 90When a patients systolic and diastolic blood pressures fall into different categories, the higher category should apply, Isolated systolic hypertension can also be gradeed (grades 1, 2, 3) according to systolic blood pressure values in the ranges indicated, provided diastolic values are < 90.ESC/ESH 2003
-
Classification of blood pressure levels of the British Hypertension Society CategorySystolicDiastolic
Optimal< 120< 80Normal< 130< 85High-normal130 13985 89HypertensionGrade 1 (mild)140 15990 99Grade 2 (moderate)160 179100 109Grade 3 (severe) 180 110Isolated Systolic HypertensionGrade 1 140 149< 90Grade 2 160< 90Brit Med J 2004 : 328 : 634 - 40
-
Blood Pressure Classification160Stage 2 HypertensionDBP mmHgSBP mmHgBP ClassificationJNC 7 2003
-
THE JOINT NATIONAL COMMITTEE FOR THE DETECTION, EVALUATION AND TREATMENT OF HIGH BLOOD PRESSUREJNC 1 1977JNC 21980JNC 31984JNC 41988JNC 51993JNC 61997JNC 72003WHO-ISH GUIDELINES 1984
WHO-ISH GUIDELINES 1999
WHO-ISH GUIDELINES 2003
-
Definition and classification of blood pressure levels (mm Hg)CategorySystolicDiastolic
Normal< 120< 80High-normal120 13980 89Grade 1 (mild)140 15990 99Grade 2 (moderate)160 179100 109Grade 3 (severe) 180 110Isolated systolic hypertension 140< 90AUSTRALIA 2003
-
Hypertension Risk- Aortic and other Arterial aneurysm- Peripheral arterial Disease- Coronary Artery disease- Heart Failure- Ventricular hypertrophy- Ventricular systolic dysfunction- Hypertensive retinopathy- Fundal hemorrhages- Papilooedema- Cerebrovascular Disease- Dimentia- Renal impairment- End Stage Renal Disease- ProteinuriaTarget OrganDemageModified from:Campbell, et al. CMAJ 2002Williams B, et al. BMJ 2004
-
Hypertension RiskHypertension most important modifiable risk facto for:Coronary heart disease, stroke, congestive heart failure, end-stage renal disease, and peripheral vascular disease.Ogden LG, et al. Hypertension. 2000
-
Metabolic syndromeIts More Than Just Blood PressureDecreased Arterial ComplianceEndothelial DysfunctionAbnormal Glucose MetabolismNeurohormonal DysfunctionRenal-Function ChangesBlood-Clotting Mechanism ChangesObesityAbnormal Insulin MetabolismLV Hypertrophy and DysfunctionAccelerated AtherogenesisAbnormal Lipid MetabolismHypertensionKannel WB. JAMA. 1996;275:1571-1576. Weber MA et al. J Hum Hypertens. 1991;5:417-423. Dzau VJ et al. J Cardiovasc Pharmacol. 1993;21(suppl 1):S1-S5.
-
Management of Hypertension
The main objective in lowering BP is to reduce the patients absolute risk of premature death and disease, primarily by reducing their risk of cardiovascular diseases.
Ogden LG,et al. Hypertension. 2000
-
Hypertension Management : JNC 7All people with hypertension should be treatedPrehypertensive require health promoting lifestyleWeight loss and sodium reduction feasible and effective interventionGoal for hypertension without compelling condition is < 140 / 90 mm HgGoal for patients with diabetes and chronic renal diseases is < 130 / 80 mm Hg
-
Goals of treatmentJNC VII ( 2003 ) : @ < 140 / 90 mmHg or < 130 / 80 mmHg for those with Diabetes or Chronic Kidney disease. @ Achieve SBP goal especially in persons >50 years of age.
ESH ( 2003 ) : @ At least below 140 / 90 mmHg ( lower values if tolerated )@ Below 130 / 80 mmHg in Diabetics.@ Keeping in mind, however, that systolic below 140 mmHg may be difficult to achieved in elderly( more flexible )
-
BLOOD PRESSURE GOAL:
UNCOMPLICATED: 1G/DAY:
-
Classes of antihypertensive drugs
-
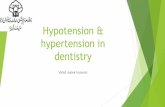
Development of Antihypertensive TherapiesDirect vasodilatorsAlpha blockersOthers?Peripheral sympatholyticsGanglion blockersVeratrum alkaloidsCentral alpha2 agonistsNon-DHP CCBsBeta blockersThiazide diureticsDHP CCBsARBsACE inhibitorsEffectivenessTolerability1940s195019571960s1970s1980s1990s2004+DHP, dihydropyridine; CCB, calcium channel blocker; ARB, angiotensin II receptor blocker.
-
THE STEPPED-APPROACH OF THE JOINT NATIONAL COMMITTEE FOR THE DETECTION, EVALUATION AND TREATMENT OF HIGH BLOOD PRESSURESTEP 1: Start all ambulatory patients with adiuretic antihypertensive agent. Usually a thiazideor thiazide-like agent.STEP 2: If insufficient response to full dosis in four weeks, add one of the following : - Clonidine - methyldopa - prazosine - propranolol - rauwolfia alkaloidSTEP 3: If insufficient response to two drugs, add an oral vasodilatoras the third agent, hydralazineSTEP 4 : If still an inadequate response, add substitute guanethidineJAMA 237(3): 255 1977
- Algorithm for Treatment of HypertensionNot at Goal Blood Pressure (
-
Compelling Indication for Individual Drug ClassesChobanian AV, JNC VII, Hypertension. 2003JNC 7
Compelling indicationRecommended DrugsDiureticBBACEIARBCCBAldo ANTHeart failureXXXXXPost-myocardial infarctionXXXHigh coronary riskXXXXDiabetesXXXXXChronic renal diseaseXXRecurrent stroke preventionXX
-
Hypertension Management
-
The ABCD system for choosing antihypertensive therapyOne drugYoungerNon blackOlder blackABCDororTwo drugsABorCDorThree drugsABorCDA = ACEI or ARBC = CCBB = Beta blockerD = Diuretic (thiazide)
-
DiureticsAT1-receptor blockersCalsium antagonists-blockers-blockersACE inhibitorsPossible combination of different classes of antihypertensive agents. The most rational combinations are represented as thick lines. ACE, angiotensin-converting enzyme. The frames indicate classes of antihypertensive agents proven to be beneficial in controlled interventional trials.ESH-ESC 2003
-
Compelling Indication for Individual Drug ClassesChobanian AV, JNC VII, Hypertension. 2003JNC 7
Compelling indicationRecommended DrugsDiureticBBACEIARBCCBAldo ANTHeart failureXXXXXPost-myocardial infarctionXXXHigh coronary riskXXXXDiabetesXXXXXChronic renal diseaseXXRecurrent stroke preventionXX
-
Hypertension Controlin 5 European Contries, Canada & the US(% achieved 140/90 mmHg threshold)Wolf-Maier et al, Hypertension. 2004
-
Potential Reasons for Treatment FailureWhite Coat hypertensionSub optimal treatment regimentDrug interactionVolume overloadSeconddary cause of hypertensionOther conditions (obesity, chronic pain, etc)Khan NA, et al. CHEP Recommendation. CMAJ, 2005
-
SummaryHypertension is becoming a burden to the community due to its debilitating impact on target organs and hence premature death
Treatment has been proven to reduce morbidity and mortality, but majority of patients were not treated adequately
-
SummaryAggressive treatment has been shown to be of great benefit in terms of achieving more prompt target pressure and preserving target organ better
More frequent visits will be necessary for patients with stage 2 hypertension or with complicating comorbid conditions
-
SummaryMajority of management guidelines recommand broader use of drug combinations to achieve target blood pressure, which are:
-130/90 mmHg for uncomplicated hypertension-130/80 mmHg for Diabetics-130/80 mmHg for pts with Kidney Disease-120/75 mmHg for proteinuria > 1 G/day
-
Refence Cited from . Chobanian,et al. JNC 7, Hypertension. 2003;42:12061252.)Original reference :Burt VL, Whelton P, Roccella EJ, Brown C, Cutler JA, Higgins M, et al.Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 19881991. Hypertension. 1995;25:305313. X
SLIDE 8Penelitian oleh WHO tahun 2000 menunjukkan bahwa Hipertensi merupakan penyebab utama kematian pada negara yang sudah berkembang ( maju / developed region ) dan juga pada negara yang berkembang ( developing region ). Dinegara yang sedang berkembang hipertensi hanya dikalahkan oleh undernutrition / underweight.
SLIDE 29.JNC VII tahun 2003 menetapkan target < dari 140 / 90 mmHg dan < dari 130 / 80 mmHg pada penderita Diabetes dan penyakit ginjal menahun. Ditekankan perlunya mencapai tekanan sistolik < 140 mmHg terutama pada usia diatas 50 tahun.ESH tahun 2003 juga menetapkan target yang serupa, tetapi pencapaian target sistolik < 140 mmHg pada penderita usia lanjut mungkin lebih sulit dan harus dilakukan dengan hati hati.
Based on the clearly established need to control blood pressure in hypertensive patients, there has been an evolution of antihypertensive medications, starting with vasodilators and diuretics and leading to the more recent development of agents that directly inhibit the renin-angiotensin-aldosterone system, such as angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers.The more recently developed agents are well tolerated, with a high degree of efficacy. Many have side effect profiles similar to placebo.