
Management of giant omphalocele with rapid creation of abdominal domain
6
Management of giant omphalocele with rapid creation of abdominal domain Robert Foglia a, * , Alex Kane b , Devra Becker b , Jose Asz-Sigall a , George Mychaliska a a Division of Pediatric Surgery, Department of Surgery, Washington University School of Medicine, St Louis Children’s Hospital, St Louis, MO 63110, USA b Division of Plastic Surgery, Department of Surgery, Washington University School of Medicine, St Louis Children’s Hospital, St Louis, MO 63110, USA Abstract Background: The management of giant omphaloceles (GO) can be quite difficult when there is absence of abdominal domain. Coverage with delayed closure has been described. We present a technique to create an adequate peritoneal domain. Methods: This is a retrospective review of our experience using an intraperitoneal tissue expander (IPTE) to create adequate abdominal domain in 2 patients with GO. Results: In 2 children with unrepaired GO, an IPTE was placed into the pelvis and was inflated to the target volume over 3 to 4 weeks. At the definitive operation for the closure of the abdominal defect, the IPTE was removed, allowing reduction of all the viscera into the peritoneal cavity and achieving complete abdominal wall closure. The patients are now 1 year postoperative, each having a normal abdomen and enjoying normal growth and development. Conclusion: Intraperitoneal tissue expander placement can create the needed domain over several weeks in GO. Its use in 2 cases was associated with satisfactory complete abdominal wall closure in short order. This technique should be considered as a treatment option. D 2006 Published by Elsevier Inc. The management of abdominal wall defects, such as omphalocele or gastroschisis, has evolved over the past 4 decades. If primary fascial closure cannot be easily achieved, the use of a silo technique with staged closure is standard. However, the management of a giant omphalocele (GO), defined as an omphalocele with a fascial defect greater than 6 cm and with most of the liver in an extraperitoneal position, remains problematic. Many strategies have been used, such as Gross’s [1] description of skin-flap closure, the use of prosthetic material as a fascial bridge under the skin, sequential sac ligation, techniques to encourage epithelial- ization of the omphalocele membrane, silo application with gradual reduction of the extraperitoneal viscera (EPV), and sequential clamping without prosthetic material [2-5]. These techniques all describe coverage of the viscera with delayed closure. Others have described the relative advantages of nonoperative initial management in treating GO [6,7]. Fundamental to the problem with GO is the disproportion between the amount of EPV and the diminutive size of the peritoneal cavity. Gross aptly described the abdominal viscera as having blost its right of domicile in the peritoneal cavity.Q We felt that the creation of an adequate peritoneal domain was the primary aim of treatment. Our effort 0022-3468/$ – see front matter D 2006 Published by Elsevier Inc. doi:10.1016/j.jpedsurg.2005.12.013 Presented at the 57th Annual Meeting of the Section on Surgery of the American Academy of Pediatrics, Washington, DC, October 7-9, 2005. * Corresponding author. E-mail address: [email protected] (R. Foglia). Index words: Abdominal wall defect; Giant omphalocele; Tissue expander; Peritoneal domain Journal of Pediatric Surgery (2006) 41, 704 – 709 www.elsevier.com/locate/jpedsurg
-
Upload
robert-foglia -
Category
Documents
-
view
213 -
download
0
Transcript of Management of giant omphalocele with rapid creation of abdominal domain
www.elsevier.com/locate/jpedsurg
Management of giant omphalocele with rapid creation ofabdominal domain
Robert Fogliaa,*, Alex Kaneb, Devra Beckerb, Jose Asz-Sigalla, George Mychaliskaa
aDivision of Pediatric Surgery, Department of Surgery, Washington University School of Medicine,
St Louis Children’s Hospital, St Louis, MO 63110, USAbDivision of Plastic Surgery, Department of Surgery, Washington University School of Medicine, St Louis Children’s Hospital,
St Louis, MO 63110, USA
0022-3468/$ – see front matter D 2006
doi:10.1016/j.jpedsurg.2005.12.013
Presented at the 57th Annual Meetin
American Academy of Pediatrics, Washi
* Corresponding author.
E-mail address: [email protected] (
Index words:Abdominal wall defect;
Giant omphalocele;
Tissue expander;
Peritoneal domain
AbstractBackground: The management of giant omphaloceles (GO) can be quite difficult when there is absence
of abdominal domain. Coverage with delayed closure has been described. We present a technique to
create an adequate peritoneal domain.
Methods: This is a retrospective review of our experience using an intraperitoneal tissue expander
(IPTE) to create adequate abdominal domain in 2 patients with GO.
Results: In 2 children with unrepaired GO, an IPTE was placed into the pelvis and was inflated to the
target volume over 3 to 4 weeks. At the definitive operation for the closure of the abdominal defect, the
IPTE was removed, allowing reduction of all the viscera into the peritoneal cavity and achieving
complete abdominal wall closure. The patients are now 1 year postoperative, each having a normal
abdomen and enjoying normal growth and development.
Conclusion: Intraperitoneal tissue expander placement can create the needed domain over several weeks
in GO. Its use in 2 cases was associated with satisfactory complete abdominal wall closure in short
order. This technique should be considered as a treatment option.
D 2006 Published by Elsevier Inc.
inal wall defects, such as use of prosthetic material as a fascial bridge under the skin,
The management of abdomomphalocele or gastroschisis, has evolved over the past
4 decades. If primary fascial closure cannot be easily
achieved, the use of a silo technique with staged closure is
standard. However, the management of a giant omphalocele
(GO), defined as an omphalocele with a fascial defect greater
than 6 cm and with most of the liver in an extraperitoneal
position, remains problematic. Many strategies have been
used, such as Gross’s [1] description of skin-flap closure, the
Published by Elsevier Inc.
g of the Section on Surgery of the
ngton, DC, October 7-9, 2005.
R. Foglia).
sequential sac ligation, techniques to encourage epithelial-
ization of the omphalocele membrane, silo application with
gradual reduction of the extraperitoneal viscera (EPV), and
sequential clamping without prosthetic material [2-5]. These
techniques all describe coverage of the viscera with delayed
closure. Others have described the relative advantages of
nonoperative initial management in treating GO [6,7].
Fundamental to the problem with GO is the disproportion
between the amount of EPV and the diminutive size of the
peritoneal cavity. Gross aptly described the abdominal
viscera as having blost its right of domicile in the peritoneal
cavity.Q We felt that the creation of an adequate peritoneal
domain was the primary aim of treatment. Our effort
Journal of Pediatric Surgery (2006) 41, 704–709
Management of giant omphalocele with rapid creation of abdominal domain 705
was focused on identifying a technique to increase
peritoneal domain to the point that the viscera could be
reduced in one operation. Most of the described techniques
often required multiple-staged operations over a protracted
period to gradually reduce the EPV as the peritoneal cavity
was progressively increased in size. We report a novel
technique using an intraperitoneal tissue expander (IPTE) to
create peritoneal domain. It was used successfully in 2 pa-
tients, a newborn and a 4-year-old child who was previously
treated nonoperatively.
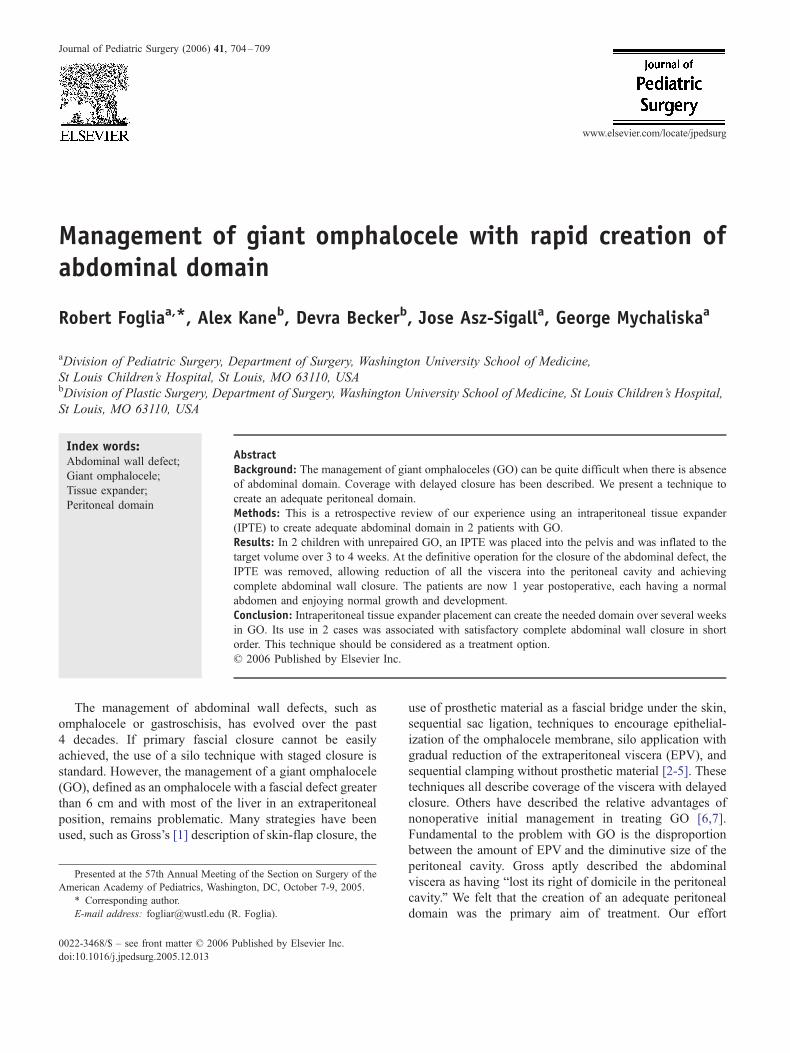
ig. 2 Computed tomography scan showing the EPV and the
iminutive peritoneal cavity.
1. Case reports
We treated 2 patients with GO, both with virtually the
entire liver extraperitoneal along with other abdominal
viscera, and minimal peritoneal domain. Both patients were
treated with the use of an IPTE to create adequate peritoneal
domain before visceral reduction and abdominal wall closure.
GH, a 4-year-old, 13-kg girl was born with a constellation
of anomalies including a left congenital diaphragmatic
hernia, an associated pulmonary hypoplasia and pulmonary
hypertension, an atrial septal defect, no inferior vena cava,
and a GO. She underwent repair of the diaphragmatic hernia
shortly after birth. No attempt was made to repair the GO
because of its massive size, the disproportion between the
EPV and the peritoneal cavity, and her associated problems.
A gastrostomy tube was placed into the stomach through a
lower left quadrant incision. She was hospitalized for the first
6 months of life. She moved to our community at 3.5 years of
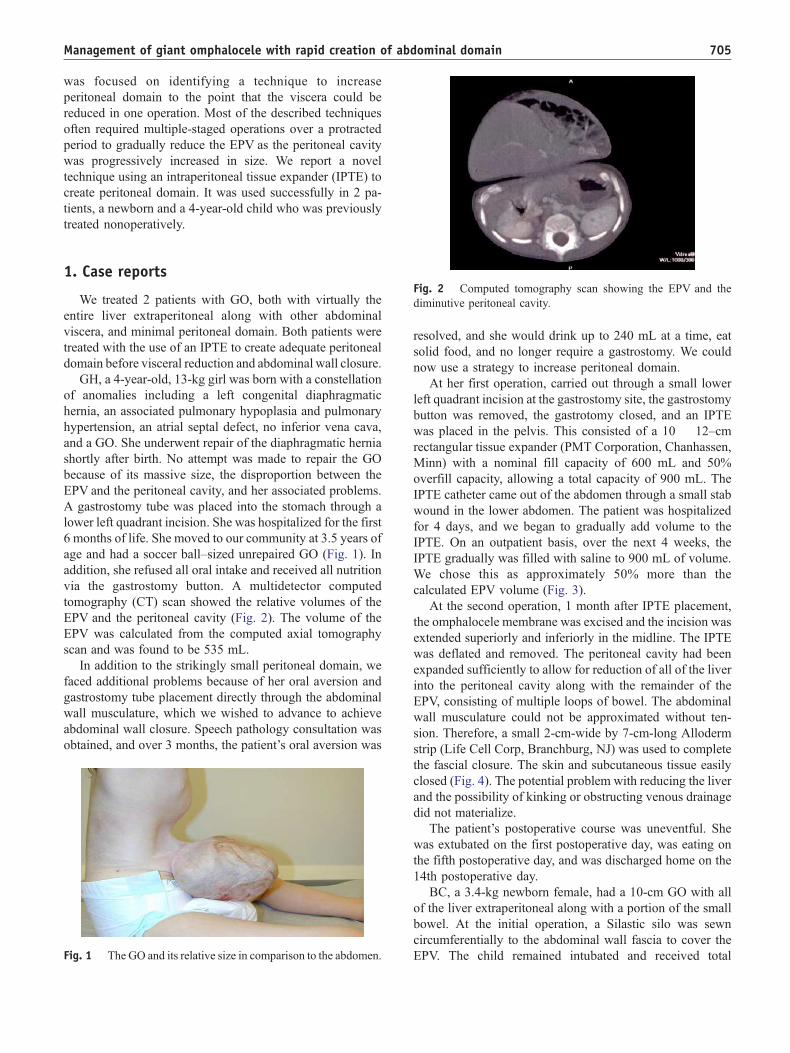
age and had a soccer ball–sized unrepaired GO (Fig. 1). In
addition, she refused all oral intake and received all nutrition
via the gastrostomy button. A multidetector computed
tomography (CT) scan showed the relative volumes of the
EPV and the peritoneal cavity (Fig. 2). The volume of the
EPV was calculated from the computed axial tomography
scan and was found to be 535 mL.
In addition to the strikingly small peritoneal domain, we
faced additional problems because of her oral aversion and
gastrostomy tube placement directly through the abdominal
wall musculature, which we wished to advance to achieve
abdominal wall closure. Speech pathology consultation was
obtained, and over 3 months, the patient’s oral aversion was
Fig. 1 The GO and its relative size in comparison to the abdomen.
Fd
resolved, and she would drink up to 240 mL at a time, eat
solid food, and no longer require a gastrostomy. We could
now use a strategy to increase peritoneal domain.
At her first operation, carried out through a small lower
left quadrant incision at the gastrostomy site, the gastrostomy
button was removed, the gastrotomy closed, and an IPTE
was placed in the pelvis. This consisted of a 10 � 12–cm
rectangular tissue expander (PMT Corporation, Chanhassen,
Minn) with a nominal fill capacity of 600 mL and 50%
overfill capacity, allowing a total capacity of 900 mL. The
IPTE catheter came out of the abdomen through a small stab
wound in the lower abdomen. The patient was hospitalized
for 4 days, and we began to gradually add volume to the
IPTE. On an outpatient basis, over the next 4 weeks, the
IPTE gradually was filled with saline to 900 mL of volume.
We chose this as approximately 50% more than the
calculated EPV volume (Fig. 3).
At the second operation, 1 month after IPTE placement,
the omphalocele membrane was excised and the incision was
extended superiorly and inferiorly in the midline. The IPTE
was deflated and removed. The peritoneal cavity had been
expanded sufficiently to allow for reduction of all of the liver
into the peritoneal cavity along with the remainder of the
EPV, consisting of multiple loops of bowel. The abdominal
wall musculature could not be approximated without ten-
sion. Therefore, a small 2-cm-wide by 7-cm-long Alloderm
strip (Life Cell Corp, Branchburg, NJ) was used to complete
the fascial closure. The skin and subcutaneous tissue easily
closed (Fig. 4). The potential problem with reducing the liver
and the possibility of kinking or obstructing venous drainage
did not materialize.
The patient’s postoperative course was uneventful. She
was extubated on the first postoperative day, was eating on
the fifth postoperative day, and was discharged home on the
14th postoperative day.
BC, a 3.4-kg newborn female, had a 10-cm GO with all
of the liver extraperitoneal along with a portion of the small
bowel. At the initial operation, a Silastic silo was sewn
circumferentially to the abdominal wall fascia to cover the
EPV. The child remained intubated and received total
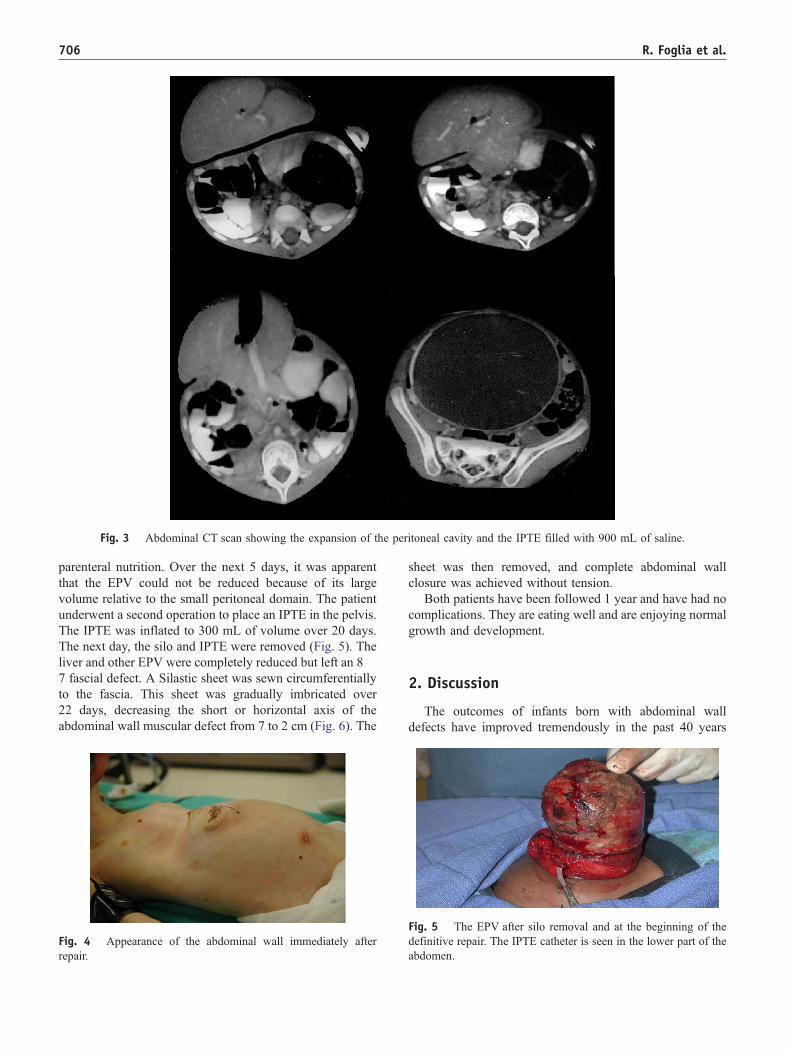
Fig. 3 Abdominal CT scan showing the expansion of the peritoneal cavity and the IPTE filled with 900 mL of saline.
R. Foglia et al.706
parenteral nutrition. Over the next 5 days, it was apparent
that the EPV could not be reduced because of its large
volume relative to the small peritoneal domain. The patient
underwent a second operation to place an IPTE in the pelvis.
The IPTE was inflated to 300 mL of volume over 20 days.
The next day, the silo and IPTE were removed (Fig. 5). The
liver and other EPV were completely reduced but left an 8 �7 fascial defect. A Silastic sheet was sewn circumferentially
to the fascia. This sheet was gradually imbricated over
22 days, decreasing the short or horizontal axis of the
abdominal wall muscular defect from 7 to 2 cm (Fig. 6). The
Fig. 4 Appearance of the abdominal wall immediately after
repair.
sheet was then removed, and complete abdominal wall
closure was achieved without tension.
Both patients have been followed 1 year and have had no
complications. They are eating well and are enjoying normal
growth and development.
2. Discussion
The outcomes of infants born with abdominal wall
defects have improved tremendously in the past 40 years
Fig. 5 The EPV after silo removal and at the beginning of the
definitive repair. The IPTE catheter is seen in the lower part of the
abdomen.

Fig. 6 Viscera reduced and the fascial defect bridged with
Silastic sheeting (8 � 7 cm) and imbricated in 2 stages.
Management of giant omphalocele with rapid creation of abdominal domain 707
because of medical and surgical advances. The development
of neonatal intensive care units, infant ventilators, and
hyperalimentation has dramatically improved survival. The
use of prosthetic material to assist in closure of the abdominal
wall was a turning point in the treatment of these children.
Before 1965, reports would often cite a mortality rate of 90%
for infants born with a gastroschisis. Schuster [2] first
described the use of prosthetic sheeting using artificial
material to bridge the abdominal muscle wall defect and then
to mobilize skin flaps in the fashion of Gross to cover the
sheeting. Pickett, Allen, and Wesselhoeft [cited in 8,9]
reported various techniques of using prosthetic material either
to bridge the fascial defect, but not to cover the prosthetic
material with skin, or to use the prosthetic material as a silo
to allow for coverage of the EPV and subsequent staged
closure. These techniques resulted in excellent outcomes for
most of the children with gastroschisis or omphalocele.
The management of the child with a GO, either a neonate
or an older child, who has never been repaired or has had a
failed repair, is complex and remains daunting. Patients with
particularly small peritoneal domain are especially challeng-
ing. Options that are available and have been used include
(1) short-term silo reduction (ideal if the peritoneal domain is
adequate), which may take several weeks followed by fascial
closure or closure with prosthetic material; (2) long-term silo
reduction over 2 to 6 weeks followed by closure; (3) a staged
reduction closing skin flaps over the omphalocele membrane
followed by delayed closure of the ventral hernia 6 to
12 months later; and (4) the use of external compression
before repair to facilitate delayed closure [10-12].
The fundamental problem with the GO is the insufficient
peritoneal domain in most of these infants. Silo placement
and staged closure allows for the gradual reduction of the
EPVwith increasing intra-abdominal pressure causing a slow
increase in peritoneal volume. Most of the aforementioned
techniques involve a series of operations over several weeks
to months to slowly and gradually increase intraperitoneal
domain. Often, the patients may not be able to be fed enterally
during this period, and there are potential complications with
silo dehiscence, infection, and compromise of blood flow to
visceral organs. Furthermore, in patients with GO, there is a
potential problem because of angulation or obstruction of
hepatic venous drainage through the suprahepatic inferior
vena cava [13,14]. Recognition of these problems is essential
in the operative treatment of these patients.
We chose to focus on a method to increase peritoneal
domain without using the viscera as the mechanism to
achieve an increase in intra-abdominal pressure. One of us
(AK) has had experience with tissue expansion. He had
identified that there was a case report of one patient in the
Netherlands with an omphalocele where a tissue expander
had been placed intraperitoneally [15]. He felt that this
might be advantageous in these patients with GO because
the peritoneal domain could be increased without using the
viscera as the source of pressure. The use of an IPTE has
several advantages: (1) one can precisely control the amount
of expansion; (2) it is less invasive than gradually
constricting or compressing the silo where the viscera are
used to exert increased intra-abdominal pressure; (3) and
with the information from the multidetector CT scan, one
can calculate the EPV volume and therefore make a
reasonable projection of how much volume the tissue
expander should be inflated.
This technique has worked well for us both in a newborn
and an older child. In the latter patient, the ability to have
her extubated and eating so quickly after the definitive
procedure is in contrast to the often prolonged postoperative
course and the need for a series of operative procedures
using a number of the other techniques in similar patients.
In the newborn, although we could reduce all of the
viscera into the peritoneal cavity proper, we could not
achieve abdominal wall closure. The gradual imbrication of
the Silastic sheet allowed us to slowly reduce the size of the
defect before abdominal wall closure. In the older child, a
small Alloderm patch was needed to bridge the fascia at
closure. These 2 points speak to the fact that surgical
judgment is necessary regarding how much abdominal wall
tension is acceptable. In the former case, the defect was so
large that we were reticent to use Alloderm for fascial
approximation. In the older patient, we felt that a small
Alloderm segment would function very well and could be
left permanently in place.

R. Foglia et al.708
References
[1] Gross RE. A new method for surgical treatment of large omphalo-
celes. Surgery 1948;24:277-92.
[2] Schuster SR. A new method for the staged repair of large
omphaloceles. Surg Gynecol Obstet 1967;125:837 -50.
[3] Hendrickson RJ, Patrick DA, Jannik JS. Management of giant
omphalocele in a premature low–birth weight neonate utilizing a
bedside sequential clamping technique without prosthesis. J Pediatr
Surg 2003;38:14 -7.
[4] Bawazir OA, Wong A, Sigalet DL. Absorbable mesh and skin flaps or
grafts in the management of ruptured giant omphalocele. J Pediatr
Surg 2003;38:725 -8.
[5] Fonkalsrud EW, Smith MD, Shaw KS, et al. Selective management of
gastroschisis according to the degree of visceroabdominal dispropor-
tion. Ann Surg 1993;218:742-7.
[6] Nuchtern JG, Baxter R, Hatch Jr EI. Nonoperative initial management
versus silo chimney for treatment of giant omphalocele. J Pediatr Surg
1995;30:771-6.
[7] Burge MD, Glasson MI. The conservative management of exompha-
los major. Aust N Z J Surg 1986;506:409 -11.
[8] Wesselhoeft CW, Randolph JG. Treatment of omphalocele based on
individual characteristics of the defect. Pediatrics 1969;44:101 -8.
[9] Randolph JG. In discussion of: evolution of staged versus primary
closure of gastroschisis. Ann Surg 2003;237:759 -65.
[10] Minkes RK. Abdominal wall defects. In: Oldman KT, Columbani PM,
Foglia RP, et al, editors. Surgery in infants and children: scientific
principles and practice. Philadelphia (Pa)7 Lippincott Raven; 2004. p.
1103-19.
[11] DeLuca FG, Gilchrist BF, Paquette E, et al. External compression as
an initial management of giant omphaloceles. J Pediatr Surg
1996;31:965 -7.
[12] Sander S, Elicevik M, Unal M. Elastic bandaging facilitates primary
closure of large ventral hernias due to giant omphaloceles. Pediatr
Surg Int 2001;17:664 -7.
[13] Carlton GR, Towne BH, Bryan RW, et al. Obstruction of the
suprahepatic inferior vena cava as a complication of giant omphalo-
cele repair. J Pediatr Surg 1979;14:733-4.
[14] Waldman JD, Fellows KE, Paul MH, et al. Angulation of the inferior
vena cava—right atrial junction in children with repaired omphalo-
cele. Pediatr Radiol 1977;5:142-4.
[15] Bax NMA, van der Zee DC, Pull ter Gunne AJ, et al. Treatment of
giant omphalocele by enlargement of the abdominal cavity with tissue
expander. J Pediatr Surg 1993;28:1181-4.
Discussion
Judson Randolph, MD (Nashville, TN): Chairman Lang-
ham, Chairman Smith, I hope everybody recognizes that
the importance of this paper is inversely proportional to
its length. This is an important concept for us. I’d like the
leave of the chairs to mention for a moment where we’ve
come from. You remember that Dr Gross developed flaps
of skin to go over the omphalocele way back in the 40s.
This worked for omphaloceles that were intact. It didn’t
work for giant omphaloceles, it didn’t work for gastro-
schisis, it didn’t work for ruptured omphaloceles, and we
ended up with defects that looked much like the first
patient that was shown. Sam Schuster, was the inventor
of the idea of plastic sewn to the rectus muscle, and then
skin closed over it. He insisted on the skin closure over
the plastic. That led to a series of operations, but
ultimately some dramatic success. It was Michel Gilbert
in Miami who first showed that the plastic didn’t need to
be covered by skin.
And shortly thereafter, Allen and Wrenn in Memphis,
Larry Pickett from New Haven, and Connie Wesselhoeft
and I in Washington all dealt with the plastic that could
be left outside the skin, and so began the long saga with
plastic pouches and then silos, and as you know, silos
were gradually improved. There was Dennis Shermeta
who had a preformed silo that could be rolled down,
Biemann Otherson, Chairman Smith’s partner, showed
that a double lumen silo would accommodate pressure
that could be pushed down. All of these things have
helped us with the problems such as were shown on these
slides. But I think that the idea that we can improve the
inner cavity of the abdomen is exciting, and I will bet
you that in just this audience, in the next year or two,
there will be 10 or 20 or even 25 patients who will
benefit from this concept.
I wish you would take just a moment to tell us a
little more about the insertion of the tissue expander.
Thank you.
R. Foglia, MD (response): Dr Randolph, thank you very
much for your comments. Essentially, what you can do if
you have an older child is to use the CT scan which will
allow you to calculate the volume of viscera that’s outside
of the peritoneal cavity. We simply took that volume,
added 50% to it, and chose an expander which could be
filled to that volume. The expander can be folded up fairly
easily so you make a small incision and put it in the
peritoneal cavity. You want to put it down in the pelvis.
You then begin to inflate through the catheter and increase
the volume over a number of weeks. In the newborn with
the giant omphalocele, a silo initially was sewn to the
fascia. When it was apparent that a typical staged closure
could not be performed easily, we chose to use an
expander. We could easily slip an expander down into
the pelvis bringing it out through a separate incision, much
the way you bring out a Tenckhoff catheter. So it’s
relatively straightforward.
Agostino Pierro, MD (London, UK): I very much enjoyed
this paper and congratulations for this treatment. This is a
difficult category of patients. We use a different strategy
that we reported in the May issue of this year’s JPS.
Twelve babies, repaired at birth with giant omphaloceles
with a defect between 8 and 15 cm, so in the same
category that you presented. What we’ve done is a series
of reductions of the silo. The key issue is that we use a
Prolene mesh and we suture it to the edges of the fascia
leaving a flat surface so that there is an ingrowth of tissue
into the mesh. The time that we needed to fully close the
abdomen was a median of 26 days. We felt that we
augmented the abdominal cavity by reducing progres-
sively, with a limited duration of technique and avoided

Management of giant omphalocele with rapid creation of abdominal domain 709
the use of a foreign body, such as a tissue expander. Did
you have any problem with breathing in your neonate,
because some of these babies have pulmonary hypoplasia
and don’t tolerate high intra-abdominal pressures or
elevation of the diaphragm?
R. Foglia, MD (response): There is no question that this
occurs in a number of children. You’ll have a chest in
some of these children which looks like a canine chest
or a Gothic window type thorax, and that’s especially
problematic. Here, I think one of the advantages we
found with the expander was that with instilling fluid in,
if there was a problem for example, you could simply
take the fluid out. So you really have a way to
accurately put fluid in or take it out, and it’s almost
like playing poker with somebody. You can raise the
amount, and if you find it’s too much, you can back it
off a little bit. The technique you’re describing sounds
like is a very good one too. I think that it’s something
that as pediatric surgeons, we should have as many
things as we can in our armamentarium that we can use
in taking care of these children.
Agostino Pierro, MD (London, UK): With our technique, we
could release the pressure by releasing the tack that we’ve
done on the Prolene mesh, but the key issue is the Prolene
mesh, and the ingrowth of the Prolenemesh into the fascia.
Arthur Cooper, MD (New York, NY): Congratulations on an
outstanding contribution. I rise primarily to call the
attention of the section to the technique described by my
colleague, Dr Barbara Barlow, here about 15 years ago,
on external reduction using an external wrap for intact
omphaloceles. We’ve continued to use that technique
over the last 15 years, and we have not needed to use a
silo for anything but the very largest omphaloceles.
Thanks to you we now have a technique to use with those
children as well.
R. Foglia, MD (response): Thanks.
Michael A. Skinner, MD (Durham, NC): This is a very
interesting technique. What was the reason for placing the
Silastic on for a period of time before putting the expander
in?Were you concerned that if you just put the expander in
with the omphalocele sac intact, that it would just stretch
the sac instead of stretching the abdominal cavity?
R. Foglia, MD (response): The short answer is that actually
one of the other surgeons had put the Silastic on first and
then I became involved afterwards, and the technique we
were looking at was evolving at the same time. So it was
a case of probably the right approach at an opportune
time. Typically with a giant omphalocele if he had
chosen not to let the thing just epithelialize, we would
cover it with Silastic and see if it could be reduced. Over
that first 5 days or so, it was apparent that we weren’t
going to get anywhere. We needed to look at doing
something else, so that’s why we chose to put the
expander in after the silo had been placed.
Michael A. Skinner, MD (Durham, NC): So, for next time,
are you just going to make an incision and place the
expander and defer repairing the omphalocele until you
have established an increased abdominal domain?
R. Foglia, MD (response): I think that’s what we’re looking
at doing next. We have another child right now who is
much like the other one, it’s a 5-year old who has a
number of other issues, so we have that one sort of in the
wings, but I think with the newborn, we would consider
using this a priori. Yes.
















![Cloacal exstrophy associated with gastroschisis: Case ...gastroschisis, omphalocele, bladder exstrophy, and cloacal exs-trophy [1,2]. Gastroschisis is a defect of the anterior abdominal](https://static.fdocuments.in/doc/165x107/5f82b6822991d932fc2027c1/cloacal-exstrophy-associated-with-gastroschisis-case-gastroschisis-omphalocele.jpg)

